Bacteremia by Streptobacillus moniliformis : First Case Described in Spain
3
Eur J Clin Microbiol Infect Dis (2003) 22:258–260 DOI 10.1007/s10096-003-0891-9 CONCISE ARTICLE L. Torres · A. I. LɃpez · S. Escobar · C. Marne · M. L. Marco · M. PȖrez · J. Verhaegen Bacteremia by Streptobacillus moniliformis : First Case Described in Spain Published online: 22 March 2003 # Springer-Verlag 2003 Abstract Described here is the case of an 87-year-old man who developed fever, chills and discomfort caused by Streptobacillus moniliformis. This pathogen is one of the causes of rat-bite fever, an uncommon bacterial illness transmitted through a bite or scratch from a rodent or the ingestion of food or water contaminated with rat faeces. Cases of rat-bite fever are rarely reported in Spain. The patient reported no history of rat bite or rodent contact, and the only known risk factor was contact with a dog and a cat that were kept as pets. Streptobacillus moniliformis was isolated in two sets of blood cultures. This case represents what is believed to be the first report of bacteremia due to Streptobacillus moniliformis in Spain. Introduction Rat-bite fever (RBF) is an infectious disease caused by two different microorganisms, Streptobacillus monilifor- mis and Spirillum minus, which are commonly found in the oropharyngeal flora of rodents [1, 2, 3]. Infection can be acquired through the bite or scratch of a rodent or the ingestion of food or water contaminated with rat faeces [2]. The term RBF encompasses three distinct clinical disorders caused by two organisms: (i) spirillary RBF caused by Spirillum minus, which is more frequent in Asia and called Sodoku; (ii) streptobacillary RBF caused by Streptobacillus moniliformis, which is more common in North America and Europe; and (iii) Haverhill fever or erythema arthriticum epidemicum, which is caused by Streptobacillus moniliformis after ingestion of milk, food or water contaminated by the excretions of infected rats [2]. In Spain, the incidence and prevalence of this infection is unknown. Our search of the medical literature (MED- LINE, January 1965–June 2002, key words: rat-bite fever, Streptobacillus moniliformis) revealed only three cases of arthritis and one case of a subcutaneous abscess related to RBF in our country [4, 5, 6, 7]. Thus, this report seems to represent the first case of bacteremia caused by Strepto- bacillus moniliformis in Spain, and the infection occurred in a patient without rodent contact. Case Report An 87-year-old man was admitted to our hospital with discomfort, anorexia, weight loss, polyuria, dysuria, slight dehydratation and mild fever of 20 days’ duration. Two sets of blood cultures were taken and empirical treatment with levofloxacin was initiated. The patient became afebrile and was discharged 8 days after hospital admission. Blood cultures were inoculated into Bactec 9240 culture vials (Becton Dickinson, USA) that yielded growth after 2 days of incubation. A Gram stain demonstrated pleomorphic, filamentous and branching gram-negative bacilli with characteristic bulbous swellings. Subcultures onto Wilkins-Chalgren and chocolate agar under anaerobic and microaerophilic conditions, respectively, were performed. After 72 h a small growth of grey, small, rounded, glistening and buttery colonies was observed on both culture media. Gram stain of the colonies revealed pleomorphic, long, some- times short, filamentous rods with specific bulbous swellings that could fold into curls and loops. Subculture in thioglycolate medium enriched with 5% foetal calf serum showed typical growth in “puff- ball” colonies (Fig. 1). Biochemical testing revealed the following: positive for arginine dihydrolase activity and negative for oxidase, catalase, urease, indole reaction, lysine and ornithine decarboxyl- ase. All these characteristics pointed to infection with Streptoba- cillus moniliformis. The strain was sent to the Department of Microbiology of the University Hospitals of Leuven (Belgium), where gas chromatog- raphy of fatty acids was performed. These tests demonstrated the L. Torres ( ) ) · A. I. LɃpez · S. Escobar · C. Marne · M. L. Marco Department of Microbiology, Miguel Servet University Hospital, Paseo Isabel la CatɃlica 1-3, 50009 Zaragoza, Spain e-mail: [email protected] Tel.: +34-97-6765542 M. PȖrez Department of Internal Medicine, Miguel Servet University Hospital, Paseo Isabel la CatɃlica 1-3, 50009 Zaragoza, Spain J. Verhaegen Department of Laboratory Medicine, Bacteriology, University Hospitals Leuven, CDG7, Herestraat 49, 3000 Leuven, Belgium
Transcript of Bacteremia by Streptobacillus moniliformis : First Case Described in Spain

Eur J Clin Microbiol Infect Dis (2003) 22:258–260DOI 10.1007/s10096-003-0891-9
C O N C I S E A R T I C L E
L. Torres · A. I. L�pez · S. Escobar · C. Marne ·M. L. Marco · M. P�rez · J. Verhaegen
Bacteremia by Streptobacillus moniliformis :First Case Described in Spain
Published online: 22 March 2003� Springer-Verlag 2003
Abstract Described here is the case of an 87-year-oldman who developed fever, chills and discomfort causedby Streptobacillus moniliformis. This pathogen is one ofthe causes of rat-bite fever, an uncommon bacterial illnesstransmitted through a bite or scratch from a rodent or theingestion of food or water contaminated with rat faeces.Cases of rat-bite fever are rarely reported in Spain. Thepatient reported no history of rat bite or rodent contact,and the only known risk factor was contact with a dog anda cat that were kept as pets. Streptobacillus moniliformiswas isolated in two sets of blood cultures. This caserepresents what is believed to be the first report ofbacteremia due to Streptobacillus moniliformis in Spain.
Introduction
Rat-bite fever (RBF) is an infectious disease caused bytwo different microorganisms, Streptobacillus monilifor-mis and Spirillum minus, which are commonly found inthe oropharyngeal flora of rodents [1, 2, 3]. Infection canbe acquired through the bite or scratch of a rodent or theingestion of food or water contaminated with rat faeces[2]. The term RBF encompasses three distinct clinicaldisorders caused by two organisms: (i) spirillary RBFcaused by Spirillum minus, which is more frequent in
Asia and called Sodoku; (ii) streptobacillary RBF causedby Streptobacillus moniliformis, which is more commonin North America and Europe; and (iii) Haverhill fever orerythema arthriticum epidemicum, which is caused byStreptobacillus moniliformis after ingestion of milk, foodor water contaminated by the excretions of infected rats[2].
In Spain, the incidence and prevalence of this infectionis unknown. Our search of the medical literature (MED-LINE, January 1965–June 2002, key words: rat-bite fever,Streptobacillus moniliformis) revealed only three cases ofarthritis and one case of a subcutaneous abscess related toRBF in our country [4, 5, 6, 7]. Thus, this report seems torepresent the first case of bacteremia caused by Strepto-bacillus moniliformis in Spain, and the infection occurredin a patient without rodent contact.
Case Report
An 87-year-old man was admitted to our hospital with discomfort,anorexia, weight loss, polyuria, dysuria, slight dehydratation andmild fever of 20 days’ duration. Two sets of blood cultures weretaken and empirical treatment with levofloxacin was initiated. Thepatient became afebrile and was discharged 8 days after hospitaladmission.
Blood cultures were inoculated into Bactec 9240 culture vials(Becton Dickinson, USA) that yielded growth after 2 days ofincubation. A Gram stain demonstrated pleomorphic, filamentousand branching gram-negative bacilli with characteristic bulbousswellings. Subcultures onto Wilkins-Chalgren and chocolate agarunder anaerobic and microaerophilic conditions, respectively, wereperformed. After 72 h a small growth of grey, small, rounded,glistening and buttery colonies was observed on both culture media.
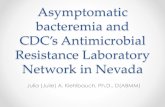
Gram stain of the colonies revealed pleomorphic, long, some-times short, filamentous rods with specific bulbous swellings thatcould fold into curls and loops. Subculture in thioglycolate mediumenriched with 5% foetal calf serum showed typical growth in “puff-ball” colonies (Fig. 1). Biochemical testing revealed the following:positive for arginine dihydrolase activity and negative for oxidase,catalase, urease, indole reaction, lysine and ornithine decarboxyl-ase. All these characteristics pointed to infection with Streptoba-cillus moniliformis.
The strain was sent to the Department of Microbiology of theUniversity Hospitals of Leuven (Belgium), where gas chromatog-raphy of fatty acids was performed. These tests demonstrated the
L. Torres ()) · A. I. L�pez · S. Escobar · C. Marne · M. L. MarcoDepartment of Microbiology,Miguel Servet University Hospital,Paseo Isabel la Cat�lica 1-3, 50009 Zaragoza, Spaine-mail: [email protected].: +34-97-6765542
M. P�rezDepartment of Internal Medicine,Miguel Servet University Hospital,Paseo Isabel la Cat�lica 1-3, 50009 Zaragoza, Spain
J. VerhaegenDepartment of Laboratory Medicine, Bacteriology,University Hospitals Leuven, CDG7,Herestraat 49, 3000 Leuven, Belgium

three peaks characteristic of Streptobacillus moniliformis: palmitic(C16:0), stearic (C18:0) and oleic acid (C18:1). Using diskdiffusion with paper disks, the strain was found to be inhibited invitro by penicillin, ampicillin, amoxicillin-clavulanate, cefotaxime,azithromycin, erythromycin, doxycycline, cotrimoxazole, vanco-mycin and teicoplanin. Resistance to polymyxin B, gentamicin,tobramycin, ciprofloxacin and levofloxacin was also revealed.
On questioning, the patient could not recall either a rat bite orcontact with rodents. He lived in an urban area with a dog and a catas pets. No further information about the patient was obtainedfollowing hospital discharge.
Discussion
Human cases of RBF are reported rarely worldwide, andthe true incidence of the disease is unknown [1, 2, 7, 8, 9].Transmission occurs via the bite or scratch of rats [1, 2],but cases have also been associated with bites of mice,squirrels and gerbils and with exposure to animals thatprey on these rodents (e.g., cats and dogs) [1, 2, 9, 10].Persons who are at risk of percutaneous inoculationusually include animal laboratory personnel, children andfarmers [2, 4, 7, 8, 11].
In the case reported here, the patient had no history ofdirect rodent contact and the source of infection wasunclear. The patient lived in the city with a dog and a cat,and these animals have been referred to previously asvectors [1, 2, 10]. It is possible that exposure to these petswas the cause of the infection.
The usual incubation period of RBF is less than 10days, with the beginning of clinical disease usually beingmarked by fever, chills, headache, vomiting, migratingarthralgia and myalgia and a petechial rash [1, 2, 5, 7, 9].In our patient, the only clinical manifestation was fever,and no evidence of arthralgia or rash was found.Complications can include arthritis [5, 6, 7, 8], endocar-ditis [12], pericarditis [13], abscess formation [4], pneu-monia [14] and meningitis [14]. Without adequatetherapy, the illness may persist for a period of months,and the mortality rate is as high as 10% (53% in the caseof endocarditis) [1, 2].
Streptobacillus moniliformis grows slowly over 2–3days, and it prefers microaerophilic conditions (CO2 5–10%) [7, 8]. Culture is difficult to perform, requiringmedia enriched with serum, blood, ascitis or yeast extract[7, 8, 9]. Blood cultures in automatic systems can beunreliable because these systems use polyanethole-sulphonate, an anticoagulant that can inhibit the growthof these bacteria [12, 16]. Nevertheless, we and otherauthors [14] have successfully isolated Streptobacillusmoniliformis using these systems.
Gram stain and typical morphology in solid and liquidmedia can allow a presumptive identification. However,definite identification is based on gas chromatography offatty acids. Recently, a polymerase chain reaction tech-nique has also been developed [15].
The typical susceptibility pattern of the organism issimilar to that of a gram-positive organism, and this cancause some confusion [8]. Streptobacillus moniliformis isusually susceptible to amoxicillin, amoxicillin-clavu-lanate, doxycycline, ceftriaxone, penicillin, oxacillin,vancomycin and erythromycin. Resistance to polymyxinB, aminoglycosides and cotrimoxazole has been reported[8]. Our strain differed in regard to cotrimoxazolesusceptibility. We found no reference to quinoloneresistance. Although our patient’s isolate demonstratedin vitro resistance to quinolones, he was treated empir-ically with levofloxacin upon admission and becameafebrile. However, long-term follow-up was not possible.
Penicillin is the first-choice therapy for RBF at arecommended dose of 1,200,000 U/day for 5–7 daysfollowed by oral penicillin for 7 days. In complicatedcases, such as endocarditis, therapy must be administeredfor 4–6 weeks [1, 6, 8]. When an allergy to penicillinexists, doxycycline is recommended [17].
In conclusion, the diagnosis of RBF is difficult tomake and can be missed. The disease should be includedin the differential diagnosis for all patients with articularpain and irregular relapsing fever. It is important toemphasize the importance of good communication be-tween clinicians and microbiologists, since this is essen-tial in order for a proper diagnosis to be made and forappropiate treatment to be started.
Fig. 1 Typical “puff-ball” colonies in thioglycolate medium
259

References
1. Washburn RG (1995)Streptobacillus moniliformis (Rat-bitefever). In: Mandell GL, Douglas RG, Bennett JE (eds)Principles and practice of infectious diseases, vol 2. ChurchillLivingstone, New York, pp 2084–2086
2. Centers for Disease Control (1998) Rat-bite fever—NewMexico, 1996. MMWR 47:89–91
3. Downing ND, Dewnany GD, Radford PJ (2001) A rare seriousconsequence of a rat bite. Ann R Coll Surg Engl 83:279–280
4. Torres A, Cuende E, De Pablos M, Lezaun MJ, Michaus L,Vesga JC (2001) Remitting seronegative symmetrical synovitiswith pitting edema associated with subcutaneous Streptobacil-lus moniliformis abscess. J Rheumatol 28:1696–1698
5. S�ez R, Alvarez B, Alegre J, Alonso JL, Ojeda E, Marne C(1996) Streptobacillus moniliformis septic oligoarthritis (fevercaused by rat bite). Rev Clin Esp 196:413–415
6. Bretal M, Mera A, Caama�o M, Insffla S, Pardo F, P�rez delMolino M (1994) Fiebre por mordedura de rata: una causainfrecuente de poliartritis. Rev Esp Reumatol 21:279–281
7. Anglada A, Comas L, Euras JM, Sanmart� R, Vilar� J, Brugu�sJ (1990) Arthritis due to Streptobacillus moniliformis: a case ofrat-bite fever. Med Clin (Barc) 94:535–537
8. Frans J, Verhaegen J, Van Noyen R (2001) Streptobacillusmoniliformis: case report and review of the literature. Acta ClinBelg 56:187–190
9. Graves MH, Janda MJ (2001) Rat-bite fever (Streptobacillusmoniliformis): a potential emerging disease. Int J Infect Dis5:151–154
10. Peel MM (1993) Dog-associated bacterial infections in humans:isolates submitted to an Australian reference laboratory, 1981–1992. Pathology 25:379–384
11. Wullenweber M (1995) Streptobacillus—a zoonotic pathogen.Taxonomic considerations, host species, diagnosis, therapy,geographical distribution. Lab Anim 29:1–15
12. Rordorf T, Zuger C, Zbinden R, Von Graevenitz A, Pirovino M(2000) Streptobacillus moniliformis endocarditis in an HIV-positive patient. Infection 28:393–394
13. Carbeck RB, Murphy JF, Britt EM (1967) Streptobacillary rat-bite fever with massive pericardial effusion. JAMA 201:133–134
14. Sens MA, Brown EW, Wilson LR, Crocker TP (1989) FatalStreptobacillus moniliformis infection in a two-month-oldinfant. Am J Clin Pathol 91:612–616
15. Lambe DWJR, McPhedran AM, Mertz JA, Stewart P (1973)Streptobacillus moniliformis isolated from a case of Haverhillfever: biochemical characterization and inhibitory effect ofsodium polyanethol sulfonate. Am J Clin Pathol 60:854–860
16. Berger C, Altwegg M, Meyer A, Nadal D (2001) Broad rangepolymerase chain reaction for diagnosis of rat-bite fever causedby Streptobacillus moniliformis. Ped Infect Dis J 20:1181–1182
17. Gilbert DN, Moellering RC Jr, Sande MA (eds) (2002) TheSanford Guide to Antimicrobial Therapy, 32nd edn. Antimi-crobial Therapy, Hyde Parke, Vermont
260