Language Modeling, Pitman-Yor, Beta Process & Stable Beta ...

Beta-lactamase inhibition: A potted history of beta lactamase and lessons from recent development of beta-lactamase inhibiter combinationsDr Shampa Das, Senior Lecturer, Molecular and Clinical Pharmacology, University of Liverpool

!-lactamase inhibition: A potted history of ! lactamase and lessons
from recent development of !-lactamase inhibitor combinations
Shampa DasShampa Das PKPD Ltd/ Senior Lecturer, University of Liverpool
BSAC, January 15th, 2019
2

Outline
• Brief overview of !-lactams (BLs) and !-lactamase inhibitors (BLIs)• Challenges of developing BL-BLI combinations• Thoughts on why we develop BL-BLI combinations rather than a
standalone inhibitor
3

What are !-lactam antibiotics?
• There are 5 basic mechanisms by which antibiotics act:• Inhibition of cell wall synthesis• Inhibition of protein synthesis• Alteration of cell membranes• Inhibition of nucleic acid synthesis• Anti-metabolite activity
4
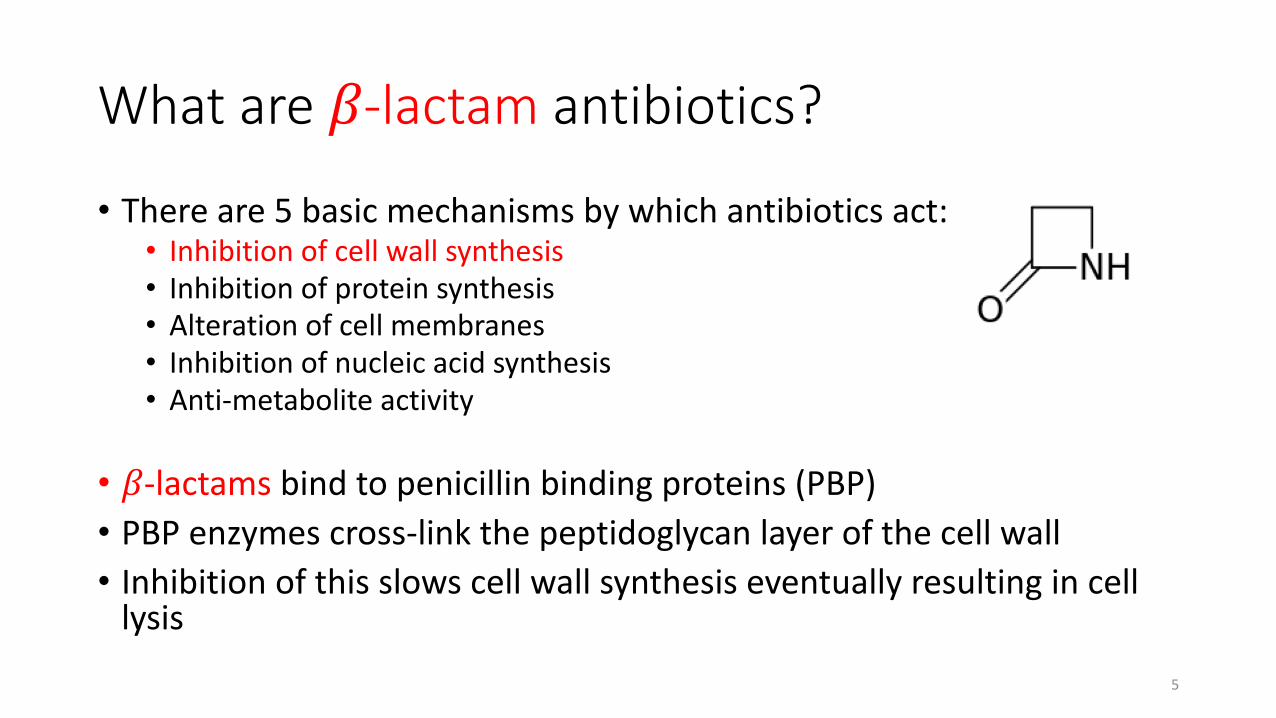
What are !-lactam antibiotics?
• There are 5 basic mechanisms by which antibiotics act:• Inhibition of cell wall synthesis• Inhibition of protein synthesis• Alteration of cell membranes• Inhibition of nucleic acid synthesis• Anti-metabolite activity
• !-lactams bind to penicillin binding proteins (PBP)• PBP enzymes cross-link the peptidoglycan layer of the cell wall• Inhibition of this slows cell wall synthesis eventually resulting in cell
lysis5

!-lactams are one of the most commonly used antibiotics• Well used because they have bactericidal effect, well tolerated and
broad spectrum• Account for majority of parenteral prescriptions in the US• There are many different PBPs and thus a diverse range of !-lactams
with different spectrum of activity:• Penicillins• Cephalosporins• Carbapenems• Monobactams
As monotherapy, cephalosporins and carbapenems account for the most use
6

Resistance to !-lactam antibiotics
• !-lactams are becoming less effective due to emerging resistance, of which there are several mechanisms: • Inactivation by !-lactamase enzymes• Changes in active site of PBPs which reduces the affinity of !-lactam
antibiotics• Alteration or loss of porin, reducing access of !-lactams in Gram-negative
bacteria• Production of efflux pumps
7

Hydrolysis by !-lactamases is the primary resistance mechanism to affect the activity of !-lactams
• There has been a rapid and growing emergence of !-lactamases since the 1960’s
!-lactamases hydrolyse the !-lactam ring thus inactivating the !-lactam
8
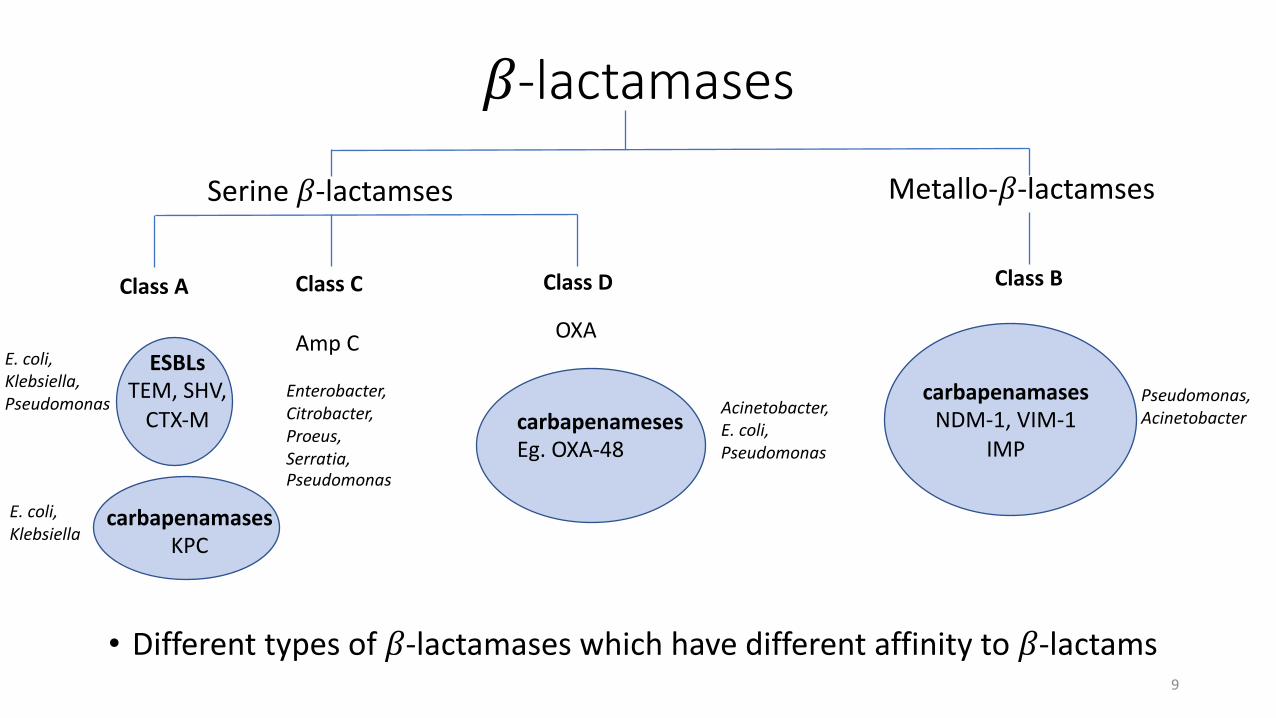
!-lactamases
• Different types of !-lactamases which have different affinity to !-lactams
Serine !-lactamses Metallo-!-lactamses
Class A Class C Class D Class B
ESBLsTEM, SHV,
CTX-M
Amp C OXA
carbapenamasesNDM-1, VIM-1
IMP
carbapenamasesKPC
carbapenamesesEg. OXA-48
Pseudomonas, AcinetobacterAcinetobacter,
E. coli, Pseudomonas
E. coli, Klebsiella, Pseudomonas
E. coli, Klebsiella
Enterobacter, Citrobacter, Proeus, Serratia, Pseudomonas
9

Impact on !-lactam antibiotics
• Penicillins – limited utility as monotherapy now due to !-lactamases• Cephalosporins – generally broad spectrum, but use is being limited
by extended spectrum !-lactamases (ESBLs) and metallo-!-lactamases (MBLs)• Monobactams – only Aztreonam licensed, labile to ESBLs and most
carbapenemases but stable to MBLs• Carbapenems – broad spectrum and not susceptible to ESBLs but are
susceptible to carbapenemases (KPC, some OXA and MBLs)
10

!-lactamase inhibitors (BLIs)
• Developed to be co-admistered with !-lactam antibiotics• BLIs bind to !-lactamases, preventing hydrolysis of the !-lactam• Used in combination with a !-lactam to extend its spectrum of
activity• Generally little inherent antibiotic activity
11

Early !-lactamase inhibitorsContain !-lactam ring in structure
• Some !-lactam activity• Inhibit non-carbapenamse Class A enzymes (i.e. not KPC)
12

BL-BLI combinations
• Clavulanic acid was developed with amoxycillin as the first BL-BLI combination • Subsequently tazobactam and sulbactam developed with similar
spectrum of activity• Sulbactam is generally combined with ampicillin• Tazobactam is combined with piperacillin • More recently tazobactam has been approved in combination with
ceftolozane• AAI101 is a new BLI currently in development with extended activity
13
Non-!-lactam-!-lactamase inhibitors
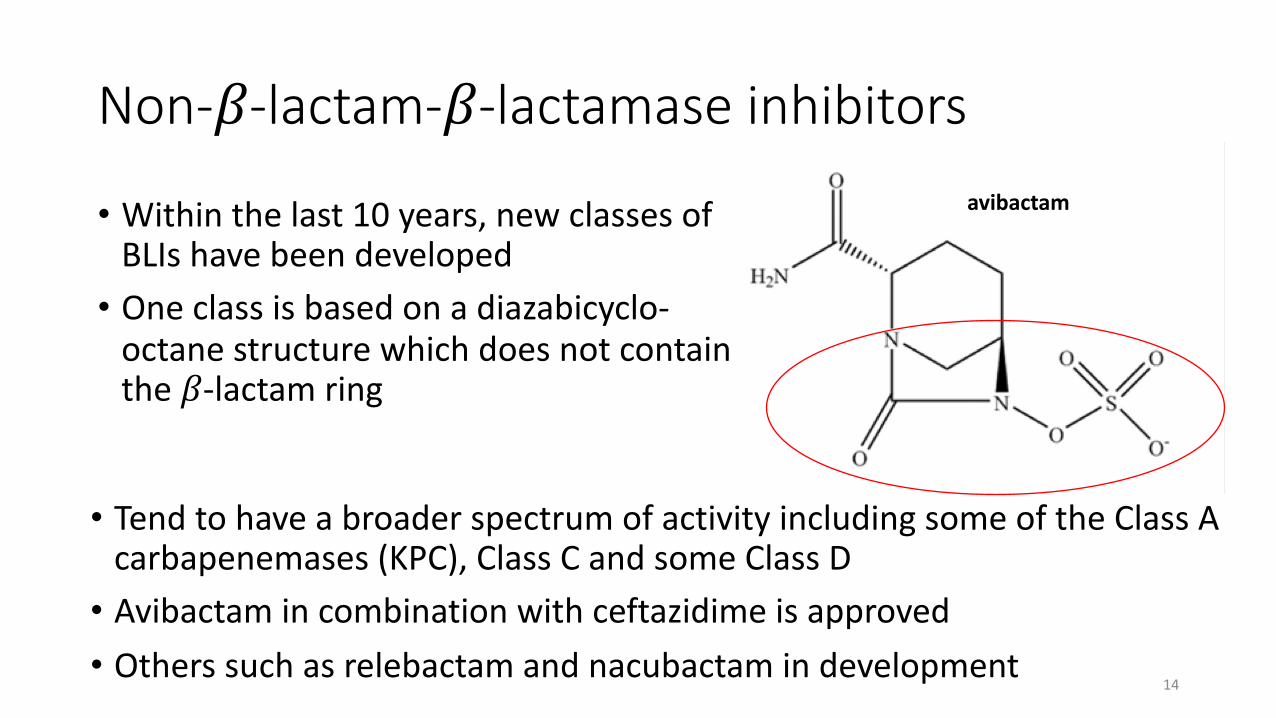
• Within the last 10 years, new classes of BLIs have been developed• One class is based on a diazabicyclo-
octane structure which does not contain the !-lactam ring
avibactam
• Tend to have a broader spectrum of activity including some of the Class A carbapenemases (KPC), Class C and some Class D• Avibactam in combination with ceftazidime is approved• Others such as relebactam and nacubactam in development
14

Other BLI’s
• Vaborbactam is boronic acid and also doesn’t contain the !-lactam ring• Developed to target KPC
carbapenemases• Recently approved in combination
with meropenem
15

Activity of recently approved BL/BLI combinations
Class A Class B Class C Class DBL/BLI ESBL KPC MBL Amp C OXA - carbapenemases
Ceftazidime-avibactamCeftolozane-tazobactamMeropenem-vaborbactam
• Different BL/BLI combinations have different spectrum of activity
16

Challenge of metallo-!-lactamases (MBLs)
• Broad substrate specificity and can hydrolise most !-lactams apart from monobactams• NDM-1 is a metallo-!-lactamase• Treatment options are more limited to agents such as colistin and
tigecycline which are associated with more toxicity• Aztreonam-avibactam is currently in clinical development• Novel MBL inhibitors are in development
17

Development of BL-BLI combinations
• Developed as combination agent• Need to demonstrate that the combination provides activity that the
single agent doesn’t• Can’t compare BL-BLI to !-lactam partner alone, as this would exclude
patients for which the !-lactam is resistant• Regulatory pathway is to conduct a non-inferiority study • However, this can provide limited information on activity of the BLI
18

Limitations with data from the non-inferiority study• Ceftazidime-avibactam compared to meropenem and meropenem
vaborbactam compared to piperacillin-tazobactam in Phase 3• This precludes the recruitment of patients with carbapanemases (KPC)• Comparator arm not efficacious against KPC
• Stringent requirements about prior use of antibiotics• Impacts the type of patient recruited – less likely to be infected with resistant
pathogens
• Percentage of patients with resistant pathogens in randomised-control trials is low (<20%)
19
Resistant pathogen studies
• In both the ceftazidime-avibactam and meropenem-vaborbactamprogrammes a resistant pathogen study was conducted• Comparator arm was best available therapy • Studies very difficult to recruit especially in US and central Europe• Trying to develop drugs for emerging problem
20

Dose selection
• Correct dose selection is critical• Under-dosing will lead to emergence of resistance• BLI doesn’t have activity:• Need quantify dose of BLI through the activity of the BL partner
• Dose ranging in clinical studies will not help dose selection of the BLI• Understanding the pharmacokinetic-pharmacodynamic (PK-PD)
relationship becomes more critical
21

Pharmacodynamics of BLI
• Need to understand the pharmacodynamics (PD) of the BLI• PD may be different to the partner !-lactam
• Aim is to convert infecting bacteria to !-lactamase-negative phenotype• Due to lack of inherent activity, PD measurement is impact on activity of
the !-lactam partner• Experiments must be in !-lactam-resistant organisms with a background of !-lactam which is ineffective alone, but efficacious in combination with the BLI• More challenging than experiments to understand the PD of a single agent
22
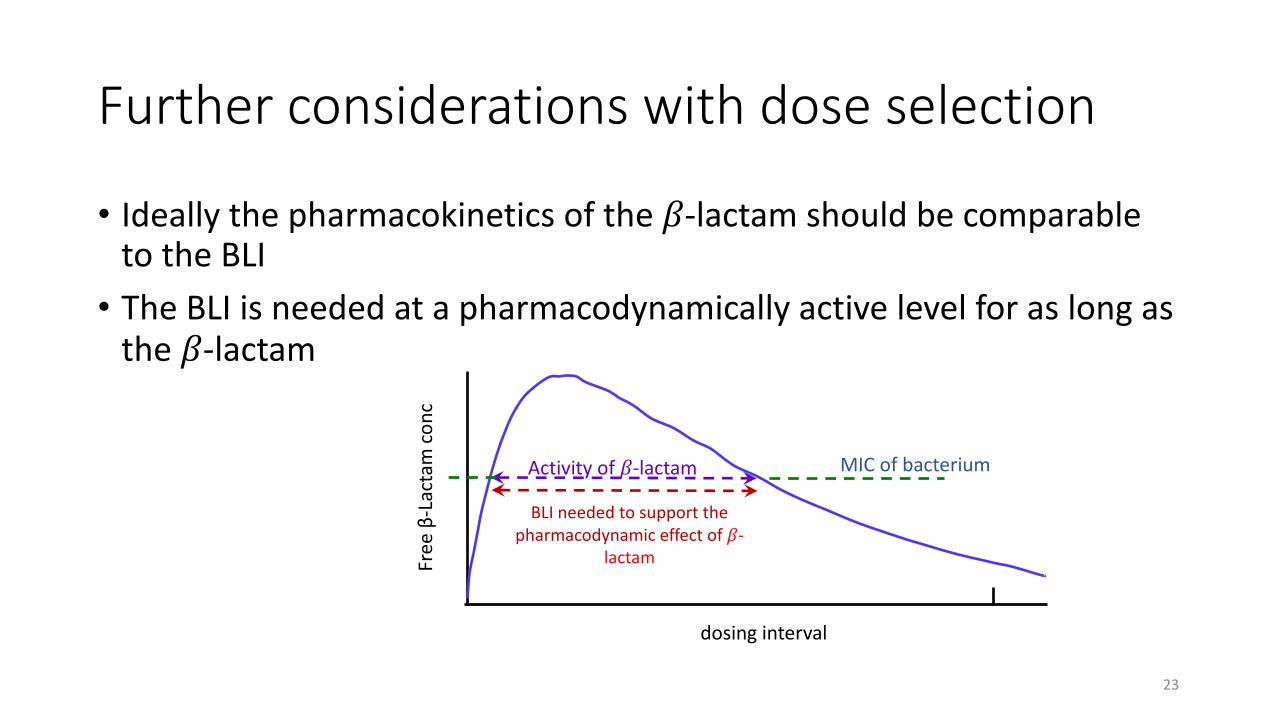
Further considerations with dose selection
• Ideally the pharmacokinetics of the !-lactam should be comparable to the BLI• The BLI is needed at a pharmacodynamically active level for as long as
the !-lactam
BLI needed to support the pharmacodynamic effect of !-
lactam
dosing interval
Free
β-L
acta
m co
nc
Activity of !-lactam MIC of bacterium
23

Challenges with PK of both agents
• BL-BLIs developed as combination agents:• Designed to be administered from a single vial
• Eg. if !-lactam with long half life partnered with BLI with short half-life• Difficult it will be difficult to adjust the
dosing of each to administer together
Time
Conc
entra
tion
!-lactam
!-lactamase inhibitor
• Need to consider on dose adjustments, eg. renal impairment, DDI, hepatic impairment, paediatric dosing etc
24

Partnering BLIs with multiple !-lactams
• Because of the heterogeneity of !-lactamases, they bind to different !-lactams and BLI’s with different affinity• Thus there is a difference to how labile different !-lactams are to the
presence of !-lactamases• This in turn impacts the amount of BLI that is required • The amount of BLI required for one !-lactam partner may differ from
other !-lactam partners, which will impact the dose and regimen• i.e. PD may be different
25

An example of this is avibactam
• Avibactam is a BLI which is approved for use in combination with ceftazidime (CAZ-AVI):• Avibactam dose designed to achieve PD target of fT> threshold concentration of 1mg/L
• Approved dose is 2g CAZ/500mg AVI, 2h infusion, q8h
• Avibactam is also currently in development with aztreonam (ATM-AVI)• However the PD target in combination with aztreonam is different• Threshold target is higher at 2.5mg/L• Thus dosing needs to be different • ATM-AVI tested in Phase 3 trials at 500mg ATM /167mg AVI 30min infusion loading
dose, with maintenance doses of 1500 ATM/500mg AVI 3h infusion, q6h
26
Why don’t we develop a standalone BLI?
• Dosing is the biggest challenge:• Different requirements with different !-lactam partners due to different
binding affinity• Accounting for differences in PK• Incorrect and inadequate dosing is a significant risk and threat to emergence
of resistance• Currently there is no regulatory pathway• What clinical evidence would be required?• Clinical trials with at least one !-lactam partner would be needed• Clinical programme with multiple partners would be costly and challenging
27

Conclusions
• !-lactams are a vital and commonly used antibiotic but emergence of resistance is threatening their utility• Development of BL-BLI combinations has been critical to the
continued use of !-lactams • Clinical development is challenging• Currently a development path for standalone BLI’s is not apparent
28