Benign Diseases of Cervix, Uterus & Ovary
58
Benign Diseases of Cervix, Uterus & Ovary
-
Upload
ahmad-faheem-hassan -
Category
Documents
-
view
15 -
download
2
description
obstetrics & gynaecology
Transcript of Benign Diseases of Cervix, Uterus & Ovary

Benign Diseases of Cervix, Uterus &
Ovary
Benign Disease of Cervix

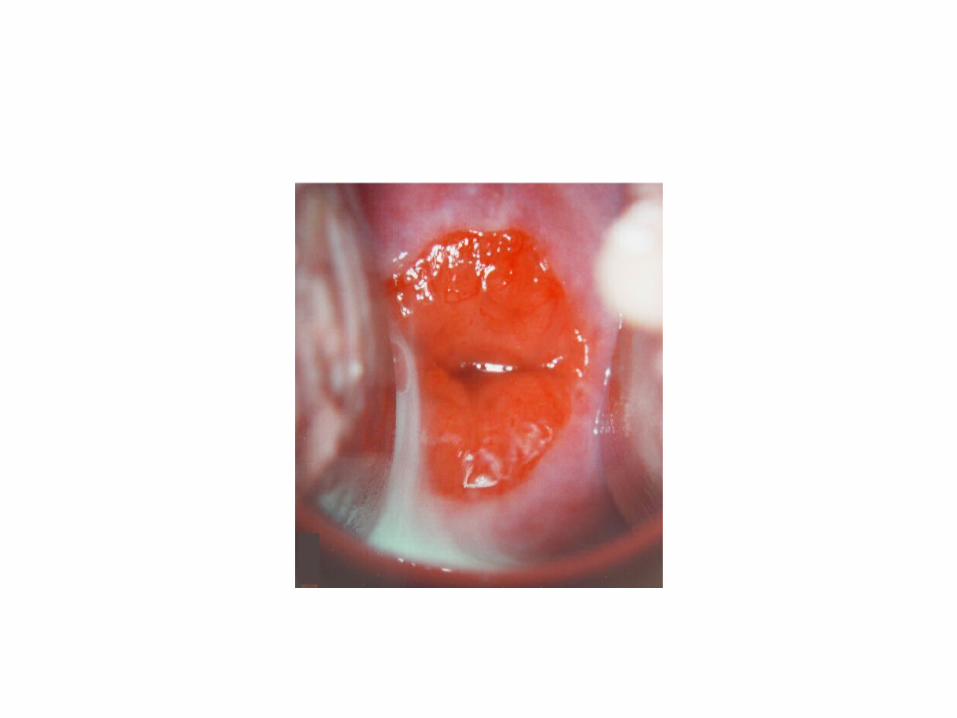
Cervical Ectropion


Formation
Squamocolumnar junction is located at the external os
before puberty
As estrogen levels rise during puberty, the cervical os opens,
exposing the endocervical columnar epithelium onto the
ectocervix
This area of columnar cells on the ectocervix forms an area
that is red and raw in appearance called an
ectropion (cervical erosion).
It is then exposed to the acidic environment of the vagina and, through a process of
squamous metaplasia, transforms into stratified
squamous epithelium

Causes
• Puberty• During pregnancy• Oral contraceptive pill• Congenital • Sexual intercourse
Signs and Symptoms
• Excessive but non-purulent vaginal discharge• Post-coital bleeding

Treatment
• No treatment for asymptomatic• Hormonal therapy• Discontinuing oral contraceptives • Ablation treatment
Cervical Stenosis

Definition
• The endocervical canal is more narrow than is typical. In some cases, the endocervical canal may be completely closed.

Symptoms
Before menopause• Menstrual abnormalities• Amenorrhea, dysmenorrhea and abnormal bleeding.
• Infertility After menopause• Not cause symptomsA hematometra or pyometra can cause pain or cause the uterus to bulge

Causes
• congenital cervical stenosis• chronic infection (chronic cervicitis)• trauma
• from previous instrumentation• cone biopsy/loop electrosurgical excision procedures (LEEP) • cryotherapy• laser treatment
• stenosis secondary to a tumour/mass: • cervical polyp• carcinoma of the cervix
• post radiation therapy• cervical endometriosis

Investigation
• Hysterosalpingogram• narrowing of the endocervical canal (normal diameter:
0.5-3.0 cm)• complete obliteration of the cervical os, preventing
insertion of the hysterosalpingographic catheter.
• Pelvic ultrasound• visualisation of an underlying mass if its complicated by
proximal dilatation of the female genital tract (e.g. hematometra)

Treatment
• Vaginal delivery of a baby• Insertion of dilators with ultrasound guidance• Laser treatment if caused by scar tissue• Hysteroscopic shaving of cervical tissue

Cervical Intraepithelial Neoplasia• Potentially premalignant transformation and
abnormal growth (dysplasia) of squamous cells on the surface of the cervix.• May progress to become cervical cancer, usually
cervical squamous cell carcinoma (SCC)• Major cause - human papillomavirus (HPV) 16, 18

Risk Factors
• Infected by a high risk type of HPV, such as 16, 18, 31, or 33• Immunodeficient • Women who give birth before age 17• Poor diet• Multiple sexual partners• Lack of condom use• Cigarette smoking.

Classification
Sign and Symptoms
• Usually causes no symptoms, and is most often discovered by a routine Pap test. • The prognosis is excellent for who receive
appropriate follow-up and treatment. • But women who go undiagnosed or who don't
receive appropriate care are at higher risk of developing cervical cancer.

Pap Smear
• Cells are collected from the cervical surface and examined under microscope to look for the signs of abnormal and cancerous cells • In Malaysia, all women who are, or who have been
sexually active, between the ages of 20 and 65 years, are recommended to undergo Pap smear testing. • If the first two consecutive Pap results are negative,
screening every three years is recommended.

Management
• CIN 1 – Conservative • CIN 2, 3 & persistent CIN 1 (more than 1 year)• Surgical
• Loop electrosurgical excision procedure (LEEP)• Cold knife conization• Laser vaporization and cryotherapy
Prevention - Vaccine (13 year-old girls)• Gardasil (HPV 16, 18)• Cervarix (HPV 16, 18, 6, 11)


Endometrial Polyps&
Asherman syndrome

Endometrial Polyps
• Discrete outgrowth of endometrium, attached by a pedicle which move with the flow of the distension medium.
• It may be pedunculated or sessile, single or multiple and vary in size. (0.5-4 cm)
• Women under 40 years old unlikely to have this.
• May cause intermenstrual bleeding and treatment is by removal if the symptoms persistent at least 3 months or more.

• Women more than 40 years old & pre-menaupausal and have endometrial polyps that diagnosed by ultrasound or hysteroscopy. Should consider removal of the polyps.
• Increasing in age, most common abnormality is endometrial hyperplasia which can present in just the endometrial polyps tissue.
• Post-menopausally, mandatory to remove endometrial polyps which can be due hyperplasia or malignancy.
• Polyps can also caused by tamoxfen (drug) to treat breast cancer.
• Most cases, polyps are benign but removal is necessary to prevent possibility of malignancy.

Signs of uterine polyps include:• Irregular menstrual bleeding — for example, having
frequent, unpredictable periods of variable length and heaviness
• Bleeding between menstrual periods
• Excessively heavy menstrual periods
• Vaginal bleeding after menopause

Investigation:
• Transvaginal ultrasoud
• Hysteroscopy
• Curretage

Treatments
• Watchful waiting. Small polyps without symptoms (asymptomatic) may resolve on their own. Treatment is unnecessary unless you're at risk of uterine cancer.
• Medication. Certain hormonal medications, including progestins and gonadotropin-releasing hormone agonists, may shrink a uterine polyp and lessen symptoms.
• Curettage

Asherman Syndrome• An irreversible damage of the single layer thick basal
endometrium does not allow normal regeneration of endometrium.
• It undergoes fibrosis and adhesion formation termed “Asherman Syndrome”
• Result is reduced or absent menstrual shedding.
• Can happen because of overzealous curettage of the uterine cavity during evacuation of retained product of conception after miscarriage

Causes:
• DNC
• Tuberculosis & schistosomiasis

Symptoms:
• The adhesions may cause amenorrhea (lack of menstrual periods), repeated miscarriages, and infertility.
• However, such symptoms could be related to several conditions. They are more likely to indicate Asherman syndrome if they occur suddenly after a D&C or other uterine surgery.

Investigation:
A pelvic exam is usually normal.
Tests may include:• Blood tests to detect tuberculosis or
schistosomiasis• Hysteroscopy• Hysterosonogram• Infertility evaluation• Transvaginal ultrasound examination

Management:• Hysteroscopic technique to manually breakdown or
lyse the intrauterine adhession.
• After scar tissue is removed, the uterine cavity must be kept open while it heals to prevent adhesions from returning.
• Your health care provider may place a small balloon inside the uterus for several days and prescribe estrogen therapy while the uterine lining heals.

• Antibiotic treatment may be necessary if there is an infection.

Uterine Fibroids

• Noncancerous growths of the uterus that often appear during childbearing years. Also called leiomyomas or myomas, uterine fibroids aren't associated with an increased risk of uterine cancer and almost never develop into cancer.
• Uterine fibroids develop from the smooth muscular tissue of the uterus (myometrium). A single cell divides repeatedly, eventually creating a firm, rubbery mass distinct from nearby tissue.
• Fibroids range in size from seedlings, undetectable by the human eye, to bulky masses that can distort and enlarge the uterus. They can be single or multiple.
• As many as 3 out of 4 women have uterine fibroids sometime during their lives, but most are unaware of them because they often cause no symptoms. Doctors may discover fibroids incidentally during a pelvic exam or prenatal ultrasound.

Sites:
• SubmucosalFibroids grow into the uterine cavity.• IntramuralFibroids grow within the wall of the uterus.• Subserosal Fibroids grow on the outside of the uterus.• Pedunculated fibroids Some fibroids grow on stalks that grow out from the surface of the uterus or into the cavity of the uterus.
Symptoms:
• Heavy menstrual bleeding• Prolonged menstrual periods — seven days or more
of menstrual bleeding• Pelvic pressure or pain• Frequent urination• Difficulty emptying bladder• Constipation

Causes:
• Genetic changes. Changes in genes that differ from those in normal uterine muscle cells. Fibroids also run in families and that identical twins are more likely to both have fibroids than non identical twins.
• Hormones. Fibroids contain more estrogen and progesterone receptors than normal uterine muscle cells do. Fibroids tend to shrink after menopause due to a decrease in hormone production.
• Other growth factors. Substances that help the body maintain tissues, such as insulin-like growth factor, may affect fibroid growth.

Risk factors:• Nulliparity• Obesity• Heredity. If your mother or sister had fibroids, you're at increased risk of developing them.• Race. Black women are more likely to have fibroids than women of other racial groups. • Other factors:Onset of menstruation at an early age, having a diet higher in red meat and lower in green vegetables and fruit, and drinking alcohol and beer.
Factors that lower the risk of fibroids:• Pregnancy (the risk decreases with increasing number of pregnancies)• Long-term use of progestin-only birth control pills or oral contraceptives• Use of the birth control shot (depot medroxyprogesterone acetate or Depo-
Provera)

Investigations:
Blood:FBC to determine if the patient has anemia duet to chronic blood loss and other blood tests to rule out bleeding disorders or thyroid problems.
Special tests:• HysterosalpingogramX-ray test that looks at the inside of the uterus and fallopian tubes and the area around them.
• Hysterosonography. (Saline infusion sonography)
Injection of salt solution into the uterus to help create the ultrasound image.
• Laparoscopy Look and locate fibroids on the outer surface of the uterus.
Imaging:• Pelvic USS• MRIShow the size and location of fibroids, identify different types of tumours and help determine appropriate treatment options.• CT SCAN

Treatments:
Conservative: Medical: Surgical:
• Emotional support
• Bed rest• Practice
healthy and balanced diet
• Pain medication• Birth control pills &
hormonal birth control pills.
These medications control heavy bleeding and painful periods.• Progestin-releasing
intrauterine device (IUD)Reduces heavy and painful bleeding but does not treat the fibroids themselves.• Gonadotropin-releasing
hormone agonists.Stop ovulation, helps in reducing the size of fibroids. • Antihormonal agents. Mifepristone, can slow or stop the growth of fibroids.
• Endometrial AblationDestroys the lining of the uterus. It is used to treat small fibroids inside the uterus.• MyomectomyThis procedure removes only the fibroids and leaves the healthy areas of the uterus intact. Preserve the ability to get pregnant.• HysterectomyCure uterine fibroids completely. Recommended if fibroids are large, very heavy bleeding, near or past menopause. • Uterine Artery Embolization cuts off the blood supply to the fibroids, causing them to shrink and be reabsorbed by your body.

Complications:
• Iron-deficiency anaemia.
• Bladder frequency, constipation (due to increased pelvic pressure).
• Torsion of pedunculated fibroid.
• Ureteral obstruction causing hydronephrosis.
• Infertility: as a result of narrowing of the isthmic portion of the Fallopian tube or as a consequence of interference with implantation (submucosal fibroids).
In pregnancy:
• Recurrent miscarriage.
• Fetal malpresentation.
• Intrauterine growth restriction.
• Premature labour.
• Postpartum haemorrhage.

• History Taking • Physical Examination
• Age: Reproductive age• Pregnancy: Nulliparity?• Menstrual History: • Early menarche?• Length of bleeding (usually
prolonged)• Intermenstrual bleeding• Bleeding after intercourse• Nature of periods:
Heavy/Clot/Flooding?• Menorrhagia, metrorrhagia• Associated symptoms:
dysmenorrhea, dyspareunia, urinary frequency/constipation
• Pelvic pain?• Diet? (high in red meat,soy)• Family history of fibroids
• Enlarged uterus extending above the symphysis pubis
• Fibroid typically has an irregular contour.• Fibroids are muscular in origin and have a
solid consistency.• They feel firmer than the uterine fundus.• During a bimanual pelvic exam,
irregularities can be palpated near the adnexa or even posterior on the uterus.
• The majority of fibroids can be palpated near the midlines, which are usually mobile.
• In cases of large tumours, a central irregular mass can be palpated on transabdominal examination.
• Enlarged uterus (>8 weeks)

Benign diseases of the ovary
Functional ovarian cystsInflammatory ovarian cysts
Germ cell tumoursEpithelial tumours
Sex cord stromal tumours
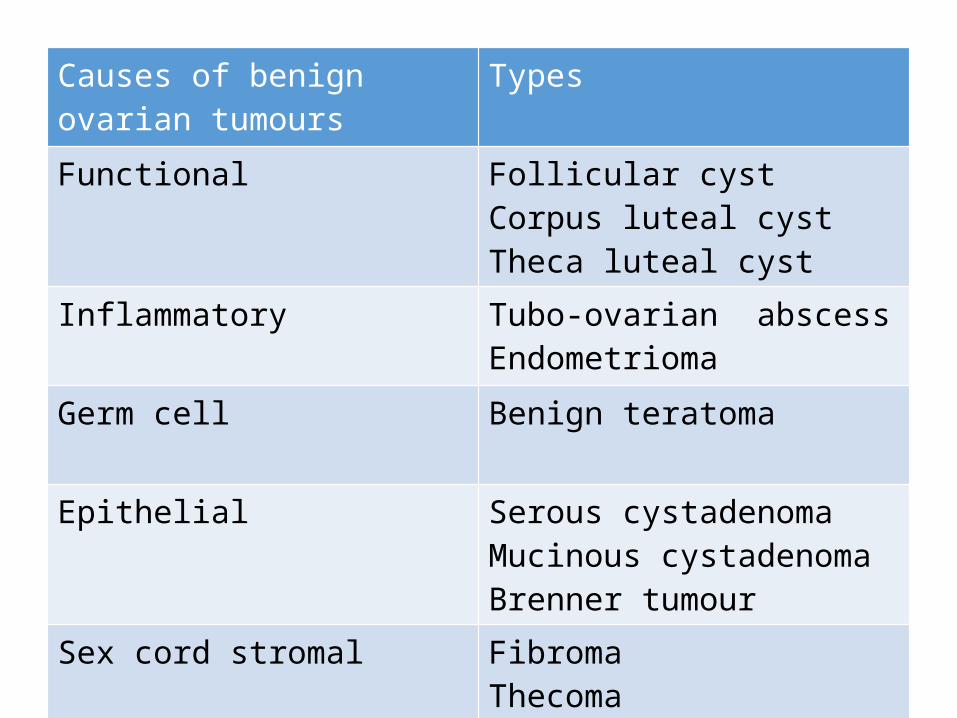
Causes of benign ovarian tumours
Types
Functional Follicular cystCorpus luteal cystTheca luteal cyst
Inflammatory Tubo-ovarian abscessEndometrioma
Germ cell Benign teratoma
Epithelial Serous cystadenomaMucinous cystadenomaBrenner tumour
Sex cord stromal FibromaThecoma

Functional ovarian cysts
Follicular Dx when cyst >3cmRarely grow >10cmUSS-simple unilocular cyst Asymptomatic- observation/ sequential repeat USSSymptomatic- laparoscopic cystectomy
Corpus luteal Following ovulation May have pain –rupture/haemorrhageMx- analgesia/ ovarian cystectomy
Theca luteal a/w pregnancy (particularly multiple pregnancy)Often dx incidentally at routine USSMost resolve spontaneously

Inflammatory ovarian cysts
• Usually a/w PID• Most common in young women• Noted as mass/ abscess• May involve ovary, tube & bowel• Occasionally can develop from other infective
causes (appendicitis, diverticulitis)• Dx : PID-based, inflammatory markers• Mx: antibiotics, surgical drainage or excision • May present with endometriomas
Germ cell tumours• Most common ovarian tumours in young women• The most common form is mature dermoid cyst
(cystic teratoma)-80%**combination of all tissue types • Can be bilateral -10%• Risk of malignant transformation is rare- <2%• Dx: usually incidental, 15% with torsion, MRI is helpful • Mx: surgical excision (cystectomy)/ complete
oophorectomy-if present with torsion

Epithelial tumours • Increase with age, most common in peri-menopausal
women
Serous cystadenomas Most common20-30% of benign tumours in women under 40Unilocular, rarely involve opposite ovary
Mucinous cystadenomas
Large multiloculatedBilateral in 10% of cases
Brenner tumours Often small, found incidentallySecrete estrogen
Sex cord stromal tumours Fibromas Most common form
Solid tumours composed of stromal cellsOlder womenOften with torsion d/t heaviness of ovaryMeig syndrome (pleural effusion, ascites, ovarian fibroma)Mx- removal of fibroma
Thecomas Oestrogen-secreting tumoursOften in post-menopause, with manifestations of excess oestrogen production (post-menopausal bleeding)May induce endometrial Ca

History
• Pain• Pelvic/ abdominal swelling (DDx??) • Pressure on bowel or bladder• Acute, intermittent pain – torsion of cyst, rupture
or haemorrhage • Age-causes vary with age

Physical Examination
• Pelvic/abdominal mass (separate from the uterus) **sometimes incidentally found in USS• Tenderness

Investigation • FBC –infection,
haemorrhage • UPT • Inflammatory markers (CRP,
WCC)• Tumour markers• Imaging- USS/ CT scans/ MRI• Diagnostic laparoscopy • Fine-needle aspiration and
cytology • alpha-fetoprotein (AFP) and
human chorionic gonadotrophin (hCG)
Management • Follow-up • Analgesic• Antibiotics• Surgical excision/
drainage