Asymptomatic Left Ventricular Dysfunction After Myocardial Infarction Nancy M. Albert PhD, CCNS,...
24
Asymptomatic Left Ventricular Dysfunction After Myocardial Infarction Nancy M. Albert PhD, CCNS, CCRN, NE-BC, FAHA, FCCM Nursing Research & Kaufman Center for Heart Failure Cleveland Clinic, Cleveland OH
-
Upload
zachariah-medler -
Category
Documents
-
view
220 -
download
0
Transcript of Asymptomatic Left Ventricular Dysfunction After Myocardial Infarction Nancy M. Albert PhD, CCNS,...

Asymptomatic Left Ventricular Dysfunction
After Myocardial Infarction
Nancy M. Albert PhD, CCNS, CCRN, NE-BC, FAHA, FCCMNursing Research & Kaufman Center for Heart FailureCleveland Clinic, Cleveland OH

LV Dysfunction Post MI• Nov. 2002 - May 2006, Olmsted Cty, MN
– 835 incident MI’s; 246 Troponin; 589 CK-MB– Echo ~ 24 hours later:
• 33% systolic dysfunction• 53% diastolic dysfunction
– Preserved LV systolic function, 33%• Mean follow-up of ~ 0.8 yrs:
– 142 patients developed clinical HF• 29% 1-year rate of HF development
– 87% of episodes occurred within the 1st month of AMI
Arruda-Olson AM et al. Am Heart J 2008;156:810-5.

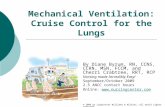
Trends in HF After AMI• 676 Framingham Heart Study patients; 45-85 yrs old
– 1st MI between 1970-1999– Incidence of HF and 30 day and 5 year death by decade over time
Velagalati VS et al. Circulation 2008;118:2057-62.
Incidence of HF at 30 days
1970-79: 10%
1990-99: 23.1%
P trend = 0.003
Incidence of HF at 5 years
1970-79: 27.6%
1990-99: 31.9%
P trend = 0.02
Time (years)
0 0.2 0.4 0.6 0.8 10.75
0.80
0.85
0.90
0.95
1.00
Su
rviv
al f
ree
of
CH
F
1970-791980-891990-99

Ventricular Remodeling After Acute Infarction
Jessup & Brozena. NEJM 2003:348: 2007

KILLIP Class and AMI
Killip Class Definition
I No evidence of HF
2 Rales up to ½ of lung fields or S3 heart sound, and Systolic BP > 90 mmHg
3 Frank pulmonary edema andSystolic BP > 90 mmHg
4 Cardiogenic shock with rales,Systolic BP < 90 mm Hg andSigns of tissue hypoperfusion

Parakh K, et al. Am J Med 2008;21:1015-1018.
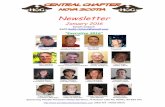
KILLIP Class and Outcomes Post AMI
Years 0 2 4 6 8 10At risk 282 227 198 167 145 130Killip 1 168 149 137 121 109 100Killip 2 64 48 43 33 26 23Killip 3/4 50 30 18 13 10 7
Per
cen
tag
e S
urv
ivin
g
0
50
100
Killip Class 1Killip Class 2Killip Class 3 or 4
Ten
Yea
r M
ort
alit
y R
ate
(%)
0
40
80
60
20
P < 0.001
KillipClass 1
& no LVSD
KillipClass 1& LVSD
KillipClass >1
& no LVSD
KillipClass >1& LVSD

Zhang Y, et al. Am Heart J 2008;156:1124-32.
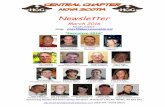
Cardiac Remodeling Post AMI
ESV, end systolic volume; Ts-SD: Standard deviation of time to peak myocardial contraction Te-SD: Standard deviation of time to peak early relaxation
Characteristic Normal LV Gp Remodeled Gpearly Post MI (n = 31) (n=16) P value
Q waves 24/31 13/16 NS
Anterior wall 11/31 14/16 .007
Peak CK (u/L) 1910 ± 1046 4098 ± 2081 .006
ESV mL 40.6 ± 8.5 47.6 ± 8.4 .006
Ts-SD 33.7 ± 7.5 50.9 ± 10.8 <.0005
Te-SD 36.2 ± 20.2 45.2 ± 23.2 .048
EF% 53.1 ± 11.7 40.8 ± 7.6 <.0005
Infarct size 10.7 ± 5.9 26.4 ± 10.2 <.0005
Transmurality % 73.6 ± 17.3 85.7 ± 19.6 .039

Zhang Y, et al. Am Heart J 2008;156:1124-32.
Cardiac Remodeling Post AMIContrast-enhanced cardiac MRI shows a non transmural MI
Infarct
Epi.
Papi.Endo.


Pt Characteristics by Killip Class
Parakh K, et al. Am J Med 2008;21:1015-1018.
Killip 1 Killip 2 Killip 3 / 4Characteristic n=168 n=64 n=50 P value
Age, yrs (mean age 50 yrs) 62.0 ± 12 68.5 ± 11 69.3 ± 10 <.001
Diabetes Mellitus, % 24 40 70 <.001
Previous MI, % 26 36 42 .06
Hx COPD 19 14 27 .009
Family history, % 41 44 20 .02
LV systolic dysfunction, % 47 76 88 <.001
Treatments
Medication only, % 67 70 86 .036
Primary PCI, % 16 3.1 0 <.001
Discharge ACE-I, % 41 61 50 .02
Discharge beta-blocker, % 85 84 74 .20
Discharge statin, % 48 31 38 .051
Discharge ASA, % 89 90 72 .006
Discharge digoxin, % 9 16 28 .002

Cardiac Remodeling Post AMI47 patients with normal QRS underwent echo 2-6 days, 3 months and 1 year after AMI to determine if systolic dyssynchrony predicted cardiac remodeling post MI
Zhang Y, et al. Am Heart J 2008;156:1124-32.
*P < 0.05 from baseline†P < 0.05 between groups
ES
V (
ml)
Baseline 3 mos. 1 year0
20
40
60
80
ED
V (
ml)
0
20
60
100
140
Baseline 3 mos. 1 year
40
80
120
Remodeling groupNon-remodeling group
LV
EF
(%
)
0
10
30
50
70
Baseline 3 mos. 1 year
20
40
60
† *
† † †
† *
*
*

Zhang Y, et al. Am Heart J 2008;156:1124-32.
*P < 0.05 from baseline†P < 0.05 between groups
Cardiac Remodeling Post AMI47 patients with normal QRS underwent echo 2-6 days, 3 months and 1 year after AMI to determine if systolic dyssynchrony predicted cardiac remodeling post MI
Ts-
SD
(m
s)
0
20
40
60
80
Baseline 3 mos. 1 year0
Baseline 3 mos. 1 year
Remodeling groupNon-remodeling group
Te-
SD
(m
s)
20
40
60
80
Ts-SD: Standard deviation of time to peak myocardial contraction Te-SD: Standard deviation of time to peak early relaxation
**
* *
†† *
† †

TRACE Study: Wall Motion Index Prevalence and Mortality at 3 years by CHF status
Prevalence of WMI < 1.2 was 40%
Kober L et al. Am J Cardiol 1996;78:1124-1128.
Mortality at 3 years
0
10
20
30
40
Per
cen
t
<0.8 0.8-1.2 1.3-1.6 >1.60
20
40
80
100
Per
cen
t
<0.8 0.8-1.2 1.3-1.6 >1.6
60
WMI
No CHFCHF

1-Year Rehospitalization Based on Diastolic Dysfunction Post MI
Khumri TM et al. Am J Cardiol 2009;103:17-21.
Severe Diastolic Dysfunction HR (SD) for hospitalization: 3.31 (1.26, 8.69)
N = 190
Reh
osp
ital
izat
ion
Fre
e (%
)
p=0.0052
NormalModerateMildSevere
Months0 3 6 9 12
0
20
40
60
80
100

TRACE Study: Proportion of patients with HF or LVSD within the 1st few days post MI
40
54
30
64
0
20
40
60
80
LVSD HF HF and LVSD HF or LVSD
Pa
tie
nts
(%
)
Kober L et al. NEJM 1995;333:1670-1676.

Pathophysiology of Life Threatening Arrhythmias In CAD
Myerburg MJ et al. NEJM 2008;359:2245-2253.

VT/VF Post Acute Myocardial Infarction: Valiant Registry
Piccini JB et al. Am J Cardiol 2008;102:1427-31.
VT / VFCharacteristic No Yes (n=306)early Post MI (n = 5085) 5.7% overall P value
Worsening heart failure 6.4% 13.1% <0.001
Cardiogenic shock 3.9% 14.1% <0.001
Coronary angioplasty 41.5% 41.5% .997
CABG 10.6% 13.4% .122
Stent 36.7% 36.9% .924
In Hospital Mortality 5.9% 20.3% <0.001

Post AMI – LVD Treatments
Flaherty JD et al. Am J Cardiol 2008;102(5A)38G-41G
Goal TherapyImprove symptoms Tx aimed at ischemia and/or congestion
Prevent future coronary Statinsevents (CAD progression) Antiplatelet agents
ACE-I/ARBCoronary revascularization (PTCA or CABG)
Attenuate progressive ACE-I/ARBpathologic LV remodeling Beta blockers
Aldosterone antagonistCRT
Prolong survival by Beta blockerspreventing SCD or ICD
progression of HF CRTLVAD

Nursing Leadership
Stage A: Pre Heart Failure• Therapies: Treat or control medical conditions
– CAD, HTN, lipid abnormalities, metabolic syndrome, obesity, vascular disease, ETOH, smoking Hx
• Nursing Leadership– Develop/implement algorithms or care pathways to
optimize use of evidence-based therapies
– Admission order sets to include specialty consultation and treatment of medical conditions that place patients at high risk for HF
– Ensure RN’s understand education principles to deliver patient self-care education
Albert NM, Lewis C. Critical Care Nurse 2008;28(2):20-37.

Nursing LeadershipStage B: Left Ventricular Systolic Dysfunction (structural heart disease) but Pre Heart Failure (Asymptomatic)
Albert NM, Lewis C. Critical Care Nurse 2008;28(2):20-37.
• Therapies: ACE-I, Beta blockers, ICD– Post MI discharge therapies:
• Statins• Aldosterone antagonists• Antiplatelet agents• Smoking cessation• Cardiac rehabilitation• Control BP as needed• Low fat diet• Loose weight, as needed• Clopidogrel (if PCI)

Nursing Leadership
Stage C: Left Ventricular Systolic Dysfunction (structural heart disease) and current or past symptoms of heart failure
• Therapies: ACE-I, Beta blockers, ICD– Post MI discharge therapies:
• Same as Stage B, but if EF </= 35%, – Aldosterone antagonist therapy
– Eplerenone– Spironolactone
Jessup M, Abraham WT, Casey DE, et al. JACC. 2009;53:online 03/26/09.

Median, 33.3Mean, 35.0
Variation in Outpatient HF Care:IMPROVE-HF (LVEF ≤ 35%)
Fonarow GC, et al. Circ Heart Fail. 2008;1:98–106.

Nursing Leadership
Stage B or C heart failure: Pre Heart Failure and Clinical Heart Failure
Albert NM, Lewis C. Critical Care Nurse 2008;28(2):20-37.
• Nursing Leadership– Patient education materials /delivery– Admitting order set with criteria for use– Pre-printed discharge instructions– Algorithm for follow up care after discharge– Reminder systems or check lists – Ongoing quality monitoring – Preventive therapies (flu shot)– Transition care (from hospital to home)*

CV Protection is in Your Hands
Be a patient Advocate & Champion