Bovine and human NPH insulins as T cell immunogens
8
Diabetes Research and Clinical Practice, 20 (1993) 139- 146 0 1993 Elsevier Scientific Publishers Ireland Ltd. All rights reserved. 016%8227/93/$06.00 139 DIABET 00730 Bovine and human NPH insulins as T cell immunogens Robert Gregorya, and Robert B. Tattersallb ‘Department of Immunology and ‘Diabetes Unit, University Hospital, Queen’s Medical Centre, Nottingham. UK (Received 10 December 1992; revision accepted 29 December 1992) Summary The aim of this study was to assess the immunocompetence of T cells from patients with poorly controll- ed diabetes with respect to Candida albicans antigen and to compare the relative immunogenicity of human insulin, bovine insulin and protamine at the T-cell level during 6 months treatment with human or bovine NPH insulins. T-cell proliferation was measured in vitro in response to C. albicans, bovine and human in- sulin, bovine and human NPH and protamine in 17 patients with newly-diagnosed type 1 (insulin- dependent) and 12 with poorly-controlled type 2 (non-insulin-dependent diabetes) before and after 0.5, 1, 3 and 6 months of treatment with either bovine or human NPH insulin. The following results were found: Baseline responses to C. albicans (as a recall antigen) were similar for patients and controls despite marked hyperglycaemia in the patients. No patient had a response greater than mean + 2 S.D. of controls to human or bovine insulin before starting treatment, or had insulin autoantibodies. Treatment with human NPH insulin did not induce T-cell responses to human or bovine insulin, but 3113 (23%) patients treated with bovine NPH responded to bovine and human insulin after 6 months, of whom one responded exclusively to human. In contrast, 6 (46%) bovine and 3 (19%) human NPH-treated patients responded to protamine. It was concluded that there is no evidence of T-cell immunosuppression in poorly-controlled diabetes or of T-cell autoimmunity to insulin in newly-diagnosed type 1 diabetes. Treatment with bovine NPH insulin immunizes T cells to insulin, but human NPH does not. Regardless of insulin species the main immunogen in NPH insulins is protamine. Key words: T cells; NPH insulin; Bovine insulin; Human insulin Introduction The function of T lymphocytes in patients start- ing insulin therapy is of interest for several reasons: firstly, T cells regulate the antibody re- sponse and, as injected insulin is immunogenic [1,2], it should be possible to detect T cells which recognise one or more components of exogenous insulin. Secondly, it is thought that uncontrolled Correspondence to: Dr. R. Gregory, Department of Diabetes & Endocrinology, Clinic 12, Addenbrooke’s Hospital, Hills Road, Cambridge CB2 ZQQ, UK. diabetes is a state of acquired immunosuppression predisposing to infections, including those due to Candida albicans [3]. Finally, T cells are involved
-
Upload
robert-gregory -
Category
Documents
-
view
212 -
download
0
Transcript of Bovine and human NPH insulins as T cell immunogens

Diabetes Research and Clinical Practice, 20 (1993) 139- 146
0 1993 Elsevier Scientific Publishers Ireland Ltd. All rights reserved. 016%8227/93/$06.00 139
DIABET 00730
Bovine and human NPH insulins as T cell immunogens
Robert Gregorya, and Robert B. Tattersallb
‘Department of Immunology and ‘Diabetes Unit, University Hospital, Queen’s Medical Centre, Nottingham. UK
(Received 10 December 1992; revision accepted 29 December 1992)
Summary
The aim of this study was to assess the immunocompetence of T cells from patients with poorly controll- ed diabetes with respect to Candida albicans antigen and to compare the relative immunogenicity of human insulin, bovine insulin and protamine at the T-cell level during 6 months treatment with human or bovine NPH insulins. T-cell proliferation was measured in vitro in response to C. albicans, bovine and human in- sulin, bovine and human NPH and protamine in 17 patients with newly-diagnosed type 1 (insulin- dependent) and 12 with poorly-controlled type 2 (non-insulin-dependent diabetes) before and after 0.5, 1, 3 and 6 months of treatment with either bovine or human NPH insulin. The following results were found: Baseline responses to C. albicans (as a recall antigen) were similar for patients and controls despite marked hyperglycaemia in the patients. No patient had a response greater than mean + 2 S.D. of controls to human or bovine insulin before starting treatment, or had insulin autoantibodies. Treatment with human NPH insulin did not induce T-cell responses to human or bovine insulin, but 3113 (23%) patients treated with bovine NPH responded to bovine and human insulin after 6 months, of whom one responded exclusively to human. In contrast, 6 (46%) bovine and 3 (19%) human NPH-treated patients responded to protamine. It was concluded that there is no evidence of T-cell immunosuppression in poorly-controlled diabetes or of T-cell autoimmunity to insulin in newly-diagnosed type 1 diabetes. Treatment with bovine NPH insulin immunizes T cells to insulin, but human NPH does not. Regardless of insulin species the main immunogen in NPH insulins is protamine.
Key words: T cells; NPH insulin; Bovine insulin; Human insulin
Introduction
The function of T lymphocytes in patients start- ing insulin therapy is of interest for several
reasons: firstly, T cells regulate the antibody re- sponse and, as injected insulin is immunogenic [1,2], it should be possible to detect T cells which recognise one or more components of exogenous insulin. Secondly, it is thought that uncontrolled
Correspondence to: Dr. R. Gregory, Department of Diabetes & Endocrinology, Clinic 12, Addenbrooke’s Hospital, Hills Road, Cambridge CB2 ZQQ, UK.
diabetes is a state of acquired immunosuppression predisposing to infections, including those due to Candida albicans [3]. Finally, T cells are involved

140
in the pathogenesis of type 1 diabetes. Insulin autoantibodies have been reported in 15-20% of newly diagnosed patients [4] and, as insulin is a T- dependent antigen, there should be insulin-specific autoimmune T-cell reactivity in such patients.
Our aim was to assess the immuno-competence of T cells from diabetic patients with substantial hyperglycaemia (newly-diagnosed type 1 and poorly-controlled type 2) in an in vitro lymphocyte proliferation assay using Candida albicans anti- gen, and compare the relative immunogenicity of human and bovine insulin and protamine at the T- cell level during 6 months treatment with bovine or human NPH insulin.
TABLE I
Characteristics of patients randomised to receive human or bovine NPH
Research Design and Methods
Subjects
Twenty-nine consecutive patients starting insulin as outpatients were classified as having either type 1 or type 2 diabetes by National Diabetes Data Group criteria [5], and were ran- domised to receive either twice daily human or purified bovine NPH (isophane) insulin. The characteristics of the groups are shown in Table 1. Ketonuria was defined as >7.8 mmol I-’ (Ketostix, Ames, Slough, UK) Patients were studied before and at 0.5, 1, 3 and 6 months after starting insulin. Age- and sex-matched controls
Human NPH
Type l diabetes
Type 2 diabetes
Bovine NPH
Type l diabetes
Type 2 diabetes
Number
Age (years) median (range)
24 (13-52) 72 (43-82)
Ketonuria > 7.8 mm01 1-l 0
Duration of diabetes for type 2 patients (years) median (range)
Islet cell antibodies (titre z l:4)
HbA, (%) median (range)
Random blood glucose (mm01 1-1) median (range)
HLA-DR phenotype DR3/- DR4/- DR3/4 Other No result
10
-
8 14.8 (9.9-22.8) 24.8 (9.9-35.8)
6
2.5 (I-12)
0
I5 (8.9-21.4) 22.8
(16.2-33.8)
7
28 (20-62)
6a 14.6
(11.3-21.0) 24.6
(12.6-30.7)
6
60 (55-78)
0
4 (0.5-10)
0
14.5 (13.7-16.5) 21.5
(I 3.9-29.8)
a One patient had a high titre of anti-mitochondrial antibodies so that islet cell antibodies could not be measured.

141
were healthy medical, nursing and laboratory staff or hospital voluntary workers without a personal or family history of diabetes.
All subjects gave informed consent and the study was performed in accordance with the prin- ciples of the Declaration of Helsinki.
Lymphocyte proliferation assay Peripheral blood mononuclear cells were
obtained by centrifuging heparinised blood on lymphocyte separation medium (Gibco Ltd., Paisley, Scotland) at 600 x g for 20 min. The cells (86-91% lymphocytes) were washed and resus- pended at 2 x lo9 1-l in RPMI-1640 (Northum- bria Biologicals Ltd., Cramlington, UK) con- taining 200 mmol 1-l L-glutamine, 2.38 g I-’ HEPES, non-essential amino acids, penicillin and streptomycin. This was supplemented with 20% heat inactivated human male AB serum. Aliquots (100 ~1) were cultured in quadruplicate with 100 ~1 of RPM1 (non-stimulated wells) or antigen solution at the appropriate concentration (stimu- lated wells) in round bottomed microtitre plates for 6 days at 37°C in 5% CO*. Cultures were pulsed with 1 $Zi [3H]thymidine (Amersham Radiochemicals Ltd., Aylesbury, UK) for the final 20 h. Plates were harvested semi-automatically and the incorporated radioactivity measured by liquid scintillation.
Results were expressed as incremental counts per minute (A c.p.m.) for each antigen, the differ- ence between the mean c.p.m. for antigen stimu- lated cultures and mean c.p.m. for non-stimulated cultures.
Antigens C. albicans antigen-crude whole cell extract
CAD-l 1 was kindly provided by Professor D.W.R. MacKenzie (PHLS, Mycological Refer- ence Laboratory, Colindale, UK). Single batches of purified bovine NPH (Monophane, The Boots Company PLC, Nottingham, UK) and semi- synthetic human NPH (Human Protaphane emp, Novo Industri A/S, Bagsvaerd, Denmark) were obtained for use by patients and in cultures. Freeze-dried, preservative-free, purified bovine (Monocomponent Bovine, Novo, Copenhagen) and semi-synthetic human insulin (Novo,
Copenhagen) and dried protamine sulphate, (Salmine, Novo, Copenhagen) for use in cultures were stored at -20°C.
Antigen solutions were freshly prepared for each experiment and used at pre-determined opti- mum concentrations for lymphocytes from sub- jects with delayed type hypersensitivity reactions to bovine insulin: insulins 100 and 250 mg l-i, protamine sulphate 50 and 100 mg l-‘, and C. albicans 100 mg 1-l (the standard concentration for lymphocyte stimulation in this laboratory).
Insulin antibodies were measured by fluid-phase radioimmunoassay using semi-synthetic human in- sulin and purified bovine insulin as ligands [6]. Results are expressed as insulin binding in pg 1-l. The normal range for non-diabetic control sub- jects (mean + 3 S.D.) is < 5 pg 1-l.
Haemoglobin Al (HbAl) was measured by mobile affinity electrophoresis [7]. The normal range for the assay is 4.0-7.5”/0. Islet cell anti- bodies were measured with an indirect immuno- fluorescence method which detects total ICA-IgG [8,9]. HLA phenotyping was by standard micro- lymphocytotoxicity methods [lo].
Statistical analysis Baseline lymphocyte proliferation data for all
patients and controls were compared using a Wilcoxon Rank Sum Test for unpaired data, as were comparisons between results for type 1 and type 2 diabetic patients, and between bovine and human NPH recipients. Serial data for patients were compared using the Wilcoxon test for paired data. Serial comparisons of HbA, were by paired t-tests. Two-tailed tests of significance were used in all cases.
Results
C. albicans The results of seven experiments over 9 months
for one control subject were A c.p.m. 6375 f 1896 (mean + S.D.); coefficient of variation 30%. The range for non-stimulated cultures was 277-1000 c.p.m.
There was no difference between the responses of patients and controls at the start of the study

142
TABLE 2
Candida-specific T-cell proliferation before and after insulin therapy
Duration of insulin therapy (months)
0 6 Controls
Type 1 diabetes Proliferation (A c.p.m. x 103) 10.7 zt 8.3 10.4 zt 5.8” 10.9 f 7.4c n = 17 (HbA, o/u) (15.3 l 4.3) (10.2 f 3.2)b
Type 2 diabetes Proliferation (A c.p.m. X 103) 9.1 f 6.4 7.2 f 5.0” 7.4 f 5.2c n = 12 (HbA, %) (IS.2 f 2.9) (10.9 zt 2.7)b
All results shown as m f S.D. a N.S. Wilcoxon test for paired data. b P < 0.001 Paired r-test. c N.S. Wilcoxon test for unpaired data.
and no change during 6 months despite improved blood glucose control (P < 0.001) (Table 2).
Components of NPH insulins A positive response to each antigen was defined
as A c.p.m. greater than the mean f 2 SD. of that
3 DuDration “df’ treatrknt [months)
6 CONTROLS
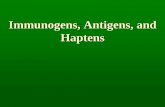
Fig. I. Lymphocyte proliferation to human NPH insulin at 100 mg 1-l. Results for 29 patients and controls. Error bars = mean f S.D. 0, bovine-treated type 1 patients; n , bovine- treated type 2 patients; A, human-treated type I patients; v, human-treated type 2 patients. Hatched area represents a
response to the antigen.
for control subjects. To illustrate this, the results for one antigen, human NPH, are shown in Fig. 1. The definition of response for each antigen is given in Table 3: The P-values in the text refer to results obtained for insulins at 100 mg 1-l and protamine at 50 mg 1-l. Similar results were obtained at the higher concentrations.
There was no difference between the responses
TABLE 3
Definition of T-cell response to each antigen
Antigen (Cont.)
Mean f 2 S.D. c.p.m.
Bovine insulin 100 mgl-’ 250 mg I-’
> 2084 > 2078
Hwnan insulin IO mg I-’ 250 mg I-’
Proramine sulphate 50 mg I-’ 100 mg I-’
Bovine NPH 100 mg I-’ (insulin) 250 mg I-’
Human NPH 100 mg I-’ (insulin) 250 mg I-’
> IO55 > 1766
> 2612 > 3026
>774 > 903
> 633 >889

143
TABLE 4
Proliferation of T cells from 29 diabetic patients to insulin antigens during 6 months of treatment with bovine or human NPH insulins
Antigen Duration of insulin therapy (months)
0 0.5 I 3 6
Bovine insulin solution (100 mg I-‘)
Human insulin solution (100 mg I-‘)
Protamine sulphate (50 mg I-‘)
Bovine NPH (100 mg I-‘)
Human NPH (100 mg I-‘)
132 f 219 (n = 28) 193 f 318 (n = 28) 324 zt 145 (n = 28) -47 f 263 (n = 21) -35 f 167 (n = 27)
313 l 593 (n = 26) 213 f 361 (n = 27) 562 zt 854 (n = 27) 273 zt 94rj6 (n = 27) 31 f 441 (n = 27)
117 f 572 (n = 26) 65 f 411 (n = 27) 653 zt 1062 (n = 27) 273 zt 192c (n = 26) -118 f 661 (n = 28)
269 zt 554 (n = 29) 195 f 325 (n = 29) 1067 zt 1272’ (n = 29) 655 f 830c (n = 29) 238 f 48Sb (n = 29)
437 f 887 (n = 29) 390 f 678 (n = 29) 999 f 1868” (n = 29) 554 f 1030’ (n = 28) 391 f 756’ (n = 28)
Results expressed as mean A c.p.m. f I SD. a,b*CResults differ significantly from pre-treatment values. Wilcoxon paired rank sum test: “P < 0.05; bP < 0.02; ‘P < 0.005
TABLE 5
Patients responding to components of NPH insulins
Type of diabetes
Bovine insulin
Human insulin
Responder to
Protamine Bovine Human NPH NPH
Responders in human NPH group 1 1 I 1 2 I I
++ ++ ++ + ++ + +
++ 4-f ++
+ +
Responders in bovine NPH group 1 ++ ++ ++ ++ i-k 2 ++ + ++ ++ -k-t 2 ++ ++ + i+ i+ 2 ++ + 2 ++ ++ ++ 1 ++ ++ ii 1 + ++ ++ 2 ++ ++ 1 +
++, > mean + 3 SD. of controls; +, > mean + 2 S.D. of controls.

I44
of type 1 and type 2 diabetic patients at any time for any antigen and they have been amalgamated (Table 4). No significant changes were seen in serial responses to bovine or human insulin. Pro- tamine responses were significantly greater after 3 (P < 0.005) and 6 months (P < 0.05) of treatment. A response to bovine NPH was apparent at 2 weeks (P < 0.05) and peaked at 3 months (P < 0.005). The response to human NPH took 3 months to develop (P < 0.02).
Patients who responded to at least one antigen (at either concentration) at any time are shown in Table 5. No patient treated with human NPH responded to human or bovine soluble insulin at any time. In contrast 3 patients treated with bovine NPH responded to both bovine and human insulin, and one responded exclusively to human after 6 months. Nine of 29 (3 1%) patients respond- ed to protamine sulphate alone, of whom 6 had received bovine and 3 human NPH. The NPH insulins elicited more responses in vitro; of 9 patients on bovine, 7 responded to bovine and human NPH, one exclusively to bovine NPH and one to human NPH. Three patients on human NPH responded exclusively to bovine and two more to human NPH.
1’. 1 I I 1 I I I
0 10 20 30 40 50 60 70 80 90
Fig. 2. The lack of correlation between amount of lymphocyte
proliferation to bovine insulin at 100 mg I-’ and insulin anti-
body concentration in 13 bovine NPH-treated patients.
r = 0.20.
Humoral immunity to insulin No patient had a significant concentration of
insulin binding. IgG (> 5.0 mg 1-l human insulin) before starting insulin. After 6 months 12/13 patients on bovine and 6/16 on human NPH (5 with type 1 diabetes) had significant concentra- tions of antibody. As expected, those on bovine NPH made more antibody than the human treated group; median 19.3 pg I-’ (range 3.9-89.0), vs. 3.6 pg 1-j (0.3-6.6). High levels of circulating insulin antibody did not correlate with T-cell responsiveness to insulin (Fig. 2).
Discussion
Using serial lymphocyte proliferation assays in type 1 and type 2 diabetic patients during the first 6 months of insulin therapy, we found no evidence of T-cell immunosuppression in poorly controlled diabetes, or of T-cell autoimmunity to insulin in newly-diagnosed type 1 diabetes. Treatment with bovine NPH immunized 23% of patients to bovine insulin within 6 months, whereas no patient treated with human NPH responded to insulin. Thirty-one percent of patients responded to pro- tamine within 6 months.
It is difficult to compare our results directly with those from earlier studies owing to differences in patient selection, methodology and handling of data; previous workers have maximised their chances of finding responders to insulin by look- ing at patients with insulin allergy, or high levels of circulating insulin antibody. Thus, Mann et al. [l l] claimed that 48% of insulin allergic patients responded to bovine or porcine insulin, but includ- ed no results from control subjects. Kurtz et al. 112) found that 57% of patients with high insulin antibody levels made a T-cell response to insulin, defined as total c.p.m. more than 250 above that of controls. Others using recently diagnosed or longstanding insulin-treated patients found that 25-60% responded to insulin [ 13- 161.
There is disagreement about the optimum dura- tion of cultures and concentration of insulin. Five- or 6-day cultures are usual, but some suggest 9 days [ 151. We chose 6 days because longer cultures led to unacceptably high non-stimulated c.p.m.

145
(> 2500), and lymphocytes from normal subjects often responded at 9 days but not at 6 days, par- ticularly when the insulin concentration was raised to 500 mg 1-l (data not shown).
We found no evidence of T-cell autoimmunity in untreated type 1 diabetic patients, consistent with the absence of insulin antibodies. Scheinin et al. [ 171 reported that lymphocytes from 68% of child- ren responded in vitro to bovine and/or porcine insulin when tested within 2 weeks of diagnosis but only 11% had IgG insulin autoantibodies. The difference between this result and ours may owe as much to the definition of responses than to other differences such as the ages of patients. Scheinin et al. did not define responsiveness as a function of control data, but used a stimulation index > 1.5 as the threshold. Had we used this definition, 8/17 (47%) patients and 8117 controls would have ‘responded’ to bovine or human insulin before starting therapy. We acknowledge that immuno- logical markers of type 1 diabetes including insulin autoantibodies are found more frequently in children.
The lack of detectable T-cell autoimmunity to insulin is not explained by hyperglycaemia. The responses to the third party antigen, C. albicans, were similar for patients and controls despite substantial hyperglycaemia in the patients. This is consistent with the work of Ragab et al. [la] who found no difference between 23 patients with unclassified diabetes and 24 healthy controls. T- cell function might be impaired by poor diabetic control in vivo, with the defect corrected by 6 days in optimal conditions in vitro but, against this, Candida-specific T-cell proliferation is unimpaired by glucose 20 mmol 1-l and /3-hydroxybutyrate 8 mm01 1-l in vitro [ 191.
We confirm the low immunogenicity of human insulin. No patient treated with human NPH had a T-cell response to human insulin after 6 months. The lower incidence of responders to bovine insulin compared with other studies is partly explained by the purity of the insulin ( <40 p.p.m. proinsulin), by a rigorous definition of response and patient selection. We cannot explain why high levels of insulin antibody failed to predict T-cell responsiveness. One possibility is that T cells are primed in vivo not by monomeric insulin, but by
an insulin transformation product present in the vial, such as covalent dimer [20]. Monomeric insulin might be an inadequate stimulus to T cells in vitro. Alternatively, peripheral blood may not contain the insulin-specific T memory cells which are trapped in lymph nodes draining the injection sites where they proliferate and activate insulin- specific B cells, resulting in antibody production. Whatever the explanation, we believe antigen- specific T-cell function is more important than antibody levels as T cells are central to the induc- tion of the immune response.
NPH (isophane) insulins which contain pro- tamine, an immunogenic salmon sperm protein, form more than 70% of most insulin regimens. IgG anti-protamine antibodies were described in 93% of patients treated with bovine NPH for a mean of 20 years, and in 38% of patients treated with highly purified porcine NPH for 1 year [21]. Six of 21 (29%) type 2 diabetic patients treated with porcine NPH insulin for 1 year also produced protamine- specific IgG [22]. In the only report of cellular immunity to protamine, 59% of insulin allergic patients responded to it, usually with stimulation indices greater than those for insulin [l 11.
In general, physicians are satisfied with the pharmacokinetics of NPH insulins and this has perpetuated the continued adulteration of a protein of very low immunogenicity, human insulin, by a fish protein of moderate immuno- genicity. Allergy to protamine probably accounts for most cases of insulin allergy [23], and the clini- cal relevance of this is that some patients previous- ly immunised with NPH have had anaphylactic reactions after intravenous protamine during surgery or cardiac catheterisation [24,25].
We conclude that, regardless of insulin species, the main immunogen in NPH insulins is pro- tamine.
Acknowledgements
We acknowledge support from Gordon Reeves. We thank Ann Douglas for measuring insulin anti- bodies, Keith Gelsthorpe for arranging HLA typing and Joan Bennett and Pat Lister for typing the manuscript. Robert Gregory was supported by

146
a Clinical Research Fellowship from Novo Labo- ratories Ltd., Basingstoke, UK. Preliminary data from this study has been presented in abstract form [26].
References
1
2
3
4
5
6
Reeves, W.G., Barr, D., Douglas, C.A. et al. (1984) Fac- tors governing the human immune response to injected insulin. Diabetologia 26, 266-271, Heding, L.G., Marshall, M.O., Persson, B. et al. (1984) Innnunogenicity of monocomponent human and porcine insulin in newly-diagnosed type 1 (insulin-dependent) diabetic children. Diabetologia 27, 96-98. Raytield, E.J., Ault, M.J., Keosch, G.T., Brothers, M.J., Nechemias, C. and Smith, H. (1982) Infection and diabetes: the case for glucose control. Am. J. Med. 72, 439-450. Palmer, J.P., Asplin, CM., Clemm, P. et al. (1983) Insulin antibodies in insulin-dependent diabetics before insulin treatment. Science 222, 1337-1339. National Diabetes Data Group. (1979) Classification and diagnosis of diabetes mellitus and other categories of glu- cose intolerance. Diabetes 28, 1029-1057. Reeves, W.G. and Kelly, U. (1980) An immunochemical method for the quantification of insulin antibodies. J. bnmunol. Methods 34, 329-338. Ambler, J., Janik, B. and Walker, G. (1983) Measurement of glycosylated hemoglobin on cellulose acetate mem- branes by mobile affinity electrophoresis. Clin. Chem. 29, 340-343. Lendrum, R., Walker, G., Cudworth, A.G.. Theophamides, C. and Pyke, D. (1976) Islet cell anti- bodies in diabetes mellitus. Lancet 2, 1273-1276. Pilcher, C. and Elliott, R.B. (1984) Improved sensitivity of islet cell cytoplasmic assay in diabetics. Lancet 2. 1352 (letter). Reeves, W.G., Gelsthorpe, K., Van der Minne, P., Torensma, R. and Tattersall, R.B. (1984) HLA phenotype and insulin antibody production. Clin. Exp. Immunol. 57, 443-448. Mann, D.L., Mendell, N., Kahn, C.R., Johnson, A.M. and Rosenthal, A. (1983) In vitro lymphocyte prolifera- tion response to therapeutic insulin components. Evi- dence for genetic control by the human major histocompatibility complex. J. Clin. Invest. 72, 1130-1138. Kurtz, A.B., Di Silvio, L. and Lydyard, P. (1985) Lym- phocyte proliferation as a test of the immune response to insulin in diabetics. Diabetes Res. 2, 175-178.
13
14
15
16
17
18
19
20
21
22
23
24
25
26
Faulk, W.P., Girard, J.P. and Welscher, H.D. (1975) Cell- mediated immunity to insulin and its polypeptide chains in insulin-treated diabetics. Int. Archs. Allergy Appl. Immunol. 48, 364-371. MacCuish, A.C., Urbaniak, S.J., Campbell, C.J., Duncan, L.J.P. and Irvine, W.J. (1975) Cell-mediated immunity in diabetes mellitus. Diabetes 24, 36-43. Nell, L.J. and Thomas, J.W. (1983) The human immune response to insulin. I. Kinetic and cellular aspects of lym- phocyte proliferative responses in diabetics. J. Immunol. 131,701-705. Scheinin, T., Groop, L., Nikklia, E. and Kontianen, S. (1983) Proliferative responses to insulin antigens in diabetics and controls. J. Clin. Lab. Imrnunol. 2, 135-141. Scheinin, T., Maenpaa, J., Koskimies, S.. Dean, B.M.. Bottazzo, G.F. and Kontianen, S. (1989) Insulin responses and lymphocyte subclasses in children with newly diagnosed insulin-dependent diabetes. Clin. Exp. Irnmunol. 71, 91-95. Ragab, A.H., Hazlett, B. and Cowan. D. H. (1972) Responses of peripheral blood lymphocytes from patients with diabetes mellitus to phytohaemagglutinin and Cun- dida albicans antigen. Diabetes 21, 906-907. Gregory, R., McElveen, J. and Todd, I. (1990) The effects of glucose and ketones on antigen-specific human T cell responses in vitro. Diabetic Med 75 (2) 22A (abstract). Maislos, M., Mead, P.M., Gaynor, D. and Robbins, D.C. (1986) The source of covalent aggregates of insulin in type 1 diabetic patients is therapeutic insulin. J. Clin. Invest. 77, 717-723. Kurtz, A.B., Gray, R.S.. Markanday, S. and Nabarro. J.D.N. (1983) Circulating IgG antibody to protamine in patients treated with protamine insulins. Diabetologia 25, 322-324. Ellerhorst, J.A., Comstock, J.P. and Nell, L. J. (1990) Protamine antibody production in diabetic subjects treated with NPH insulin. Am. J. Med. Sci. 299, 298-301. Sanchez, M.B., Paolillo. M., Chacon, S.R. and Camejo, M. (1982) Protamine as a cause of generalised allergic reaction to NPH insulin. Lancet 1. 1243. Moorthy, S.S., Pond, W. and Rowland, R.G. (1980) Severe circulatory shock following protamine (an anaphylactic reaction). Anaesth. Analg. 59, 77-78. Stewart, W.J., McSweeny, S.M., Kellett, M.A., Faxon. D.P. and Ryan, T.J. (1984) Increased risk of severe pro- tamine reactions in NPH insulin-dependent diabetics undergoing cardiac catheterisation. Circulation 70, 788-792. Gregory, R. and Reeves, W.G. (1987) T cell reactivity in newly diagnosed diabetic patients and the effect of treat- ment with isophane insulins. Diabetologia 30. 525A (abstract).