BE Healthybehealthy.baystatebanner.com/issues/2012/0405/... · 1 If there’s no history of breast...
4
Ellvera Nusum, 56, had her routine down pat. She religiously underwent yearly mammo- grams and checked her breasts monthly for any changes. She even timed her self-exams correctly — a few days after her period — when her hormone level was lower. After all, she was always taught that breast cancer begins with a lump. The fact that both her maternal grandmother and aunt were diagnosed at a young age and eventually died of breast cancer kept her vigilant. But in July 2010 she observed changes in her breast. At first she paid little attention. She had seen this before. When she breast-fed her children years ago she sometimes noticed similar symptoms. Back then she had mastitis, an inflammation of the breast tissue, which occurs most commonly in women who are breast-feeding. The symptoms eventually subsided. But not this time. The changes escalated. When her breasts became two different sizes, making it difficult to wear a bra, she knew some- thing was wrong. She visited her doctor. Without even a physical examination, the doctor came right to the point. “I know exactly what this is,” he said, and referred her for a biopsy. Nusum had inflammatory breast cancer (IBC), a rare but very aggressive form of breast cancer that tends to strike women younger than the typical age of onset and is seen more frequently in black women, according to the American Cancer Society. “I had never heard of IBC,” she said. “I had no idea there was more than one type of breast cancer.” She is not alone. Contrary to common beliefs, breast cancer is not just one disease; it’s an umbrella of many different cancers, some of which may differ considerably. As in the case of Nusum, many women initially ignore the symptoms of IBC, attributing the changes to a mosquito bite, a bruise or a transient infection. Breast cancer is the most common cancer in women and the second most deadly, trailing only lung cancer. And race matters. While the median age of diagnosis is 61, incidence rates in women under the age of 45 are higher among African Americans than whites. In addition, breast cancers diagnosed in black women are more likely to be advanced or aggressive, resulting in a poor prognosis. Overall, the incidence of breast cancer is highest in white women, but black women die of it at a greater rate. According to statistics from the National Cancer Institute, between 2004 and 2008, the U.S. death rate from breast cancer in black women was 32 per 100,000 women versus 23 per 100,000 in white women, a difference of 39 percent. Yet, many surveys indicate that black women have a high rate of breast cancer screen- ing. For instance, the Behavioral Risk Factor Surveillance System, a survey conducted by the Centers for Disease Control and Prevention, indicates that in 2008, over 87 percent of black women in Massachusetts aged 40 and older said that they had a mammogram within the past two years as compared to 85 percent of white women. In 2008, however, the death rate from breast cancer in black women in the state exceeded that in whites by 32 percent. The type of cancer is not the only factor that may contribute to poor outcomes. Disparity can be attributed to a gap between screening and fol- low-up for suspicious results. Researchers from the University of Alabama cited seven major bar- riers to following up on abnormal mammograms by black women: emotional, financial, social, religious, lack of transportation and even the vagaries of the healthcare system. But the most cited was lack of awareness or understanding of the disease itself. Regardless of the reason, survival rates differ significantly. The five-year relative survival rate of breast cancer is 90 percent for white women and 77 percent for black women. All females are at risk for breast cancer, and with each passing year, the risk increases. That’s why early detection is key. The American Cancer Society recommends that “women age 40 and older should have a mammogram every year and should continue to do so for as long as they are in good health.” Women of very high risk, for instance, those with genetic mutations, are advised to get Sponsored by Nusum, continued to page 4 BE Healthy ™ VOL. 6 • NO. 8 © April 2012 BE Healthy ™ Ellvera Nusum (left) was diagnosed with inflammatory breast cancer, a rare but aggressive type of cancer. Nusum is shown here with her mother, Ursula Lovell. (Photo courtesy of Ellvera Nusum) BREAST CANCER: Early detection still key to beating the odds Ernie Green, 73, was a force to be reckoned with on the football field. He played seven seasons for the Cleveland Browns, and has two Pro Bowl appearances under his belt. But seven years ago he had to reckon with a force that had nothing to do with football — breast cancer. He now has a clean bill of health but that was after surgery, eight rounds of chemotherapy and several years of tamoxifen to decrease the risk of recurrence. He laughs as he describes his yearly follow-up mammograms. Most men in the waiting room are there to support their wives, while Green is there patiently waiting his turn. The technicians have to clear the way for him before he goes back to avoid exposure of women in various stages of undress. He admitted that he knew that men could get breast cancer. Richard Roundtree, the actor who played the detective Shaft in three movies, was very vocal about his experience with the disease. But Green saw breast cancer a little closer to home. Two of his sisters as well as two first cousins had breast cancer. But despite the apparent genetic link, he reasoned it could not happen to him. “I was an athlete and took care of myself,” he explained. “I was doing all the right things and I wasn’t going to worry about it.” So much for being macho. By far, breast cancer is considered a woman’s dis- ease, but men are not exempt. Misperception is a big part of the problem. Men do not realize they have breasts. Actually, both males and females are born with breasts, but they grow and develop differently. At puberty, while female hormones spur the growth of the mammary gland, male hormones stem its growth. Yet, the basic anatomy remains similar. All breasts have ducts — the most common site of cancer in both men and women. According to the American Cancer Society, about 2,200 new cases of breast cancer in men are expected in 2012 and an estimated 410 deaths. Experts at one time thought breast cancer in men was more deadly than the disease in women. Recently, it was discovered that sur- vival rates are similar. The issue is that men are not look- ing or checking for breast cancer and once discovered, it is at an advanced stage when survival is lower. A study published in the Journal of Clinical Oncol- ogy in 2007, however, determined that, like breast cancer in women, black men die at a rate higher than white men. Certain factors increase the risk of breast cancer in men. It is most common between the ages of 60 and 70. Men who have a close family member with breast cancer have a greater chance of developing the disease. Those exposed to radiation or those born with a genetic defect that limits the production of male hormones are targets. Estrogen, the female hormone, impacts men as well. Men with liver disease may have lower male hormones and increased female hormones. As in women, obesity plays a part. Fat cells in males convert a male hormone into estrogen, thereby exposing Ernie Green played seven seasons with the Cleveland Browns. Green and his wife Della are known for their philanthropic work in the Dayton, Ohio area. (Photo courtesy of Ernie Green Industries, Inc.) FORMER NFL STAR RAISES AWARENESS OF BREAST CANCER IN MEN Green, continued to page 4
Transcript of BE Healthybehealthy.baystatebanner.com/issues/2012/0405/... · 1 If there’s no history of breast...

Ellvera Nusum, 56, had her routine down pat. She religiously underwent yearly mammo-grams and checked her breasts monthly for any changes. She even timed her self-exams correctly — a few days after her period — when her hormone level was lower.
After all, she was always taught that breast cancer begins with a lump. The fact that both her maternal grandmother and aunt were diagnosed at a young age and eventually died of breast cancer kept her vigilant.
But in July 2010 she observed changes in her breast. At fi rst she paid little attention. She had seen this before.
When she breast-fed her children years ago she sometimes noticed similar symptoms. Back then she had mastitis, an infl ammation of the breast tissue, which occurs most commonly in women who are breast-feeding. The symptoms eventually subsided.
But not this time. The changes escalated. When her breasts became two different sizes,
making it diffi cult to wear a bra, she knew some-thing was wrong.
She visited her doctor. Without even a physical examination, the doctor came right to the point. “I know exactly what this is,” he said, and referred her for a biopsy.
Nusum had infl ammatory breast cancer (IBC), a rare but very aggressive form of breast cancer that tends to strike women younger than the typical age of onset and is seen more frequently in black women, according to the American Cancer Society.
“I had never heard of IBC,” she said. “I had no idea there was more than one type of breast cancer.”
She is not alone. Contrary to common beliefs, breast cancer is not just one disease; it’s an umbrella of many different cancers, some of which may differ considerably. As in the case of Nusum, many women initially ignore the symptoms of IBC, attributing the changes to a mosquito bite, a bruise or a transient infection.
Breast cancer is the most common cancer in women and the second most deadly, trailing only lung cancer. And race matters. While the median age of diagnosis is 61, incidence rates in women under the age of 45 are higher among African Americans than whites.
In addition, breast cancers diagnosed in black women are more likely to be advanced or aggressive, resulting in a poor prognosis.
Overall, the incidence of breast cancer is highest in white women, but black women die of it at a greater rate. According to statistics from the National Cancer Institute, between 2004 and 2008, the U.S. death rate from breast cancer in black women was 32 per 100,000 women versus 23 per 100,000 in white women,
a difference of 39 percent.Yet, many surveys indicate that black
women have a high rate of breast cancer screen-ing. For instance, the Behavioral Risk Factor Surveillance System, a survey conducted by the Centers for Disease Control and Prevention, indicates that in 2008, over 87 percent of black women in Massachusetts aged 40 and older said that they had a mammogram within the past two years as compared to 85 percent of white women.
In 2008, however, the death rate from breast cancer in black women in the state exceeded that in whites by 32 percent.
The type of cancer is not the only factor that may contribute to poor outcomes. Disparity can be attributed to a gap between screening and fol-low-up for suspicious results. Researchers from the University of Alabama cited seven major bar-riers to following up on abnormal mammograms by black women: emotional, fi nancial, social, religious, lack of transportation and even the vagaries of the healthcare system. But the most cited was lack of awareness or understanding of the disease itself.
Regardless of the reason, survival rates differ signifi cantly. The fi ve-year relative survival rate of breast cancer is 90 percent for white women and 77 percent for black women.
All females are at risk for breast cancer, and with each passing year, the risk increases. That’s why early detection is key. The American Cancer Society recommends that “women age 40 and older should have a mammogram every year and should continue to do so for as long as they are in good health.”
Women of very high risk, for instance, those with genetic mutations, are advised to get
Sponsored by
Nusum, continued to page 4
BE Healthy™
VOL. 6 • NO. 8 © April 2012
BE Healthy™
Ellvera Nusum (left) was diagnosed with infl ammatory breast cancer, a rare but aggressive type of cancer. Nusum is shown here with her mother, Ursula Lovell. (Photo courtesy of Ellvera Nusum)
BREAST CANCER:Early detection still key to beating the odds
Ernie Green, 73, was a force to be reckoned with on the football fi eld. He played seven seasons for the Cleveland Browns, and has two Pro Bowl appearances under his belt.
But seven years ago he had to reckon with a force that had nothing to do with football — breast cancer. He now has a clean bill of health but that was after surgery, eight rounds of chemotherapy and several years of tamoxifen to decrease the risk of recurrence.
He laughs as he describes his yearly follow-up mammograms. Most men in the waiting room are there to support their wives, while Green is there patiently waiting his turn. The technicians have to clear the way for him before he goes back to avoid exposure of women in various stages of undress.
He admitted that he knew that men could get breast cancer. Richard Roundtree, the actor who played the detective Shaft in three movies, was very vocal about his experience with the disease. But Green saw breast cancer a little closer to home. Two of his sisters as well as two fi rst cousins had breast cancer. But despite the apparent genetic link, he reasoned it could not happen to him. “I was an athlete and took care of myself,” he explained. “I was doing all the right things and I wasn’t going to worry about it.”
So much for being macho.By far, breast cancer is considered a woman’s dis-
ease, but men are not exempt. Misperception is a big part of the problem. Men do not realize they have breasts.
Actually, both males and females are born with breasts, but they grow and develop differently. At puberty, while female hormones spur the growth of the mammary gland, male hormones stem its growth. Yet, the basic anatomy remains similar. All breasts have ducts — the most common site of cancer in both men and women.
According to the American Cancer Society, about 2,200 new cases of breast cancer in men are expected in 2012 and an estimated 410 deaths. Experts at one time thought breast cancer in men was more deadly than the disease in women. Recently, it was discovered that sur-vival rates are similar. The issue is that men are not look-ing or checking for breast cancer and once discovered, it is at an advanced stage when survival is lower.
A study published in the Journal of Clinical Oncol-ogy in 2007, however, determined that, like breast cancer in women, black men die at a rate higher than white men.
Certain factors increase the risk of breast cancer in men. It is most common between the ages of 60 and 70. Men who have a close family member with breast cancer have a greater chance of developing the disease. Those exposed to radiation or those born with a genetic defect that limits the production of male hormones are targets. Estrogen, the female hormone, impacts men as well. Men with liver disease may have lower male hormones and increased female hormones.
As in women, obesity plays a part. Fat cells in males convert a male hormone into estrogen, thereby exposing
Ernie Green played seven seasons with the Cleveland Browns. Green and his wife Della are known for their philanthropic work in the Dayton, Ohio area. (Photo courtesy of Ernie Green Industries, Inc.)
FORMER NFL STAR RAISES AWARENESS OF BREAST CANCER IN MEN
Green, continued to page 4

1 If there’s no history of breast cancer in your family, you don’t need to have a
mammogram.
❒ True ❒ FalseFalse. Just 5-10 percent of breast cancer cases can be traced to genetic glitches handed down through your family, says the American Cancer Society (ACS). Roughly 20-30 percent of women diagnosed with breast cancer have a family member who has had it, too. That means 70-80 percent of women who develop it have no family history of breast cancer. So mammograms are an important screening tool for all women. Talk to your doctor about when to start having mammograms and how often to have them. The answer varies depending on family history and other risk factors.
BRCA1 and BRCA2 are the most well-known gene muta-
tions affecting breast cancer risk. They raise risks for cancer of the breast, ovaries, prostate and other sites. While these gene changes are most common in people of Ashkenazi Jewish descent, they occur more often than usual in Norwegian, Dutch and Icelandic people also. African Americans are not exempt, however.
2Having a mammogram is the only way to fi nd breast cancer.
❒ True ❒ FalseFalse. Certain physical signs are warning fl ags for breast cancer. As a tumor grows, it can change how a breast looks or feels. That’s why it’s important to have regular clinical breast exams performed by your doctor or another clinician trained to check for worrisome changes, such as :
• a lump or thickened area on the breast or underarm
HELPFUL TIPS“It’s impossible to eliminate all risks for breast can-
cer,” said Dr. Jan Cook, medical director of Blue Cross Blue Shield of Massachusetts. “You can’t change family medical history, for example, or whether you had your fi rst period at an early age. But you can lower the odds for developing breast cancer by making certain healthy choices. The fi rst three do double duty by improving your overall well-being.”
BE ACTIVE. Regularly engaging in activities deemed moder-
ate (brisk walks, dancing) to vigorous (jogging, biking) lowers risk for breast cancer. The U.S. physical activity guidelines for adults recommend spreading through-out the week 150 minutes of moderate activity, or 75 minutes of vigorous activity or a mix. Start small (fi ve minutes of walking every hour) and build up.
ATTAIN A HEALTHY WEIGHT. Fat cells are a source of estrogen, a natural female
hormone. After menopause, they become the main producer of estrogen in the body and being overweight increases breast cancer risk. So does weight gain as an adult. To prevent weight gain and work toward shed-ding excess pounds if necessary, eat healthy, wholesome foods, limit calories and exercise more often. Skipping a daily can of non-diet soda, for example, cuts out 150 calories on average.
LIMIT OR AVOID ALCOHOL. The American Cancer Society recommends no
more than one drink per day for women. That’s a 12-ounce beer, 5 ounces of wine, or 1½ ounces of hard liquor (80 proof).
RETHINK HORMONE THERAPY. Hormone therapy, which is used to quell certain
symptoms of menopause, raises your risk for breast cancer. If you do have bothersome menopausal symp-toms, such as hot fl ashes or vaginal dryness, talk to your doctor about other options for handling them.
• changes in breast size or shape• dimpled or puckered skin• a nipple turning inward into the breast or leaking fl uid
other than breast milk• scaly, reddened or swollen skin on breast, nipple or
areola (the darker circle of skin around the nipple)• ridges or pitting that looks much like the skin of an
orangeWhile the American Cancer Society no longer recom-
mends doing monthly breast self-exams, it continues to em-phasize breast awareness — that is, knowing how your breasts usually look and feel as you shower or dress so that you’ll notice changes like those described above. If this happens, call your doctor for advice.
3Mammograms can fi nd every breast cancer.
❒ True ❒ FalseFalse. According to the National Cancer Institute (NCI), screen-ing mammograms may miss up to 20 percent of breast cancers in women who have no signs or symptoms. Called a false negative, this is more likely to occur in younger women, who generally have a higher proportion of dense breast tissue, which can hide tumors. That’s why it is important to have periodic clinical breast exams and to keep your mammogram appointments.
4 Mammograms cause cancer.
❒ True ❒ FalseFalse. Radiation is one cause of cancer. Like any X-ray, mammograms use radiation to form images of breast tissue. The radiation doses are very small and the risk of harm is considered low although it can potentially rise with repeated exposure. The National Cancer Institute (NCI) states that the benefi ts of mam-mography nearly always outweigh the risks.
Some people worry that bruising or even touching the breast can cause cancer. While mammograms require compression of the breast to get the clearest images, you cannot get cancer by bump-ing, bruising or touching the breast, notes the NCI.
5 All mammograms diagnose breast cancer.
❒ True ❒ FalseFalse. There are two kinds of mammograms. Screening mam-mograms check for breast cancer when a woman has no obvious signs or symptoms. Diagnostic mammograms take a closer look at a suspicious area in the breast. Neither test can actually diag-nose cancer. Only a biopsy — a procedure to remove breast cells or tissue via a hollow needle or scalpel — can do that. The cells or tissue must then be checked under a microscope for abnor-malities that indicate cancer.
MAMMOGRAMSMAMMOGRAMS Myths aboutMyths about
Got a pencil? Great! Sharpen it, please, and take this quiz on mammograms. Quite likely, you’ve heard a lot about these breast X-rays, which may detect cancer long before it can be seen or felt. Just as likely, only part of what you’ve heard is true.
BE Healthy • http://behealthy.baystatebanner.com2

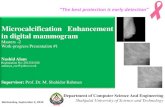
0
5
10
15
20
25
30
35
Age-
adju
sted
Dea
th R
ates
Race and ethnicity
Asian AmericanIndian
Hispanic White Black
12.215.1 17.2
22.8
32.0
Mortality rates
1. Is a lump in the breast always an indica-tor of cancer?
A breast lump in a woman is not always a sign of breast cancer. For example, benign cysts can come and go according to the menstrual cycles and these do not turn into can-cer. However, any woman who has a breast lump that does not go away after a few days should contact her health care provider to evaluate it. In addition, men who notice a breast mass should contact their doctor as well.
2. Should women do regular breast self-examinations?Currently, the professional guidelines including those from the Ameri-
can Cancer Society do not recommend that women do routine breast self-examinations, since two large randomized trials did not show a benefi t. However, if a women notices a mass in her breast that does not go away, she should contact her health care provider for evaluation.
3. If a person has a mutation in a BRCA gene does that mean that he or she will get breast cancer?
The BRCA gene is not associated with 100 percent chance of getting breast cancer. Depending upon whether the mutation is in the BRCA1 or BRCA2 gene, the lifetime risk of breast cancer for a woman ranges from 40-60 percent, according to different studies. The risk of male breast cancer is also elevated with both BRCA mutations, although the risk is higher with BRCA2 mutations. The lifetime risk of breast cancer for a male BRCA mutation carrier ranges from 1-6 percent.
4. Why is obesity correlated to the incidence of breast cancer?Although there is a clear link between obesity and increased risk of
postmenopausal breast cancer, the mechanism is not defi nitely known. One possible cause would be due to estrogen, since estrogen is mainly produced by the fat tissue in postmenopausal woman, and heavier postmenopausal women are known to have higher estrogen levels then thinner postmenopausal women. However, other mechanisms besides estrogen are probably involved as well.
5. What is the link between alcohol and breast cancer?Regular alcohol consumption has been associated with an increased
risk of breast cancer. However, low levels of consumption — three or fewer servings per week — have not been shown to be strongly related to breast cancer risk. There does not appear to be a difference by alcohol type (wine, beer or liquor) when it comes to breast cancer risk. In addition, it is long-term use that is associated with greater risk rather than short-term risk.
6. Does a father’s family history of breast cancer affect a person’s risk of breast cancer?
Yes, a father’s family history of breast cancer does affect a person’s risk of breast cancer since the BRCA1 and 2 genes can be passed to a woman or a man through either the mother or father.
7. Does breast size increase the likelihood of getting breast cancer?
Although a few studies have suggested that increased breast size may be associated with increased breast cancer risk, it is diffi cult to disentangle this from the effects of obesity. Heavier weight is associ-ated with larger breast size.
Wendy Y. Chen, M.D., M.P.H.Medical OncologistDana-Farber Cancer Institute
Questions & Answers
The information presented in BE HEALTHY is for educational purposes only, and is not intended to take the place of consultation with your private physician. We recommend that you take advantage of screenings appropriate to your age, sex, and risk factors and make timely visits to your primary care physician.
• Older age• Certain genetic mutations• A fi rst-degree relative with breast cancer• A personal history of breast cancer • Race and ethnicity
• Dense breast tissue• Previous chest radiation• Hormone replacement therapy• Obesity, particularly postmenopausal• Excessive alcohol consumption
RISK FACTORS
April 16-21 is National Minority Cancer Awareness Week
Source: Virtual Medical Centre
The female breast contains lobes, which are made up of smaller sacs called lobules, in which milk is produced. Thin tubes called ducts carry the milk from the lobules to the nipple when a woman is breastfeeding. The breast also contains vessels that carry clear fl uid, or lymph, to small, round organs called lymph nodes.
Most breast cancers begin in the ducts or lobules. Infl ammatory breast cancer infi ltrates the lymph vessels, causing noticeable changes to the breast.
When breast cancer spreads, it travels through the lymph nodes to other organs — usually the bones, liver, lungs and brain.A C
LOSE
R LOO
K
Although the incidence of breast cancer is lower in black women than in white women, between 2004 and 2008, the death rate in blacks exceeded that of all ethnicities.
The age-adjusted rates are per 100,000 women
Source: National Cancer Institute, SEER Research Data, November, 2011
Source: National Cancer Institute
Lymph
RACE MATTERS
A risk factor is a characteristic that increases a woman’s chance of getting breast cancer. Having one or more risk factors is not a guarantee that you will get the disease. In fact, many women with multiple risk factors never get breast cancer. However, having no identifi able risk factor other than gender or age does not make a women immune to breast cancer. Some of the major risk factors are:
BE Healthy • http://behealthy.baystatebanner.com 3

CELEBRATING 10 YEARS OF SERVING THE WOMEN OF BOSTON
BREAST CANCER
SCREENING101
Become familiar with how your breasts normally feel so you can detect changes.
Initiate yearly mammograms and clinical breast exams at the age of 40.
Get a yearly MRI as well as mammogram if you are at very high risk for breast cancer.
Establish a screening schedule with your doctor that accommodates your personal risk. Some people may start screening before the age of 40.Source: American Cancer Society
April is National Minority Health Month
April 10 Harvard Street Neighborhood Health Center 632 Blue Hill Ave., Dorchester April 11The Dimock Center 55 Dimock St., Roxbury April 12 South End Community Health Center 1601 Washington St., South End
April 19 Geiger Gibson Community Health Center 250 Mount Vernon St., Dorchester April 24 Bowdoin Street Health Center 230 Bowdoin St., Dorchester April 26 Mattapan Community Health Center 1425 Blue Hill Ave., Mattapan
The Dana-Farber Mammography Van comes to your neighborhood.
Have clinical breast exams — exams by a health professional — at least once every three years starting in your 20s and 30s.
Boston Public Library Cancer Awareness Display - April 1- 30Lower Mills Branch 27 Richmond Street, Dorchester
Charlestown Branch 179 Main Street, Charlestown
Grove Hall Branch 41 Geneva Avenue, Dorchester
West End Branch 151 Cambridge Street, Boston
Alternative and Complementary Health and Wellness FairApril 11, 11 a.m. — 2 p.m.University of Massachusetts BostonCampus Center, 1st Floor Terrace
NUTRITIONCook Healthy with Chef JD WalkerApril 14, 12 — 2 p.m.Twelfth Baptist Church150-160 Warren Street, Roxbury
Ethnic Cooking with Tara Mardigan, R.D.April 25, 12 — 1 p.m.Hope Lodge161 S Huntington Avenue, Jamaica Plain
Boston Organics - Differences between organic vs conventional produceAmy LevineApril 27, 12 — 1 p.m.The Historic Charles Street AME Church551 Warren Street, Roxbury
INFORMATION ON CLINICAL TRIALSMark KennedyMay 2, 12-1 p.m.Roxbury Comprehensive Health Center435 Warren Street, Roxbury
Seniors on the Move May 21, 11 a.m. — 1 p.m.Roxbury YMCA285 Martin Luther King Boulevard, Roxbury
DANA-FARBER/HARVARD CANCER CENTERINITIATIVE TO ELIMINATE CANCER DISPARITIES
All Programs are open to the public.For any additional information,please contact Athene Wilson Glover at 617-632-4860.
Cancer screening is recommended for women without breast symptoms. Screening can often detect tumors before they spread, which increases the probability of successful treatment. The Affordable Care Act mandates mammograms at no cost.
Comments on Be Healthy? Contact Health Editor Karen Miller at [email protected].
men to a greater risk of estrogen-fuelled breast cancer.
Green knew something was wrong in July 2005 when he noticed a lump in his right breast. “Initially, I didn’t think it was anything,” he said. “The last thing I thought about was breast cancer.”
That’s when his wife, Della, stepped in. He immediately saw a doc-tor, who assumed it was a cyst. The doctor explained to Green that in his 37 years of practice, he had never had a male patient with breast cancer.
Green took it one step further. It’s a good thing he did. The next doctor was not so cavalier. “It could be a cyst,” he said, “but it should not be there.” He recommended sur-gery to take a better look at it.
Green remem-bers the day well. When he woke up from surgery, the doctor was stand-ing over him with a look on his face that spelled trouble. “I have good news and bad news,” his surgeon said. The good news was that they got “it” all; the bad news was that the “it” was cancer.
Green said he fell apart. “I was never afraid of dying from football,” he said. “But I knew that people died of breast cancer.” One of his sisters had already succumbed to the disease.
The news wasn’t all that bad. His breast cancer was stage I, which meant that cancer cells had invaded surround-ing breast tissue but had not reached the lymph nodes.
Green said his eight sessions of che-motherapy were harsh and implied that getting beaten up on the football fi eld was a walk in the park in comparison.
He is not embarrassed to discuss his breast cancer; nor does he see it as a threat to his manhood.
As a matter of fact, it’s the exact opposite. He’s on a mission. He made a vow that if he could get through his treatment he would “come out” and let men know about this problem.
Green imparts words of wisdom to all men. “Do breast self-examina-
tions,” he advised, and “demand that a doctor examine your breasts as well.”
He emphasizes the importance of knowing your fam-ily tree and to look at both parents for a history of breast cancer. The ge-netic link can come from one’s mother or father. “And don’t look at just your parents,” he advised. “Find out the history of aunts and uncles and fi rst cousins.”
Green says he will keep on preach-ing. He has to. An elderly woman approached him and confessed that her husband died of breast cancer because he refused to seek treatment. Green said he wants to make sure these scenarios are not repeated. “There’s no need to get to stage III or IV if we are vigilant,” he said.
An unexpected result of his cancer is increased empathy. “I’m more sensi-tive to women’s issues,” he explained.
And that must make Della very happy.
Green, continued from page 1
an MRI as well as a mammogram. In addition, yearly breast examinations by a health profes-sional are recommended for all women.
Though it’s not possible to absolutely fend off the disease it is possible to reduce its risk by monitoring three factors — weight, physical activity and alcohol consumption.
Fat produces estrogen and many breast cancers are estrogen-based. Keeping a healthy weight thereby reduces a woman’s exposure to the hormone. The 2008 Physical Activity Guide-lines for Americans recommend 150 minutes of moderate activity, such as walking, every week. Physical activity not only improves cardiovascu-lar health, it keeps the pounds from adding up.
Too much alcohol was found to be another culprit. In a recent study published in the Jour-nal of the American Medical Association, the researchers found an increased risk of breast cancer with consumption of just three to six drinks a week.
In addition, women should consider the increased risk of breast cancer associated with combined estrogen and progestin menopausal hormone therapy use when evaluating treatment options for menopausal symptoms.
For her part, Nusum keeps a positive at-titude. Her 21-year-old daughter accompanies her for her treatments in Boston — visits that Nusum has called their “Boston Boob Adventure.”
Nusum was referred to Dr. Beth Over-moyer, the director of the Infl ammatory Breast Cancer Program at Dana-Farber Cancer Institute, and has undergone a very aggressive treatment regimen that consisted of chemotherapy, surgery, radiation and hormonal treatment. The cancer has
metastasized but is responding to therapy.Overmoyer is no stranger to IBC. “It’s
known by its very rapid onset,” she explained. “Usually three to six months.” Or even overnight. The breast becomes enlarged and red, and the skin of the breast thickens, she added.
Usually there is no mass, which causes it to escape a mammogram’s detection. “A better im-aging tool is the MRI,” she said. But she admits that a good old fashioned physical examination works well. “You can see it,” she explained.
While other types of cancers can affect one section of the breast allowing the possibility of breast-conserving surgery, IBC encompasses the entire breast. It enters the lymph vessels of the breast, which empty into the lymph nodes, allowing quick and ready access to the rest of the body. That’s how cancer cells spread. That also explains why once IBC is detected, it has pro-gressed to Stage III or Stage IV, indicating that it has moved beyond the confi nes of the breast.
IBC constitutes no more than 5 percent of all breast cancers, but, according to Overmoyer, its numbers are increasing. The problem of detecting IBC is two-pronged. Women have been educated to look for lumps — not physical changes in the breast itself. Unfortunately, because of its rarity, many doctors often do not recognize it either.
Because its symptoms mirror those of an infec-tion, the fi rst line of attack is typically antibiotics, but the results can be deceiving. “Sometimes redness waxes and wanes,” said Overmoyer. “Two weeks of antibiotics is not harmful,” she said. If the medicine has not done its job in two weeks, however, it’s best to see a surgeon that
specializes in breast care. There is some good news. A change
in order of treatment strategy has increased survival rates. When chemotherapy precedes surgery, followed by radiation and hormone treatment, the fi ve-year survival increased from about 10-15 percent to over 50 percent, according to Overmoyer.
And that is what Nusum is counting on — good news. But she is practical as well. “I put my will in order and divided up the house and jewelry,” she said. But she is not letting her IBC to get the better of her.
“I survived two divorces,” she said. “I will survive this.”
Nusum, continued from page 1
Edward W. Brooke, the fi rst African American to be elected to the Senate since the Civil War, was diagnosed with breast cancer in 2003. Brooke served two terms as the U.S. Senator from Massachusetts.
BE Healthy • http://behealthy.baystatebanner.com4
Dr. Beth Overmoyer (left) is the director of the Infl am-matory Breast Cancer Program at Dana-Farber Cancer Institute. (Photo courtesy of Dana-Farber Cancer Institute)




![Mammogram Image Feature Extraction using Pulse-Coupled ... · features in mammogram images for analysis and identification of micro calcification [3, 4]. The Pulse-Coupled Neural](https://static.fdocuments.us/doc/165x107/5f38bbc79fd88c29067e140b/mammogram-image-feature-extraction-using-pulse-coupled-features-in-mammogram.jpg)