base form page1 - webtools1.televoxsites.com · X_____ I certify that I have read and understand...
4
Patient Information Sex Name Middle First Last Insurance Information Policy Owner's Name Group No. (plan, local, or policy) Insurance Company Insurance Co. Address Insurance Phone No. General Dentist Last Visited Who may we thank for referring you to our office Policy Owner's Social Security # Home Phone Work Phone 999-999-9999 999-999-9999 E-mail No. Years Employed Occupation Employer ext. 999-99-9999 Social Security# Cell Phone 999-999-9999 Street Address Zip City State Birthdate MM-DD-YYYY Marital Status Name Middle First Last Home Phone Work Phone 999-999-9999 999-999-9999 E-mail No. Years Employed Occupation Employer ext. Cell Phone 999-999-9999 Street Address Zip City State Relationship to Patient Birthdate MM-DD-YYYY Marital Status Spouse / Additional Contact Information Policy Owner's Birthdate Relationship to Patient MM-DD-YYYY 999-99-9999 Policy Owner’s Employer Employer’s Address Policy Owner's Name Group No. (plan, local, or policy) Insurance Company Insurance Co. Address Insurance Phone No. Policy Owner's Social Security # Policy Owner's Birthdate Relationship to Patient MM-DD-YYYY 999-99-9999 Policy Owner’s Employer Employer’s Address Secondary Insurance
Transcript of base form page1 - webtools1.televoxsites.com · X_____ I certify that I have read and understand...

Patient Information
Sex
NameMiddleFirstLast
Insurance Information
Policy Owner's Name
Group No. (plan, local, or policy)Insurance Company
Insurance Co. Address Insurance Phone No.
General Dentist Last Visited
Who may we thank for referring you to our o�ce
Policy Owner's Social Security #
Home Phone Work Phone999-999-9999 999-999-9999
No. Years EmployedOccupationEmployer
ext.
999-99-9999Social Security#
Cell Phone999-999-9999
StreetAddress
ZipCity State
BirthdateMM-DD-YYYY
Marital Status
NameMiddleFirstLast
Home Phone Work Phone999-999-9999 999-999-9999
No. Years EmployedOccupationEmployer
ext.Cell Phone999-999-9999
StreetAddress
ZipCity State
Relationship to PatientBirthdateMM-DD-YYYY
Marital Status
Spouse / Additional Contact Information
Policy Owner's Birthdate Relationship to PatientMM-DD-YYYY
999-99-9999
Policy Owner’s Employer Employer’s Address
Policy Owner's Name
Group No. (plan, local, or policy)Insurance Company
Insurance Co. Address Insurance Phone No.
Policy Owner's Social Security #
Policy Owner's Birthdate Relationship to PatientMM-DD-YYYY
999-99-9999
Policy Owner’s Employer Employer’s Address
Secondary Insurance

Medical History
Physician
Address
Are you pregnant If so how many weeks
Do your gums bleed?
Phone Last Visit
Do you have speech problems? if Yes, explain
Are you under the care of a physician? Yes No If Yes, explain
Do you smoke? Do you like your smile?
Have you ever been evaluated for orthodontic treatment?
What are the main concerns that you would like orthodontics to accomplish?
Have you ever experienced jaw joint pain/ discomfort (TMJ/TMD)?
Do you have any missing or extra permanent teeth?
MouthTeeth ChinHave you ever had an injury to : (select all that apply)
Aspirin
Any Metals/Plastics
Latex
Penicillin
Are you allergic to any of the following?
Does/Have you ever had any of the following habits?
Have you tonsils or adenoids been removed?
Clenching/Grinding Teeth
Lip Sucking/Biting
Mouth Breather
Nail biting
Thumb/ Finger Sucking
Prolonged Bottle/Paci�er
Tongue Thrusting
Codeine
Erythromycin
Tetracycline
Other Allergies/Sensitivites:
List all drugs you are currently taking List any serious medical condition(s) treated
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No Yes No Yes No
Signature
I understand that the information that I have provided is correct to the best of my knowledge, that it will be held in the strictest of con�dences and it is my responsibility to inform this o�ce of any changes in my medical status.I hereby authorize the release of any information related to insurance claims. I consent to the examination by the doctor and I authorize payment of any insurance bene�ts to the o�ce.I understand that where appropriate, credit bureau reports may be obtained.
Name of person �ling out this form Date
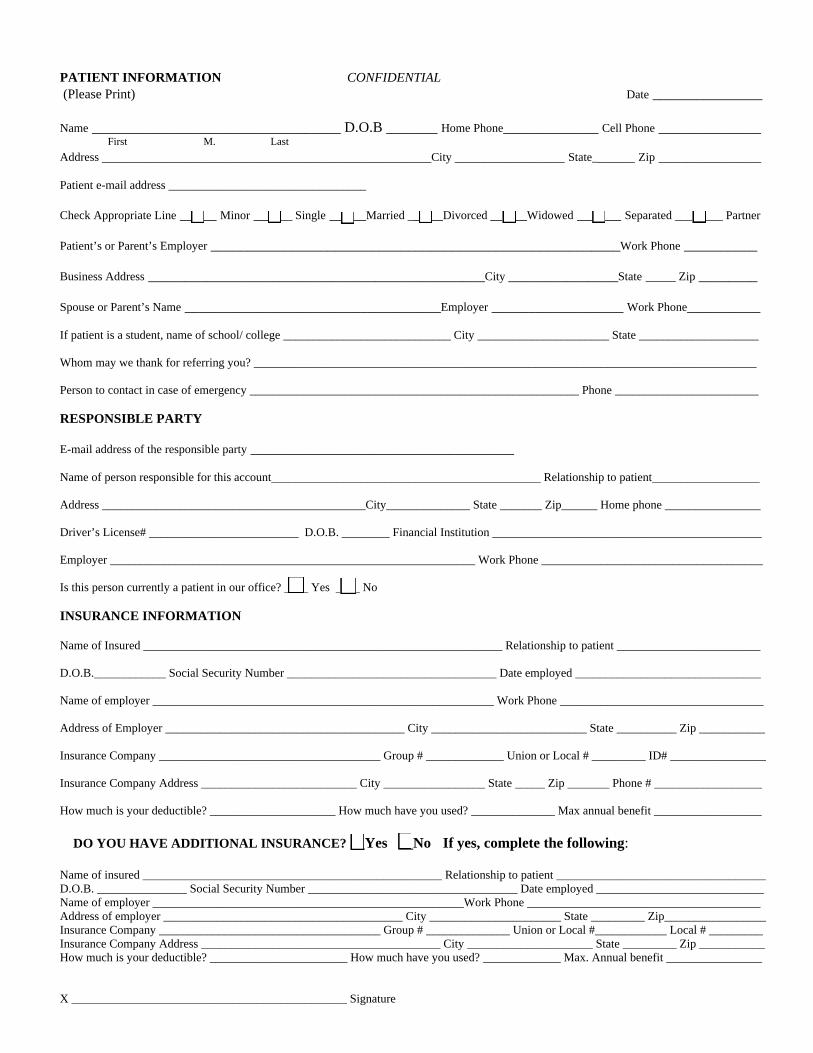
PATIENT INFORMATION CONFIDENTIAL (Please Print) Date _______________ Name __________________________________ D.O.B _______ Home Phone_____________ Cell Phone ______________ First M. Last Address _____________________________________________City _______________ State______ Zip ______________ Patient e-mail address _________________________________ Check Appropriate Line _____ Minor ______ Single _____Married _____Divorced _____Widowed ______ Separated ________ Partner Patient’s or Parent’s Employer ________________________________________________________Work Phone __________ Business Address ______________________________________________City _______________State _____ Zip ________ Spouse or Parent’s Name ___________________________________Employer __________________ Work Phone__________ If patient is a student, name of school/ college ____________________________ City ______________________ State ____________________ Whom may we thank for referring you? ____________________________________________________________________________________ Person to contact in case of emergency _______________________________________________________ Phone ________________________ RESPONSIBLE PARTY E-mail address of the responsible party ____________________________________ Name of person responsible for this account_____________________________________________ Relationship to patient__________________ Address ____________________________________________City______________ State _______ Zip______ Home phone ________________ Driver’s License# _________________________ D.O.B. ________ Financial Institution _____________________________________________ Employer _____________________________________________________________ Work Phone _____________________________________ Is this person currently a patient in our office? ____ Yes ____ No INSURANCE INFORMATION Name of Insured ____________________________________________________________ Relationship to patient ________________________ D.O.B.____________ Social Security Number ___________________________________ Date employed _______________________________ Name of employer _________________________________________________________ Work Phone __________________________________ Address of Employer ________________________________________ City __________________________ State __________ Zip ___________ Insurance Company _____________________________________ Group # _____________ Union or Local # _________ ID# ________________ Insurance Company Address __________________________ City _________________ State _____ Zip _______ Phone # __________________ How much is your deductible? _____________________ How much have you used? ______________ Max annual benefit __________________ DO YOU HAVE ADDITIONAL INSURANCE? __Yes __No If yes, complete the following: Name of insured __________________________________________________ Relationship to patient ___________________________________ D.O.B. _______________ Social Security Number ___________________________________ Date employed ____________________________ Name of employer ____________________________________________________Work Phone _______________________________________ Address of employer ________________________________________ City ______________________ State _________ Zip_________________ Insurance Company _____________________________________ Group # ______________ Union or Local #____________ Local # _________ Insurance Company Address ________________________________________ City _____________________ State _________ Zip ___________ How much is your deductible? _______________________ How much have you used? _____________ Max. Annual benefit ________________ X ______________________________________________ Signature

PATIENT MEDICAL HISTORY
Physician ____________________________________Office Phone __________________ Date of Last Exam ______________________ General Dentist _______________________________Office Phone __________________ Date of Last Exam______________________ 1.) Are you under medical treatment now? ____ Yes ___ No If yes, for what condition? _______________________________________ For how long?_______________________________________ 2.) Have you ever been hospitalized for any surgical operation or serious injury? ____ Yes ____ No If yes, for what condition? _______________________________________ When? _____________________________________________ 3.) Are you taking any medication (s) including non-prescription medicine? ____ Yes ____ No If yes, what medication (s) are you taking? 1. _________________________________ For? ___________________________________ 2. _________________________________ For? ___________________________________ 4.) Do you use tobacco? ____ Yes ____ No 5.) Do you use alcohol, cocaine or other drugs? ____Yes ____ No 6.) Are you wearing contact lenses? ____Yes ____ No 7.) Are you allergic to or have you had any reactions to the following? a.) Local anesthetics (e.g. Novocaine) ___ Yes ____ No f.) Iodine ____ Yes ____ No b.) Penicillin or other antibiotics ___ Yes ____ No g.) Aspirin ____ Yes ____ No c.) Sulfa drugs ___ Yes ____ No h.) Latex ____ Yes ____ No d.) Barbiturates ___ Yes ____ No i.) Metals ____ Yes ____ No e.) Sedatives ___ Yes ____ No 8.) WOMEN ONLY: a.) Are you pregnant or think you may be pregnant? ___ Yes ____ No b.) Are you nursing? ___ Yes ____ No c.) Are you taking birth control pills? ___ Yes ____ No Do you have or have you had any of the following?
Yes No Yes No Yes No ___ ___ High blood pressure ____ ___ Heart disease ___ ___Chest pains ___ ___ Heart attack ____ ___ Cardiac pacemaker ___ ___Easily winded _ ___ ___ Rheumatic fever ____ ___ Heart murmur ___ ___ Stroke ___ ___ Swollen ankles ____ ___ Angina ___ ___ Hay fever/allergies ___ ___ Fainting/Seizures ____ ___ Frequently tired ___ ___ Tuberculosis ___ ___ Asthma ____ ___ Anemia ___ ___ Radiation therapy ___ ___ Low blood pressure ____ ___ Emphysema ___ ___ Glaucoma ___ ___ Epilepsy/Convulsions ____ ___ Cancer ___ ___ Recent weight loss ___ ___ Leukemia ____ ___ Arthritis ___ ___ Liver disease ___ ___ Diabetes ____ ___ Joint replacement or implant ___ ___ Heart trouble ___ ___ Kidney diseases ____ ___ Hepatitis/jaundice ___ ___Respiratory problems ___ ___ AIDS or HIV ____ ___ Sexually transmitted diseases ___ ___ TMJ/Headaches ___ ___ Thyroid problem ____ ___ Stomach troubles/ulcers Other ________________________________ PATIENT DENTAL HISTORY Yes No Yes No 1.) Do your gums bleed while brushing or flossing? ___ ___ 8.) Do you have frequent headaches? ___ ___ 2.) Are your teeth sensitive to hot or cold liquids/foods? ___ ___ 9.) Do you clench or grind your teeth? ___ ___ 3.) Are your teeth sensitive to sweet or sour liquids/foods? ___ ___ 10.) Do you bite your lips or cheeks frequently? ___ ___ 4.) Do you feel pain to any of your teeth? ___ ___ 11.) Have you ever had any difficult extractions 5.) Do you have any sores or lumps in or near your mouth? ___ ___ in the past? ___ ___ 6.) Have you had any head, neck or jaw injuries? ___ ___ 12.) Have you had orthodontic work? ___ ___ 7.) Have you ever experienced any of the following 13.) Have you ever had prolonged bleeding problems in your jaw? following extractions? ___ ___
a.) clicking? ___ ___ 14.) Have you ever had instruction on the b.) pain (joint, ear, side of face)? ___ ___ correct method of brushing your teeth? ___ ___ c.) difficulty in opening or closing? ___ ___ 15.) Have you ever had instructions on the d.) difficulty in chewing? ___ ___ care of your gums? ___ ___
16.) Have you had trauma to your face/teeth? ___ ___ When? ___________________________________________ 17.) Have you been in an accident? ___ ___ When? ___________________________________________
X____________________________________ I certify that I have read and understand the above information. To the best of my knowledge, the above questions have been accurately answered. I understand that providing incorrect information can be dangerous to my health.