Asymmetric dimethylarginine levels in children with sickle cell disease and its correlation to...
7
ORIGINAL ARTICLE Asymmetric dimethylarginine levels in children with sickle cell disease and its correlation to tricuspid regurgitant jet velocity Mohamed El-Shanshory 1 , Ibrahim Badraia 1 , Amr Donia 1 , Faten Abd El-hameed 1 , Mokhtar Mabrouk 2 1 Department of Pediatrics, Faculty of Medicine, University of Tanta, Tanta; 2 Department of Pharmaceutical Chemistry, Faculty of Pharmacy, University of Tanta, Tanta, Egypt Abstract Background: Pulmonary hypertension (PH) is an increasingly recognized life-threatening complication in sickle cell disease (SCD), with associated high mortality in adults. The prevalence of PH in children with SCD is still unknown. The etiology and pathophysiologic mechanisms are still not well understood. Aim of the study: To assess the plasma levels of asymmetric dimethylarginine (ADMA) in children with SCD and its correlation with elevated tricuspid regurgitant jet velocity and other hemolytic markers. Subjects & Methods: This study was carried out on a cohort of patients (30) with SCD and 30 healthy children as a control group. Certain investigations were carried out for all subjects: CBC, lactate dehydrogenase (LDH), ferritin, reticulocytic count, bilirubin, AST, ALT, and plasma levels of ADMA. Doppler echocardiography was carried out for all subjects. Results: The prevalence of high tricuspid regurgitant velocity (TRV) was 30% in SCD patients. ADMA mean plasma level was significantly higher in patients than in controls (0.79 0.15 lmol/L and 0.46 0.11 lmol/L, respectively, P < 0.001). ADMA was significantly higher in patients with high TRV than those with normal TRV (1.10 0.11 lmol/L, 0.80 0.06 lmol/L, respectively, P < 0.001). There was a significant positive correlation between ADMA plasma levels and TRV 2.5 m/s (r = 0.475). Conclusion: High plasma ADMA levels may be implicated in the pathogenesis of increased tricuspid regurgitant jet velocity in children with SCD. Key words sickle cell disease; tricuspid regurgitant jet velocity; asymmetric dimethylarginine Correspondence M. El-Shanshory, Department of Pediatrics, Faculty of Medicine, University of Tanta, Tanta, Egypt. Tel: +20 1005680834; Fax: +20 403407734; e-mail: [email protected] Accepted for publication 27 March 2013 doi:10.1111/ejh.12114 Sickle cell disease (SCD) is a hemoglobinopathy that fea- tures hemoglobin polymerization, resulting in erythrocyte rigidity, hemolysis, and elements of endothelial dysfunction. Increased expression of adhesion molecules on erythrocytes and endothelial cells, interactions with leukocytes, increased levels of circulating inflammatory cytokines, enhanced micro vascular thrombosis, and endothelial damage are all thought to contribute to obstruction of the arterioles by sickled erythrocytes (1). Endothelial dysfunction, defined as alterations in the normal properties of the endothelium that are inappropriate for preservation of organ function, is char- acterized by loss of protective endothelial characteristics. Endothelial dysfunction is characterized by decreased production and/or bioavailability of nitric oxide (NO) (2). Among the mechanisms for impaired NO synthesis is the accumulation of the endogenous nitric oxide synthase inhibitor (NOS), asymmetric dimethylarginine (ADMA) (3). ADMA is a naturally occurring amino acid. Methylated arginine derivatives were first isolated from human urine in 1970 (4). In 1992, Vallance et al. (5) first described ADMA as an endogenous inhibitor of the arginine-NO pathway. From then, the role of this molecule in the regulation of endothelial NO synthesis has increasingly attracted attention (6). ADMA is synthesized during the methylation of protein arginine residues by S-adenosylmethionine: protein argi- nine methyltransferases [protein methylases, (PRMT)]. These enzymes transfer the methyl group from S-adenosylmethio- nine (SAM) to arginine thus forming methylated arginine © 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 55 European Journal of Haematology 91 (55–61)
Transcript of Asymmetric dimethylarginine levels in children with sickle cell disease and its correlation to...

ORIGINAL ARTICLE
Asymmetric dimethylarginine levels in children with sicklecell disease and its correlation to tricuspid regurgitant jetvelocityMohamed El-Shanshory1, Ibrahim Badraia1, Amr Donia1, Faten Abd El-hameed1, Mokhtar Mabrouk2
1Department of Pediatrics, Faculty of Medicine, University of Tanta, Tanta; 2Department of Pharmaceutical Chemistry, Faculty of Pharmacy,
University of Tanta, Tanta, Egypt
Abstract
Background: Pulmonary hypertension (PH) is an increasingly recognized life-threatening complication in
sickle cell disease (SCD), with associated high mortality in adults. The prevalence of PH in children with
SCD is still unknown. The etiology and pathophysiologic mechanisms are still not well understood. Aim of
the study: To assess the plasma levels of asymmetric dimethylarginine (ADMA) in children with SCD and
its correlation with elevated tricuspid regurgitant jet velocity and other hemolytic markers. Subjects &
Methods: This study was carried out on a cohort of patients (30) with SCD and 30 healthy children as a
control group. Certain investigations were carried out for all subjects: CBC, lactate dehydrogenase (LDH),
ferritin, reticulocytic count, bilirubin, AST, ALT, and plasma levels of ADMA. Doppler echocardiography
was carried out for all subjects. Results: The prevalence of high tricuspid regurgitant velocity (TRV) was
30% in SCD patients. ADMA mean plasma level was significantly higher in patients than in controls
(0.79 � 0.15 lmol/L and 0.46 � 0.11 lmol/L, respectively, P < 0.001). ADMA was significantly higher in
patients with high TRV than those with normal TRV (1.10 � 0.11 lmol/L, 0.80 � 0.06 lmol/L,
respectively, P < 0.001). There was a significant positive correlation between ADMA plasma levels and
TRV � 2.5 m/s (r = 0.475). Conclusion: High plasma ADMA levels may be implicated in the pathogenesis
of increased tricuspid regurgitant jet velocity in children with SCD.
Key words sickle cell disease; tricuspid regurgitant jet velocity; asymmetric dimethylarginine
Correspondence M. El-Shanshory, Department of Pediatrics, Faculty of Medicine, University of Tanta, Tanta, Egypt. Tel: +20
1005680834; Fax: +20 403407734; e-mail: [email protected]
Accepted for publication 27 March 2013 doi:10.1111/ejh.12114
Sickle cell disease (SCD) is a hemoglobinopathy that fea-tures hemoglobin polymerization, resulting in erythrocyterigidity, hemolysis, and elements of endothelial dysfunction.Increased expression of adhesion molecules on erythrocytesand endothelial cells, interactions with leukocytes, increasedlevels of circulating inflammatory cytokines, enhanced microvascular thrombosis, and endothelial damage are all thoughtto contribute to obstruction of the arterioles by sicklederythrocytes (1). Endothelial dysfunction, defined asalterations in the normal properties of the endothelium thatare inappropriate for preservation of organ function, is char-acterized by loss of protective endothelial characteristics.Endothelial dysfunction is characterized by decreasedproduction and/or bioavailability of nitric oxide (NO) (2).
Among the mechanisms for impaired NO synthesis is theaccumulation of the endogenous nitric oxide synthaseinhibitor (NOS), asymmetric dimethylarginine (ADMA) (3).ADMA is a naturally occurring amino acid. Methylated
arginine derivatives were first isolated from human urine in1970 (4). In 1992, Vallance et al. (5) first described ADMAas an endogenous inhibitor of the arginine-NO pathway.From then, the role of this molecule in the regulation ofendothelial NO synthesis has increasingly attracted attention(6). ADMA is synthesized during the methylation of proteinarginine residues by S-adenosylmethionine: protein argi-nine methyltransferases [protein methylases, (PRMT)]. Theseenzymes transfer the methyl group from S-adenosylmethio-nine (SAM) to arginine thus forming methylated arginine
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 55
European Journal of Haematology 91 (55–61)

and S-adenosylhomocysteine (SAH); the latter is subsequentlyhydrolyzed to homocysteine (7). Upon proteolytic cleavage ofarginine-methylated proteins, free monomethylarginine(MMA), ADMA, or symmetric dimethylarginine (SDMA) isgenerated and released into the cytoplasm. MMA and ADMA,but not SDMA, act as endogenous NOS inhibitors (8). As onlyminor amounts of MMA are found in human plasma andSDMA has no direct effect on NOS activity, ADMA is nowthought to be the major type of endogenously generatedmethylated arginine (2). ADMA is hydrolyzed by dimethy-larginine dimethyl aminohydrolase (DDAH) to dimethylamineand citrulline (9). Pulmonary hypertension (PH) is a recog-nized complication of SCD, which occurs in approximately6–11% of adult patients with sickle cell anemia. However, itsprevalence in children is still unknown (10).
Patients and methods
Enrollment of patient
This study was conducted between April 2011 and April2012 at Hematology and Oncology Unit of Pediatric Depart-ment, Tanta University Hospital. This cross-sectional studywas carried out on 30 children with sickle cell disease (17homozygous sickle cell anemia ‘Hb SS’ and 13 sickle thal-assemia ‘Hb Sb’). Thirty healthy children were recruited asa control group matched in ethnic, age, and sex distribution.Only seven cases of the patient group were taking hydroxy-urea. All subjects were subjected to complete history takingand full clinical examination. The following data were takenfrom the medical records: HB electrophoresis analysis, chestX-ray, X-ray on head of femur, and abdominal ultrasound.
Laboratory determinations
Venous blood was drawn for hemoglobin levels, leukocyteand platelet counts, reticulocyte counts, lactate dehydrogenase(LDH), ferritin, alanine aminotransferase, aspartateaminotransferase, bilirubin, blood urea, and serum creatinine.Human plasma ADMA was analyzed using a commercialADMA ELISA Kit (Immundiagnostik AG, Stubenwald-Allee8a, D 64625 Bensheim, made in Germany); citrated anti-coag-ulated plasma of all subjects was collected in complete aseptictechnique. Venous fasting blood samples were centrifuged atleast for 5 min at 10 000 g within 30 min of collection.Samples were frozen at �20°C till the measurement by ELISA.
Doppler echocardiography
Doppler echocardiography was carried out for all subjectsusing ultrasound machine, Vivid 7, G.E, at Tanta Universityhospital, Pediatric Department, Pediatric EchocardiographicLaboratory according to the standard protocol following theguidelines of the American Society of Echocardiography.
Subjects were screened for tricuspid regurgitant velocity(TRV) by echocardiography performed at steady state, definedas follows: � 2 wks from an acute illness including paincrisis, acute chest syndrome, febrile illness, or hospital admis-sion. TRV was measured by pulsed-wave and continuous-wave Doppler echocardiography where applicable. Multipleviews (apical 4-chamber, parasternal short axis, parasternallong axis) were obtained to record optimal tricuspid Dopplerflow signals, and a minimum of five sequential signals wererecorded (11, 12). Patients with pulmonary stenosis or otherstructural obstruction to pulmonary blood flow, evidence ofleft ventricular failure (defined as fraction shortening below28% and ejection fraction below 50%), atrial fibrillation orventricular tachycardia, significant mitral valve regurgitation>2/4 or mitral valve stenosis, severe pericardial effusion, andsubjects with no measurable TRV were excluded.
Statistics
The collected data were organized, tabulated, and statisti-cally analyzed using SPSS software statistical computer pack-age version 16 (SPSS Inc., Chicago, IL, USA). The numberand percent distribution of data was calculated. Chi-squarewas used as a test of significance and when found inappro-priate Fisher exact test was used. ANOVA test was used forcomparison among different times in the same group inquantitative data. Correlation between variables was evalu-ated using Spearman’s correlation coefficient. Significancewas adopted at P < 0.05 for interpretation of results of testsof significance.
Results
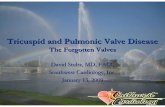
Patients characteristics and clinical and laboratory data areshown in Tables 1, 2, and 3. The prevalence ofTRV � 2.5 m/s in the studied cases was 30% (Table 4);nine patients with TRV 2.5–2.9 m/s and only four patientshad TRV � 3 m/s. Plasma ADMA levels were significantlyhigher in patient than in control group (Table 3) with asignificantly higher ADMA levels in patients withTRV � 2.5 m/s than in patients with TRV less than 2.5 m/s (Table 4). LDH, reticulocytic count, serum ferritin, andbilirubin levels were significantly higher in patients withTRV � 2.5 m/s when compared to patients withTRV < 2.5 m/s (Table 4). There were significant positivecorrelations between the plasma level of ADMA and LDH,reticulocytic count, ferritin, bilirubin, and tricuspid regurgit-ant jet velocity, while there was a negative correlation withHb level (Fig. 1).
Discussion
In the current study, the plasma ADMA levels were signifi-cantly higher in patient than in control group with a mean
56 © 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
ADMA levels in children with SCD El-Shanshory et al.

value 0.79 � 0.15 lmol, 0.46 � 0.11 lmol, respectively.Similar results were found by Schnog et al. (13), Kato et al.(14), and Landburg et al. 2010 (15).Elevated plasma ADMA levels lead to a reduced NO bio-
availability. Potential causes of elevated ADMA concentra-tions occur in SCD explained firstly due to increased releaseof free ADMA by increased proteolysis associated with theincreased erythrocyte turnover (13), which turn over at a rateup to twenty times normal (15). Furthermore, SCD is char-acterized by chronically elevated vascular wall shear stress(16), which is known to induce expression of endothelial
type-I protein arginine methyltransferase, a catalyst of argi-nine methylation (17). In addition, Billecke et al., (18)reported for the first time the presence of a large store ofprotein-incorporated ADMA in close proximity to the vascu-lar endothelium. This store could be released under certainpathological conditions. These findings may have clinicalimplications for those diseases displaying increased redblood cell (RBC) lysis and/or blood protein turnover. Davidset al., (19) also reported that intact erythrocytes play animportant role in storage of ADMA, whereas upon erythro-cyte lysis, large amounts of free ADMA are generated byproteolysis of methylated proteins, which may affect plasmalevels in hemolysis-associated diseases. The second causeoccurs due to impaired metabolism of ADMA followinginhibition of the DDAH, by oxidative stress triggered by
Table 1 Demographics of studied groups
Patients(n = 30)
Controls(n = 30) P-value
Age in years
(mean � SD)
6–18
(11.63 � 3.96)
6–18
(12.20 � 4.05)
0.586
M/F (%) 16 : 14
(53% : 47%)
17 : 13
(56.7% : 43.3%)
0.795
Table 2 Clinical characteristics of patient group
Medical history
Patients (n = 30)
Mean � SD Range
Interval between blood transfusion (wks) 4.2 � 1.9 2–7
% N
Cholelithiasis 10 3/30
Acute chest syndrome 3.3 1/30
A vascular necrosis 3.3 1/30
Stroke 3.3 1/30
Crises � 2/yr 26.7 8/30
ACS, acute chest syndrome; AVN, a vascular necrosis of femur.
Table 3 Laboratory data of studied groups
Parameter
Patients(n = 30)mean � SD
Controls(n = 30)mean � SD P-value
HB (gm/dL) 8.36 � 0.99 12 � 1.36 0.030*
MCV (fL) 77.3 � 11.4 80.1 � 3.5 0.663
MCH (pg) 25.9 � 4.2 29.8 � 2.3 0.057
Reticulocyte (%) 9.37 + 3.89 1 � 1.99 0.036*
White blood cell counts (thousands/lL) 10.395 � 1.56 7.036 � 1.85 0.042*
Platelet counts (thousands/lL) 458.2 � 75.6 355.5 � 68.9 0.006*
Lactic dehydrogenase (u/L) 370.6 � 128.49 185 � 58.5 0.044*
Ferritin (ng/mL) 2189.73 � 548.58 122.6 � 5.4 0.020*
Total bilirubin (mg/dL) 2 � 0.67 0.5 � 0.02 0.008*
Aspartate aminotransferase (U/L) 33.3 � 9.36 22.4 � 7.53 0.009*
Alanine aminotransferase (U/L) 23.5 � 4.7 17.2 � 2.6 0.362
Creatinine (mg/dL) 0.65 � 0.18 0.60 � 0.14 0.147
Urea (mg/dL) 26.4 � 13.5 28.4 � 8.2 0.089
ADMA (lmol/L) 0.79 � 0.15 0.46 � 0.11 0.007*
TRV (m/s) 2.387 � 0.551 2.14 � 0.2343 0.032*
ADMA, asymmetric dimethylarginine; TRV, tricuspid regurgitant velocity.
*Significant.
Table 4 Clinical and laboratory associations with TRV in SCD patients
TRV � 2.5 m/s(No. = 9/30) = 30%mean � SD
TRV < 2.5 m/s(No. = 21/30) = 70%mean � SD P-value
Age (yrs) 12.5 � 1.15 11.2 � 0.91 0.414
HB (gm/dL) 7.42 � 0.30 7.54 � 0.22 0.667
LDH (u/L) 935.7 � 83.79 406.3 � 45.19 0.001*
RETICS (%) 12.9 � 0.751 7.7 � 0.735 0.001*
Ferritin
(ng/mL)
3749 � 307.4 1521.4 � 273.77 0.001*
Bilirubin
(mg/dL)
2.48 � 0.185 1.79 � 0.133 0.008*
ADMA
(lmol/L)
1.10 � 0.11 0.80 � 0.06 0.001*
LDH, lactate dehydrogenase; SCD, sickle cell disease; ADMA,
asymmetric dimethylarginine.
*Significant.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 57
El-Shanshory et al. ADMA levels in children with SCD

several cardiovascular risk factors (20, 21). Also, hypoxiaand elevated levels of pro-inflammatory cytokines mayinhibit or down-regulate DDAH (22). Decreased DDAHexpression/activity is evident in disease states associatedwith endothelial dysfunction (23). It is notable that normalarginine metabolism is impaired in SCD through the loss ofde novo arginine synthesis from citrulline, which occurs pri-marily in the kidney. Renal dysfunction, a common occur-rence in SCD, will impair the major route for endogenousarginine biosynthesis (24). Plasma arginase activity is ele-vated in SCD as a consequence of inflammation, liver dys-function, and, most significantly, by the release oferythrocyte arginase during intravascular hemolysis, whichhas been demonstrated by the strong correlation betweenplasma arginase levels and cell-free hemoglobin levels andother markers of increased hemolytic rate (25). Low arginine
bioavailability may be exacerbated further by the presenceof elevated ADMA, which is a competitive inhibitor of argi-nine transport and all nitric oxide synthase isoenzymes (26).The state of activation or inhibition of NOS will depend onthe local intracellular concentrations of substrate and inhibi-tor, or the L-arginine/ADMA concentration ratio (27). Thus,even modest reductions in plasma arginine concentration cansignificantly impact cellular arginine uptake and bioavailabil-ity (25). On the other hand, other diseases without hemolysiscan induce ADMA elevation such as idiopathic PH (28),chronic renal failure, and moderately increased in patientswith many other diseases including hyperlipidemia, diabetesmellitus, arterial hypertension, hyperhomocysteinemia, andheart failure (7).Our results show that the prevalence of high
TRV (� 2.5 m/s) represents 30% of SCD children.
6
7
8
9
10 A
B
C
D
E
F
ADMA (umol/L)
HB
(gm
/dL)
1.251.151.050.950.850.750.65
1.251.151.050.950.850.750.65
1.251.151.050.950.850.750.65
1500
1000
500
0
ADMA (umol/L)
LDH
(u/l)
r = –0.352
P = 0.021*
r = 0.749
P = 0.001
1.251.151.050.950.850.750.650
1000
2000
3000
4000
ADMA (umol/L)
ferri
tin (n
g/m
l)
r = 0.707
P = 0.001
1.251.151.050.950.850.750.652
7
12
17
ADMA (umol/L)
Ret
icul
ocyt
ic %
r = 0.615
P = 0.001
2
3
4
ADMA (umol/L)
TJV
(m/s
)
1.251.151.050.950.850.750.65
1
2
3
ADMA (umol/L)
bilir
ubin
(mg/
dL)
r = 0.554
P = 0.001
r = 0.481, P = 0.007
Figure 1 Correlations between asymmetric dimethylarginine (ADMA) levels and Hb level (A), lactate dehydrogenase (LDH) (B), ferritin (C), reticul-
ocytic count (D), bilirubin (E), and tricuspid regurgitant velocity (TRV) (F) in patient group. The reference cutoff value for ADMA levels was
0.58 lmol/L.
58 © 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
ADMA levels in children with SCD El-Shanshory et al.

TRV � 2.5 m/s represents a threshold that is associatedwith increased hemolytic rate and oxygen desaturationduring 6-min walk test (29). However, it is still unclearwhether this measurement in SCD reflects true pulmonaryhypertension per se or is a biomarker of disease severity andsystemic vasculopathy (30). Also, Voskaridou et al., (31)found that the prevalence of high TRV in their study was33%. This is similar to prevalence in previous pediatric stud-ies (32, 33, 34, 35). Prevalence of elevated TRV in the pedi-atric population of SCD is almost comparable to occurrencesin the adult population, although similar effects on mortalityare not observed (36).However, the prevalence and prognosis of PH in children
with SCD remain largely unknown despite retrospectivestudies that suggest a similar prevalence to adults (34, 35).As the pathophysiological changes that lead to developmentof PH may be reversible in children, it may be necessaryto do effective screening of PH using TRV measurementsto select candidates for RHC. On the other hand, Qureshiet al., (37) reported only 16% prevalence of high TRV inSCD; however, their study was carried out on subjects asyoung as 6 months, too early for development of pulmo-nary hypertension. Minniti C et al., (38) showed that theprevalence of elevated tricuspid regurgitant velocity was11%, which is lower than the prevalence in most of theprevious studies of pediatric sickle cell disease patients(32). This could be due to using a threshold of 2.6 m/s ormore in their study.This study demonstrates that age and HB levels were not
significantly associated with high TRV, while reticulocytecount, LDH, ferritin, and bilirubin levels were significantlycorrelated to high TRV. A similar observation was made byQureshi et al., (37) and Pashankar et al., (32). The dataemerging from the PUSH study and others provide addi-tional evidence to suggest that children with a high TRVrepresent a sicker subpopulation of pediatric SCD patients(39). These children will likely grow up to be adults with anelevated TRV (11).Minniti et al., (38) generated the ‘hemolytic index’ by
principal component analysis of the levels of lactate dehy-drogenase, aspartate aminotransferase, bilirubin, and reticulo-cyte count. This hemolytic index (and not Hb levels) wascorrelated with high TRV in their children subjects withSCD. These children may still be at greater risk of complica-tions in young adulthood and warrant close observation (40).Ataga et al., (41) found that high TRV was correlated withthe degree of hemolysis as manifested by significantly higherlactate dehydrogenase and bilirubin, lower hemoglobin, andhematocrit levels. However, after statistical adjustment forage and sex, increased serum LDH was not associated withincreased TRV. Voskaridou et al., (31) found that patientswith high TRV had elevated values of reticulocyte countsand serum ferritin compared with patients with normal TRV.This is consistent with Ambrusko et al., (34) who found that
elevated TRV is associated with low hemoglobin and ele-vated reticulocyte count. Also, Gladwin et al., 2004 (11)demonstrated a TRV � 2.5 m/s is a risk factor for PH inSCD, and screening for SCD-related PH with echocardiogra-phy is generally recommended in adults with SCD. In con-trast, Pashankar et al., 2008 (32), Suell et al. 2005 (35), andKato et al. (42) did not find a significant associationbetween markers of hemolysis and high TRV.This study demonstrates that ADMA is significantly
higher in patients with high TRV than in patients with nor-mal TRV. This is consistent with Kato et al., 2009 whonoticed that ADMA levels in patients with SCD are linkedto high TRV (43). A similar observation was found byLandburg et al., (15) who reported that plasma ADMA con-centrations were significantly higher in patients with highTRV. Moreover, plasma ADMA concentrations were identi-fied as a risk factor for early death in SCD. Also, Landburget al., (16) identified an association of plasma ADMA con-centrations with high TRV and hence risk of PH in SCD,possibly identifying a novel factor of importance in itspathophysiology. They hypothesize that chronic hemolysis-induced ADMA elevations significantly contribute to endo-thelial activation and dysfunction in SCD via NOS inhibitionand that patients with higher ADMA concentrations aremore prone to develop a vasculopathy leading to complica-tions such as PH over time. Multivariate analysis was carriedout and showed that high TRV was significantly associatedwith high ferritin, high reticulocytic count, high bilirubin,and high ADMA. In addition, ADMA was associated signifi-cantly with high LDH, high reticulocytic count, high ferritin,and high serum bilirubin. Although difference in ADMAbetween patients with and without high TRV seems modest,even small increases in extracellular ADMA lead to signifi-cant intracellular NOS inhibition through preferred cellularADMA uptake over arginine (44). Although ADMA levelsare now documented by literature to be associated with bio-markers of hemolytic rate, yet this is the first study to dem-onstrate this on children.The present study has some limitations that deserve men-
tion. First of all, our study includes relatively a small numberof patients. In addition, we used ELISA method for measure-ment of ADMA. Yokoro et al. (44) reported that ADMAhas been measured by HPLC/MS; however, these methodshave disadvantages such as difficulty in getting reproducibleresults and the necessity of using expensive instrument.Although the ELISA method is characterized by simplicity,sensitivity, and specificity and can measure the concentra-tions of ADMA in large numbers of samples efficiently (45),yet comparative studies revealed that ELISA overestimatesADMA concentration as compared with LC-MS/MS and itruns varyingly in different laboratories (46). So, Pecchiniet al. have showed in their study that appropriate calibrationis needed when ADMA is measured by ELISA (47). Anotherlimitation in our study is that echocardiography was used to
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 59
El-Shanshory et al. ADMA levels in children with SCD

estimate the TRV instead of performing a right heart cathe-terization to avoid subjecting the patients to invasive mea-sures (48). Parent et al. found that true pulmonaryhypertension, using right heart catheterization, was only 6%of SCD patients while it was 27% using the TRV threshold.However, Gladwin et al., 2004 (11) demonstrated aTRV � 2.5 m/s is a risk factor for PH in SCD and screen-ing for SCD-related PH with echocardiography is generallyrecommended in adults with SCD.
Conclusion
From this study, it can be concluded that the increasedtricuspid regurgitant jet velocity is common in pediatricSCD. ADMA may be implicated in the pathogenesis ofSCD; high plasma ADMA levels are a risk factor for hightricuspid regurgitant jet velocity in children with SCD, andit is correlated with the hemolytic markers.
Recommendation
Further pediatric studies are warranted to determine the roleof ADMA in children with SCD and its association with anelevated TRV, vasculopathy, and alterations of the argininemetabolome.
Funding
The authors declare no competing financial interests.
Reference
1. Hebbel RP, Osarogiagbon R, Kaul D. The endothelial biologyof sickle cell disease: inflammation and a chronic vasculopa-thy. Microcirculation 2004;11:129–51.
2. Ueda S, Yamagishi S, Okuda S. New pathways to renal dam-age: role of ADMA in retarding renal disease progression. JNephrol 2010;23:377–86.
3. Pope AJ, Karuppiah K, Cardounel AJ. Role of the PRMT-DDAH-ADMA axis in the regulation of endothelial nitricoxide production. Pharmacol Res 2009;60:461–5.
4. Kakimoto Y, Akazawa S. Isolation and identification of NG3NG- and NG3 WG-dimethylarginine, W-mono-, di-, and trim-ethyllysine, and glucosylgalactosyl- and galactosyl-s -hydroxy-lysine from human urine. J Biol Chem 1970;245:5751–8.
5. Vallance P, Leone A, Calver A, Collier J, Moncada S. Accu-mulation of an endogenous inhibitor of nitric oxide synthesisin chronic renal failure. Lancet 1992;339:572–5.
6. Siroen MP, Teerlink T, Nijveldt RJ, Prins HA, Richir MC,van Leeuwen PA. The clinical significance of asymmetricdimethylarginine. Annu Rev Nutr 2006;26:203–28.
7. Betowski J, Kedra A. Asymmetric dimethylarginine (ADMA)as a target for pharmacotherapy. Pharmacol Rep2006;58:159–78.
8. Tain YL, Huang LT. Asymmetric dimethylarginine: clinicalapplications in pediatric medicine. J Formos Med Assoc2011;110:70–7.
9. Millatt LJ, Whitley GS, Li D, Leiper J, Siragy H, Carey R,Johns R. Evidence for dysregulation of dimethylarginine dim-ethylaminohydrolase I in chronic hypoxia-induced pulmonaryhypertension. Circulation 2003;108:1493–8.
10. Savale L, Maitre B, Bachir D, Galacteros F, Simonneau G,Parent F. Pulmonary arterial hypertension and sickle cell dis-ease. Presse Med 2013;42:338–46.
11. Gladwin MT, Sachdev V, Jison ML, et al. Pulmonary hyper-tension as a risk factor for death in patients with sickle celldisease. N Engl J Med 2004;350:886–95.
12. Lee MT, Small T, Khan MA, Rosenzweig EB, Barst RJ, Brit-tenham GM. Doppler-defined pulmonary hypertension and therisk of death in children with sickle cell disease followed fora mean of three years. Br J Haematol 2009;146:437–41.
13. Schnog JB, Teerlink T, van der Dijs FPL, Duits AJ, MuskietFAJ. Plasma levels of asymmetric dimethylarginine (ADMA),an endogenous nitric oxide synthase inhibitor, are elevated insickle cell disease. Ann Hematol 2005;84:282–6.
14. Kato GJ, Wang Z, Machado RF, Blackwelder WC, TaylorJG, Hazen SL. Endogenous nitric oxide synthase inhibitors insickle cell disease: abnormal levels and correlations withpulmonary hypertension, desaturation, haemolysis, organdysfunction and death. Br J Haematol 2009;145:506–13.
15. Landburg PP, Teerlink T, Biemond BJ, Brandjes DP, MuskietFA, Duits AJ, Schnog JB; CURAMA study group. Plasmaasymmetric dimethylarginine concentrations in sickle cell dis-ease are related to the hemolytic phenotype. Blood Cells MolDis 2010;44:229–32.
16. Landburg PP, Teerlink T, Muskiet FA, Duits AJ, Schnog JJ;CURAMA study group. Plasma concentrations of asymmetricdimethylarginine, an endogenous nitric oxide synthase inhibi-tor, are elevated in sickle cell patients but do not increase fur-ther during painful crisis. Am J Hematol 2008;83:577–9.
17. Osanai T, Saitoh M, Sasaki S, Matsunaga T, Okumura K.Effect of shear stress on asymmetric dimethylarginine releasefrom vascular endothelial cells. Hypertension 2003;42:985–90.
18. Billecke SS, Kitzmiller LA, Northrup JJ, Whitesall SE, Kim-oto M, Hinz AV, D’Alecy LG. Contribution of whole bloodto the control of plasma asymmetrical dimethylarginine. Am JPhysiol Heart Circ Physiol 2006;291:H1788–96.
19. Davids M, van Hell AJ, Visser M, Nijveldt RJ, van LeeuwenPA, Teerlink T. Role of the human erythrocyte in generationand storage of asymmetric dimethylarginine. Am J PhysiolHeart Circ Physiol 2012;302:H1762–70.
20. De Gennaro Colonna V, Bianchi M, Pascale V, Ferrario P,Morelli F, Pascale W, Tomasoni L, Turiel M. Asymmetricdimethylarginine (ADMA): an endogenous inhibitor of nitricoxide synthase and a novel cardiovascular risk molecule. MedSci Monit 2009;15:RA91–101.
21. B€oger RH. Asymmetric dimethylarginine, an endogenousinhibitor of nitric oxide synthase, explains the “L-arginineparadox” and acts as a novel cardiovascular. J Nutr2004;134:2842S–7S.
60 © 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
ADMA levels in children with SCD El-Shanshory et al.

22. Vladimirova-Kitova LG. Asymmetric dimethylarginine –
mechanisms and targets for therapeutic management. FoliaMed (Plovdiv) 2008;50:12–21.
23. Pope AJ, Karrupiah K, Xia Y, Cardounel AJ. Role of dime-thylarginine dimethylaminohydrolases in the regulation ofendothelial nitric oxide production. J Biol Chem 2009;18:284.
24. Morris CR. Mechanisms of vasculopathy in sickle cell diseaseand thalassemia. Haematology 2008;1:177–85.
25. Morris CR, Kato GJ. Dysregulated arginine metabolism,hemolysis-associated Pulmonary hypertension and mortality insickle cell disease. JAMA 2005;294:81–90.
26. Vallance P. The asymmetrical dimethylarginine/dimethylargi-nine dimethylaminohydrolase pathway in the regulation ofnitric oxide generation. Clin Sci 2001;100:159–60.
27. Teerlink T, Luo Z, Palm F, Wilcox CS. Cellular ADMA: reg-ulation and action. Pharmacol Res 2009;60:448–60.
28. Kielstein JT, Impraim B, Simmel S, Bode-B€oger SM, TsikasD, Fr€olich JC, Hoeper MM, Haller H, Fliser D. Cardiovascu-lar effects of systemic nitric oxide synthase inhibition withasymmetrical dimethylarginine in humans. Circulation2004;109:172–7.
29. Minniti CP, Sable C, Campbell A, et al. Elevated tricuspid re-gurgitant jet velocity in children and adolescents with sicklecell disease: association with hemolysis and haemoglobin oxy-gen desaturation. Haematologica 2009;94:340–7.
30. Kato GJ, Onyekwere OC, Gladwin MT. Pulmonary hyperten-sion in sickle cell disease: relevance to children. PediatrHematol Oncol 2007;24:159–70.
31. Voskaridou E, Tsetsos G, Tsoutsias T, Spyropoulou E, Chris-toulas D, Terpos E. Pulmonary hypertension in patients withsickle cell/b thalassemia: incidence and correlation with serumN-terminal pro-brain natriuretic peptide concentrations. Hae-matologica 2007;92:738–43.
32. Pashankar FD, Carbonella J, Bazzy-Asaad A, Friedman A.Prevalence and risk factors of elevated pulmonary artery pres-sures in children with sickle cell disease. Pediatrics2008;121:777–82.
33. Zuckerman WA, Rosenzweig EB. Pulmonary hypertension inchildren with sickle cell disease. Expert Rev Respir Med2011;5:233–43.
34. Ambrusko SJ, Gunawardena S, Sakara A, Windsor B, LanfordL, Michelson P, Krishnamurti L. Elevation of tricuspid re-gurgitant jet velocity, a marker for pulmonary hypertension inchildren with sickle cell disease. Pediatr Blood Cancer2006;47:907–13.
35. Suell MN, Bezold LI, Okcu F, Mahoney DH Jr, ShardonofskyF, Mueller BU. Increased pulmonary artery pressures amongadolescents with sickle cell disease. J Pediatr Hematol Oncol2005;27:654–8.
36. Akinsheye I, Klings ES. Sickle cell anemia and vascular dys-function: the nitric oxide connection. J Cell Physiol2010;224:620–5.
37. Qureshi N, Joyce JJ, Qi N. Right ventricular abnormalities insickle cell anemia: evidence of a progressive increase in pul-monary vascular resistance. J Pediatr 2006;149:23–7.
38. Minniti C, Sable C, Campbell A, et al. Elevated tricuspidregurgitant jet velocity in children and adolescents with sicklecell disease: association with hemolysis and hemoglobin oxy-gen desaturation. Haematologica 2009;94:340–7.
39. Gordeuk V, Minniti CP, Nouraie M, et al. Elevated tricuspidregurgitation velocity and decline in exercise capacity over22 months of follow up in children and adolescents withsickle cell anemia. Haematologica 2011;96:33–40.
40. Kato GJ, Gladwin MT, Steinberg MH. Deconstructing sicklecell disease: reappraisal of the role of hemolysis in the develop-ment of clinical subphenotypes. Blood Rev 2007 Jan;21:37–47.
41. Ataga KI, Sood N, Gent GD, Kelly E, Henderson AG, Jones S,Strayhorn D, Lail A, Lieff S, Orringer EP. Pulmonary hyperten-sion in sickle cell disease. Am J Med 2004;117:665–9.
42. Kato GJ, Hebbel RP, Steinberg MH, Gladwin MT. Vasculop-athy in sickle cell disease: biology, pathophysiology, genetics,translational medicine, and new research directions. Am JHematol 2009;84:618–25.
43. Wilcken DE, Sim AS, Wang J. Asymmetric dimethylarginine(ADMA) in vascular, renal and hepatic disease and the regula-tory role of L-arginine on its metabolism. Mol Genet Metab2007;91:309–17.
44. Yokoro M, Suzuki M, Yatani M, Yamashita H, Takahashi Y,Tsuji H, Kimoto M. Development of an enzyme-linked immu-nosorbent assay system for the determination of asymmetricdimethylarginine using a specific monoclonal antibody. BiosciBiotechnol Biochem 2012;76:400–3.
45. Tsikas D. Determination of asymmetric dimethylarginine inbiological fluids: a paradigm for a successful analytical story.Curr Opin Clin Nutr Metab Care 2008;11:592–600.
46. Pecchini P, Malberti F, Mieth M, Quinn R, Tripepi G, Mal-lamaci F, Maas R, Zoccali C, Ravani P. Measuring asymmet-ric dimethylarginine (ADMA) in CKD: a comparison betweenenzyme-linked immunosorbent assay and liquid chromatogra-phy-electrospray tandem mass spectrometry. J Nephrol2012;25:1016–22.
47. El-Beshlawy A, Youssry I, El-Saidi S, El Accaoui R, MansiY, Makhlouf A, Taher A. Pulmonary hypertension in b-thalas-semia major and the role of L-carnitine therapy. PediatrHematol Oncol 2008;25:734–43.
48. Parent F, Bachir D, Inamo J, et al. A hemodynamic study ofpulmonary hypertension in sickle cell disease. N Engl J Med2011;365:44–53.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 61
El-Shanshory et al. ADMA levels in children with SCD