
BREAKING THE CYCLE OF REJECTION THE PERSONALITY...
18
www.nimhe.org.uk BREAKING THE CYCLE OF REJECTION THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK National Institute for Mental Health in England 33954 1p 10k Nov 03 (EDW) For more copies of this document, please contact your local development centre or the central team in Leeds. Contact NIMHE Central Team The National Institute for Mental Health in England Blenheim House West One Duncombe Street Leeds LS1 4PL Tel: 0113 254 5000 Web: www.nimhe.org.uk NIMHE is part of the modernisation Agency at the Department of Health
Transcript of BREAKING THE CYCLE OF REJECTION THE PERSONALITY...

www.nimhe.org.uk
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
National Institute forMental Health in England
33954 1p 10k Nov 03 (EDW)
For more copies of this document, please contact your local development centre or the central team in Leeds.
Contact NIMHE Central Team
The National Institute for Mental Health in EnglandBlenheim HouseWest OneDuncombe StreetLeeds LS1 4PL
Tel: 0113 254 5000
Web: www.nimhe.org.uk
NIMHE is part of the modernisation Agency at the Department of Health

BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
Contents
2
3
4
1
Foreword
Executive summary
SECTION ONEIntroducing the PersonalityDisorder CapabilitiesFramework
SECTION TWOMeeting the needs of service users
SECTION THREEThe broader policy context
SECTION FOURThe Personality DisorderCapabilities Framework
AppendicesI Acknowledgements 32II Contact details 34
04
06
10
16
22
32
05

05
NIMHE (2003) PersonalityDisorder: No longer a diagnosis of exclusion. Policyimplementation guidance forthe development of servicesfor people with personality disorder. Department of Health
NOTES
Purpose
FOREWORD EXECUTIVE SUMMARY
The publication of the National Institute for Mental Health (NIMHE) guidance onpersonality disorder, Personality Disorder: No Longer a Diagnosis of Exclusion, wasan important first step towards ending the marginalisation of services to peoplewith this deeply stigmatising diagnosis.
The guidance aimed to ensure that, in addition to the development of bothspecialist mental health and forensic services to people with personality disorder,staff would be equipped with the education and training they need to workeffectively. The NIMHE guidance signalled the commitment of the DH to pumpprime the development of new training initiatives to underpin the policyimplementation process.
This document, the Personality Disorder Capabilities Framework, has beenproduced by NIMHE to support this pump priming process. It does this byhighlighting some of the capabilities, appropriate to interactions with people withpersonality disorder, required within services, by staff at all levels of their careers. Inrecognition of the fact that, in many cases, people with personality disorder seekhelp from a wide range of specialist and non specialist agencies, it aims to describewhat capabilities are required across the whole system. This is the first time thatthis has been attempted. It is not, therefore, a definitive list. As the policyguidance is implemented, our understanding of what is required, and in particularhow these capabilities may be applied by different professional groups, or withinspecific services will evolve and understanding will grow.
Through eight Regional Development Centres and our website: www. nimhe.org.ukwe will be working to support local and regional agencies and partnerships toassess training needs and define the content of education and trainingprogrammes to support the development of approaches which will break the cycleof rejection, which is so frequently experienced by people with personality disorder.
Contact details for the eight NIMHE Regional Development Centres are provided.Do get in touch if you want to discuss any of the issues discussed in the document,or to explore ways forward for personality disorder services in your area.
Professor Eddie KaneSenior Advisor to the Department of Health Forensic and High Secure Psychiatric Services
Training: one of the keys topolicy implementationAs part of the process forimplementing the guidance onpersonality disorder, local healthand social care communities areasked to assess how agenciesacross primary and specialist healthcare, A&E services, housing andsocial services, are responding toand providing for people withpersonality disorder. Thisassessment should be followed byinter-agency arrangements toredesign and improve services.Training may be critical inimproving services, particularlythose provided by generic workerswhether in health, local authorityor voluntary sector services.Evidence suggests that there areparticular training needs amongststaff working in primary care, inself-access health services such ashospital emergency departments,PALs services, housing agencies andthe police. This framework isdesigned to support local andregional partners and WorkforceDevelopment Confederations indesigning and commissioning therequired education and training.
The Characteristics of theFramework The Framework is based on anumber of clear principles aimed atbreaking the cycle of rejection,which has characterised the debateabout personality disorder andshaped service delivery up to now.It is driven by optimism about thepossibility of creating responsiveand non-stigmatising services,promoting social inclusion anddelivering better outcomes forindividuals with a diagnosis ofpersonality disorder.
This document provides further information on the implementation of the NIMHEguidance on personality disorder: Personality Disorder: No Longer a Diagnosis of Exclusionwhich was published in January 2003.1
The Aim of the FrameworkThe Personality DisorderCapabilities Framework identifiesthe specific capabilities required ofstaff working with people withpersonality disorder in a range ofsettings and at various differentstages of their careers.
Agencies wishing to developtraining programmes for staff willbe able to use the Framework as aguideline to identify which groupsof staff require training to supportthe user pathway at identifiedpoints including:
� Initial access and referral;
� Sustained episodes of treatmentand care;
� Supporting recovery and steppingdown from treatment.
Staff can expect to develop thesecapabilities through innovative,multi disciplinary training courses,at appropriate levels for their jobroles, which are linked to career/skills escalator approaches and life-long learning frameworks. Staffshould be able to progress alongthe personality disorder skillsescalator to achieve senior clinicaland/or managerial positions withinthe web of new services that willemerge in the next few years, asthe NIMHE guidance is fullyimplemented. New local trainingprogrammes will ensure thatpeople with the right attitudes,values and life experiences to workeffectively with people withpersonality disorder are alsoprovided with the necessary skillsand knowledge. These trainingprogrammes, or components ofthem, should be embedded fullywithin local education and trainingprogrammes at all levels.
An Evolving FrameworkThe Framework should be seen as awork in progress, underpinning thedevelopment of new trainingprogrammes for staff in order tofurther the implementation of theNIMHE guidance. One by-productof this implementation process willbe better knowledge about whatconstitutes effective service modelsfor people with personality disorder– and of the capabilities required ofstaff. This increasing knowledgeand confidence will ensure that theFramework continues to evolve.
1
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
04
07
NIMHE (2003) PersonalityDisorder: No longer a diagnosisof exclusion. Policy implementation guidance forthe development of servicesfor people with personality disorder. Department of Health
Sainsbury Centre for MentalHealth (2001) The CapablePractitioner. A framework andlist of practitioner capabilitiesrequired to implement theNational Service Frameworkfor Mental Health
http://www.doh.gov.uk/mentalhealth/personalitydisorder.htm
Duggan, Conor (2002)Pathways in and out of secure care for people withpersonality disorder.www.nimhe.org.uk/archivepolicy/nhs.asp#pd
Duggan, Maria (2002)Developing Services for Peoplewith Personality Disorder: Thetraining needs of staff andservices.www.nimhe.org.uk/archivepolicy/nhs.asp#pd
NOTES
Purpose Developing the Framework
SECTION ONE
INTRODUCING THE PERSONALITYDISORDER CAPABILITIES FRAMEWORK
This document represents an important step forwards in the implementation of theNIMHE guidance on personality disorder: Personality Disorder: No Longer a Diagnosis ofExclusion which was published in January 2003.2 A copy of the NIMHE guidance can bedownloaded from www.nimhe.org.uk
The document sets out a Framework to support the development of practitionercapabilities and workforce capacity programmes within new, dedicated personalitydisorder services, in mainstream mental health services, primary care and in the widerange of other agencies involved in treating and supporting people with personalitydisorder. The Framework is at the end of this document
The fundamental aim of this Capabilities Framework is to help create a workforce thathas a better understanding of personality disorder and is more aware of its impact onindividuals, families, agencies and society more broadly. This workforce will be able torespond more appropriately, compassionately and non-judgementally to behaviours thatare often hard to understand and change. The workforce should be able to work moreconfidently within well managed teams delivering the wide range of evidence-basedinterventions that we increasingly understand can help those labelled personalitydisordered to make positive changes in their lives in much the same way as people withother forms of mental illness. This workforce will also be able to support and empowerthose who use services, taking into account their needs for social support and theresources to support daily living and will be able to collaborate across teams and sectorsto access these services.
These efforts may interrupt the cycle of rejection that is deeply implicated in thedevelopment of personality disorders and which is compounded by the negative andrejecting attitudes and practices of many agencies.
The Personality DisorderCapabilities Framework builds onThe Capable PractitionerFramework3 proposed by theSainsbury Centre for Mental Health(SCMH), which sets out a list ofpractitioner capabilities for multidisciplinary groups of staff workingwithin mainstream mental healthservices. The Personality DisorderCapabilities Framework identifiesthe specific capabilities required ofstaff working with people withpersonality disorder in a range ofsettings and at various differentstages of their careers. The NIMHEGuidance envisages that, in future,mental health services and otheragencies will be better prepared torespond to the needs of peoplewith personality disorder. It isappropriate therefore to ensurethat the capabilities required ofstaff in this area are fully integratedinto pre and post qualifyingtraining for all mental health carestaff to ensure that this aspirationcan be realised. Indeed, many ofthe required capabilities for work inthis area are exactly the same asthose required in other areas ofmental health services. These ‘core’capabilities are listed in detail in theSCMH Capable Practitioner
Framework and are therefore notincluded here. A copy of theCapable Practitioner Frameworkcan be downloaded from:www.scmh.org.uk
The Personality DisorderCapabilities Framework takes intoaccount the emerging work on the‘shared capabilities’ of the mentalhealth workforce being undertakenby a range of national partnersunder the auspices of NIMHE,which is beginning to map out thepotential content of a pre-registration core curriculum for allmental health staff to underpinspecific, professional training. TheNIMHE guidance is clear that infuture, staff will need to developthe capability to work with peoplewith personality disorder in theirinitial training and thatopportunities for updating andextending these skills will need tobe provided through continuingprofessional development andother forms of life long learning.
The Framework also links withother key national workforcedevelopment initiatives within theNHS and related sectors. It drawson extensive research into theavailability and characteristics of
existing training relevant to workwith people with personalitydisorder undertaken to support thedevelopment of PersonalityDisorder: No Longer a Diagnosis ofExclusion and a number of othertechnical papers, which informedits conclusions.4 These papers canbe accessed at:www.nimhe.org.uk/archivepolicy/nhs.asp#pd
The Framework was tested andmodified by a working group ofexperts from a variety of agenciesand disciplines.
The development process wasstrengthened by the comments of anumber of service users whoshared their experiences, describedgood multi disciplinary practicefrom their perspective andunderscored the need for the user’s perspective to be central tothe development of approacheswhich work.
Members of the expert group, theservice-users group and others whosupported the development processare listed at Appendix I.
We are grateful to the many peoplewho have helped with thedevelopment of the Framework.
2
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
06
1
Why do we need a Capabilities Framework?Lack of Skills and knowledgeThere is very limited good-qualityevidence about what happens atthe moment to people withpersonality disorder outside of thehigh secure sectors. However, suchevidence as exists suggests thatpeople with personality disordervery frequently become revolvingdoor patients, attempting to obtainhelp from a wide range ofcommunity services that are oftenunable and / or unwilling to provideit. There may be particularproblems in primary care whenspecialist services reject people withpersonality disorder and refer themback to GPs. Like other clinicalstaff, GPs and other disciplineswithin primary care teams havevery little specific training in thediagnosis, treatment and
management of personalitydisorders; yet, they are frequentlythe first point of contact for manyservice users. Similar difficulties arereported within PALs services, andin the range of self-access services,often provided by the voluntarysector, to which people may turnfor help, as well as in socialhousing.
The lack of adequate community-based provision has a triple effect.The endless cycle of rejection canintensify the distress and thereforethe difficult behaviour of someindividuals. It also means that thosewho are receiving intensive supportand therapy, possibly in in-patientsettings, can experience numerousbarriers in returning to thecommunity and in coping
effectively. This in turn impacts onthe capacity of the specialistservices to successfully treat andrehabilitate patients.5
The NIMHE guidance cites evidencethat the negative attitudes andpractices of many agencies reflect alack of skills and knowledge inrelation to the specific needs ofpeople with personality disorder.6
Staff currently have no explanatoryframework for the challengingbehaviours which may be exhibitedby people with disorders or theskills to address these behaviourseffectively. As a consequence theymay respond with negativejudgements and exclusionarypractices, which may denyindividuals the services they need,including health care.
3
4
5
6
09
Sainsbury Centre for MentalHealth: (2001) The CapablePractitioner. www.scmh.org.uk
Haigh Rex and Pearce Steve (January 2003) Clinical Ideasfor a comprehensive personalitydisorder service for the ThamesValley. unpublished
Birmingham and SolihullMental Health NHS Trust.Standards for Clinical Teams:From medium security into the community. unpublished
NOTES
The scope of the Personality Disorder Capabilities Framework Who is the Framework for?
SECTION ONEINTRODUCING THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
This Framework is relevant to thechallenges faced by the wide rangeof organisations involved indelivering health, social care,housing, employment and othersupport to people with personalitydisorder, their carers and membersof their wider social networks. It istherefore relevant for all of thefollowing:
� NHS organisations; includingPCTs, mental health trusts(general, acute andcommunity services), strategichealth authorities andworkforce developmentconfederations
� Social Services
� Independent GP practices
� Housing agencies
� Criminal Justice Systemagencies.
The Personality DisorderCapabilities Framework aims todescribe what is required of all staffworking with people withpersonality disorder, in primarycare, in secondary mental healthservices including new personalitydisorder units and in the widerange of other community basedagencies, which people maycontact.
Levels of capability The Framework recognises thatstaff may need different levels ofthe same capability depending ontheir roles and functions withindifferent service contexts. Itintroduces the concept of the skills/careers escalator which enables thedevelopment of valued careerpathways in working with peoplewith personality disorder,recognising that, as in many otherareas of health and social careprovision, some of the mostvaluable work is undertaken bythose who may not have formalprofessional qualifications – orindeed by service users themselves.The range and complexity of theneeds presented by those withpersonality disorder requires the co-ordinated input of many differentdisciplines and of specialist andnon-specialist agencies. As aconsequence, many of these staffmay work outside of the mentalhealth sector, or indeed, the NHSor local authorities. These staffneed an appropriate level ofunderstanding and skill inengaging, communicating with,delivering specific services to andundertaking appropriate referralof people with personality disorderwho request help.
Capabilities for management and leadershipMoreover, as the NIMHE guidancepoints out, the management ofteams and the leadership of organisations providing services topeople with personality disorder areparticularly important. Without this,there is likely to be a high degreeof staff burnout, absenteeism, sickness and disillusion. Staff working in specialist community agencies will need to be supportedjust as much as those within dedicated services in sustaininggood practice. The Framework outlines the management and leadership capabilities required
to support staff and therefore toensure the sustainability of services.In line with the whole systemsapproach of the NIMHE Guidance,the Framework outlines capabilitiesin liaison and consultancy, whichshould be central to the role ofmanagers and leaders within spe-cialist services in supporting thewider service network.
Capable organisationsStaff can only become and remaineffective if the organisation andsystem within which they workunderstands what is required tosupport capable practice. Goodmanagement and leadership arekey. However the capableorganisation requires more thanthis, including:
� Operational models that canrespond to the complexity ofthe needs presented byservice users 8
� Ease of access to appropriatelevels of treatment andsupport
� The development of standardsfor multi disciplinary servicedelivery 9
� Cross boundary and crossagency agreements tosupport the, movement ofservice users away fromdependency on services andtowards proper socialinclusion.
� Consistent support for staffteams
� Access to supervision,education and training.
Sustaining learningThe concept of the capableorganisation has importantimplications for the way in whichlearning opportunities are deliveredand sustained. This Frameworkilluminates some of the content ofeducation and training programmesfor staff working with people withPD. However, it does notrecommend or imply any particularmode of delivery. The boundarybetween training, practicedevelopment and supervision isvery blurred in mental health andall of these may have a role to playin supporting and extending thecapabilities of staff. Attention isincreasingly being focussed onlearning approaches that supporteffective team and servicefunctioning. These may includedistance learning, whole-teamtraining and practice developmentmentoring amongst others. Thechallenge will be to identify modelsthat can be applied to groups ofstaff drawn from services acrosswhole-systems as well as withindiscrete services and teams. Oneby-product of the implementationof the Framework may be greaterconfidence about whichapproaches work.
It is useful for staff throughoutthese organisations from boardlevel to those involved in servicedelivery.
It is also relevant for professionaland regulatory bodies andeducation providers in further andhigher education who will workwith trusts and other organisationsto translate this framework intocurricula at various levels todevelop a career skills escalator forworking with people withpersonality disorder.
It will underpin the implementationof the NIMHE guidance PersonalityDisorder: No Longer a Diagnosis ofExclusion.
How can you use the Framework?The Personality DisorderCapabilities Framework can beused in a variety of ways,depending on your role within anorganisation. For example:
� To initiate ‘whole-systems’workforce developmentplanning for personalitydisorder services
� To develop targeted trainingfor specific groups and sectorswithin a strategic approach toimplementing the NIMHEguidance on personalitydisorder
� To align career and trainingpathways to existing lifelonglearning approaches withintrusts and other organisations
� To influence the developmentof multi-disciplinary pre andpost qualification traininglocally, regionally andnationally.
� To align the content of pre-registration and CPDprogrammes for the mentalhealth disciplines
� To strengthen themanagement and leadershipof personality disorderservices.
It can also be used to develop user-focused approaches to training andto stimulate the development ofprogrammes that actively involveservice users as trainers.
7
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
08
� Performance – skills practitioners need to possess and what they need to achieve in the workplace
� Ethics – integrating a knowledge of culture, values and social awareness inprofessional practice
� Reflective practice. The capability to effectivelyimplement evidence-basedinterventions
� A commitment to lifelonglearning.7
THE PERSONALITY DISORDERCAPABILITIES FRAMEWORKENCOMPASSES:
8
9

11
Moran, Paul (2002) TheEpidemiology of PersonalityDisorder. www.nimhe.org.uk/archivepolicy/nhs.asp#pd
From a service user quoted inPersonality Disorder NorthEssex News. July/August 2003– issue 24
NOTES
Towards Positive Practice
SECTION TWO
MEETING THE NEEDS OF SERVICE USERS
De-stigmatising personality disorder
In order to work positively with people with personality disorder, there is a need to understand the causes and the consequences of this complexcondition. In recent years, the emphasis on risk and dangerousnessassociated with a very small number of people with personality disorder,has obscured the fact that very many people with this diagnosis are highly vulnerable to abuse and violence themselves – and to self-harm and suicide.10
The NIMHE guidance aims to challenge the discriminatoryassociation between personality disorder and dangerousness byputting in place services aimed at reducing vulnerability andpromoting more effective coping by individuals.
Developing reflective practicePeople with personality disorderscan behave in ways that mightappear to invite rejection. They mayfeel that no help is ever goodenough, they may be hostile ordemanding. They can, at times,sabotage all attempts at help. Thiscan be frustrating and difficult forpractitioners. Skills and knowledgeare required to enable staff tounderstand the reasons for thisbehaviour; to ‘rise above’ rejecting,judgmental or compulsiveresponses and to reflect calmlyabout what may be happening.Practitioners who have thesecapabilities can maintain a focus onthe underlying needs of individualsand can sustain the effort to assistthe individual in developing lessdestructive ways of dealing withrelationships. These staff can alsosupport the individual in obtainingthe range of social resources thatare a fundamental determinant ofgood mental health, includinghousing, employment, socialsupport and access to leisure andeducational opportunities.
From revolving doors topathway approaches to care and treatment The inadequacy of integratedservice provision and the lack ofskills within the workforce meansthat, at the moment, people withpersonality disorder are obliged toseek help from multiple agencies.An example of this negative,‘revolving door’ pathway isdescribed on the next page. Theimplementation of the NIMHEguidance will ensure that a morecoherent approach is taken at locallevel to responding to these needs.The development of a skilledworkforce will be key to thesedevelopments.
Service users themselves suggestanother way of understanding theissues, which they face.
10
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
10
2
We have been damaged, often early in life and we have grown up withmistaken beliefs about ourselves. For these reasons we have difficulties with relationships because we oftenbelieve that we are unlovable and we are very sensitive to rejection. For thatreason, we need easier and known access to services.11
We suffer from post-traumaticpersonality disorder. We have a reactivemental illness.
”
”
“
“
11
13
Case study
negativeWho is the Framework for?
SECTION TWOMEETING THE NEEDS OF SERVICE USERS
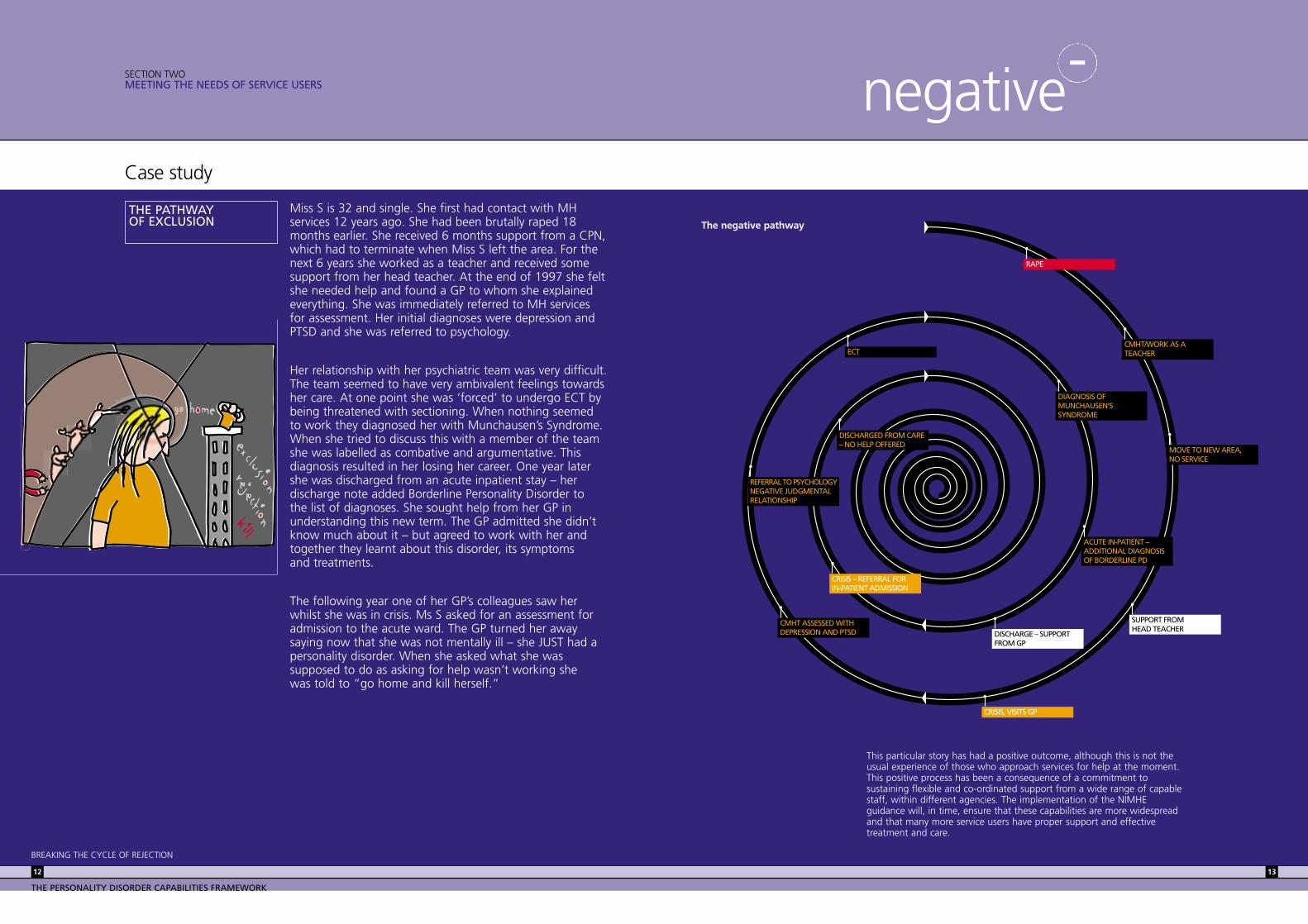
Miss S is 32 and single. She first had contact with MHservices 12 years ago. She had been brutally raped 18months earlier. She received 6 months support from a CPN,which had to terminate when Miss S left the area. For thenext 6 years she worked as a teacher and received somesupport from her head teacher. At the end of 1997 she feltshe needed help and found a GP to whom she explainedeverything. She was immediately referred to MH servicesfor assessment. Her initial diagnoses were depression andPTSD and she was referred to psychology.
Her relationship with her psychiatric team was very difficult.The team seemed to have very ambivalent feelings towardsher care. At one point she was ‘forced’ to undergo ECT bybeing threatened with sectioning. When nothing seemedto work they diagnosed her with Munchausen’s Syndrome.When she tried to discuss this with a member of the teamshe was labelled as combative and argumentative. Thisdiagnosis resulted in her losing her career. One year latershe was discharged from an acute inpatient stay – herdischarge note added Borderline Personality Disorder to the list of diagnoses. She sought help from her GP inunderstanding this new term. The GP admitted she didn’tknow much about it – but agreed to work with her andtogether they learnt about this disorder, its symptoms and treatments.
The following year one of her GP’s colleagues saw herwhilst she was in crisis. Ms S asked for an assessment foradmission to the acute ward. The GP turned her awaysaying now that she was not mentally ill – she JUST had apersonality disorder. When she asked what she wassupposed to do as asking for help wasn’t working she was told to “go home and kill herself.”
This particular story has had a positive outcome, although this is not theusual experience of those who approach services for help at the moment.This positive process has been a consequence of a commitment tosustaining flexible and co-ordinated support from a wide range of capablestaff, within different agencies. The implementation of the NIMHEguidance will, in time, ensure that these capabilities are more widespreadand that many more service users have proper support and effectivetreatment and care.
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
12
THE PATHWAY OF EXCLUSION
-
RAPE
CMHT/WORK AS A TEACHER
MOVE TO NEW AREA,NO SERVICE
SUPPORT FROMHEAD TEACHER
CRISIS, VISITS GP
CMHT ASSESSED WITH DEPRESSION AND PTSD
REFERRAL TO PSYCHOLOGYNEGATIVE JUDGMENTAL RELATIONSHIP
ECT
DIAGNOSIS OF MUNCHAUSEN’SSYNDROME
ACUTE IN-PATIENT –ADDITIONAL DIAGNOSISOF BORDERLINE PD
DISCHARGE – SUPPORT FROM GP
CRISIS – REFERRAL FOR IN-PATIENT ADMISSION
DISCHARGED FROM CARE– NO HELP OFFERED
The negative pathway

15
Gunn J. (April 2000) Futuredirections for treatment inforensic psychiatry. The BritishJournal of Psychiatry. Vol 176.Page 332-339
NOTES
Case study Recovery and Personality Disorder
positiveSECTION TWOMEETING THE NEEDS OF SERVICE USERS
On recovering from this crisis Ms S complained to thehospital medical director, who took over her care. Thechange in this relationship was instant. She felt supportedat last by her psychiatrist who listened to her and workedwith her. The psychiatrist prescribed a number of differentmedications to find the best ones for her symptoms. Herpsychologist saw her regularly for work on getting hermore settled emotionally. Her GP reviewed her fortnightlyand as necessary if she was in crisis. Her psychiatristreviewed her case and said that the ECT was given for nomedical reason. The diagnosis of Munchausen’s Syndromewas overturned. The psychiatrist, psychologist and GPremained in close contact through letters and email.
This relationship ended when the psychiatrist changed jobs,however she arranged for Miss S to be placed under thecare of another colleague whom she thought would beable to work well with Miss S. This new relationship wasgood from the start. He listened and explained things toher as needed.
She has now had consistent support from her GP andpsychologist for 6 years and good psychiatric support forthree years. She has completed a course of DialecticalBehaviour Therapy (DBT) and is self harming less frequently.She has done some work with her psychologist on dealingwith the traumatic thoughts around the rape. Her careteam see her regularly and respond quickly to any crisis.The change over the last couple of years has been dramatic– this she feels is due to both the DBT and the fact that shehas consistent support from her GP, Psychologist andPsychiatrist.
She is now moving on, using the insight she has gained tohelp deliver the DBT course in her area from a service usersperspective and is helping others both locally and nationallyto live with this diagnosis.
As this story illustrates, the conceptof recovery, which is gainingground within mainstream mentalhealth services, has been influentialin shaping the Personality DisorderCapabilities Framework.
Driven in large part by anincreasingly assertive andsophisticated user movement, theconcept directly challenges thepreviously negative judgementsheld by mental health staff andsociety at large about the prospectsof those affected with mental
illness. These negative judgementsare particularly problematic forpeople with personality disorder,which has up to now been a deeplystigmatising label. The conditionhas, until recently, been considereduntreatable by many specialistmental health services. As aconsequence, the psychological andsocial distress experienced bypeople labelled as personalitydisordered has been compoundedby their exclusion from services. It has been suggested that:
In Britain we havethe remarkable
phenomenon that largenumbers of quite severelydisordered people whorequire considerabletherapeutic effort aredeemed ‘untreatable’ 12
However, these negative views areincreasingly being challenged bythe findings of research. TheNIMHE guidance devotes significanteffort to specifying treatments forwhich there is growing evidence ofeffectiveness. However, it is clearthat, in order to be effective,treatment and support regimesshould be intensive, are frequentlylong term and based on a cleartreatment alliance betweenclinicians and patients. These kinds of relationships and theinterventions that are deliveredthrough them require well-trainedstaff with positive attitudes and an appreciation of ethical practice issues.
12
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
14
THE RECOVERY PATHWAY
+
”
“
SUSTAINED SUPPORTFROM PSYCHIATRIST
MEDICATIONS REVIEWAND MANAGEMENT
RECOVERY FROM CRISIS
FIORTNIGHTLY REVIEWWITH GP
SENSITIVE TRANSFER OFCARE WHEN STAFF CHANGE
REFERRAL FOR DBT
CLOSE LIAISON BETWEENGP, PSYCHIATRIST ANDPSYCHOLOGIST
DIAGNOSIS OF MUNCHAUSEN’SSYNDROME OVERTURNED
SUSTAINED CONSISTENTCARE OVER A LONG PERIOD
CARE CO-ORDINATEDTHROUGH THE HOSPITAL’SMEDICAL DIRECTOR
REGULAR SUPPORTFROM PSYCHOLOGIST
The positive pathway

17
DH (March 2003) Agenda forChange: proposed agreement.DH Publications
DH (November 2001) WorkingTogether – Learning Together. A Framework for LifelongLearning in the NHS. DH Publications
DH (March 2003) Agenda forChange: Knowledge and Skills Framework. DH Publications
NOTES
Modernising Mental Health services
SECTION THREE
THE BROADER POLICY CONTEXT
The ways in which the mental health disciplines and related staff groupsdevelop, update and extend their capabilities are currently under scrutinyfrom the Government, Strategic Health Authorities and WorkforceDevelopment Confederations. This scrutiny reflects a range of demand andsupply factors, which affect the implementation of the overall NHSmodernisation agenda in relation to mental health and the development ofpersonality disorder services in particular.
Furthermore, the supply of relevanttraining is limited at both pre andpost qualification levels. Suchtraining as exists is frequentlydriven by the energy andcommitment of local ‘productchampions’ rather than thestrategic needs of services. As aconsequence, training provision isskewed towards addressing theinterests of these committedindividuals. There is very littletraining that is particularly relevantto the needs of staff working ingeneric, community based servicesincluding primary care, PALs,emergency departments, socialhousing, social services or thevoluntary sector, although theseagencies are undoubtedly burdenedby the demands made by peoplewith personality disorder. Howevertraining development has not, todate, been configured to addressthe needs of service users or carersholistically or to support the effortsof the wide range of servicespotentially involved with individualswhose needs are both profoundand complex.
See: www.nimhe.org.uk/downloads/ReportJuly112002.doc
The Personality DisorderCapabilities Framework aims to support a strategic approach to workforce and skills development across the systemswithin the national policy contextdescribed above.
Demand factorsThe Mental Health NationalService FrameworkOn the demand side, we canidentify the requirements ofnational mental heath policy for thedevelopment of responsive,effective and comprehensiveservices to people with mental illhealth and their carers, as set outin the Mental Health NationalServices Framework. Standards 4and 5 of the Mental Health NSF aredirectly applicable to thedevelopment of personality disorderservices. The publication of theNIMHE guidance was expresslydesigned to assist local services ininterpreting and applying thesestandards to this neglected andmarginalised area.
See:www.doh.gov.uk/nsf/mentalhealth.htm
Reform of Mental HealthlegislationIt is proposed that there will be anew Mental Health Bill in the nearfuture which will propose a broad,generic and inclusive definition ofmental disorder. It is likely that thisnew legislative context willhighlight the need for newcommunity and in-patient servicesfor people with personalitydisorder.
See: www.doh.gov.uk/mentalhealth forfurther information
Developments in Mental HealthcommissioningAdditionally there are a range ofdemands arising from changingcommissioning behaviour by PCTs,which will increasingly want toensure that both service andtraining delivery supportsmodernisation goals and targets.
Further detailed Information aboutmental health modernisation can beobtained at: www.nimhe.org.uk and at:www.doh.gov.uk/mentalhealth/atozpubs
NHS Workforce ModernisationMore broadly the recent publicationof HR in the NHS, the humanresource strategy for the NHSmakes clear that in future jobs willbe evaluated according to the skills,knowledge, responsibilities andqualifications they require ratherthan traditional ‘titles’.13 Payprogression will take place at aseries of ‘gateways’ linked to thedemonstration of appliedknowledge and skills followingassessment through theestablishment of a personaldevelopment plan for each staff member.
See: www.doh.gov.uk/hrinthenhsplanfor further information
The NHS Knowledge and SkillsFrameworkThe NHS Knowledge and SkillsFramework (KSF), will help staffdevelop their capabilities to the fullin a particular NHS post. It will helpto ensure better links betweeneducation, development and careerand pay progression. It has stronglinks with a number of other skills-based initiatives such as theLifelong Learning Framework inEngland14 and it will be important
in supporting the NHS Plan goal ofdeveloping a workforce focused onpatient care and serviceimprovements. It has particularrelevance to the development of aworkforce, which has the rightcapabilities to implement NationalService Frameworks. The KSF willnot replicate existing work, forexample on national occupationalstandards, but rather will provide acommon framework, which unitesexisting initiatives with localstandards in a way that supportsthe consistent development andappraisal of staff as they movearound the service. The KSF, it issuggested, is ‘A common way ofdescribing applied knowledge andskills that could be used for anypost in the NHS and givesemployers and staff a commoncurrency for use in recruitment anddevelopment’.15 The linkagebetween lifelong learning, the KSFand service modernisation will besupported increasingly by the NHSUniversity (NHSU) which will befully established in 2003.
See:www.doh.gov.uk/thenhsksf/kssummaryfor further information
The national policy context willdrive the development of newcareer pathways where certainkinds of aptitudes and emotionalcharacteristics may be as or moreimportant than formal professionalqualifications and wherecompetency involves theappropriate blending ofknowledge, skills and attitudeswithin specific service contexts.
Supply factorsRecruitment and retentionOn the supply side, there are manyworkforce-related challengesrelated to mental healthmodernisation. There are criticalstaff-shortages across a range ofroles and functions within servicesfrom top to bottom and skills andpractices have not kept up with thepace of change in both clinical andnon-clinical areas. There are likelyto be particular challenges inrecruiting and retaining staff towork directly within personalitydisorder services without theincentives of training and careerprogression. There is increasingrecognition that career pathwaysneed to be opened up to enablethose from non-standardbackgrounds to work competentlywithin services and to haveopportunities to progress withintheir careers at their own pace.
The proposal to define and developthe new role of Support, TimeRecovery workers, to work withservice users as part of the mentalhealth team is an example ofmental health workforcemodernisation.
For further information aboutmental health workforcemodernisation see:www.doh.gov.uk/cgwt/mhbackground.htm
Inconsistent servicesThere is significant disparity in theavailability of services for peoplewith personality disorder. As theNIMHE guidance makes clear only17% of mental health trustsprovide a dedicated servicecurrently and within the rest, thereis very variable provision. Moreoversuch services as exist arecharacterised by a disparity oftherapeutic approaches and servicedelivery models. As a consequence,people with PD are forced to seekhelp on the margins of existingservices – through emergencydepartments, through inappropriateadmission to in-patient wards, onthe caseloads of CMHT staff, inprimary care or through other self-access services. This is no longertenable. If the NIMHE guidance isto be implemented and standardsare to be achieved in a uniformway across the country thedevelopment of a local strategicapproach to service development is essential.
Inadequate pre- and postqualification trainingRecent research suggests that pre-registration and pre-qualificationtraining, for most mental healthdisciplines, generally provides littlespecific content that would enabletrainees to understand and feelconfident to assess or managepersonality disorder, although thosewho are interested in this area ofwork can sometimes seek outtraining attachments that mayaddress this gap. This is also true ofthe courses chosen for thepurposes of continuing professionaldevelopment (CPD).
13
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
16
3
14
15
PRE-EMPLOYMENT EMPLOYMENT
Awareness of opportunities
Vocational skills and pre-vocational skillsand basic skills/English
Job application skills
Vocational qualifications (NVQs and NHS individual Learning Accounts)Frontline/Foundation Capabilities
Professional qualificationsFrontline and Foundation/Treatment and Support Capabilities
Continual professional developmentTreatment and Support/Team and Services Management Capabilities
19
North East London WorkforceDevelopment Confederation.(November 2001) TheWorkforce Planning &Education Strategy.
NOTES
The Personality Disorder Career/Skill Escalator Who is the Framework for?
SECTION THREETHE BROADER POLICY CONTEXT
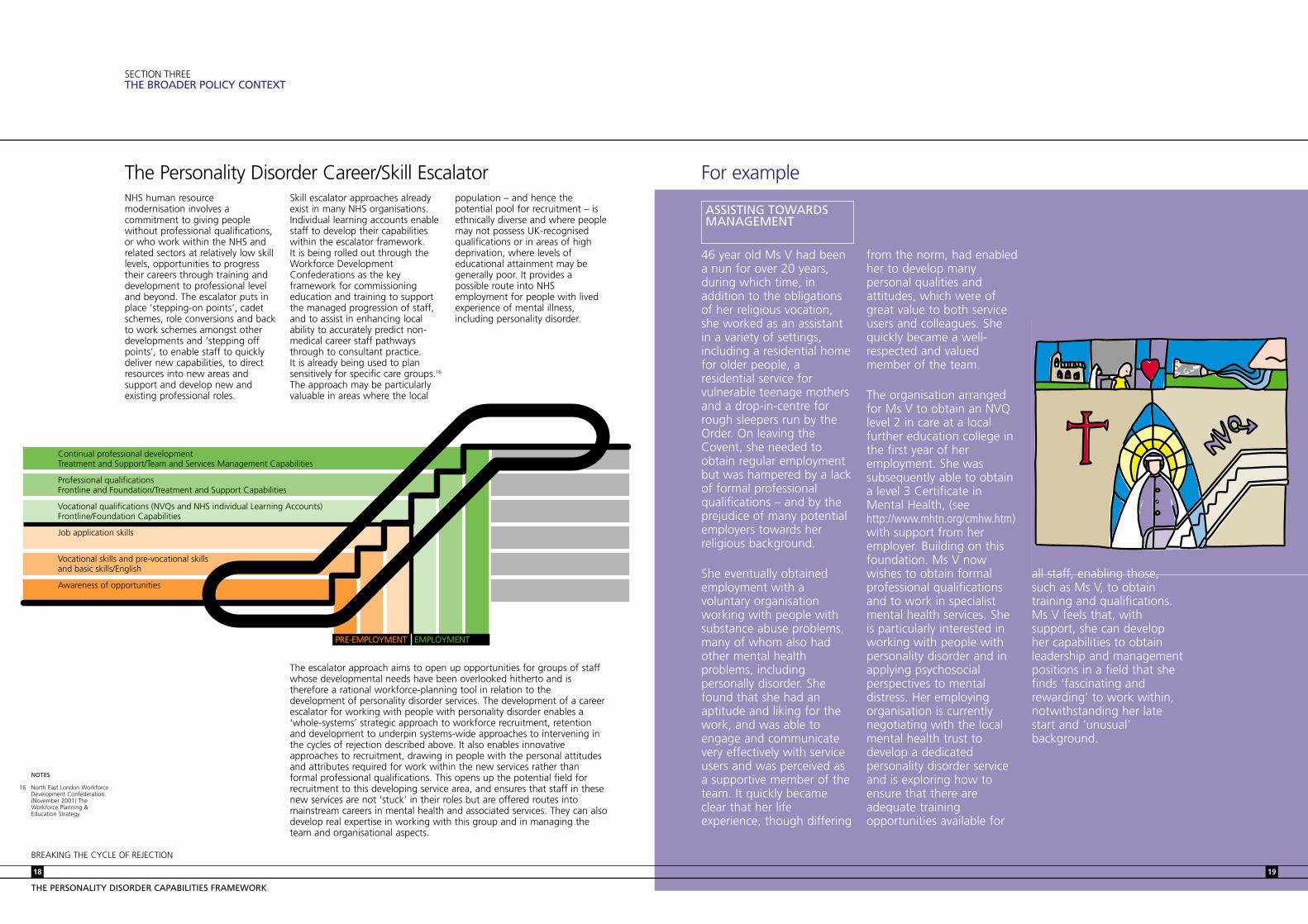
NHS human resourcemodernisation involves acommitment to giving peoplewithout professional qualifications,or who work within the NHS andrelated sectors at relatively low skilllevels, opportunities to progresstheir careers through training anddevelopment to professional leveland beyond. The escalator puts inplace ‘stepping-on points’, cadetschemes, role conversions and backto work schemes amongst otherdevelopments and ‘stepping offpoints’, to enable staff to quicklydeliver new capabilities, to directresources into new areas andsupport and develop new andexisting professional roles.
Skill escalator approaches alreadyexist in many NHS organisations.Individual learning accounts enablestaff to develop their capabilitieswithin the escalator framework. It is being rolled out through theWorkforce DevelopmentConfederations as the keyframework for commissioningeducation and training to supportthe managed progression of staff,and to assist in enhancing localability to accurately predict non-medical career staff pathwaysthrough to consultant practice. It is already being used to plansensitively for specific care groups.16
The approach may be particularlyvaluable in areas where the local
population – and hence thepotential pool for recruitment – isethnically diverse and where peoplemay not possess UK-recognisedqualifications or in areas of highdeprivation, where levels ofeducational attainment may begenerally poor. It provides apossible route into NHSemployment for people with livedexperience of mental illness,including personality disorder.
The escalator approach aims to open up opportunities for groups of staffwhose developmental needs have been overlooked hitherto and istherefore a rational workforce-planning tool in relation to thedevelopment of personality disorder services. The development of a careerescalator for working with people with personality disorder enables a‘whole-systems’ strategic approach to workforce recruitment, retentionand development to underpin systems-wide approaches to intervening inthe cycles of rejection described above. It also enables innovativeapproaches to recruitment, drawing in people with the personal attitudesand attributes required for work within the new services rather thanformal professional qualifications. This opens up the potential field forrecruitment to this developing service area, and ensures that staff in thesenew services are not ‘stuck’ in their roles but are offered routes intomainstream careers in mental health and associated services. They can alsodevelop real expertise in working with this group and in managing theteam and organisational aspects.
16
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
18
For example
46 year old Ms V had beena nun for over 20 years,during which time, inaddition to the obligationsof her religious vocation,she worked as an assistantin a variety of settings,including a residential homefor older people, aresidential service forvulnerable teenage mothersand a drop-in-centre forrough sleepers run by theOrder. On leaving theCovent, she needed toobtain regular employmentbut was hampered by a lackof formal professionalqualifications – and by theprejudice of many potentialemployers towards herreligious background.
She eventually obtainedemployment with avoluntary organisationworking with people withsubstance abuse problems,many of whom also hadother mental healthproblems, includingpersonally disorder. Shefound that she had anaptitude and liking for thework, and was able toengage and communicatevery effectively with serviceusers and was perceived asa supportive member of theteam. It quickly becameclear that her lifeexperience, though differing
ASSISTING TOWARDSMANAGEMENT
from the norm, had enabledher to develop manypersonal qualities andattitudes, which were ofgreat value to both serviceusers and colleagues. Shequickly became a well-respected and valuedmember of the team.
The organisation arrangedfor Ms V to obtain an NVQlevel 2 in care at a localfurther education college inthe first year of heremployment. She wassubsequently able to obtaina level 3 Certificate inMental Health, (seehttp://www.mhtn.org/cmhw.htm)with support from heremployer. Building on thisfoundation. Ms V nowwishes to obtain formalprofessional qualificationsand to work in specialistmental health services. Sheis particularly interested inworking with people withpersonality disorder and inapplying psychosocialperspectives to mentaldistress. Her employingorganisation is currentlynegotiating with the localmental health trust todevelop a dedicatedpersonality disorder serviceand is exploring how toensure that there areadequate trainingopportunities available for
all staff, enabling those,such as Ms V, to obtaintraining and qualifications.Ms V feels that, withsupport, she can developher capabilities to obtainleadership and managementpositions in a field that shefinds ‘fascinating andrewarding’ to work within,notwithstanding her latestart and ‘unusual’background.
BREAKING THE CYCLE OF REJECTION
21
Endnote
SECTION THREETHE BROADER POLICY CONTEXT
The NIMHE guidance acknowledgesthat there is a need to develop theskills and capacity of staff if astrategic approach to servicedevelopment is to be successfullyimplemented. The CapabilitiesFramework set out in thisdocument will underpin newtraining initiatives for staff acrossthe wide range of specialist andnon-specialist agencies that workwith people with PD. Theframework also addresses thetraining needs of whole teams andorganisations with specificreference to the management andleadership requirements that are ata premium in personality disorderservices.
As this framework is implemented,in time, local service systems willsupport staff in various agencies indeveloping capabilities inidentification, referral, assessment,treatment and care at appropriatelevels. Staff will use thesecapabilities within a broad range of
local services which support thepathways of people with apersonality diagnosis, and whichaim towards recovery.
Staff can expect to develop thesecapabilities through innovative,multi disciplinary training courses,at appropriate levels for their jobroles, which are linked to careerskills escalator approaches and life-long learning frameworks. Staffshould be able to progress alongthe personality disorder skillsescalator to achieve senior clinicaland/or managerial positions withinthe web of new services that willemerge in the next few years, asthe NIMHE guidance is fullyimplemented. New local trainingprogrammes will ensure thatpeople with the right attitudes,values and life experiences to workeffectively with people withpersonality disorder are alsoprovided with the necessary skillsand knowledge. These trainingprogrammes, or components ofthem, should be embedded fullywithin local education and trainingprogrammes at all levels.
Service users have most to gainfrom the implementation of thisFramework. Staff with greaterawareness of personality disorderand the capabilities to identify,refer, support and treat in inclusiveand non judgmental ways are thekey to better outcomes for peoplewith personality disorder. Thisframework identifies an approach,which can ensure that the verybroad range of staff potentiallyinvolved in this are enabled todevelop these capabilities.
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
20
BREAKING THE CYCLE OF REJECTION

23
The underlying principles
SECTION FOUR
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
The Personality Disorder Capabilities Framework outlined below reflects thefollowing principles as distilled from the NIMHE guidance and theaccompanying technical papers and the comments of the working groupand service users and other informants:
� Training should be based on respect for the human rights ofservice users and their carers
� Training programmes should consider how best to reflect theviews and experiences service users and carers
� Training should be aimed at breaking the cycle of rejection at alllevels including self-rejection, the social support system,practitioners and the wider health and social care systems
� Training should encourage patient/client autonomy and thedevelopment of individual responsibility
� Training should be multi agency and multi-sectoral� Training should support team and organisational capacity as well
as that of individual practitioners� Training programmes should be connected to meaningful life long
learning and skill escalator programmes� Training should be based on promoting learning in approaches to
treatment and care that are supported by research evidence,where it exists.
Examples
Using the FrameworkAgencies or partnerships wishing to develop training programmes for staffwill be able to use it as a guideline to identify which groups of staff requiretraining to support the user pathway at identified points and then select fromthe list of capabilities those to be addressed within training programmes.
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
22
4
PALS Service Vocationalqualifications
Accessingappropriate andtimely help
Primarily fromPromoting SocialFunctioning domain
Primary CareTeamProfessionals
Professional andCPD
Accessingappropriate andtimely help
Receiving co-ordinated andeffective help andsupport
Moving on fromintensive treatmentand supportingimproved coping
Selection from allCapability domains
For exampleSTAFF GROUP/SERVICE CAREER/TRAINING STAGE IMPACTS ON USER PATHWAY CAPABILITIES REQUIRED
The FrameworkThe Framework itself is presenteddiagrammatically here.
CAREER/TRAINING STAGE
KNOWLEDGE AND CAPABILITY
Pre-
employment
Vocational
Continued
professional
development
Professional
SERVICE TASK AREA
Management and leadership
Assessin
g and managing risk to
self a
nd others
Improving psychological well-b
eing
Promoting social fu
nctioning and obtaining social su
pport
Getting
access
to help
Receiving
help and
support
Moving on
USER PATHWAY
REQUIRED CAPABILITY
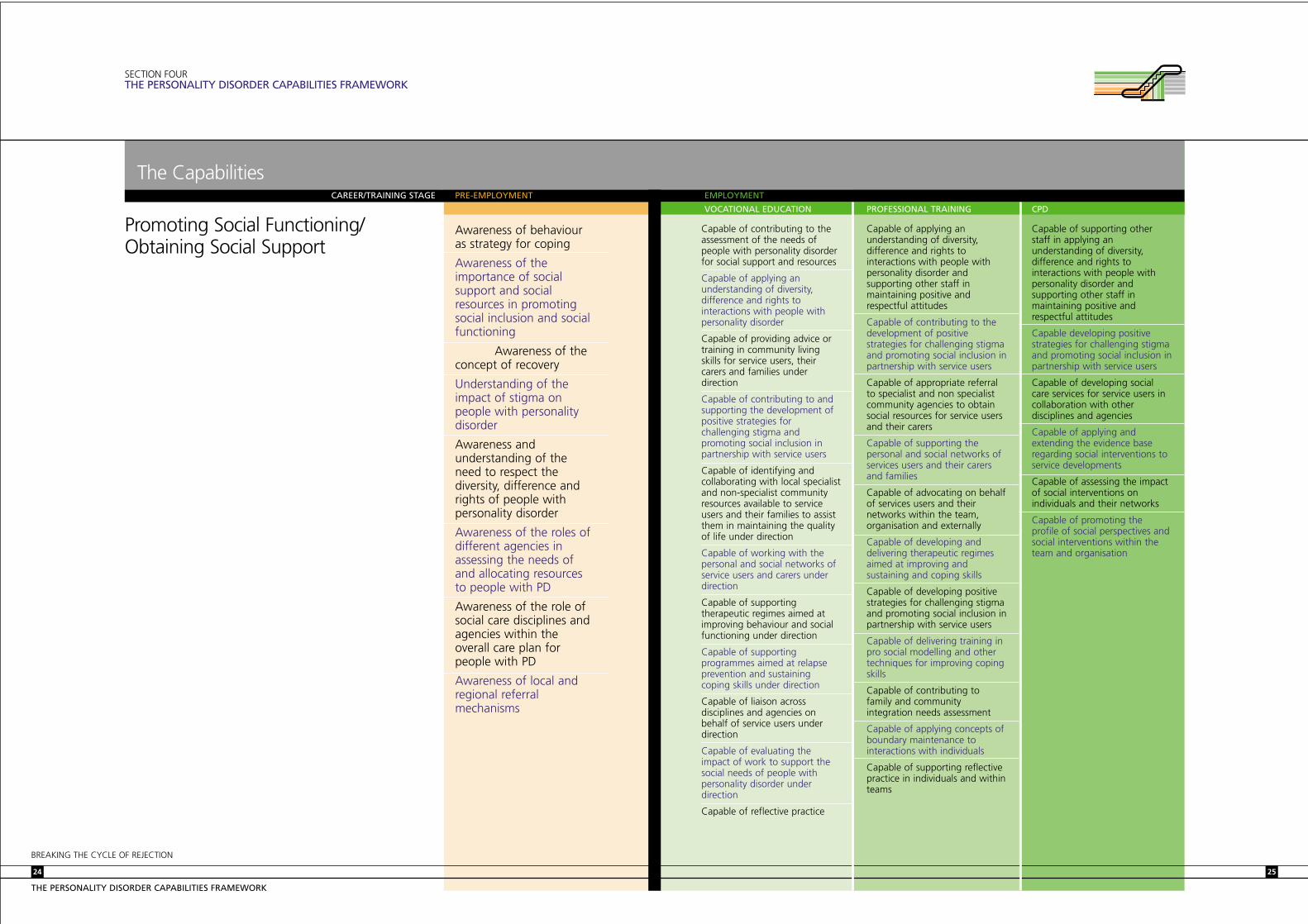
Capable of contributing to theassessment of the needs ofpeople with personality disorderfor social support and resources
Capable of applying anunderstanding of diversity,difference and rights tointeractions with people withpersonality disorder
Capable of providing advice ortraining in community livingskills for service users, theircarers and families underdirection
Capable of contributing to andsupporting the development ofpositive strategies forchallenging stigma andpromoting social inclusion inpartnership with service users
Capable of identifying andcollaborating with local specialistand non-specialist communityresources available to serviceusers and their families to assistthem in maintaining the qualityof life under direction
Capable of working with thepersonal and social networks ofservice users and carers underdirection
Capable of supportingtherapeutic regimes aimed atimproving behaviour and socialfunctioning under direction
Capable of supportingprogrammes aimed at relapseprevention and sustainingcoping skills under direction
Capable of liaison acrossdisciplines and agencies onbehalf of service users underdirection
Capable of evaluating theimpact of work to support thesocial needs of people withpersonality disorder underdirection
Capable of reflective practice
Capable of applying anunderstanding of diversity,difference and rights tointeractions with people withpersonality disorder andsupporting other staff inmaintaining positive andrespectful attitudes
Capable of contributing to thedevelopment of positivestrategies for challenging stigmaand promoting social inclusion inpartnership with service users
Capable of appropriate referralto specialist and non specialistcommunity agencies to obtainsocial resources for service usersand their carers
Capable of supporting thepersonal and social networks ofservices users and their carersand families
Capable of advocating on behalfof services users and theirnetworks within the team,organisation and externally
Capable of developing anddelivering therapeutic regimesaimed at improving andsustaining and coping skills
Capable of developing positivestrategies for challenging stigmaand promoting social inclusion inpartnership with service users
Capable of delivering training inpro social modelling and othertechniques for improving copingskills
Capable of contributing tofamily and communityintegration needs assessment
Capable of applying concepts ofboundary maintenance tointeractions with individuals
Capable of supporting reflectivepractice in individuals and withinteams
Capable of supporting otherstaff in applying anunderstanding of diversity,difference and rights tointeractions with people withpersonality disorder andsupporting other staff inmaintaining positive andrespectful attitudes
Capable developing positivestrategies for challenging stigmaand promoting social inclusion inpartnership with service users
Capable of developing socialcare services for service users incollaboration with otherdisciplines and agencies
Capable of applying andextending the evidence baseregarding social interventions toservice developments
Capable of assessing the impactof social interventions onindividuals and their networks
Capable of promoting theprofile of social perspectives andsocial interventions within theteam and organisation
25
SECTION FOURTHE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
Promoting Social Functioning/Obtaining Social Support
Awareness of behaviouras strategy for coping
Awareness of theimportance of socialsupport and socialresources in promotingsocial inclusion and socialfunctioning
Awareness of theconcept of recovery
Understanding of theimpact of stigma onpeople with personalitydisorder
Awareness andunderstanding of theneed to respect thediversity, difference andrights of people withpersonality disorder
Awareness of the roles ofdifferent agencies inassessing the needs ofand allocating resourcesto people with PD
Awareness of the role ofsocial care disciplines andagencies within theoverall care plan forpeople with PD
Awareness of local andregional referralmechanisms
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
24
The CapabilitiesCAREER/TRAINING STAGE PRE-EMPLOYMENT
VOCATIONAL EDUCATION PROFESSIONAL TRAINING CPD
EMPLOYMENT

Capable of applying a criticalunderstanding of the naturalhistory of personality disordersto interactions with people withpersonality disorder
Capable of establishing andmaintaining long termtherapeutic relationships withservice users under direction
Capable of providing advice ortraining in community livingskills for service users, theircarers and families underdirection
Capable of understanding andapplying the classifications ofpersonality disorders underdirection
Capable of applying theoreticalperspectives to the treatment ofpersonality disorder underdirection
Capable of supportingpsychological treatment regimesunder direction
Capable of contributing to theassessment of co-morbid factors
Capable of contributing to thedelivery of a range ofpsychological interventionsunder direction
Capable of collaborating withmulti-disciplinary colleagues andservices
Capable of working accountablywithin teams and organisationsand awareness of the impact onteams of working with peoplewith personality disorders
Capable of reflective practice
Capable of applying a criticalunderstanding of theories ofpersonality disorder: subjectivity,symptoms and social function,reliability and validity
Capable of the clinicalassessment of personalitydisorder and other mental healthneeds using standardisedinstruments and contributing tothe formulation of treatmentand care plans
Capable of applying caseformulation based on a range ofevidence based models
Capable of establishing andmaintaining long termtherapeutic relationships withservice users and supportingother staff in maintainingtherapeutic relationships
Capable of applying awarenessof clinical significance andtreatment methods appropriatefor various categories of PD
Capable of assessing co-morbidfactors
Capable of planning andapplying a range of evidence-based psychologicalinterventions
Capable of collaborating withmulti-disciplinary colleagues andservices
Capable of tolerating frustrationand anxiety
Capable of working accountablywithin teams and organisationsand awareness of the impact onteams of working with peoplewith personality disorders
Capable of supporting reflectivepractice in individuals and withinteams
Capable of extending theevidence base in relation topsychological treatments forvarious categories of PD
Capable of evaluating theimpact of psychologicaltreatments on individuals,groups and services
27
SECTION FOURTHE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
Improving psychologicalwell-being
Awareness of theoriesregarding the causation ofpersonality disorder
Framework forunderstanding personalitydisorder within thenational policy context
Awareness of treatmentoptions
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
26
The CapabilitiesCAREER/TRAINING STAGE PRE-EMPLOYMENT
VOCATIONAL EDUCATION PROFESSIONAL TRAINING CPD
EMPLOYMENT

29
SECTION FOURTHE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
Assessing and managingrisk to self and others
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
28
The CapabilitiesCAREER/TRAINING STAGE PRE-EMPLOYMENT
VOCATIONAL EDUCATION PROFESSIONAL TRAINING CPD
EMPLOYMENT
Awareness of risk to theindividual and to others inthe context of personalitydisorder
Awareness of riskassessment and riskmanagementmethodologies
Awareness of riskto self and others fromoffending behaviour
Awareness of localpolicies and procedures
Capable of applying a criticalunderstanding of risk ininteractions with individuals
Capable of applying riskassessment and riskmanagement strategies underdirection
Capable of contributing toactuarial and dynamic riskassessment strategies, payingattention to the risk ofoffending or of harm to self orothers, under direction
Capable of monitoring signs ofrelapse and taking appropriateaction under direction
Capable of undertaking actuarialrisk assessment paying attentionto the risk of offending and ofharm to self or others
Capable of undertaking adynamic risk needs assessmentpaying particular attention tocognitive and inter-personalfactors, substance abuse and lifestyle indicators
Capable of understanding andsupporting criminogenic needsassessment paying particularattention to cognitive and inter-personal factors, substanceabuse and life style indicatorsunder direction under direction
Capable of undertaking a familyand community risk needsassessment
Capable of planning anddelivering interventions based oncase formulation addressingspecific risk factors, providingproposals for risk managementand for motivating individuals
Capable of applying anunderstanding of legal andethical issues in the context ofrisk assessment andmanagement
Capable of collaborating withmulti-disciplinary and multi-sectoral risk management plans
Capable of reflective practice
Capable of developing systemsof risk management based oncurrent evidence
Capable of evaluating riskmanagement strategies onindividuals, groups, teams andorganisations
Capable of providing leadershipfor programmes aimed attackling offending behaviour
Capable of extending theevidence base regarding theimpact of offender behaviourprogrammes in relation to PD
Capable of evaluating theimpact of offender behaviourprogrammes on individuals,groups, teams and organisations

Capable of critical and reflectivepractice in the delivery andmanagement of value-basedservices to individuals with PD
Capable of recognisinglimitations and the need to seeksupport, supervision or theinvolvement of other agencies
Capable of bearing hostility andaggression without retaliation
Capable of managing self andothers in the context of nationaland local policies in relation to PD
Capable of applying a criticalunderstanding of theimportance of management andleadership in supporting teamand organisational functioningin relation to PD
Capable of applying a critical understanding ofcontemporary theories ofleadership and management at an appropriate level
Capable of working acrosstraditional service boundaries toinclude a wider systemic andmulti-agency approach toensuring seamless and effectivecare is provided
Capable of reflecting on ownand others’ reactions to clients and offering a considered response
Capable of bearing hostility andaggression without retaliation
Capable of using and offeringsupport and supervision
Capable of maintaining clearpersonal and professionalboundaries
Capable of managing self andothers in the context of nationaland local policies in relation to PD
Capable of providingprofessional supervision toindividuals and teams
Capable of providing leadershipand support to non-specialiststaff and services
Capable of applying a criticalunderstanding of theimportance of management andleadership in supporting teamand organisational functioningin relation to PD
Capable of contributing toorganisational change: positivepartnerships with users and carers,promoting strategies for socialinclusion, challenging stigma
Capable of working acrosstraditional service boundaries toinclude a wider systemic and multi-agency collaborative approachto ensuring that seamless andeffective care is provided
Capable of applying a criticalunderstanding of underlyingprinciples, main frameworks andtheories of effective leadershipand management of change
Capable of applying theseprinciples and frameworks topractice, to include effectivecommunication, influencing,negotiating, coaching andconflict resolution
Capable of applying knowledgeof the underlying principles ofmotivation theories and theirapplication in motivating andinspiring teams and individuals
Capable of appraising relevantinternal and external factors thatmight influence the way inwhich PD services operate
Capable of identifying, analysingand evaluating strategies toimprove the effectiveness ofmulti disciplinary team working
Capable of translating policyinto practice within the teamand organisation
Capable of developing a positivenetworking culture andstrategies for sharing goodpractice in developing services topeople with PD
Capable of developing andmaintaining cultures andstrategies which are positive inrelation to PD
Capable of leading andsustaining innovations in servicemodels and treatment optionsfor people with PD
Capable of providing clinicalleadership and supervision toteams and organisations
Capable of leading programmesof career development within PDservices
31
SECTION FOURTHE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
Management and leadership
Awareness of of the rolesof managers and leaderswithin personality disorderservices
Awareness of theimportance of selfmanagement ininteractions with serviceusers, colleagues and thewider organisation
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
30
The CapabilitiesCAREER/TRAINING STAGE PRE-EMPLOYMENT
VOCATIONAL EDUCATION PROFESSIONAL TRAINING CPD
EMPLOYMENT

33
Who is the Framework for?
APPENDIX I
ACKNOWLEDGEMENTS
Particular thanks are due to DrSteve Miller at the South WestLondon and St George’s NHSMental Health Trust who shareduseful insights from his work withservice users on a user-orientatedtraining programme, to ProfessorBrian Thomas Peter of theBirmingham and Solihull MentalHealth Trust for his generouscontribution of ideas and graphicsand to Dr Rex Haigh forcontributing ideas on servicemodels and for facilitating thecontribution of service users to this work.
Revolving Doors provided very usefulmaterial on user pathways and ontraining programme content.
Maria Duggan developed andwrote the Framework on behalf of NIMHE.
Design and illustration byFoundation design consultancy:www.foundationdesign.co.uk
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
32
Ms Mary-Anne Ambrose Colchester
Ms Yolande Hadden Berkshire
Ms Sheena Money Berkshire
Ms Donna Smart West Midlands
Ms Jayne Treby Jersey
Ms Nikki Tysoe Berkshire
SERVICE USER FOCUS GROUP
Mr Ian Baguley National Programme ManagerMental Health Workforce Development
Ms Heather Castillo Advocacy Services ManagerNorth Essex Mental Health Partnership Trust
Mr Tony Butterworth Chief ExecutiveTrent Workforce Development Confederation
Ms. Jackie Craissati Head of Forensic Clinical Psychology ServicesThe Bracton Centre
Ms Maria Duggan Independent Consultant
Dr. Rex Haigh Consultant PsychotherapistWinterbourne House
Ms Roslyn Hope Director of National Workforce Development Programme
Professor Eddie Kane Senior Adviser on Mental Health and High Secure ServicesDepartment of Health
Ms Mhairi Macpherson Director of ModernisationEast London & The City Mental Health NHS Trust
Dr Gill McGauley Consultant Forensic PsychotherapisBroadmoor Hospital
Dr Kingsley Norton DirectorThe Henderson Hospital
Ms Laura Roberts Chief ExecutiveNorth Manchester PCT
Dr Anthony Roth Joint Course Director, and Chartered Clinical PsychologistDepartment of Clinical Psychology, UCL
Dr Pete Snowden Consultant Forensic PsychiatristAshworth Hospital
Professor Brian Thomas Peter Director of Psychological ServicesThe Raeside Clinic
Ms Deirdre Vereker Training Co-ordinatorTurning Point
MEMBERSHIP OF THEEXPERT GROUP

NIMHE Development Centres
APPENDIX II
CONTACT DETAILS
EasternNIMHE Eastern Development Centre654 The CrescentColchester Business ParkColchesterEssex CO4 9YQTel: 01206 287 583EMail: [email protected]
East MidlandsNIMHE East Midlands Development CentrePleasley Vale Business ParkOutgang LanePleasleyMansfieldNotts NG19 8RLTel: 01623 819370EMail: [email protected]
LondonNIMHE London Development Centre11-13 Cavendish SquareLondon W1G 0ANTel: 020 7307 2433EMail: [email protected]
North East Yorks and HumbersideNIMHE North East, Yorkshire and HumbersideDevelopment CentreBlenheim HouseWest OneDuncombe StreetLeeds LS1 4PLTel: 0113 253 3821EMail: [email protected]
North WestNIMHE North West Development CentreHyde HospitalGrange Road SouthHyde SK14 5NYTel: 0161 351 4920EMail: [email protected]
South EastNIMHE South East Development CentreParklands HospitalAldermaston RoadBasingstokeHampshire RG24 9RHTel: 01256 376 394EMail: [email protected]
South WestNIMHE South West Development Centre2 Tower LaneTower StreetTauntonSomerset TA1 4ARTel: 01823 337879EMail: [email protected]
West MidlandsNIMHE West Midlands Development CentreOsprey HouseAlbert StreetRedditchWorcestershire B97 4DETel: 01527 587 620EMail: [email protected]
Department of Health leads
Nick BenefieldSecure Commissioning TeamSefton Health AuthorityBurlington HouseCrosby Road NorthLiverpool L22 0QBTel: 0151 478 1804Email: [email protected]
Prof. Eddie KaneGONWSunley TowerRoom 1809Piccadilly PlazaManchester M1 4BETel: 0161 952 4294Email: [email protected]
Dr Pete SnowdenClinical DirectorAshworth HospitalParkbournMaghullLiverpool L31 1HWTel: 0151 472 4501Email: [email protected]
and also [email protected]
BREAKING THE CYCLE OF REJECTION
THE PERSONALITY DISORDER CAPABILITIES FRAMEWORK
34


















