BACK TO BASICS: DEBRIDEMENT
8
BACK TO BASICS: DEBRIDEMENT Guide To Wound Bed Preparation Cutimed®, an Essity brand
Transcript of BACK TO BASICS: DEBRIDEMENT

BACK TO BASICS: DEBRIDEMENT
Guide To Wound Bed Preparation
Cutimed®,an Essity brand

WHEN SHOULD YOU DEBRIDE?
When it is safe to do so and the practitioners possess the
appropriate skills.1
Early debridement accelerates healing1
Frequent debridement leads to better healing outcomes1
Some areas demand extra caution and should not be debrided before advice is sought² � High-risk areas: face, hands, feet, genitalia � Ischaemic limbs � Wounds associated with congenital malformations or in which malignancy is suspected � Wounds in proximity to blood vessels, nerves and tendons � Wounds in patients who cannot give informed consent, or in those on palliative treatment regimens � Any wound that has not been properly assessed by a competent practitioner (origin and diagnosis unknown) � Wounds in patients with blood clotting disorders � Wounds in patients with possible implants and/or dialysis fistulas � Patients with inflammatory conditions, such as Pyoderma gangrenosum
2

HOW TO CHOOSE A DEBRIDEMENT METHOD
The debridement method chosen should follow a full, holistic assessment of the patient and the wound2
The choice of method should be based on:
� Nature of the tissue
� Anatomical location
� Size of the wound
� Speed of debridement required2
You should also take into account3:
Patient factors Clinician factors
� Level of pain � Environment � Choice and consent � Age and any comorbidities � Quality of life
� Level of skill � Available resources � Organisation’s policy � Organisation’s guidelines (local formulary listings)
3

DEBRIDEMENT METHODS IN PRIMARY CARE
Autolytic
� Occurs naturally using body’s own enzymes
� This method uses moisture to soften hard necrotic tissue and liquify slough, e.g. hydrogels, hydrocolloids
� Suitable for most types of devitalised tissue
� May not be suitable if high volume of exudate present
� The process may be slower than other methods
� Suitable for self-care / supported care by patients and carers
� Known to be an over-used method because selection based on familiarity rather than need of the patient
� Relatively pain-free
Mechanical
� Use of monofilament pads or debridement cloths containing a surfactant
� Monofilament pads can help remove bacteria and biofilm
� Suitable for softer and not tenacious or hard devitalised tissue, unless softened beforehand with autolytic debridement
� Offers rapid debridement and suitable for self-care by patients and carers
Larval (via specialist referral)
� Sometimes referred to as Biosurgical debridement
� Uses the sterile larvae of the greenbottle fly
� A form of autolytic debridement as the larvae produces an enzyme that liquifies devitalised tissue
� Rapid debridement
� Not always acceptable with patients or healthcare workers
Debridement methods require varying levels of expertise. You need to consider your skills to perform the task and refer to a specialist if necessary4 .
4

MECHANICAL DEBRIDEMENT
Mechanical debridement refers to the process of removing dead, devitalised or contaminated tissue from the wound bed in order to encourage wound healing1. Debridement removes bacteria and can disrupt biofilm. It is recognised as an essential step to facilitate wound healing4.
Reasons to debride:
We debride to remove dead and devitalised tissue.
This tissue: � forms a physical barrier to healing
� allows bacteria to proliferate
� masks or mimics infection
� increases risk of infection and malodour
� reduces effectiveness of topical preparations
� increases volume of exudate
� hinders wound assessment2,5
Debridement aims to3:
Remove: Decrease:
� Necrotic, devitalised, sloughy tissue
� Sources of infection, inflammation
� Exudate, dried exudate and dry skin/hyperkeratosis
� Pus
� Haematoma
� Debris or foreign bodies
� Any other barriers to healing
� Odour
� Excess moisture
� Risk of infection
Stimulate:
� Wound edges and epithelialisation
Improve:
� Quality of life
5

MECHANICAL DEBRIDEMENT USING CUTIMED® DEBRICLEAN®
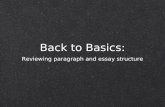
Cutimed® DebriClean® is a brand new, innovative product. It contains gentle looped monofilament fibres in white alongside more abrasive looped monofilament fibres in blue. It is able to absorb bacteria and remove firm/viscous slough.In in vitro testing, Cutimed® DebriClean excelled in bacterial binding when compared to standard debridement options.
Clean Cutimed® DebriClean pad
A sample of the clean product is placed in a test tube with bacteria
(Pseudomonasaeruginosa)
Sample was thenintensively rinsed mechanically to remove loosely
attached bacteria
High quantity of bacterial microbes bound to
Cutimed® DebriClean pad
After rinsing, Cutimed® DebriClean shows much higher bacterial binding to wound microorganisms
than other products
CO
LON
Y F
OR
MIN
G U
NIT
S / M
L
1
100000
200000
300000
400000
500000
600000
700000
800000
Cutisoft® Cotton Cutimed® DebriClean(white)
*Initial concentration 2.5 Mio cfu/ml Pseudomonas aeruginosa DSM1117. Contact time 15 min. intensive rinsing with Tween 20 (non ionic tenside)
Effective bacterial binding
How many bacteria remained bound to the debridement pad after rinsing?
800,000 colony forming units per
ml remained bound to the Cutimed® DebriClean pad*
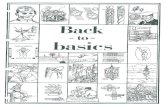
In chronic wounds, devitalised tissue and biofilm forms a physical barrier that inhibits the formation of new tissue. For the wound to heal properly, the devitalised tissue and biofilm must be removed.3 That’s why every layer of the Cutimed® DebriClean pad has been specially designed to support you in the mechanical debridement process and lead to more effective wound healing.
Blue, more abrasive fibres for a stronger debridement
option (if required)
White, looped monofilament fibre for gentle abrasion and slough / biofilm
/ microorganism removal
Perforated adhesive layer supports absorption / rinsing
Foam layer also supports the absorption / rinsing function during use. This novel feature supports the cleaning efficency of the pad.
Strong adhesive layer bonds the backing to the foam core
Printed backing supports correct use and reduces fluid strike-through
Hand loop for easy, comfortable and accurate use
Hard blister pack for moistening and disposal. Dependant on your local guidelines, all commonly used wound rinsing solutions can be used.*
* Product is compatible with commonly used wound cleansing solutions based on PHMB, sodium hypochloriteor hypochlorous acids, octenidine, 0.9% medical saline solution, water and Ringer’s solution
Fast and effective wound debridement
Meet Cutimed® DebriClean
DebriClean® offers:
> 99% biofilm removal with just four wipes6
Strong cleaning efficiency6.7
Effective bacterial binding8
6

DEBRIDEMENT METHODS AVAILABLE VIA SPECIALIST REFERRAL
Specialist Referral1,2,9
Ultrasonic
Using ultrasound either directly on the wound bed or by an atomised solution
Hydrosurgical
The use of a high energy saline beam as a cutting implement
Sharp
Using a scalpel, scissors or curette to remove tissue. Often used in conjunction with other methods
Surgical
Excision and removal performed by a specialist in an acute, operating theatre environment
It is important to know when to refer to a specialist best qualified to debride. Remember that NOT debriding / referring can potentially cause harm to your patients; involve your multidisciplinary team where you need to in order to provide the care your patients need¹.
7

BACK TO BASICS: DEBRIDEMENT If you have found this Back to Basics guide helpful, look out for futher guides in the series - including the guide on Identification and Management of Wound Infection.
References
1. Harries R, Bosanquet D, Harding K (2016) Wound bed preparation: TIME for an update. Int Wound J 13(Suppl 3): 8–14
2. Wounds UK (2013) Effective debridement in a changing NHS: A UK consensus. Wounds UK, London. Available online: www.wounds-uk.com
3. Strohal R, Apelqvist J Dissemond J, et al (2013) EWMA document: Debridement. J Wound Care 22(Suppl 1): S1–S52
4. Vowden K and Vowden P (2011) Debridement made easy. Wounds UK 7(4) S1-S4
5. Price P, Young T (2013) Debridement consensus: Recommendations for practice. Wound Essentials 8(1): 71–6
6. JB4 40031908, In vitro evaluation of removal of viable biofilm by Cutimed® DebriClean and Cutisoft Cotton. August 2018, BSN medical data on file.
7. JB4 40031810, In vitro evaluation of the cleansing effect of Cutimed® DebriClean and Cutisoft Cotton. August 2018, BSN medical data on file.
8. JB4 40031811, In vitro evaluation of the bacterial adhesion to Cutimed® DebriClean and Cutisoft Cotton. July 2018, BSN medical data on file.
9. Mahoney K (2020) Part 2: Wound cleansing and debridement. J Community Nurs 34(3): 26–32
Cutimed®,an Essity brand
EssityT/A BSN medical LimitedPO Box 258 • Willerby • Hull • HU10 6WT
www.bsnmedical.co.uk Tel: 01482 670100 • Fax: 01482 670111 E-mail: [email protected]/1020