BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf

of 79
-
Upload
medicine4themasses -
Category
Documents
-
view
219 -
download
0
Transcript of BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
1/79
Benign Disorders of WBC:
Neutrophilia and Neutropenia
Elizabeth Quinlan-Bohn, MS, PA-C
Clinical Assistant Professor
DYouville College PA Program
October 23, 2014
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
2/79
What does the term benign WBCdisorders mean?
The term benign WBC disorders refers to
non-malignant causes of either decreased
or elevated WBCs.
Therefore, for the purpose of this
discussion, we will not include any
malignant disorders (e.g., leukemia) or
HIV-related illness which directly result inWBCs or WBCs.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
3/79
Blood Cell Maturation
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
4/79
Important Definitions
Granulocyte:
This term refers to a category white blood cells which have granulesin the cytoplasm, and includes: neutrophils, basophils, andeosinophils.
Granulocytopenia:
This term refers to a reduced granulocyte count.
Neutropenia:
This term refers to a reduced neutrophil count, and typically isused when the absolute neutrophil count (ANC) < 1,500. The riskfor infection increases once the ANC < 1,000, and the risk for severe
life-threatening infection increases significantly if the ANC < 500.
Neutrophilia:
This term refers to an increase in the absolute neutrophil count(ANC) > 7,500
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
5/79
More Important Definitions
Agranulocytosis:
This term refers to a complete absence of blood granulocytes, and isoften used to indicate very severe neutropenia when the ANC < 500.
Absolute Neutrophil Count (ANC):
[Total WBC x (% segmented neutrophils + % bands)] = ANC
Leukopenia:
This term refers to a total WBC below the normal range, and generallythat is defined as a total WBC < 4,300. For many institutions, the normalWBC range = 4.5K-11K.
Pancytopenia: This term refers to a decrease in the number of blood cells from all
three cell lines: WBCs, RBCs, and platelets.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
6/79
More Important Definitions
Left shift or shift to the left: Theconcept of a left shift or shift to the left
originated in 1904, when German scientist
Josef Arneth published a monograph,Neutrophile Leucocytes in Infectious
Diseases, based on a study of blood
smears from many types of acute andchronic infections. He divided the
neutrophils into five classes, based on the
number of lobes in the nucleus.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
7/79
More Important Definitions
Class I: horseshoe shape; one lobe (band)
Class II: two nuclear lobes
Class III: three nuclear lobes
Class IV: four nuclear lobes
Class V: five or more nuclear lobes
Arneth determined that younger neutrophils
had one or two nuclear lobes, and olderneutrophils had increasing number of lobes.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
8/79
More Important Definitions
Arneth found that when infection was present,
there was an increase in Class I and Class II
cells, representing an influx of less mature
neutrophils being released by the body inresponse to the toxic state.
Hence, this was termed a shift to the left.
The Arneth count determined the percentage of
each type of neutrophil in Class I Class V.
While the Arneth count is no longer used today,
the term left shift has endured.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
9/79
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
10/79
Lets try to calculate the absoluteneutrophil count (ANC)
Mrs. S. is a 42-year-old female with recent onset leukopenia.
On recent CBC, she was noted to have:
Total WBC: 1,800 and Differential: [38S 2B 54L 2M 1E 1BAS]
[38% segs, 2% bands, 54% lymphs, 2% monos, 1% eos,
1% basos]
ANC = [Total WBC x (% segmented neutrophils + % bands)]
ANC = [1,800 x (38% + 2%)] = [1,800 x 0.40] = 720
Based on this information, is Mrs. S. neutropenic?
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
11/79
Life Cycle of the Neutrophil
Phase I: Bone Marrow
10-14 daysPhase II: Peripheral Blood
life of peripheral blood neutrophils is 6-10 hoursPhase III: Tissue Phase
2-4 daysNeutrophils not actively involved in an inflammatoryresponse in the tissue will die (apoptosis).
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
12/79
Life Cycle of the Neutrophil
Phase One: Bone Marrow Phase
Takes approximate 10-14 days
Most of the bodys neutrophil pool exists in the bone marrow
As neutrophils mature, they develop the capacity to enter thebloodstream due to increased deformability and changes in
adhesion proteins on surface membranes Stimulation of neutrophil release from the bone marrow with G-
CSF*, GM-CSF**, corticosteroids, or endotoxin administration canresult in doubling or tripling of the blood neutrophil count within3-5 hours.Ref: Scientific American Web MD 2002
*Granulocyte colony stimulating factor
**Granulocyte monocyte colony stimulating factor
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
13/79
Life Cycle of the Neutrophil
Phase Two: Peripheral Blood Phase
Blood half-life of neutrophils is approximately 6-10 hours
In a healthy individual, ~ 5% of the bodys total neutrophils are in theperipheral blood at any given time. The remaining neutrophils (~ 95% of thetotal body neutrophils) reside in the bone marrow, ready to be released inthe event of bacterial infection or other trigger (e.g., G-CSF)
Within the peripheral blood compartment, the neutrophils are equallydivided between the circulating pooland the marginating pool
Cells in the marginating poolcan be swept into the circulation withinminutes by:
a) endogenous or exogenous epinephrine
b) as a result of exercise
c) any cause of cardiac outputThis response is known as demargination, and is also quickly reversible.
The process whereby cells in the c i rculat ing poo lenter the marginat ingpoo lis known as margination.
Ref: Scientific American Web MD 2002
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
14/79
Equilibrium between circulating pool and
marginating pool neutrophils
Peripheral Blood Neutrophils
Circulating pool Marginating pool
At any given time, the number of neutrophils
in the circulating pool is approximatelyequal to the number of neutrophils in the
marginating pool.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
15/79
http://www.ndsu.nodak.edu/instruct/tcolvill/435/hematopoiesis.htm
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
16/79
Life Cycle of the Neutrophil
Phase Three: Tissue phase
Neutrophils in the marginating pool leave the blood and enter thetissues by migrating between endothelial cells and penetrating thecapillary basement membrane. They remain in the tissues for 2-4days.
It is believed that neutrophils that are not actively engaged in anextravascular inflammatory process will die by a process known asapoptosis, in the blood or bone marrow. This is a process wherecell death occurs by a predetermined sequence of events, resultingin elimination of the cell without releasing harmful substances intothe surrounding area.
Ref: Scientific American Web MD 2002
Ref: http://www.medterms.com/script/main/art.asp?articlekey=11287
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
17/79
Endothelial cells
Almost all tissues depend on a blood supply, and the blood supply dependson endothelial cells, which form the linings of the blood vessels.
The largest blood vessels are arteries and veins, which have a thick, toughwall of connective tissue and many layers of smooth muscle cells.
The wall is lined by an exceedingly thin single sheet of endothelial cells,the endothel ium, separated from the surrounding outer layers by a basallamina.
Endothelial cells line the entire vascular system, from the heart to the
smallest capillary, and control the passage of materialsand the transit ofwhite blood cellsinto and out of the bloodstream.
Ref: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=mboc4.section.4126
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
18/79
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
19/79
http://home.ccr.cancer.gov/connections/features3.asp
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
20/79
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
21/79
Causes of Neutropenia
Increased Neutrophil Destruction Primary autoimmune neutropenia
Secondary autoimmune neutropenia
Drug induced neutropenia
Decreased or Ineffective Neutrophil Production Megaloblastic Anemia
Drug-induced decreased or ineffective neutrophil production
Infections
Congenital defects
Chronic idiopathic neutropenia (CIN) Cyclic neutropenia
T-cell lymphocyte induced
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
22/79
Causes of Neutropenia
Abnormal Distribution
Sequestration of Neutrophils
Margination of Neutrophils
Miscellaneous or Combination Causes
Pseudoneutropenia
Benign chronic neutropenia (including ethnic neutrop enia
variant)
Complement-activated neutropenia
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
23/79
Quick Review: Causes of Neutropenia
Increased neutrophil destruction
Decreased or ineffective neutrophil
production
Abnormal distribution
Miscellaneous or combination causes
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
24/79
Causes of Neutropenia: Increased
Neutrophil Destruction
Autoimmune neutropenia:
In autoimmune neutropenia, the body developsantibodies to white blood cells (WBCs). This can be dueto either a pr imaryor secondarydisorder.
Primary autoimmune neutropenia (AIN) is a raredisorder, and most often is diagnosed in early childhood,with the average age of onset of 6-12 months. Infectionsare typically mild or moderate; serious infections areuncommon. Spontaneous remission occurs in 95% ofcases of childhood AIN within 2 years.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
25/79
Causes of Neutropenia: Increased
Neutrophil Destruction
Secondary autoimmune neutropenia:
Antineutrophil antibodies have been reported in conjunction withother autoimmune disorders including systemic lupuserythemotosus (SLE), and rheumatoid arthritis (RA).
Approximately 50% of patients with SLE will develop neutropenia,although less than 5% of patients with SLE develop severeneutropenia.
Only ~ 1% of patients with RA will develop Feltys syndrome, andthese patients may be at increased risk for non-Hodgkinslymphoma.
Feltys syndrome = triad of RA + splenomegaly + neutropenia.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
26/79
Causes of Neutropenia: Increased
Neutrophil Destruction
Drug-induced increased neutrophildestruction:
Many different drugs can cause this type of
neutropenia, but antibiotics are most commonlyimplicated. Examples include: sulfa-containingmedications, cephalosporins, and penicillins.
Ref: http://www.harrisonpractice.com/practice/ub/view/Harrisons_Practice/Neutropenia/141535
http://www.harrisonpractice.com/practice/ub/view/Harrison%E2%80%99s_Practice/Neutropenia/141535http://www.harrisonpractice.com/practice/ub/view/Harrison%E2%80%99s_Practice/Neutropenia/141535 -
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
27/79
Causes of Neutropenia: Decreased or
Ineffective Neutrophil Production
Megaloblastic anemia: Megaloblastic anemia is a type of macrocyt ic anemiacaused by
either vitamin B12 or folic acid deficiency.
Recall that vitamin B12 and folate are needed for DNA synthesis.
Folic acid or vitamin B12 deficiency may result in ineffectiveneutrophil production:
Lack of these essential cofactors interferes with nucleic acidsynthesis of myeloid precursors in the bone marrow andresults in ineffective graunulopoiesis.
Ref: Wintrobes Clinical Hematology, by Maxwell Myer Wintrobe & John P. Greer (2004)
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
28/79
Causes of Neutropenia: Decreased or
Ineffective Neutrophil Production
Drug-induced Decreased or Ineffective Neutrophil Production:
Many drugs can cause decreased neutrophil production bydirectly suppressing the bone marrow. For example,chemotherapy drugs induce a very predictable neutropenic periodrelated to both the dose of the drug and the frequency of thechemotherapy regimen being used. Other examples include:antiretroviral drugs (e.g., zidovudine), chloramphenicol, andtrimethoprim-sulfamethoxazole (Bactrim).
Drugs may selectively cause a decreased production ofneutrophils, without causing either anemia or thrombocytopenia.
Multiple mechanisms for drug-induced decreased neutrophilproduction exist, and the list of potential offending agents is quiteextensive.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
29/79
Causes of Neutropenia: Decreased or
Ineffective Neutrophil Production
Infection-associated neutropenia:
Infection is one of the most common causes of neutropenia.
There are multiple types of infections that can result in decreasedneutrophil production. For example:
a) Chronic infections such as tuberculosis, brucellosis, malaria,and typhoid fever can result in decreased neutrophil production dueto bone marrow suppression by the infection.
b) Viral infections commonly cause neutropenia in the pediatricsetting. Examples include: respiratory syncytial virus (RSV),influenza, measles, rubella, and varicella.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
30/79
Causes of Neutropenia: Decreased or
Ineffective Neutrophil Production
Infection-associated neutropenia (contd):c) Some viral agents such as those causing infectious
hepatitis and infectious mononucleosis can causeneutropenia and pancytopenia by infecting thehematologic progenitor cells in the bone marrow. This
may result in severe neutropenia.
d) Infection-related neutropenia may occur with acute andchronic bacterial, viral, parasitic, and rickettsialdiseases.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
31/79
Causes of Neutropenia: Decreased or
Ineffective Neutrophil Production
Congenital defects:
There are a number of congenital disorders that cause
neutropenia, including, but not limited to the following:
a) Severe congenital neutropenia syndrome (also known as
Kostmann syndrome)b) Shwachman-Diamond syndrome (neutropenia, short stature,
pancreatic insufficiency, skeletal abnormalities, developmental
retardation)
c) Chdiak-Higashi syndrome (neutropenia, oculocutaneous
albinism)d) Cartilage-Hair Hypoplasia syndrome (neutropenia, short-limbed
dwarfism, fine hair)
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
32/79
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
33/79
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
34/79
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
35/79
Causes of Neutropenia: Decreased or
Ineffective Neutrophil Production
Chronic idiopathic neutropenia (CIN): There are a number offactors that help to distinguish CIN from other chronic neutropenicstates:
Acquired disorder that typically follows a benign and uncomplicatedcourse.
Median age at diagnosis is 50 years; female:male ratio of 3-6:1
May occur during childhood; with only slight female predominance inpatients < 18 years old
ANC < 1500 for more than three months
No clinical evidence of underlying disease that could be associatedwith neutropenia
No history of exposure to radiation, use of chemical compounds, orintake of drugs that could potentially cause neutropenia
Normal bone marrow karyotype analysis
Absence of antineutrophil antibodies
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
36/79
Causes of Neutropenia: Decreased or
Ineffective Neutrophil Production
. Cyclic neutropenia:
This is an autosomal dominant trait with variable degrees of
expression. While it may often present during childhood, it can also
present during adulthood.
Typically, this disorder is manifested by predictable periods of
neutropenia approximately every 21 days, lasting 3-4 days.
The patient may complain of mouth sores, malaise, and fatigue.
The patient may also develop bacterial infection and fever duringthese periods of neutropenia.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
37/79
Autosomal Dominant Inheritance
wikis.lib.ncsu.edu
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
38/79
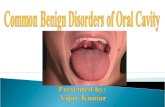
Example of Neutropenia-Related Oral
Ulcers
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
39/79
Causes of Neutropenia: Decreased or
Ineffective Neutrophil Production
T-cell lymphocyte induced neutropenia:
Studies of rheumatoid arthritis patients who are
neutropenic, have demonstrated clonal expansion of
large granular lymphocytes (T-cell lymphocytes) that
may impair neutrophil production, suggesting amultifactorial basis for the neutropenia associated with
Feltys syndrome. This lymphocytosis may gradually
evolve into a lymphoid malignancy.
Recall that patients with Feltys syndrome are atincreased risk for non-Hodgkins lymphoma.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
40/79
Causes of Benign Neutropenia: Abnormal
Neutrophil Distribution
Sequestration of neutrophils: Portal HTN When the spleen becomes congested due to portal hypertension,
the blood flow is preferentially shunted toward the spleen resulting insplenic sequestration of the blood cells with resultant cytopenias.
Examples of disorders that may cause portal HTN include:
a) Hepatic cirrhosis
b) Budd-Chiari syndrome(results from hepatic venous outflow obstruction due to thrombosis and can becaused by infections, myeloproliferative disorders, liver cancer, oralcontraceptive use, among others)
c) Splenic vein thrombosis
d) Hepatitis
e) Portal vein thrombosis
f) Splenic A-V fistula
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
41/79
Hepatic Vascular System
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
42/79
Anatomy of Various Conditions Causing
Portal HTN
http://clinicalexamprep.wordpress.com/tag/gastro/
http://clinicalexamprep.wordpress.com/tag/gastro/
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
43/79
Budd-Chiari Syndrome
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
44/79
Causes of Benign Neutropenia: Abnormal
Neutrophil Distribution
Sequestration of neutrophils: Splenic trapping of neutrophils due
to infection:
In cases of parasitic infections causing splenomegaly, such as acute
malaria, splenic sequestration and accelerated destruction of
neutrophils can cause a resultant neutropenia.
Sequestration of neutrophils: Feltys syndrome:
Recall that splenomegaly is associated with Feltys syndrome. As a
result of the splenomegaly, there can be splenic trapping ofneutrophils and accelerated destruction. These factors contribute to
the multi-factorial neutropenia seen in Feltys syndrome.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
45/79
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
46/79
Causes of Neutropenia: Abnormal
Neutrophil Distribution
Margination of neutrophils:
Severe bacterial infections release endotoxin into the
bloodstream causing margination, which results in the
neutrophils remaining in the infected tissues and notreturning to the bloodstream, especially in patients with
already depleted bone marrow reserve due to prior
chemotherapy, other drugs, or alcohol. If a patient w ith
a severe bacter ial infect ion has a low neutro ph i lcou nt, th is is a grave prognost ic sign.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
47/79
Causes of Neutropenia: Miscellaneous and
Combination Causes
Pseudoneutropenia:
Interestingly, in situations where a patient suffers from chronic anxiety or
other underlying emotional disorder, such as anorexia nervosa, a significant
chronic neutropenia may occur. However, despite the low neutrophil count,
there is no history of recurrent infection. The total body neutrophil pool is
normal, however, a larger portion of their neutrophils are in the marginatingpool rather than the circulating pool. This type of neutropenia is termed
pseudoneutropenia.
In these patients, there may be a dramatic response to epinephrine. Recall
that epinephrine is one of the stiumuli than can cause demargination,
resulting in the movement of neutrophils from the marginating pool to the
circulating pool. Therefore, there is no indication for further evaluation
and treatment of this condition.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
48/79
Causes of Neutropenia: Miscellaneous and
Combination CausesBenign chronic neutropenia (BCN):
This condition often begins within the first two years of life (alsoknown as pediatr ic benign c hronic neutropenia). Most childrenare asymptomatic.
A variant of BCN involves persons who are of African, YemeniteJewish, or of Western European descent. This is sometimes termed
ethnic neutropenia. Both the total WBC and ANC may be as low as 50% of normal
levels. In stimulation tests, there is normal granulocyte reserve,suggesting that the low neutrophil count is related to the degree ofneutrophil marrow release.
Life expectancy is normal, and these patients do not generallyexperience recurrent infections.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
49/79
Causes of Neutropenia: Miscellaneous and
Combination Causes
Complement-activated neutropenia: The complement system plays an integral role in the bodys defense
against infection and in response to tissue injury. When the system is
working correctly, the complement fragments play a pivotal role in the acute
inflammatory response.
In certain situations, if there is excessive local or systemic complement
activation, the result may be to stimulate the formation of neutrophil
aggregates that are transiently sequestered in the pulmonary capillary
bed, which can result in respiratory distress.
Dialysis patients may experience this type of neutropenia, which is
thought to be stimulated by certain types of dialysis membrane.
Septic patients or patients undergoing cardiopulmonary bypass surgery
may also experience complement-activated neutropenia.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
50/79
Clinical Evaluation of New-Onset
Neutropenia of Unknown Cause:
Workup of new-onset neutropenia of unknown cause may include: CBC with differential
Examination of peripheral blood smear
Antinuclear antibody (ANA), Rheumatoid factor (RF), and antineutrophilantibody testing (to rule out underlying autoimmune disease)
Serum B12 and folate levels (to rule out meglaoblastic anemia)
Serial CBC with differential (ANC calculated serially in cyclic neutropenia) Assess spleen size (liver/spleen scan, CT scan, or ultrasound to rule out
splenic sequestration)
Obtain bone marrow aspirate and biopsy (to rule out underlying bonemarrow disorders or malignancy)
Epinephrine and prednisone mobilization tests (if suspect benign chronic
neutropenia or pseudoneutropenia) though in clinical practice, thesetests are not routinely done
Complete medication history is required (to rule out drug-inducedneutropenia)
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
51/79
Clinical Evaluation of New-Onset
Neutropenia of Unknown Cause:
Important Questions to Consider:
Is the patient of African American or Yemenite Jewish descent?
Has the patient had recent surgery (CABG) or hemodialysis?
Is the patient septic? Has the patient had a recent acute illness or infection?
Is there a family history of cyclic neutropenia?
Is there a family history of congenital syndromes associatedwith neutropenia?
Does the patient have an underlying emotional disorder(e.g.,anorexia nervosa or chronic anxiety)?
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
52/79
Treatment of the Afebrile Neutropenic
Patient:
The most appropriate treatment is to address theunderlying condition:
In cases of hypersplenism (enlarged spleenaccompanied by decrease in one or more blood celllines), if it can be determined with a significant degree of
clinical certainty that the enlarged spleen is the likelycause of the neutropenia, splenectomy may be helpful.
In Feltys syndrome, 80-90% of patients will respond tosplenectomy, though the result is generally transient. Atleast 30% of the patients relapse, and even among those
with normalization of the neutrophil count, recurrentinfections still may occur in 1/3 of these patients.
Recall Check: What is the clinical triad in Feltyssyndrome?
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
53/79
Treatment of the Afebrile Neutropenic
Patient:
Antibody-mediated neutropenia or lymphocyte inducedneutropenia may respond to corticosteroids.Corticosteroids cause an increase in neutrophil countwithin 4-6 hours, due to release of neutrophils from thebone marrow storage pool, and a decrease in themovement of neutrophils from the marginating pool intotissues.
Helpful hint: Corticosteroids will cause an elevated
WBC with an associated lymphopenia (decrease innumber of lymphocytes) and no left shift (i.e., bandsshould remain within normal range in absence ofinfection).
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
54/79
Treatment of the Afebrile Neutropenic
Patient:
In cases of complement-activated neutropenia, treatment withcorticosteroid (e.g., methylprednisolone) may help decrease theneutrophil aggregates and improve respiratory function.
Granulocyte-Colony Stimulating Factor (G-CSF) has been usedsuccessfully (1-5 g/kg/day) in treatment of congenital, idiopathic,
and cyclic neutropenia, and may hasten bone marrow recoveryfollowing chemotherapy.
If neutropenia is mild, treatment of any underlying infection anddiscontinuation of any possible offending drugs may be all that isneeded.
However, repeat CBC with differential must be done within 1-2
weeks, since in some patients, the neutrophil count may then benormalized. If, however, the patient appears very ill, even if the ANCis approaching adequate levels, more frequent and intensive follow-up may be indicated.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
55/79
How does G-CSF Work?
Granulocyte colony stimulating factors (CSFs), which
are also known as myeloid growth factors, have been
evaluated for prophylactic use following the
administration of chemotherapy when neutropenia is
anticipated ("primary prophylaxis"), during retreatment
after a previous cycle of chemotherapy that causedneutropenic fever ("secondary prophylaxis"), and to
shorten the duration of severe chemotherapy-induced
neutropenia in patients who have neutropenia without
fever ("afebrile neutropenia). They are generally notrecommended for routine use in patients with
established fever and neutropenia. http://www.uptodate.com/contents/use-of-granulocyte-colony-stimulating-factors-in-patients-with-chemotherapy-
induced-neutropenia
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
56/79
How does G-CSF Work?
Because of the potential sensitivity of rapidly dividing
myeloid cells to cytotoxic chemotherapy, growth factors
should be discontinued several days before the next
chemotherapy treatment and they should not be given
on the same day as chemotherapy. Experience from
clinical trials indicates that myelosuppression ismore profound if the myeloid growth factors were
given immediately prior to or on the same day as the
chemotherapy. For the same reason, growth factors
should not be given concurrently with radiation therapydirected at portals containing active marrow.
http://www.uptodate.com/contents/use-of-granulocyte-colony-stimulating-factors-in-patients-with-chemotherapy-
induced-neutropenia
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
57/79
How does G-CSF Work?
G-CSF is generally started 24-72 hours
after cessation of chemotherapy, and often
continued with twice weekly CBC
monitoring until after the WBC nadir hasbeen reached, and recovery of neutrophil
counts has begun.
It is important not to prematurelydiscontinue G-CSF before the WBC nadir
has been reached.
Cli i l P t ti f th F b il
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
58/79
Clinical Presentation of the Febrile
Neutropenic Patient:
Signs/symptoms:
Regardless of the underlying mechanism for neutropenia, the
presenting signs and symptoms may be similar.
Recall that since there is a very diminished number of neutrophils in
the peripheral blood, the patient may not have sufficient neutrophilsto make an inflammatory response such as an infiltrate on CXR, or
pus in an abscess.
The only presenting symptoms may be feverand malaise.
In a neutropenic patient, any fever exceeding 100.4F (38C) is
significant. There may be other signs and symptoms of underlying infections
such as shaking chills, skin breakdown (indicating a possible
portal of entry for infection), hypotension, productive cough,
urinary symptoms, among others.
Cli i l Hi t f th F b il
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
59/79
Clinical History of the Febrile
Neutropenic Patient:
Important Questions to Consider: Has the patient undergone any recent invasive procedure (e.g., Foley
catheter placement, peripheral or central venous catheter placement)?
Has the patient undergone any recent chemotherapy? When was Day 1of treatment? (The WBC nadir is typically 10-14 days after the start of thechemotherapy cycle, depending on the agents that are used).
Has the patient been receiving any recent antibiotic treatment that couldaffect culture results? When was the most recent dose of the antibiotic?
Has the patient recently started on any new non-chemotherapy drugsthat may be causing neutropenia? If so, any potential offending agentshould be discontinued if possible.
Di ti E l ti f th F b il
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
60/79
Diagnostic Evaluation of the Febrile
Neutropenic Patient:
Complete physical examination with close attention toany indwelling catheter sites, areas of skinbreakdown/cellulitis, oral exam to assess for oral ulcers
or abscesses, and perianal exam to visually inspect forany evidence of a perirectal abscess.
Note that the perirectal examination must be done verycarefully. A digital rectal exam should NEVER be
performed in a neutropenic patient, due to the concernthat bacteria from the area could enter the bloodstream ifany localized trauma to the area occurred as a result ofthe exam, or if skin breakdown was already present.
Di ti E l ti f th F b il
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
61/79
Diagnostic Evaluation of the Febrile
Neutropenic Patient:
As noted above, since findings suggesting a source of infection maybe lacking due to the neutropenic state, you must obtain culturesfrom any possible source of infection. Typically, this wouldinclude:
a) Two sets of blood cultures [Note: If patient has anindwelling venous catheter, it is often helpful to obtain oneset from the peripheral blood and one set from anyindwelling venous catheter]
b) Urine for urinalysis and culture
c) Sputum (if patient has productive cough): for gram stain andculture
d) CXRe) Stool (if patient presents with abdominal pain and diarrhea):for ova and parasites (O & P), stool culture for entericpathogens, and C. diff toxin testing.
E i i A tibi ti T t t f th
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
62/79
Empiric Antibiotic Treatment of the
Febrile Neutropenic Patient:
Empiric broad-spectrum antibiotic treatment shouldbe initiated immediately after obtaining all necessarycultures. Delay in start ing appropriate antibiot iccoverage can be l i fe-threatening fo r the febri lepat ient wi th signi f icant neutropenia
.
In absence of a known source, it is suggested thatcoverage include broad gram-negative coverage (toinclude Pseudomonas aeur ig ino sa) and gram-
positive cocci (to include alpha-hemolyticstreptococcus). Vancomycin is also often added initially,if there is suspicion of a skin source of infection (such asan indwelling catheter site), particularly if the patient isclinically unstable.
E i i A tibi ti T t t f th
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
63/79
Empiric Antibiotic Treatment of the
Febrile Neutropenic Patient:
Examples of empiric antibiotic regimens for neutropenic fever:
Monotherapy:
Ceftazadime OR Cefepime [+ Vancomycin (if clinically indicated)]
Combination therapy:
Aminoglycoside + [antipseudomonal PCN orcefepime orceftazadime or carbapenem]
---------------------------------------------------------------------------------
Aminoglycoside commonly used: Gentamicin
Antipseudomonal PCNs include: Ticarcillin, Piperacillin, Carbenicillin
Carbapenems include: Imipenem, Meropenem
N t i P ti d T t t
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
64/79
Neutropenic Precuations and Treatment
of the Neutropenic Febrile Patient:
Neutropenic precautions should be initiated at the time of admission: Private room for the patient
Reverse isolation for all caregivers of the patient, particularly if ill
Avoid use of humidifiers or humidified oxygen, due to risk of bacterialcontamination with standing water source
Use sterile technique with venous access devices
Avoid or minimize invasive techniques when possible No fresh flowers in patient room (due to risk of fungal contamination)
No fresh fruits or raw vegetables (due to risk of exposure to gram-negativebacteria in these foods)
Meticulous handwashing immediately before entering room and immediatelyafter exiting from room
Use soft swabs for oral care; avoid toothbrushing while neutropenic
Stool softener (to prevent perirectal skin trauma during bowel movement)
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
65/79
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
66/79
Causes of Benign Neutrophilia
Increased production of neutrophils Accelerated release of neutrophils from the bone marrow
storage pool into the peripheral blood, in response toinfection, inflammation, corticosteroids, or colony
stimulating factors (e.g., G-CSF, GM-CSF) Shift from the marginating pool to the circulating poolof neutrophils (demarginiation); rarely more than a two-fold increase
Reduced movement of neutrophils from the peripheral
blood to the tissues A combination of these mechanisms
Causes of Benign Neutrophilia:
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
67/79
Causes of Benign Neutrophilia:
Increased Production of Neutrophils
Increased bone marrow production of neutrophils may be due to:
Cigarette smoking (due to underlying inflammation of the
ariways/lungs); the average neutrophil count of people who smoke 2
packs of cigarettes/day is twice normal.
Even after cessation of smoking, the total WBC may remain
elevated for up to several years, possibly due to underlying
smoking-related inflammation.
Infections- may occur with localized and systemic acute bacterial,
mycotic, rickettsial, spirochetal, and certain viral infections.
Inflammatory conditions (e.g., vasculitis, gout)
Tissue necrosis (e.g., burns, following acute myocardial infarction,
pulmonary infarction, or renal infarction)
Trauma (includes surgery)
Drug-induced (e.g., lithium)
Causes of Benign Neutrophilia: Increased
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
68/79
Causes of Benign Neutrophilia: Increased
Peripheral Distribution of Neutrophils
Impaired movement of neutrophils from peripheral blood into tissues:
Glucocorticoids*
*multifactorial process also includes release of neutrophils from bone marrow
storage pool and demargination
Reduction in marginating pool with increase in circulating pool:
Exercise-induced neutrophilia (causes demargination; as endogenous
epinephrine shifts cells from marginating pool into circulating pool)
Emotional stress
Seizures
Increased peripheral distribution post-splenectomy: Since the spleen is no longer available as a reservoir for blood cells, there
will be an increase in the number of circulating neutrophils in patients after
the spleen has been removed.
Causes of Benign Neutrophilia:
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
69/79
Causes of Benign Neutrophilia:
Leukemoid Reactions
Leukemoid reactions may occur due to:
Sepsis
Hemorrhagic shock
Severe tissue injury
Secondary to congenital abnormalities (e.g., Down
syndrome [trisomy 21])
Leukemoid reaction:
Total WBC may exceed 30K-50K, mimicking leukemia;hence the name leukemoid
Leukocyte alkaline phosphatase (LAP) score is normal
or high in leukemoid reaction, and low or zero in
chronic myelogenous leukemia (CML)
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
70/79
How Is the LAP Score Determined?
The test detects the activity of alkalinephosphatase in the cytoplasm ofneutrophils (segs + bands)
100 neutrophils are evaluated and gradedon a scale of 0-4+, based on the quantityand intensity of the alkaline phosphataseactivity in each cell. The total is
determined based on the sum of the gradefor each of these cells.
Example of Leukocyte Alkaline Phosphatase
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
71/79
Example of Leukocyte Alkaline Phosphatase
(LAP) Score in Leukemoid Reaction and CML
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
72/79
LAP SCORE IN CLINICAL PRACTICE
While LAP Score has previously been used todifferentiate between leukemoid reaction andChronic Myelogenous Leukemia (CML), the testis subject to interpretation and test results are
difficult to reproduce, based on technicalvariability.
Currently, although this test remains available insome clinical laboratories, most facilities are
relying on additional molecular and cytogenetictesting for the presence of CML, thus eliminatingthe possibility of leukemoid reaction.
Causes of Benign Neutrophilia:
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
73/79
Causes of Benign Neutrophilia:
Miscellaneous Other Causes
Miscellaneous other causes of benign neutrophilia:
Hereditary neutrophilia (rare)
Idiopathic neutrophilia (rare)
Leukocyte adhesion deficiency (rare)
Familial cold urticaria and leukocytosis (rare)
Approach to Patients with Benign
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
74/79
Approach to Patients with Benign
Neutrophilia:
Signs and symptoms: May be immediately apparent what underlying process is causing the
neutrophilia and specific signs and symptoms would be associated with thatcondition.
Findings on exam that may be helpful include splenomegaly (considermyeloproliferative process)
Diagnostic tests:
Peripheral blood smear: look for evidence of immature WBCs circulating inthe peripheral blood, which may suggest leukemia. Toxic granulations orDohle bodies suggest serious underlying bacterial infection
Leukocyte alkaline phosphatase (LAP) score: should typically be elevatedwith a leukemoid reaction and low or absent in the setting of CML
Treatment of neutrophilia:
Except for the presence of an underlying myeloproliferative process,treatment of benign neutrophilia is generally not indicated. The neutrophiliawill generally resolve once the underlying inflammatory process resolves.Hereditary and idiopathic neutrophilia are quite rare and follow a benigncourse.
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
75/79
Now, lets put it all together.
Case #1: 56 year-old with fever
Case #2: 42-year-old for routine exam
Case #3: 72-year-old with low WBC
Case #4: 34-year-old follow up HTN
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
76/79
Case #1:A 56-year-old male currently undergoing chemotherapy fornon-small cell lung cancer, presents for evaluation of new-onset fever. He is currently on Day #10 of his chemotherapycycle. He reports that his temperature was 101F at homeearlier today. What important questions should you ask him
when taking the history, while you are waiting for his CBCresults?
The CBC results are as follows:
WBC: 1, 200
Hgb: 10.8 g/dL
HCT: 34%
MCV: 90Plt: 140,000
Diff: 42% segs, 4% bands, 46% lymphs, 4% monos, 2% eos, 2%baso
Calculate the absolute neutrophil count (ANC): ________
Is this patient neutropenic?
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
77/79
Case #2:
A 42-year-old female with no significant PMH, presents for a routinephysical when changing medical providers. She reports that she hasnot been to her primary care doctor in the past 5 years, so baselinelaboratory testing is done. CBC with diff is ordered and the results
reveal an elevated neutrophil count of 11,400. She denies recent acuteillness and is currently without complaints. The patient denies PMH ofcigarette smoking, frequent vigorous exercise, or increased stress.She is currently not taking any prescription medications or over-the-counter herbal remedies or supplements. She states that she wasinvolved in a motor vehicle accident several years ago and requiredhospitalization.
What do you suspect is the most likely cause of the neutrophilia inthis patient?
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
78/79
Case #3:
Patient is a 72-year-old male who presents for evaluation of
new-onset neutropenia. He was noted to have a total WBC
2,800 (ANC = 1,200). The patients PMH is significant forrheumatoid arthritis for the past 12 years. The patient denies
any recent acute viral or bacterial illness and denies fever.
Based on this information, what important diagnostic clues
would you look for on physical examination? What initiallaboratory tests would you order?
-
8/10/2019 BENIGN DISORDERS OF WHITE BLOOD CELLS102314 (1).pdf
79/79
Case #4:Patient is a 34-year-old male who presents to a new medical providerfor follow-up of his HTN and review of his recent blood work. Hereports feeling entirely well, and is afebrile on exam. His CBC resultsare as follows:
WBC: 3,000
Hgb: 14.8 g/dL
HCT: 45%
MCV: 84
Plt: 180,000
Diff: 44% segs, 3% bands, 45% lymphs, 4% monos, 2% eos, 2% baso
Based on this information, calculate the absolute neutrophil count(ANC): __________
What are some possible underlying causes of this patientsneutropenia? What initial tests would you order? How would youtreat this patient?