Asthma Medicine 5

of 52
Transcript of Asthma Medicine 5
-
8/14/2019 Asthma Medicine 5
1/52
Asthma Diagnosis &Asthma Diagnosis &Treatment:Treatment:
Update & Quality CareUpdate & Quality CareDr. Imad Salah Ahmed HassanDr. Imad Salah Ahmed Hassan
MD MRCP MScMD MRCP MScConsultant Physician & PulmonologistConsultant Physician & Pulmonologist
-
8/14/2019 Asthma Medicine 5
2/52
Burden of AsthmaBurden of Asthma
Asthma is one of the most common chronicdiseases worldwide
Prevalence increasing in many countries,especially in children
A major cause of school/work absence
An overall increase in severity of asthmaincreases the pool of patients at risk for death
-
8/14/2019 Asthma Medicine 5
3/52
Problem Scale: 350 million people around the globe
Deaths from this condition have reached 280,000 annually
Worldwide, costs of asthma greater than Tuberculosis
and HIV / AIDS
Major factors contributing to asthma morbidity andmortality are under-diagnosis and inappropriate treatment
Ref. WHO Fact Sheet N 206, Revised January 2001
GINA guidelines 1998
Bronchial AsthmaBronchial AsthmaFacts and FiguresFacts and Figures
-
8/14/2019 Asthma Medicine 5
4/52
HeadingsHeadings
Pathogenesis of AsthmaPathogenesis of Asthma
Diagnosing AsthmaDiagnosing Asthma
Treatment:Treatment:
Classification of severityClassification of severity
Therapeutic ModalitiesTherapeutic Modalities
Quality Care InterventionsQuality Care Interventions Indications for referral to the specialistIndications for referral to the specialist
Failed TreatmentFailed Treatment
-
8/14/2019 Asthma Medicine 5
5/52
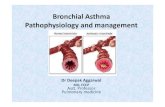
Pathogenesis of AsthmaPathogenesis of Asthma
Asthma is aAsthma is a chronic inflammatorychronic inflammatory disorderdisorder
of theof the airwaysairways.. Airway inflammation results in:Airway inflammation results in:
AirwayAirway obstructionobstruction through airway edema, mucusthrough airway edema, mucus
plugs and bronchoconstriction.plugs and bronchoconstriction.AirwayAirway hyperresponsiveness.hyperresponsiveness.
AirwayAirway remodeling.remodeling.
-
8/14/2019 Asthma Medicine 5
6/52
Pathogenesis of AsthmaPathogenesis of Asthma
Understanding of the airway inflammatory processUnderstanding of the airway inflammatory process
continues to evolvecontinues to evolve
mast cellsmast cells eosinophilseosinophils
airway epithelial cellsairway epithelial cells
lymphocytes (Th2 response)lymphocytes (Th2 response)
cytokinescytokines
leukotrienesleukotrienes
-
8/14/2019 Asthma Medicine 5
7/52
-
8/14/2019 Asthma Medicine 5
8/52
-
8/14/2019 Asthma Medicine 5
9/52
Symptoms and use of reliever
medication
Time
Exacerbation
Oral course of
steroids
Effect of steroids during
periods of worsening
Exacerbation
Asthma is aAsthma is a variablevariable diseasedisease
Medication plans need to accommodate variability among patients as
well as within individual patients over time. An essential aspect of any
treatment plan is the need to monitor the effect of the treatment and
adapting the treatment to the variability of the asthma (GINA 2002).
-
8/14/2019 Asthma Medicine 5
10/52
What isWhat is inin Bronchial Asthma?Bronchial Asthma?
Chronic inflammatory diseaseChronic inflammatory disease
Long-term therapy and care: financial,Long-term therapy and care: financial,
psychosocial, medication S/Epsychosocial, medication S/E
compounding it.compounding it.
Intermittent or persistent withIntermittent or persistent with
progressive loss of lung function.progressive loss of lung function.
Dynamic severity dictate the choice ofDynamic severity dictate the choice of
therapy: Stepwise approach.therapy: Stepwise approach.
May be fatal: no complacency is allowed.May be fatal: no complacency is allowed.
-
8/14/2019 Asthma Medicine 5
11/52
Asthma Care PlanAsthma Care Plan
Is it Asthma?Is it Asthma?
Assessment of Severity?Assessment of Severity?
Pharmacological and non-Pharmacological and non-
pharmacological therapy?pharmacological therapy?
Can I prevent re-modelling?Can I prevent re-modelling? Monitoring.Monitoring.
Prevention of Asthma.Prevention of Asthma.
Six-part Asthma Management ProgramSix-part Asthma Management Program
-
8/14/2019 Asthma Medicine 5
12/52
Asthma Care PlanAsthma Care Plan
Is it Asthma?Is it Asthma?
Detailed medical history: symptoms of asthma,Detailed medical history: symptoms of asthma,
aggravators etcaggravators etc
FH/SH/Occupational History/DrugFH/SH/Occupational History/Drug
History/AllergiesHistory/Allergies
Physical examPhysical exam
Spirometry to demonstrate reversibilitySpirometry to demonstrate reversibility
-
8/14/2019 Asthma Medicine 5
13/52
Diagnosis of Asthma: History
Episodes (especially recurrent) of cough,
wheeze, shortness of breath or chesttightness
Colds that go to the chest and stay there for> 10 days
-
8/14/2019 Asthma Medicine 5
14/52
Diagnosis of Asthma: HistoryDiagnosis of Asthma: History
Cough, wheeze, shortness of breath or chest
tightness during particular seasons (Fall orSpring) or with certain exposures (animals,smoke, or strong odors) or under certainconditions (exercise or strong emotions)
Use of over-the-counter medications(inhalers) which relieve these symptoms
-
8/14/2019 Asthma Medicine 5
15/52
Historical Clues to Asthma
Childhood lung disease (BPD, parentalChildhood lung disease (BPD, parental
smoking, pneumonias)smoking, pneumonias)
Allergies, hay fever, sinusitis, rhinitis, nasalAllergies, hay fever, sinusitis, rhinitis, nasal
polyps, eczema, aspirin sensitivitypolyps, eczema, aspirin sensitivity
Family history of asthmaFamily history of asthma
-
8/14/2019 Asthma Medicine 5
16/52
Asthma Care PlanAsthma Care Plan
Is it Asthma: SpirometryIs it Asthma: Spirometry
Home PEFR Charting:Home PEFR Charting: 20%20% dipsdips FEVFEV11 < 80%< 80% predicted;predicted;
FEVFEV11/FVC/FVC 12%12% andand
at leastat least 200200 ml after using a short-acting inhaledml after using a short-acting inhaledbetabeta22-agonist.-agonist.
-
8/14/2019 Asthma Medicine 5
17/52
Asthma Care PlanAsthma Care Plan
Is it Asthma: SpirometryIs it Asthma: Spirometry
Steroid Trial: Increase bySteroid Trial: Increase by 12%12% in FEV1 afterin FEV1 afteraa 22 wks PO steroid orwks PO steroid or66 wks inhaled steroid.wks inhaled steroid.
Exercise test.Exercise test.
Methacholine challengeMethacholine challenge
-
8/14/2019 Asthma Medicine 5
18/52
Patient/parent Confident ;to manage own medication,
increasing and decreasing usingPEF,
start oral steroid and attend clinic.
Patient/parent Knows ;how to monitor PEF & symptoms,
when to increase dose of inhaledsteroids,
how to contact med practice.
Patient/parent ACCEPTS & AGREES ;about use of medication,
importance of preventers,
recognition of symptoms.
Ladder of Asthma Knowledge
Patient/parent UNDERSTANDS ;what relief medication does,
side effects which may occur,
aims of treatment,
what is happening to them in their chest,educational material is made available.
3
1
2
4
3
1
2
4
-
8/14/2019 Asthma Medicine 5
19/52
Additional TestsAdditional Tests
Reasons for Additional TestsReasons for Additional Tests The TestsThe TestsPatient has symptoms but spirometry
is normal or near normal.
Assess diurnal variation of peak flow
over 1 to 2 weeks.
Refer to a specialist for
bronchoprovocation with methacholine ,histamine, or exercise; negative test
may help rule out asthma.
Suspect infection (TB), large airway lesions, heart
disease, orobstruction by foreign object
Chest x-ray
-
8/14/2019 Asthma Medicine 5
20/52
Additional TestsAdditional Tests
Reasons for Additional TestsReasons for Additional Tests The TestsThe Tests
.
Suspect coexisting chronic obstructive pulmonary
disease, restrictive defect, or central airway
obstruction
Additional pulmonary function studies
Diffusing capacity test
Suspect other factors contribute to asthma
(These are not diagnostic tests for asthma.) Allergy testsskin or in vitro
Nasal examination
Gastroesophageal
reflux assessment
-
8/14/2019 Asthma Medicine 5
21/52
Asthma Care PlanAsthma Care Plan
Assessment of Severity?Assessment of Severity?
SymptomsSymptoms
SpirometrySpirometry
OthersOthers
-
8/14/2019 Asthma Medicine 5
22/52
Classification of SeverityClassification of Severity
CLASSIFY SEVERITYClinical Features Before Treatment
SymptomsSymptoms NocturnalNocturnalSymptomsSymptoms
FEVFEV11 or PEFor PEF
STEP 4STEP 4
SevereSevere
PersistentPersistent
STEP 3STEP 3
ModerateModeratePersistentPersistent
STEP 2STEP 2
MildMildPersistentPersistent
STEP 1STEP 1
MildMild
IntermittentIntermittent
ContinuousContinuous
Limited physicalLimited physicalactivityactivity
DailyDaily
Attacks affect activityAttacks affect activity
> 1 time a week> 1 time a week
but < 1 time a daybut < 1 time a day
< 1 time a week< 1 time a week
Asymptomatic andAsymptomatic and
normal PEFnormal PEF
between attacksbetween attacks
FrequentFrequent
> 1 time week> 1 time week
> 2 times a month> 2 times a month
< 2 times a month2 times a month
60% predicted60% predicted
Variability > 30%Variability > 30%
60 - 80% predicted60 - 80% predicted
Variability > 30%Variability > 30%
80% predicted80% predicted
Variability 20 - 30%Variability 20 - 30%
80% predicted80% predicted
Variability < 20%Variability < 20%
The presence of one feature of severity is
sufficient to place patient in that category.
-
8/14/2019 Asthma Medicine 5
23/52
Seven Goals Asthma Management ProgramSeven Goals Asthma Management Program
Goals of Long-term ManagementGoals of Long-term Management
Achieve and maintain control of symptomsAchieve and maintain control of symptoms
Prevent asthma episodes or attacksPrevent asthma episodes or attacks
Maintain pulmonary function as close toMaintain pulmonary function as close to
normal levels as possiblenormal levels as possible Maintain normal activity levels, includingMaintain normal activity levels, including
exerciseexercise
Avoid adverse effects from asthmaAvoid adverse effects from asthmamedicationsmedications
Prevent development of irreversible airflowPrevent development of irreversible airflowlimitationlimitation
Prevent asthma mortalityPrevent asthma mortality
-
8/14/2019 Asthma Medicine 5
24/52
Therapy:Therapy:
Control of AsthmaControl of Asthma
Least cost from medicationLeast cost from medication
-
8/14/2019 Asthma Medicine 5
25/52
Bronchial
Asthma
Avoidance of
Triggers
Pharmacotherapy Immunotherapy
Inhalants
IngestantsBronchodilators
Anti-inflammatory
Drugs
Desensitization
IgE Antibodies
Control of
Aggravators
GERD
Sinusitis
Smoking
Drugs
Non-Pharmacological
Education
-
8/14/2019 Asthma Medicine 5
26/52
Pharmacotherapy in AsthmaPharmacotherapy in Asthma
A stepwise approach to pharmacological therapy isA stepwise approach to pharmacological therapy is
recommendedrecommended
The aim is to accomplish the goals of therapy withThe aim is to accomplish the goals of therapy with
the least possible medicationthe least possible medication
Although in many countries traditional methods ofAlthough in many countries traditional methods ofhealing are used, their efficacy has not yet beenhealing are used, their efficacy has not yet been
established and their use can therefore not beestablished and their use can therefore not be
recommendedrecommended
-
8/14/2019 Asthma Medicine 5
27/52
Pharmacotherapy in AsthmaPharmacotherapy in Asthma
Mild, intermittentMild, intermittent
as-needed relieveras-needed reliever
Mild, persistentMild, persistent
as-needed relieveras-needed reliever
controllercontroller
Moderate, persistentModerate, persistent
as-needed relieveras-needed reliever
two controllerstwo controllers
Severe, persistentSevere, persistent
as-needed relieveras-needed reliever
two controllerstwo controllers High dose ICS andHigh dose ICS and
possibly oral CSpossibly oral CS
-
8/14/2019 Asthma Medicine 5
28/52
Relievers in Bronchial Asthma
Rapid-acting inhaled 2-agonistsSalbutamol, Terbutaline
Inhaled Long-acting 2-agonistsFormoterol
AnticholinergicsIpratropium
MethylxanthinesTheophylline
Short-acting oral 2-agonists
Salbutamol, Terbutaline
-
8/14/2019 Asthma Medicine 5
29/52
Long Term ControllersLong Term Controllers
1.1. Inhaled glucocorticosteroidsInhaled glucocorticosteroids
2.2. Long-acting inhaled 2-agonistsLong-acting inhaled 2-agonists
3.3. Leukotriene modifiersLeukotriene modifiers
4.4. Systemic glucocorticosteroidsSystemic glucocorticosteroids
5.5. CromonesCromones
6.6. MethylxanthinesMethylxanthines
7.7. Long-acting oral 2-agonistsLong-acting oral 2-agonists
8.8. Anti-IgEAnti-IgE
-
8/14/2019 Asthma Medicine 5
30/52
Whats New in the Guidelines?Whats New in the Guidelines?
When to Use INHALED STEROIDSWhen to Use INHALED STEROIDS
Early use is recommendedEarly use is recommended
HIGH vs LOW DOSE inhaled steroidsHIGH vs LOW DOSE inhaled steroidsHigh doses of inhaled glucocorticosteroids: limitedHigh doses of inhaled glucocorticosteroids: limited
benefit and potential adverse eventsbenefit and potential adverse events
Therefore add other therapies to moderate dosesTherefore add other therapies to moderate doses
-long-acting 2-agonists-long-acting 2-agonists
-leukotriene receptor antagonists-leukotriene receptor antagonists
-theophylline-theophylline At the consensus conference most would consider high dose more than 1000At the consensus conference most would consider high dose more than 1000g. (400-500g. (400-500
in children BDP e uivalentg in children) BDP equivalent
-
8/14/2019 Asthma Medicine 5
31/52
Whats New in the Guidelines?Whats New in the Guidelines?
Place of long actingPlace of long acting 2 AGONISTS2 AGONISTS Many studies have repeatedly demonstrated that adding aMany studies have repeatedly demonstrated that adding a
long-acting beta2-agonist to a lower dose of inhaledlong-acting beta2-agonist to a lower dose of inhaled
corticosteroids produces superior outcomes compared withcorticosteroids produces superior outcomes compared with
doubling or even greater dosage increases in the ICdoubling or even greater dosage increases in the IC Sole use (Salmeterol) may be fatalSole use (Salmeterol) may be fatal
Place of anti-Leukotriene blockersPlace of anti-Leukotriene blockers Improves lung function when added to inhaledImproves lung function when added to inhaled
corticosteroidscorticosteroids
Not as effective as inhaled corticosteroidsNot as effective as inhaled corticosteroids
-
8/14/2019 Asthma Medicine 5
32/52
Add-on ControllersAdd-on Controllers
Long-acting inhaledLong-acting inhaled 22-agonists-agonistsEffective bronchodilators for 12 hoursEffective bronchodilators for 12 hours
Protects against nocturnal asthmaProtects against nocturnal asthmaProtects against exercise inducedProtects against exercise induced
asthmaasthma
Improves asthma control more thanImproves asthma control more thanincreasing dose of inhaledincreasing dose of inhaledcorticosteroidscorticosteroids
Allow a reduction in the dose ofAllow a reduction in the dose ofinhaled steroid.inhaled steroid.
-
8/14/2019 Asthma Medicine 5
33/52
Long-acting Inhaled 2-Long-acting Inhaled 2-
agonistsagonists
Regular use with inhaled corticosteroidsRegular use with inhaled corticosteroids
reduces the rate of both mild and severereduces the rate of both mild and severe
exacerbations in asthmaexacerbations in asthma
May be considered as an alternative to increased dosesMay be considered as an alternative to increased doses
of inhaled steroids and should be used as add-onof inhaled steroids and should be used as add-on
therapy to glucocorticosteroidstherapy to glucocorticosteroids
Formoterol but not Salmeterol may be used for reliefFormoterol but not Salmeterol may be used for relief
of acute symptomsof acute symptoms
-
8/14/2019 Asthma Medicine 5
34/52
Add-on ControllersAdd-on Controllers
MontelukastMontelukast
Improves lung function and asthma controlImproves lung function and asthma control
May protect against exercise induced andMay protect against exercise induced and
aspirin-induced bronchoconstrictionaspirin-induced bronchoconstriction
Improves lung function when added to inhaledImproves lung function when added to inhaled
corticosteroidscorticosteroidsNot as effective as inhaled corticosteroidsNot as effective as inhaled corticosteroids
-
8/14/2019 Asthma Medicine 5
35/52
AsthmaAsthma Non-pharmacologicalNon-pharmacological
Quality of Care IssuesQuality of Care Issues
Education:Education:
What is AsthmaWhat is Asthma
Avoidance of Precipitants/Triggers:Avoidance of Precipitants/Triggers: Environmental ControlEnvironmental Control
Recognition of symptoms of poor-controlRecognition of symptoms of poor-control
Self-management plan:Self-management plan:
Home Peak Flow MeterHome Peak Flow Meter
Partnership AgreementPartnership Agreement
Regular Follow-up:Regular Follow-up: at least every 1 to 6 months.at least every 1 to 6 months.
Follow-up Indices of Control (Follow-up Indices of Control (Follow-up FormFollow-up Form))
-
8/14/2019 Asthma Medicine 5
36/52
Asthma Action PlanAsthma Action Plan
(PEFR-Based Self Management Plan)(PEFR-Based Self Management Plan)
Best
-
8/14/2019 Asthma Medicine 5
37/52
Asthma Action PlanAsthma Action Plan
(Symptom-Based Self Management Plan)(Symptom-Based Self Management Plan)
Asthma under control
Waking with asthma at night
Increased breathlessness or
poor response to
Severe attack
Continue regular treatment
Double dose of:
Start prednisone & ring
Doctor
Call emergency Dr. or Dial
---- for ambulance
-
8/14/2019 Asthma Medicine 5
38/52
-
8/14/2019 Asthma Medicine 5
39/52
. . ( ). %100-80
/1 ( )( ) ( )( )
.
2/
( )( )
/3 .......
: 3
. . %80 50
.
/1 ( )
( ) ( )( )
.
. 2/
:
.
. %50 .
()Prednisolone ( )1/
( ) ( )
/2 ( )
( )( )( )
. . 3/
-
8/14/2019 Asthma Medicine 5
40/52
OBJECTIVE:
A morally and mutually beneficial gentlemans agreement to
enhance physician and
patient medical knowledge and
communication, set standards and targets for care and
impart a stronger sense of accountability on both.
The Physician-Asthma Patient
Partnership Agreement
-
8/14/2019 Asthma Medicine 5
41/52
You can expect your physician toprovide the following services, which
are an essential part of asthmamanagement.OFFICE VISITS- every three to twelve monthsfor reviewing your progress or as frequently as yourcondition dictates.MONITORINGin every Visit Weight, lungfunction, oxygen saturation and other vital signs.EDUCATION:Provision of educational material,education by a pulmonary educator, review ofinhaler technique, provision of a self-management
The Physician-Asthma PatientPartnership Agreement
PHYSICIAN DUTIES/RESPONSIBILITIES
-
8/14/2019 Asthma Medicine 5
42/52
PERSONAL GOALS
The Physician-Asthma Patient
Partnership Agreement
PERSONAL GOALS
-
8/14/2019 Asthma Medicine 5
43/52
Current Weight/
Body MassIndex:
Goal for 3months:
Current PEFR:Ideal PEFR
Goal for 3months:
Goal for 3 months:
Current FEV1:Ideal FEV1
Goal for 3 months:
CurrentAsthma
symptoms:
Goal for 3 months:
Smoking: Y/N Goal for 3 months:
Frequency ofattacks/ER visit:
Goal for 3 months:
PERSONAL GOALS
-
8/14/2019 Asthma Medicine 5
44/52
YOUR RESPONSIBILITIES
Adhere to your allergen avoidance/smoke cessation instructions,
prescribed drugs and exercise advice.Schedulefollow-up appointments every three months or as
indicated by your doctor.Monitor Peak Expiratory Flow Rate at home at the agreed testing
frequency: _______.Always bring your prescribed medications with you.Worktoward attaining the personal goals noted above.
PATIENT SIGNATURE/ Date:
PHYSICIAN SIGNATURE/Date:
he Physician-Asthma PatientPartnership Agreement
PATIENT DUTIES/RESPONSIBILITIES
-
8/14/2019 Asthma Medicine 5
45/52
Asthma Care PlanAsthma Care Plan
Monitoring Asthma ControlMonitoring Asthma ControlFollow-up Indices of Control (Follow-up Indices of Control (Follow-up FormFollow-up Form))
Symptoms:Symptoms: Daytime and nighttime symptomsDaytime and nighttime symptoms
Severity:Severity: subjective and PEFR/Spirometrysubjective and PEFR/Spirometry
Compliance to therapy/Preventive MeasuresCompliance to therapy/Preventive Measures Use of inhaler/inhaler techniqueUse of inhaler/inhaler technique
Medication refillsMedication refills
Frequency of oral corticosteroid burst therapyFrequency of oral corticosteroid burst therapy
Side effects of medicationsSide effects of medications
Exacerbations/ER visitsExacerbations/ER visits
Psychofunctional /Social Impact:Psychofunctional /Social Impact: Missed work or schoolMissed work or school
-
8/14/2019 Asthma Medicine 5
46/52
Asthma Care PlanAsthma Care Plan
Indications for specialist referral:Indications for specialist referral:
s Patient has had a life-threateningPatient has had a life-threatening
asthma exacerbation.asthma exacerbation.
s Patient is not meeting the goals ofPatient is not meeting the goals of
asthma therapy.asthma therapy.
s Signs and symptoms are atypical.Signs and symptoms are atypical.
s Other conditions complicate asthma.Other conditions complicate asthma.
-
8/14/2019 Asthma Medicine 5
47/52
Asthma Care PlanAsthma Care Plan
Indications for specialist referral:Indications for specialist referral:
s Additional diagnostic testing is indicated.Additional diagnostic testing is indicated.
s Patient requires additional education.Patient requires additional education.
s Patient is being considered forPatient is being considered for
immunotherapy.immunotherapy.
s Patient has severe persistent asthma.Patient has severe persistent asthma.
-
8/14/2019 Asthma Medicine 5
48/52
Asthma Care PlanAsthma Care Plan
Indications for specialist referral:Indications for specialist referral:
s Patient requires continuous oralPatient requires continuous oral
corticosteroid therapy or high-dosecorticosteroid therapy or high-doseinhaled corticosteroids.inhaled corticosteroids.
s
ChildChild
-
8/14/2019 Asthma Medicine 5
49/52
Patient is not improving:Patient is not improving:
Wrong diagnosisWrong diagnosis
Inadequate/deficient treatmentInadequate/deficient treatment Poor inhaler techniquePoor inhaler technique
Uncontrolled aggravatorsUncontrolled aggravators
Continuous exposure to allergensContinuous exposure to allergens S/E of asthma therapy.S/E of asthma therapy.
-
8/14/2019 Asthma Medicine 5
50/52
Influence of pharmacotherapy on natural history of
disease still not well understood
Effect of Therapy on Remodelling?
-
8/14/2019 Asthma Medicine 5
51/52
Asthma in SudanAsthma in Sudan
No studies on epidemiologyNo studies on epidemiology Set-up for asthma care is notSet-up for asthma care is not
satisfactorysatisfactoryAsthma EducationAsthma EducationOutpatient careOutpatient careEmergency careEmergency care
-
8/14/2019 Asthma Medicine 5
52/52