Barriers to achieving the health MDGs and how these can be overcome Action for Global Health UK...
14
Barriers to achieving the health MDGs and how these can be overcome Action for Global Health UK Policy Conference London, 28 June 2010 Isabelle de Zoysa
-
Upload
avice-stanley -
Category
Documents
-
view
214 -
download
1
Transcript of Barriers to achieving the health MDGs and how these can be overcome Action for Global Health UK...
Barriers to achieving the health MDGs and how these can be overcome
Action for Global Health UK Policy ConferenceLondon, 28 June 2010
Isabelle de Zoysa
Barriers to achieving the health MDGs and how these can be overcome
Action for Global Health UK Policy ConferenceLondon, 28 June 2010
Isabelle de Zoysa

Health-related MDGs – Scorecard 2010
AFR AMR EMR EUR SEA WPR World
Child Mortality
Measles immunization
Maternal mortality
Skilled birth attendant
Contraceptive use
HIV/AIDS incidence
TB treatment success
Malaria impact
MDG 4
MDG 5
MDG 6

East Africa
Proportion of HIV-related under-5 mortality in African sub-regions, 1990-2007
Central AfricaWest Africa
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
Prop
orti
on (
%)
25
20
15
10
5
0
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
Prop
orti
on (
%)
25
20
15
10
5
0
Southern Africa
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
Prop
orti
on (
%)
25
20
15
10
5
0
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
Prop
orti
on (
%)
25
20
15
10
5
0
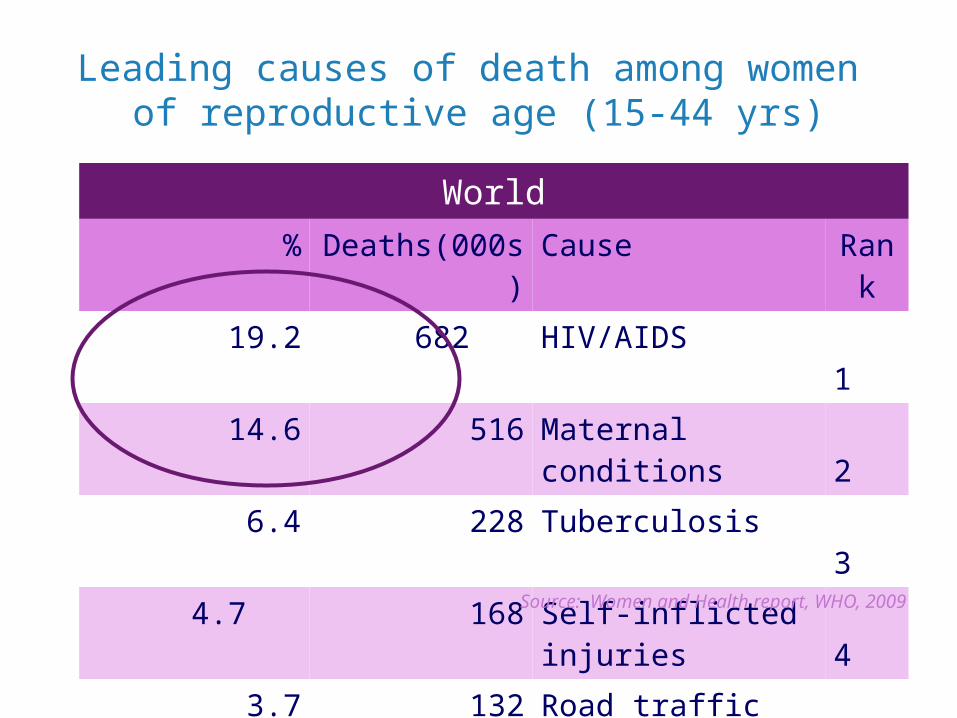
Leading causes of death among women of reproductive age (15-44 yrs)
World% Deaths(000s) Cause Ran
k
19.2 682 HIV/AIDS 1
14.6 516 Maternal conditions 2
6.4 228 Tuberculosis 3
4.7 168 Self-inflicted injuries 4
3.7 132 Road traffic accidents
5
Source: Women and Health report, WHO, 2009
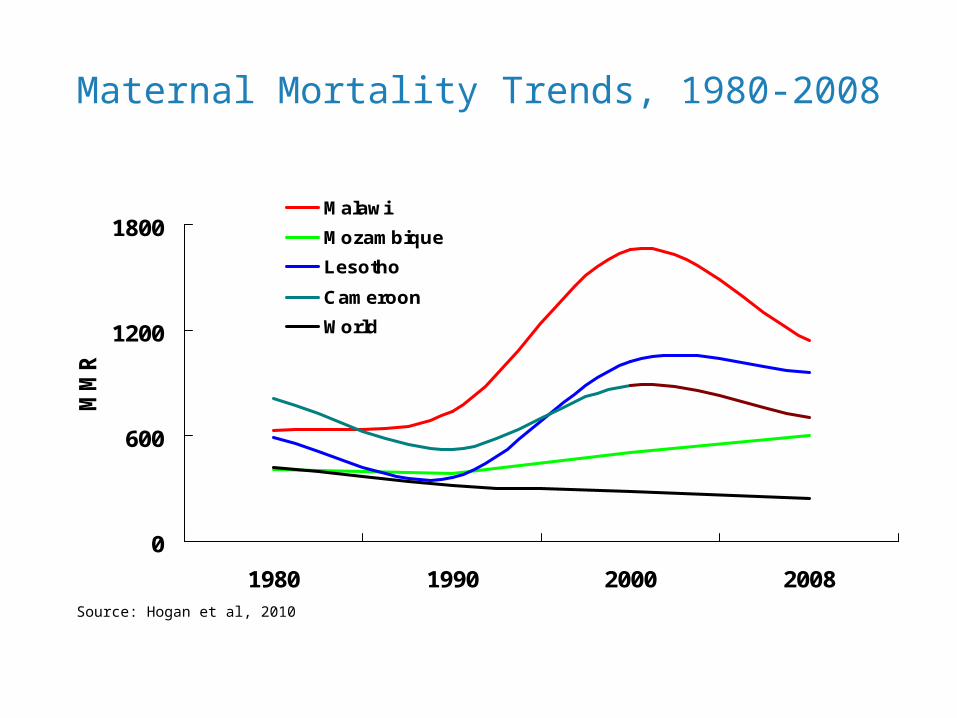
Maternal Mortality Trends, 1980-2008
0
600
1200
1800
1980 1990 2000 2008
MMR
Malawi
Mozambique
Lesotho
Cameroon
World
Source: Hogan et al, 2010

Unequal declines in under 5 mortality 1990-2008

Progress diverges across interventions
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
2002 2003 2004 2005 2006 2007 2008
• FAST - scale-up of people receiving ARVs in low- and middle-income countries
Millions
0
10
20
30
40
50
60
70
80
90
100
1990-1999 2000-2008
SLOW – coverage of skilled attendant at delivery, especially in Africa
Skilled birth attendant%
Receiving ARVs

Women and children are dippingin and out of the health care system

Current concerns and opportunities
· Dissatisfaction with fragmentation· Dissatisfaction with inequalities and
progress· Backlash against withdrawal of the
State
· Failure to reach the MDGs· Limitations of “CE interventions”· Recognition of HS bottlenecks and
of adverse effects of global fragmentation
At country level At global level
Recognition of importance of clarity on “broad policy directions (UC, PHC, HiAP, …)
Country interest in national policy dialogue on health (cfr elections, media,
lobbies)
Global interest in “one plan, one funding mechanism, one M&E framework)
E.g. China, USA, Switzerland, Thailand... E.g. IHP+, Common funding platform...

Country leadership■ Value given to health, equity, solidarity, social
justice■ Individual & institutional
capacities
Financing
Policy Directions universal coverage, primary
care, health in all policies
Strategies Plans
Pharmaceuticals Technology
Infrastructure
Infor-mation
Workforce
Policy dialogue within and
beyond health sector
Comprehensive, integrated,
continuous and people-centred care along the
life-cycle
Cost-effective and safe interventions: clinical &
public health
Universal access to close-to-client
networks, responsible for a
defined population
Including interventions for MDGs 4, 5, 6
Trust in health authorities:● Fairness
● Protection● Competence● Accountability
Health Equity
Health & health
security
Service Delivery
Outcomes
Social inclusion
and participation
Including MDGs 4-5-6
IncludingMDGs 4-5-6
Regulation & Management
institutions, rules,
incentives
Effective aid■ Ownership,
■ Alignment
■ Harmonization
■ Mutual accountability
Governance
Political commitment Mobilise & channel aid
Provide balanced inputs to support HS
Adapt service delivery models (integration, people centredness,
chronic care, access…)
Assist situation analysisAlign programme plans with
National Health PlanInclude stakeholders
Provide guidance on cost-effective interventions
Critical Subsystems
IncludingMDG 3
Integration? …how to make it work..

Don't turn away now
• .5 m cases multidrug resistant TB • 1 m malaria deaths • 2.7 m new HIV infections • 5 m people in need without access to ARVs • 3-800,000 maternal deaths• 3 m diarrhoea & pneumonia deaths in children • 8.8 child deaths• 1100 m people without access to sanitation

Addressing the challenges
• Sustain high level political commitment • Ensure sustainability of resources in times of economic crisis• Strengthen health systems to deliver integrated interventions
across the life course • Promote implementation research to learn from successes and
failures across countries and interventions• Build sound information systems to identify problem areas and
monitor change.

Opportunities to make a difference
• Regional commitments (such as the Maputo Plan of Action and Campaign on Accelerated Reduction of Maternal Mortality in Africa)
• The Joint Action Plan and accountability framework• Muskoka Initiative – additional funding for a comprehensive and
integrated approach to accelerate progress towards MDGs 4 & 5
• Commitment to integrating approaches to maximize health outcomes related to MDGs 4, 5 and 6, while strengthening health systems
• Global mobilization around scaling up PMTCT towards elimination
• GF Board Decision to explore options for optimizing synergies with Maternal and Child Health; GF replenishment
• Other programming and financing opportunities (GHI/PEPFAR etc)

Thank you!