JSNA: Data, People, Issues, Action. Mark Holtom Adult Social Services Blackburn with Darwen.
Upload
darrell-waltersCategory
view
217download
1
Blackburn with Darwen CCGProtected Learning Time Event
18th June 2015
Pendle SuiteDunkenhalgh Hotel
WelcomeDr Stephen GunnClinical Lead for Primary Care
Care.Data
Dr Hereward BrownClinical Lead for IT and Information
Contact Details:Jeanette Pearson:Engagement Lead for the CCG – 07810413402
Helen Sanderson Walker:Comms Lead for the CCG – 07880476109
Janet King: NHSE Regional Head of Intelligence – 07876851841
Justine Banks:HSCIS Project Co-ordinator – 07909093044
Email: [email protected]

Housekeeping:
Agenda
12.30 – 13.20 Registration and lunch
13.20 – 13.30 Welcome and Introduction Dr Stephen Gunn
13.30 – 15.15 PREVENT Training Marie Gibbons
15.15 – 15.45 Refreshment Break and Networking Session
15.45 – 16.45 Genetics Outreach Project Naz Khan
16.45 Close
Prevent and the NHS•Marie Gibbons
•Regional Prevent Coordinator
•NHS England (North West)
Gordon Mc Geechan Prevent Sergeant Lancashire Constabulary
Blackburn with Darwen CCG
18th June 2015
NHS | Presentation to [XXXX Company] | [Type Date]8
ContestUK Counter Terrorism Strategy
Section number
Prevent Pursue Protect Prepare
Learning Outcomes……….
Making the Link………
•Recognise
•Respond
•Refer
•Report
NHS | Presentation to [XXXX Company] | [Type Date]9
Beware of assumptions
• There is no single profile of a terrorist – there is no checklist to measure someone against
• This is not about race, religion or ethnicity - we are here to consider the exploitation of vulnerable people
NHS | Presentation to [XXXX Company] | [Type Date]10
•Counter terrorism and security Act February 2015 is intended to deal with multiple aspects of the terrorist threat ……….
• Ideology –what happens on social media-work with social media to remove /counter narratives
• Disrupt /delay travel –intended to protect the vulnerable
• Support individuals at risk of being drawn into radicalisation
Prevent in context
Prevent Objectives………..• Prevent individualsindividuals from being drawn into terrorism and ensure that they are
given appropriate advice and support;
• Respond to the ideologicalideological challenge of terrorism and the threat from those who promote it;
• Work with a wide range of institutionsinstitutions and sectors (including social care, health, HE/FE and faith communities) to address risks of radicalisation
NHS | Presentation to [XXXX Company] | [Type Date]12
Aim:-
Ensure common and higher standards across organisations ensuring that Prevent and Channel processes are effective
3 key themes …………
Leadership –
•Understand risk of radicalisation
•Ensure staff understand & build capability to deal with it
•Communicate and promote the importance of the duty
•Ensure implementation
Prevent Duty 2015
Working in partnership
• Effective partnership working
• Demonstrate compliance with the duty
• Demonstrate evidence of productive co-operation
Capabilities
• Understand radicalisation
• Help available and how to access it
• Have appropriate awareness /training
Prevent duty
Radicalisation
9/11
London Buses
Twin towers
Fundraising
PLANNING
ATTACK
Recruitment
COMMUNITIES
Vulnerable People within our community

16

Current risks and threats
Blackburn with Darwen ……….
NHS | Presentation to [XXXX Company] | [Type Date]18
Susceptibilities / Vulnerablities…..?
NHS | Presentation to [XXXX Company] | [Type Date]19
20
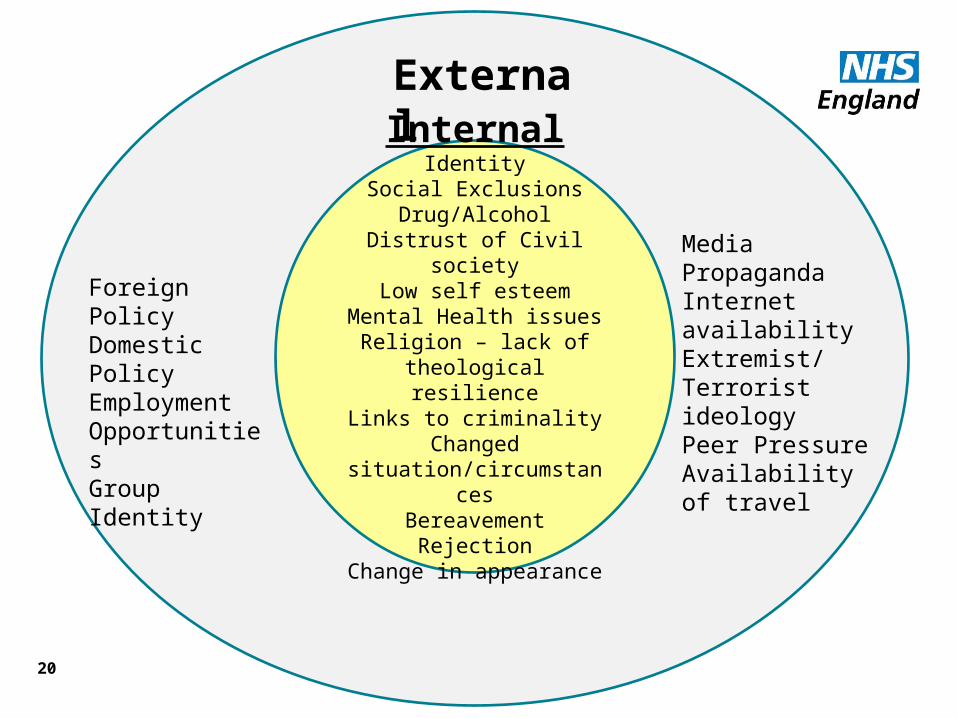
InternalIdentity
Social ExclusionsDrug/Alcohol
Distrust of Civil societyLow self esteem
Mental Health issuesReligion – lack of
theological resilienceLinks to criminality
Changed situation/circumstances
BereavementRejection
Change in appearance
External
Foreign PolicyDomestic PolicyEmployment OpportunitiesGroup Identity
MediaPropagandaInternet availabilityExtremist/Terrorist ideologyPeer PressureAvailability of travel
Your role………..? Your role………..?
• NHS Key partner • Identified Prevent Lead / Support network• Policy and Procedure • Training & Awareness raising • Sharing concerns – having a conversation!
Safeguarding is everyone’s business
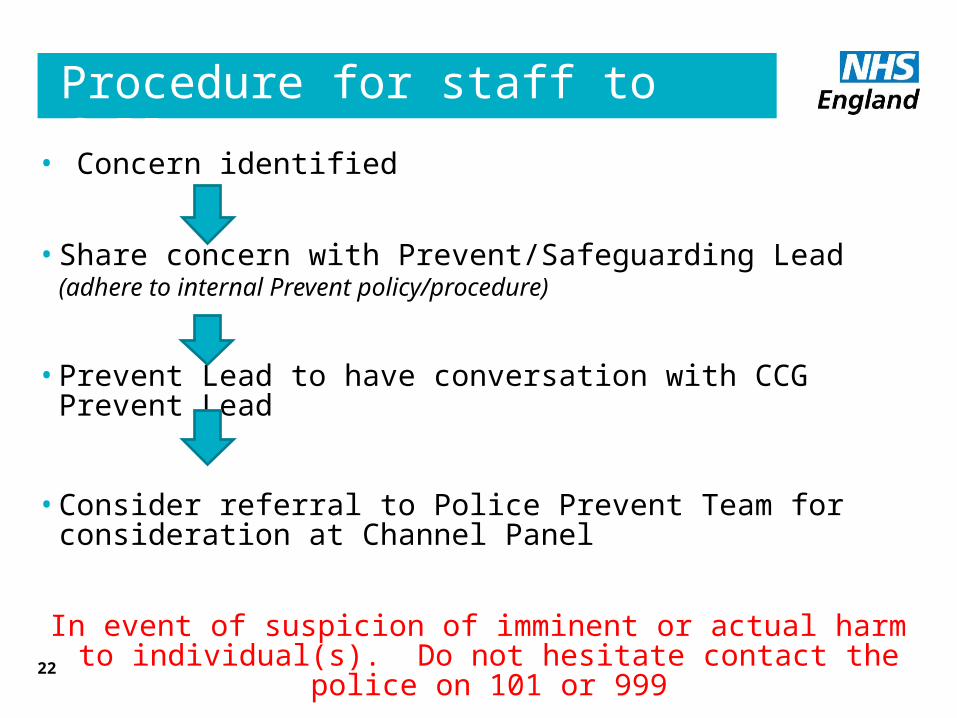
Procedure for staff to follow………..
• Concern identified
• Share concern with Prevent/Safeguarding Lead (adhere to internal Prevent policy/procedure)
• Prevent Lead to have conversation with CCG Prevent Lead
• Consider referral to Police Prevent Team for consideration at Channel Panel
In event of suspicion of imminent or actual harm to individual(s). Do not hesitate contact the police on 101 or
99922
In SummaryIn Summary
• Be vigilant
• Who is your prevent lead?
• Share your concerns with a “conversation”
• Use common sense
• Act on your concerns
Thank you
• Marie Gibbons
Regional Prevent Lead (north west) NHS England
Telephone office – 01138 248 938
Mobile – 07896717647
• Gordon McGeechan
Telephone – 01254 353541 / 01772413366
NHS | Presentation to [XXXX Company] | [Type Date]24
Refreshments and Networking
Genetic and Social Implications of Consanguineous Marriage
Naz Khan
June 2015
Objectives of training• To understand the Genetic and Social implications of
consanguineous marriage• Presentation of local data on autosomal recessive disorders• The impact of genetic disorders on infant and childhood
mortality/morbidity locally • Intervention strategies in East Lancashire • Feedback on evaluation of the service development post and
lessons learnt• Develop confidence in initiating discussions about issues
relating to marrying close relatives• To be able to identify families for referral • How to make appropriate referrals to the enhanced genetic
service • Familial cancer in South Asian communities
BWD Population
• 2011 census - BWD: 26.4% south Asian (12.1 Pakistani 13.4 Indian)
• Growing population - 2001 census 19% South Asian
• Average UK towns and cities 4.7%
• 27% Muslim in BWD (4.8% average in UK)• • 63% of Pakistani’s In Blackburn were born in Pakistan
• 25% of deliveries in East Lancashire were to women of Pakistani/Indian Heritage (based on local figures from ELHT trust 2013/2014
• BWD 17th most deprived local authority area in the Country (DCLG 2014)
Ref 2011 Census/ONS
Measuring mortality in the early years
• Measures of mortality relating to early life are critical indicators of the general health of a community
• IMR used by organisations including the WHO
• Included in NHS Outcomes Framework, Health & Wellbeing Strategies
• Allows comparisons between regions
• Can be used to track improvements over time
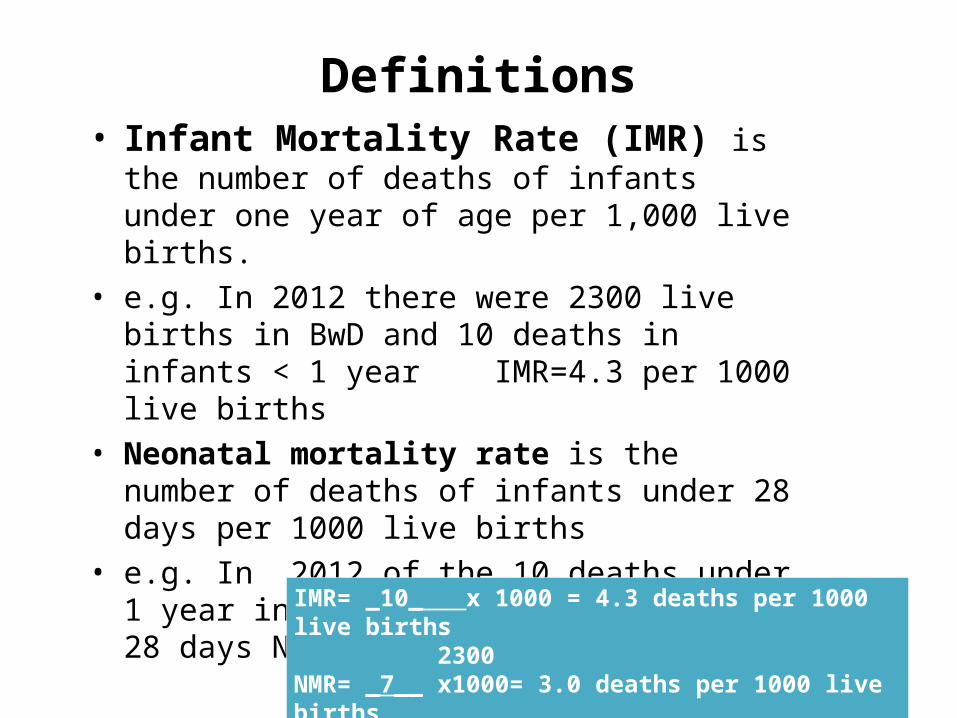
Definitions• Infant Mortality Rate (IMR) is the number
of deaths of infants under one year of age per 1,000 live births.
• e.g. In 2012 there were 2300 live births in BwD and 10 deaths in infants < 1 year IMR=4.3 per 1000 live births
• Neonatal mortality rate is the number of deaths of infants under 28 days per 1000 live births
• e.g. In 2012 of the 10 deaths under 1 year in BwD. 7 were infants < 28 days NMR= 3.0 per live births
IMR= _10_ x 1000 = 4.3 deaths per 1000 live births 2300NMR= _7__ x1000= 3.0 deaths per 1000 live births 2300

Infant mortality rates-by countrySource: OECD health data and WHO Global Health Observatory]
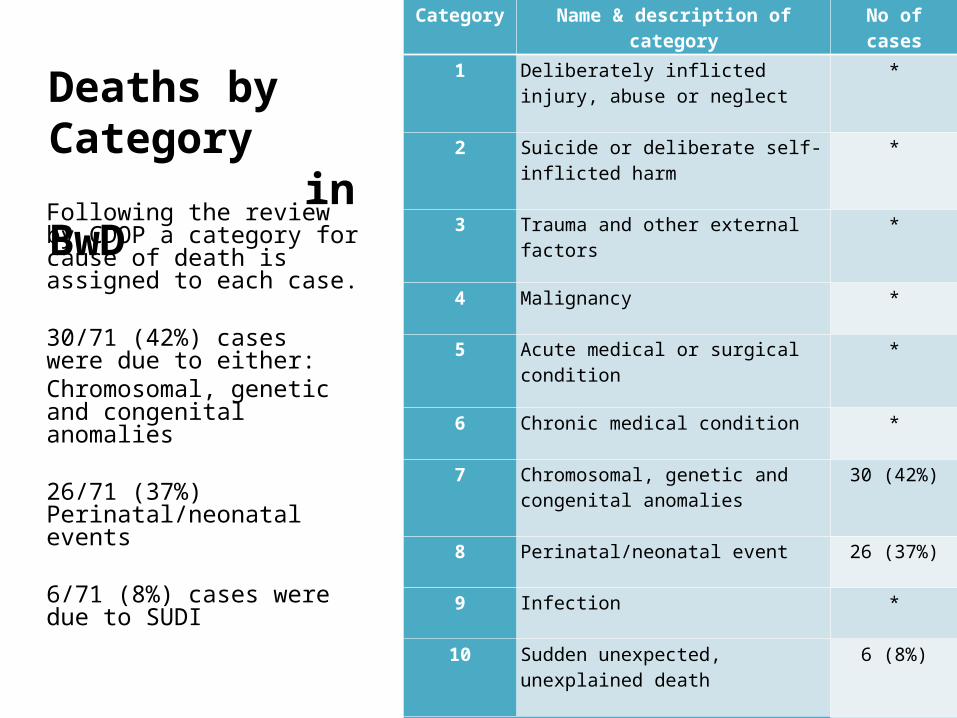
Deaths by Category in BwD
Category Name & description of category No of cases
1 Deliberately inflicted injury, abuse or neglect
*
2 Suicide or deliberate self-inflicted harm
*
3 Trauma and other external factors *
4 Malignancy *
5 Acute medical or surgical condition *
6 Chronic medical condition *
7 Chromosomal, genetic and congenital anomalies
30 (42%)
8 Perinatal/neonatal event 26 (37%)
9 Infection *
10 Sudden unexpected, unexplained death
6 (8%)
Total number of cases in BwD 71
Following the review by CDOP a category for cause of death is assigned to each case.
30/71 (42%) cases were due to either: Chromosomal, genetic and congenital anomalies
26/71 (37%) Perinatal/neonatal events
6/71 (8%) cases were due to SUDI
Blackburn
• Infant Mortality 2013-2014 : 6.5 per 1.000 significantly higher than national and North West average of 4.3 and 5.0.
• Childhood mortality 2013-2014: 16.6 higher than the national average of 12
Consanguineous marriage• Consanguineous means of the same blood• Consanguineous marriage is marriage between blood relatives• 20% of the worlds population live in communities that favour
consanguineous marriage• 8.5% of all births are to parents who are consanguineous• 25% of cousin marriages in the UK are among white
majority population Source: World Health Organization 1985 AdvisoryGroup on Hereditary Diseases. Communityapproaches to the control of hereditary diseases.Unpublished WHO document: HMG/WG/85.10.Available at:http://whqlibdoc.who.int/hq/198586/HDP_WG_85.10.pdfGenetics Communication DiversityCustoms governing first cousin marriage(GP Murdock, Ethnographic Atlas, 1967)Latitude
Consanguineous marriage
• Customary in many parts of the World Pakistan, Bangladeshi, Middle East, Some Indian, Irish travellers, Some Refugee groups.
• Pakistani Heritage have the highest rate of cousin marriage (at least 55%)
• In BwD, 95% of Asian parents with an affected child were in a consanguineous marriage
• Integral Cultural and social practice• Associated with Islam but neither encouraged nor
discouraged by Islam
Reasons why people consider consanguineous marriage
• Cultural • Strengthens family ties and support systems; keeping connections • Ease of finding a more suitable match and having more stable
marriages • Maintains a woman’s status within the family hierarchy • Maintains family lineage • Preserves culture and tradition • Financial benefits• Obligation to kin • Economic / Immigration
Health Issues associated with Consanguinity
• Increased risk of genetic disorders• High infant mortality and childhood
morbidity• Limited engagement with Health Services• Lack of awareness of inherited disorders• Stigmatisation• Communication issues
Cousin marriage and inherited/genetic disorders
• Does not influence chromosomal abnormalities, sex linked or dominantly inherited disorders
• Impacts exclusively on recessively inherited disorders• Populations where partner choice is random A.R
disorders random and scattered• Communities that practice consanguinity AR disorders
cluster within extended family groups
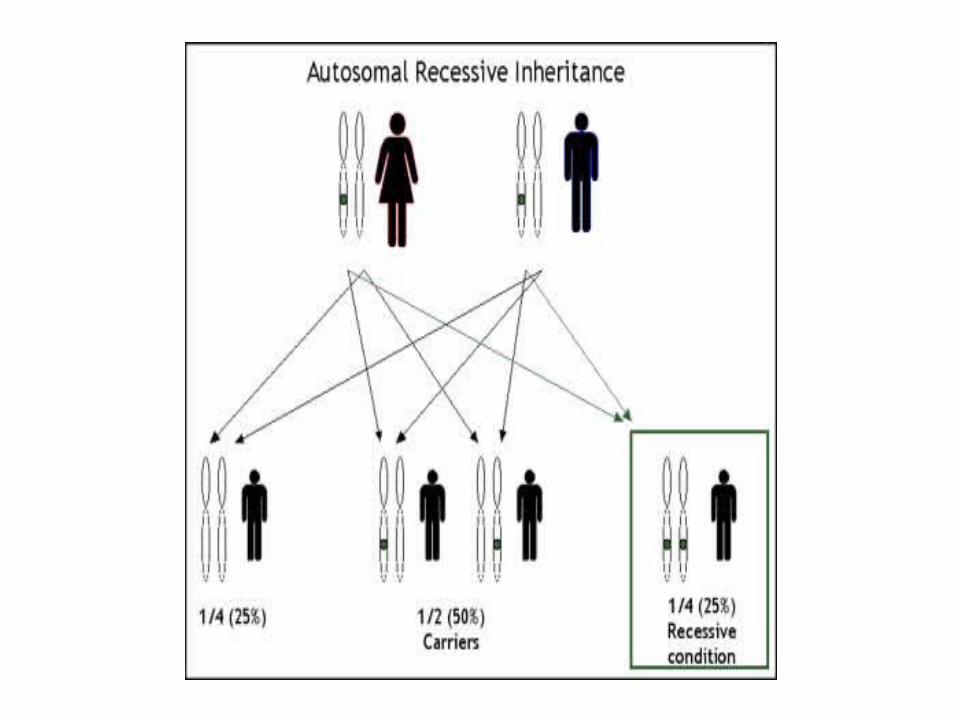
Genetics• Our bodies are made up of millions of cells. • Cells contains genes• 2 copies of every single gene• One copy inherited from mother, one copy inherited
from father• 30,000 genes• Most people are carriers for a at lease 1-2 recessive
disorders• Carriers healthy• Population risks of being a carrier for some
conditions• Rare recessive disorders
Autosomal recessive disorders• 2-3,000 known autosomal recessive disorders• Phenylketonuria (PKU)• Congenital adrenal hyperplasia• Spinal Muscular atrophy• Many biochemical/metabolic disorders
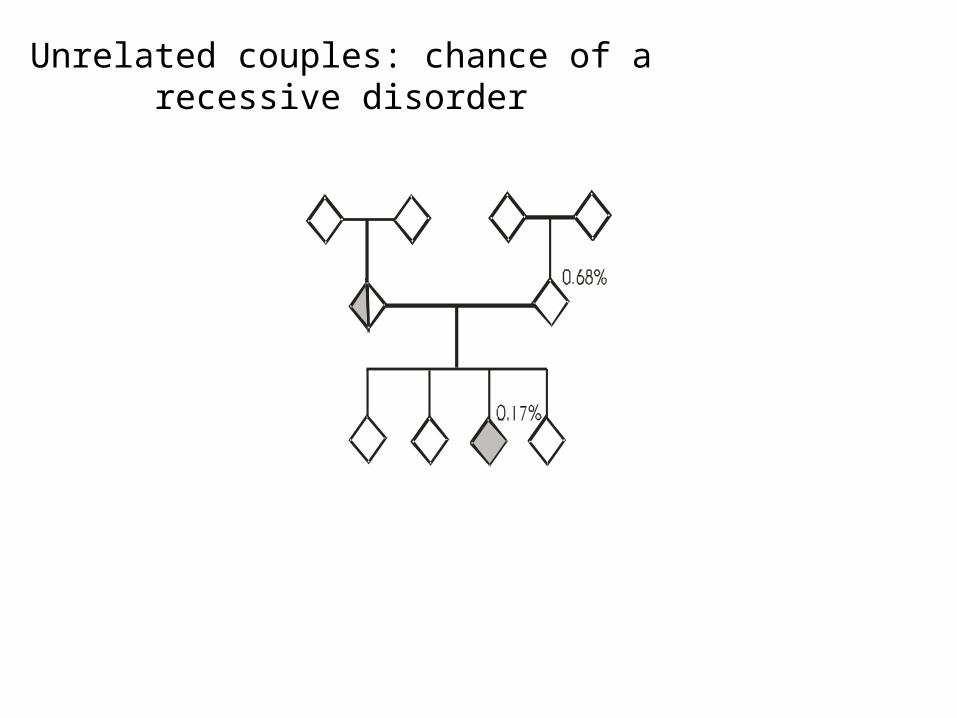
Unrelated couples: chance of a recessive disorder
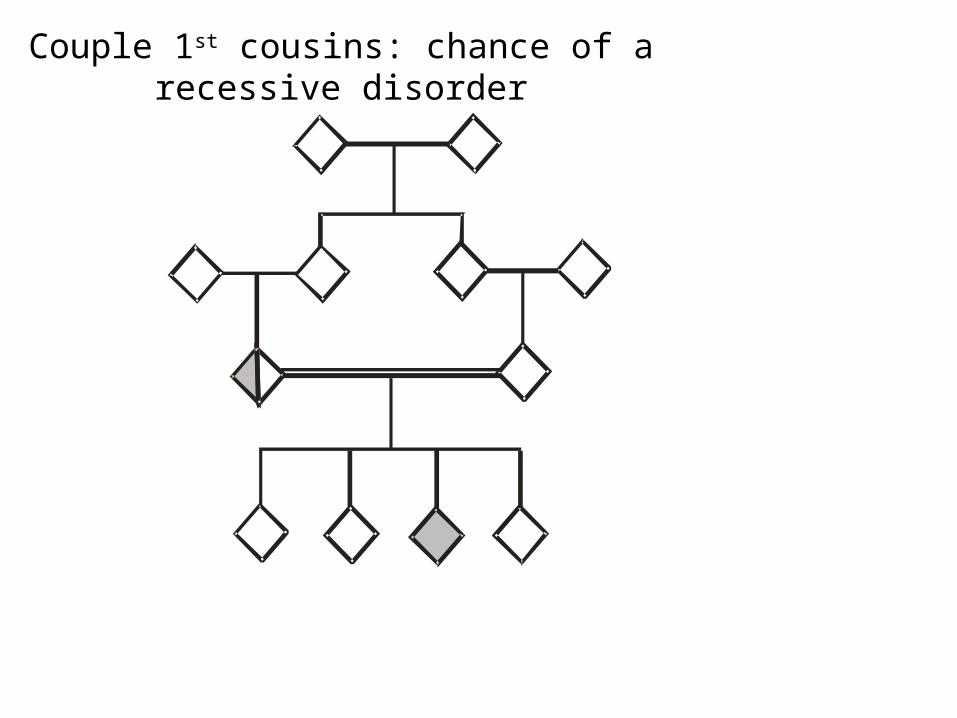
Couple 1st cousins: chance of a recessive disorder
What to do?
10-15% of consanguineous couples are at risk
85-90% of consanguineous couples are not at risk
• Discourage consanguineous marriage at the population level?
• Try to identify and inform those at risk?

Try to identify and inform those at risk?(A family-centred approach)
• In families transmitting a disorder, an affected child will be born once around 12+ cousin marriages
• Paediatric and genetic counselling services are aware of all diagnosed affected children
So, Start with the affected person
Draw up an extended family tree
Offer information to all family members
Offer carrier testing to all members
Aim for married couples & children & young peopleProvide information and long-term support
WHO recommended approach
Dr Benson’s Study (2002)
Two Part Study:
• The Range and Prevalence of Recessive disorders in the Blackburn population.
• Health Perceptions and families response to Genetic Information
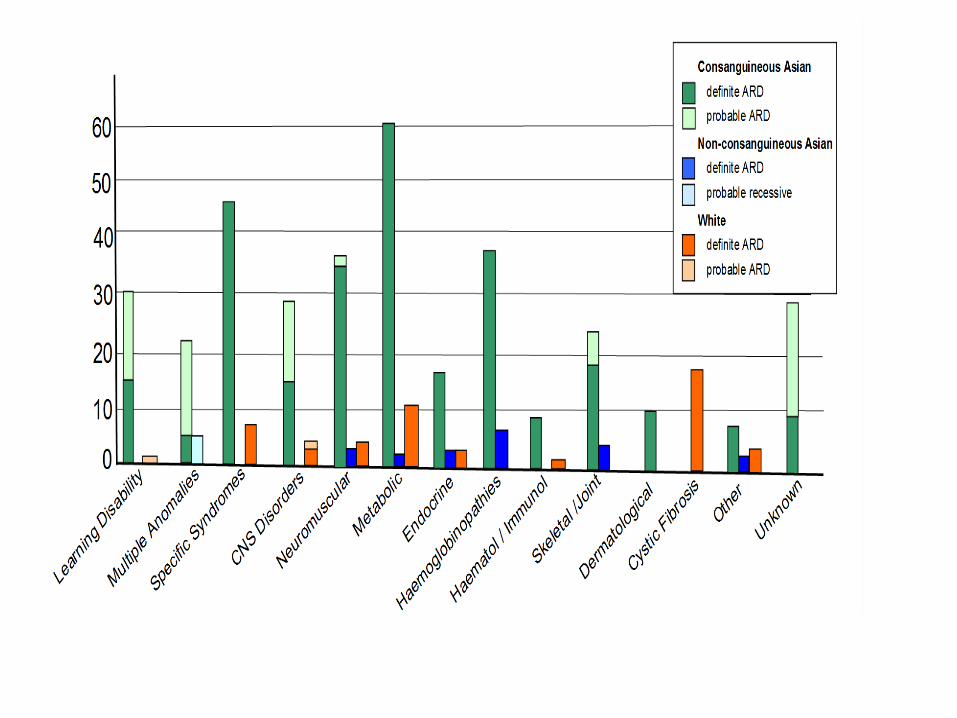
Results of Dr Benson Study
• Incidence of definite recessive disorders in the Asian population was 12 times that of the incidence in the white population.
• 83 different recessive disorders diagnosed.• Where data recorded 95% of Asian parents were
consanguineous. • 13 recessive disorders per 1000 Asian births• Several Asian families with 3 or more affected children
Service development Bid• DOH under the Genetic White paper (2003)• To improve the clinical service available to South Asian origin who
have children affected by A.R disorders.• To reach extended family members in consanguineous families so
that they understand their own risk of having affected children and can make informed reproductive choices including arranging future marriages within/without the family.
Evaluation
• Of the 72 questionnaires distributed, 46 were completed. The questionnaires were analyzed using SPSS. Overall the service to families has been received very positively
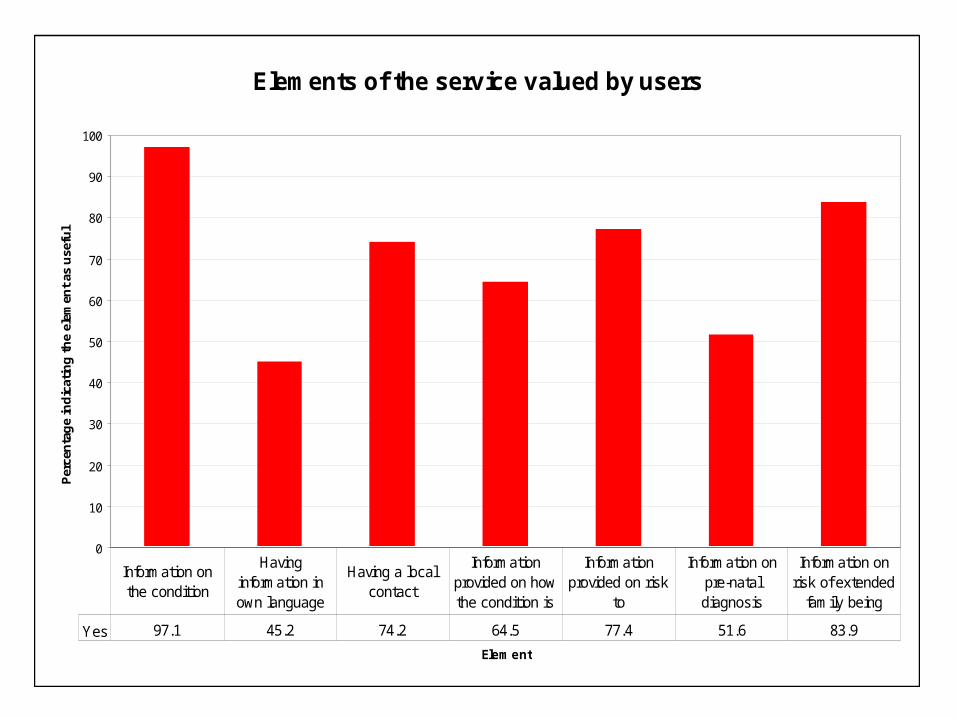
Elements of the service valued by users
0
10
20
30
40
50
60
70
80
90
100
Element
Per
cen
tag
e in
dic
atin
g t
he
elem
ent
as u
sefu
l
Yes 97.1 45.2 74.2 64.5 77.4 51.6 83.9
Information on the condition
Having information in own language
Having a local contact
Information provided on how the condition is
Information provided on risk
to
Information on pre-natal diagnosis
Information on risk of extended
family being
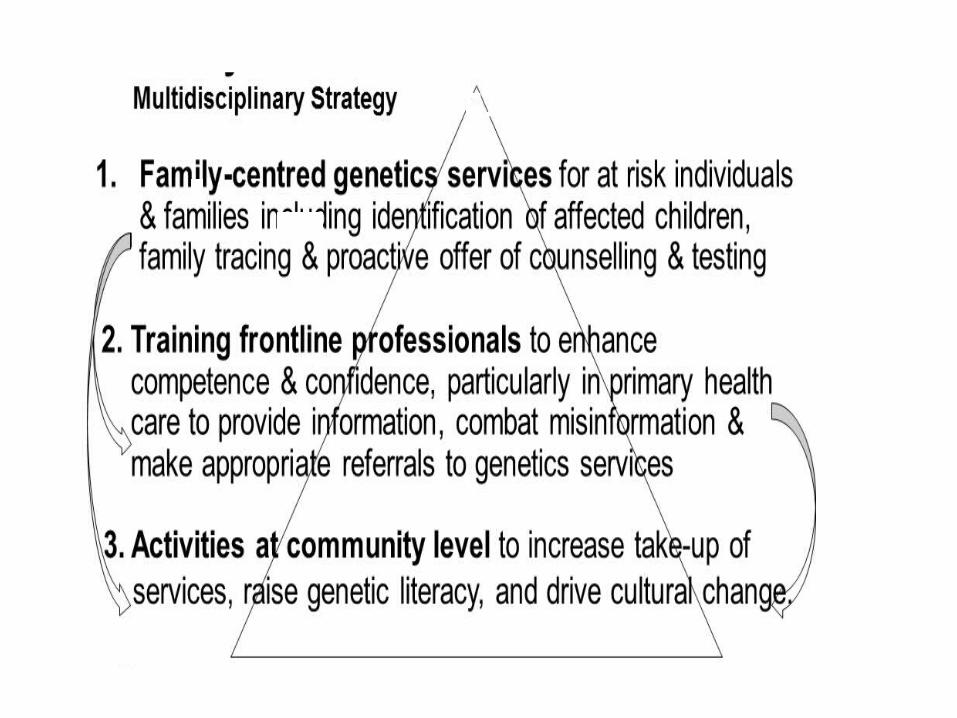
Multidisciplinary strategy
Regional Genetic serviceGenetic services
ClinicalLaboratory (Cytogenetics, Molecular and Biochemical )
Based at St Mary’s Hospital in Manchester (with some clinics in DGHs)
Covers NW region (population of approx. 5 million)
~250 people in team Doctors (consultants and Registrars)Counsellors (MSc Genetics)Clinical scientists & Admin
Enhanced Genetic service BwDClinical service:
Local, hospital-based (RBH) clinical genetic service established for families of South Asian heritage who have children affected with autosomal recessive disordersProactive service follow up extended family membersEast Lancashire service
Community engagement project:
Working with 3rd sector: Health and Well being Consortium/Home start to employ a Genetic Outreach worker, to liaise directly with families and community based health and support services (BWD and Pendle)
Training Front line Health Professionals
• Understand the genetic and social implications of consanguineous marriage
• Understand their own role in the community genetics infrastructure
• Be clear about their professional responsibility and boundaries
• Be aware of health services that people can be referred to for further help
• Speak with confidence about issues relating to marrying close relatives
Role of Genetic Outreach worker• Identify families in the community who will benefit from
additional support• Set up open access groups in children centres to make
genetic information accessible to everyone• Take family histories and explaining AR inheritance• If families unsure of referral to genetics genetic outreach
worker can work with family in own home
Challenges
• Primary care is route for access to genetics services
• To develop an approach which is feasible within a consultation (or 2)
• Screening questions (EMIS)• To ensure patients / couples have consistent
information• Which is non-judgemental and will maximise
engagement
Challenges in engaging families
• Family dynamics / non-disclosure of information
• Concept of genetic counselling• Large number of potential conditions, each
individually rare• Attitudes to termination of pregnancy• Attitudes to consanguinity
Families to consider referring
• Have an affected child – diagnosed/undiagnosed• Known A.R Genetic disorder in the family• Several individuals affected- similar clinical
phenotype • Pregnancies ascertaining family history• Diagnosis through New-born Screening• Disability/affected individuals in the family• Adult who is affected with a condition themselves• Sibling affected with a AR disorder
Exclusions
• Thalassaemia and sickle cell refer to thalassemia and sickle cell centre unless they are a carrier couple
• Eczema, haemachromatosis, Alpha1 antitrypsin, cystic fibrosis carriers.
• Child developmental delay see Paediatircian first for initial work up
Cancer and South Asian Families
• Cancer not considered genetic• Families do not reveal family history or
request referral to genetics• Underrepresented in cancer referrals to the
dept.• If cancer at young age consider referral to
genetic• Ask specific questions re family history
Cancer referrals• Early on-set cancer <50 years• Breast cancer <50 years refer family history clinic
initial assessment• Bowel cancer or multiple bowel polyps >10
<50years refer to Genetics• High grade serous ovarian cancer <60years refer to
genetics• Unusual cancer at young age <50 years refer to
genetics• If unsure phone/MANGEN website referral
guidelines

Key Messages
• GPs can identify families at high risk• Family first point of contact is with the GP• GP- ask about family health
-Know families
- assessment of the genetic risk in
the family
- refer to RGS or seek advice from RGS
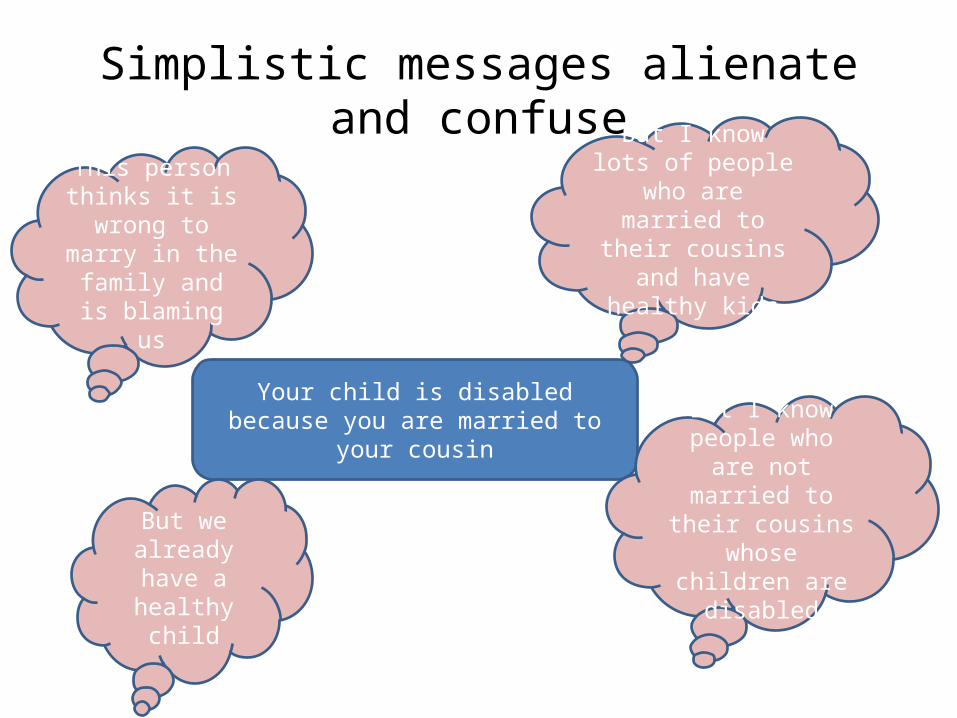
Simplistic messages alienate and confuse
Your child is disabled because you are married to your cousin
But I know lots of people who are married to their
cousins and have healthy kids
But I know people who are not
married to their cousins whose
children are disabled
But we already have
a healthy child
This person thinks it is
wrong to marry in the family and
is blaming us

Advances in Technology
• Genetic testing available for an increasing number of conditions
• Micro array• Testing through Panels• Exomes• Genome England study• NIPD• FFDNA• PGD
Key messages to share and pass onaround genetic inheritance
• Genetics affect us all, the more we understand the issues and the risks, the more we will be able to make informed choices
Referring Families
Naz Khan Genetic CounsellorGenetic Medicine6th Floor St Mary’s HospitalOxford Road Manchester M13 9WL Tel: 0161 276 6285 /Fax 0161 276 6145Email: [email protected]