
ASSESSMENT’ - EO2 Conceptseo2.com/resources/Assessment_Documentation.pdf · Oxygen Concepts, Inc....
55
Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300 ASSESSMENT AND DOCUMENTATION Shelly Monnens APRNBC, FNP, MSN, RN, CWOCN, CWS Director of Clinical Services 1
Transcript of ASSESSMENT’ - EO2 Conceptseo2.com/resources/Assessment_Documentation.pdf · Oxygen Concepts, Inc....

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
ASSESSMENT AND
DOCUMENTATION
Shelly Monnens APRN-‐BC, FNP, MSN, RN, CWOCN, CWSDirector of Clinical Services
1

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Disclaimer
The informaAon presented herein is provided for educaAonal and informaAonal purposes only. It is for the aGendees’ general knowledge and is not a subsAtute for legal or medical advice. Although every effort has been made to provide accurate informaAon herein, laws change frequently and vary from state to state. The material provided herein is not comprehensive for all legal and medical developments and may contain errors or omissions. If you need advice regarding a specific medical or legal situaAon, please consult a medical or legal professional. EO2 Concepts shall not be liable for any errors or omissions in this informaAon.
2

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Understand essenAal components of wound documentaAonExplain importance of proper and consistent wound documentaAonDifferenAate wound types and appropriate staging and documentaAonDifferenAate between inflammaAon and infecAonDescribe the different classificaAon tools
3

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Importance of DocumentaAon
Predict appropriate intervenAonsEvaluate clinical efficacyLegal protecAonGuide treatment decisionsEvaluate healing processSupport reimbursement claimsIs required for reimbursement
4

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Regulatory Issues
MedicareMDSNPUAPBackstaging
5

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Protocol for Assessment
DifferenAate wound type: pressure vs. non-‐pressure, related classificaAon/eAology, full thickness or parAal thicknessAnatomical locaAonSize (length x width x depth) in cmAppearance
Base, edge, periwoundDrainageAssess and monitor infecAon, pain, tenderness & itching Monitor the progress toward healing and potenAal complicaAonsMonitor dressing and treatment modaliAes
6
Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Daily Monitoring
EvaluaAon of ulcer if no dressing is presentEvaluaAon of the status of the dressing, if present
– Is it intact? Is there drainage? Is it leaking?
Status of the peri-‐ulcer areaArea around the ulcer that can be observed without removing the dressing
Presence of possible complicaAonsIncreased redness, swelling, drainage, etc.
Whether pain, if present, is being adequately controlled
7

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
DocumentaAon/Assessment
Weekly measurements should be performed and recorded, or any Ame there is a significant change in the wound statusMeasure linear distances from wound edge to wound edge or intact epithelial margin to intact epithelial marginMeasure all wounds using the ‘clock’ method
Wound → think of a clockTop (toward paAent’s head) = 12 o’clockBoGom (toward paAent’s feet) = 6 o’clockLength measured 12 → 6 o’clock
8

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
DocumentaAon/Assessment
Depth measured as the distance from visible surface to deepest point in wound baseMeasurements should be documented in cenAmetersInclude undermining and tunneling measurements when presentExudate if present: type, color, amount, odorPain if present: nature and frequencyWound bed: color and type of Assue
Evidence of healing or necrosis?DescripAon of wound edges and periwound
Rolled edges, eythema, induraAon, maceraAon
9

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Sinus Tract
10
A cavity or channel underlying a wound that involves an area larger than the visible Picture shows surface of the wound: the arrow represents the direcAon of the tractIt ojen results in a dead space (sac) with non-‐defined walls filled with necroAc debrisPotenAal for abscess formaAonSurgical intervenAon is required for closure

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Tunneling
11
Passageway of Assue destrucAon under the skin surface that has an opening at the skin level from the edge of the woundInvolves a small opening and extends for a distance in one direcAonThe tunnel may communicate with a nearby woundTo help prevent infecAon, tracking or extension away from the wound edge should be probed to ensure there is adequate drainage
Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
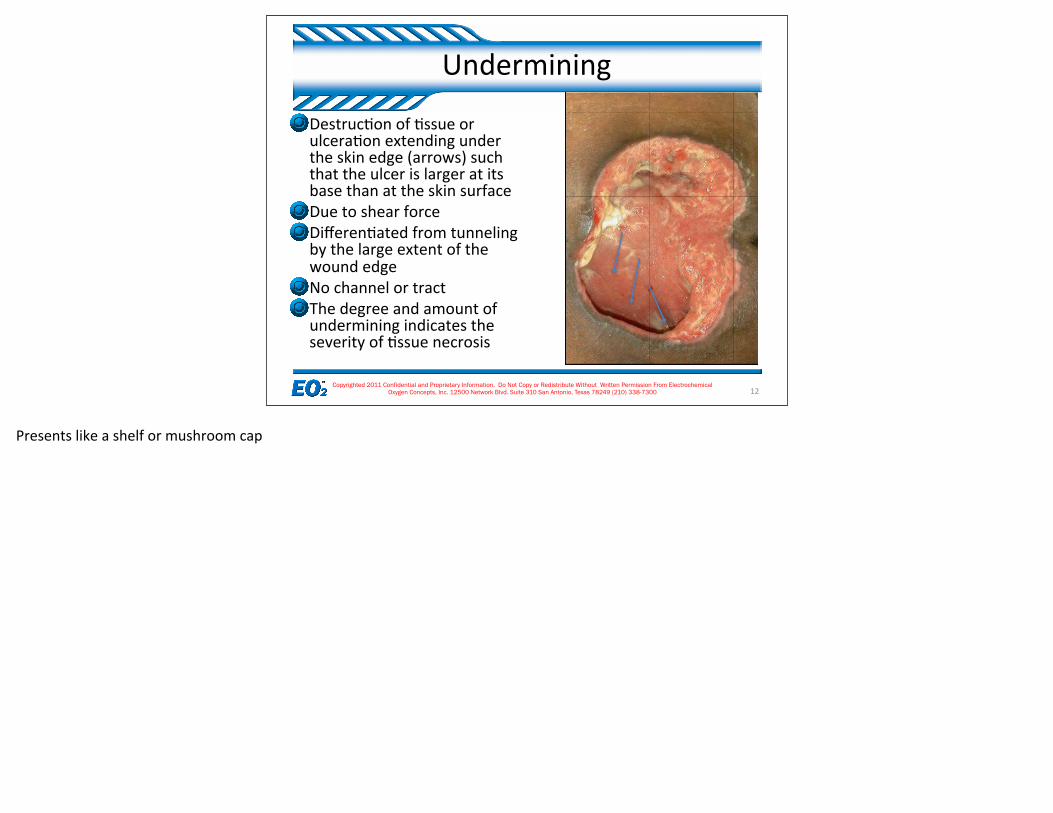
Undermining
12
DestrucAon of Assue or ulceraAon extending under the skin edge (arrows) such that the ulcer is larger at its base than at the skin surfaceDue to shear forceDifferenAated from tunneling by the large extent of the wound edgeNo channel or tract The degree and amount of undermining indicates the severity of Assue necrosis
Presents like a shelf or mushroom cap

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
DocumentaAon: ClassificaAon by Color
Used as a component of assessment, as a tool to direct treatmentDescribe percentages of each Assue type present:
Red indicates clean, healthy granulaAon AssueYellow indicates presence of exudate/slough and need for wound cleansingBlack indicates presence of eschar
13
Note: This was developed by industry to simplify Assue types. Not readily accepted in the literature.
Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
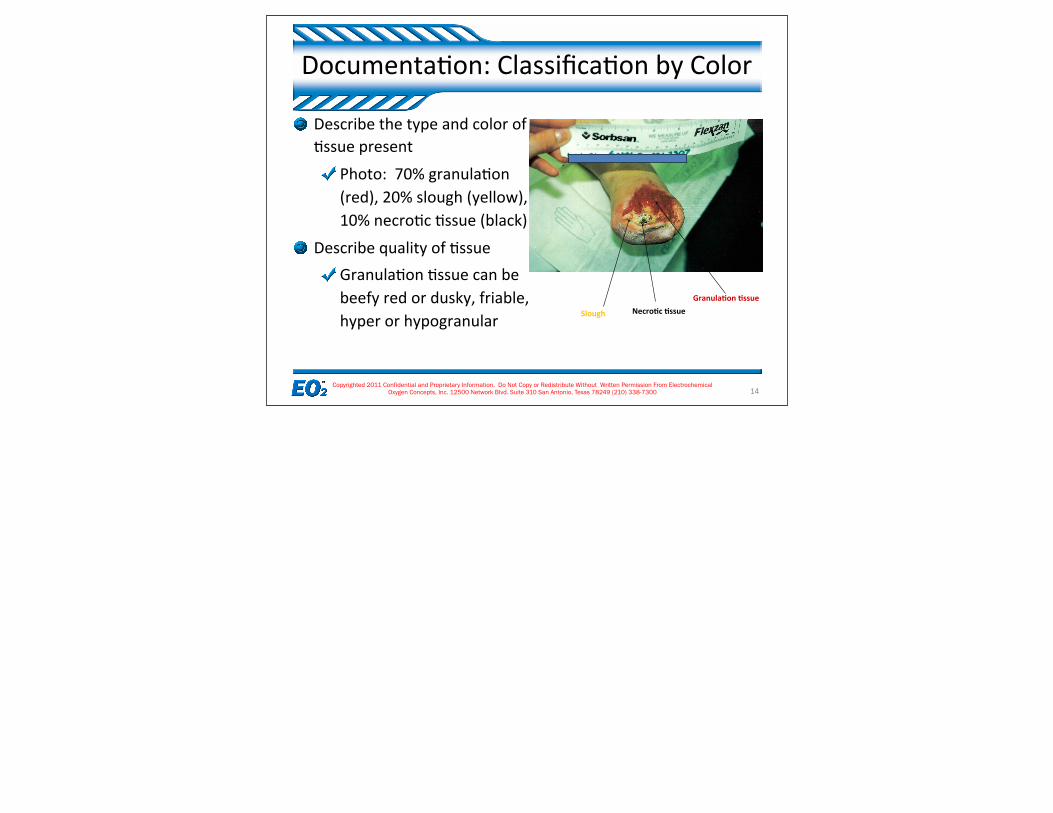
DocumentaAon: ClassificaAon by Color
14
Describe the type and color of Assue present
Photo: 70% granulaAon (red), 20% slough (yellow), 10% necroAc Assue (black)
Describe quality of AssueGranulaAon Assue can be beefy red or dusky, friable, hyper or hypogranular
Granula<on <ssueNecro<c <ssueSlough

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
DocumentaAon: Drainage
Amount: ranges from Scant, Light/Minimal, Moderate, or Heavy/CopiousColor and Consistency:
Serous-‐ clear, watery plasmaSanguineous-‐ bloody (fresh bleeding)Serosanguineous-‐ plasma and red blood cellsPurulent-‐ thick drainage, WBCs and living or dead organisms, may be yellow, green or brown (typical with infected wounds)
Odor: pungent, strong, foul, fecal, or mustyOdor does NOT necessarily mean infecAon, especially when necroAc Assue is present!Assess odor ajer wound cleansing
15
Must rely on clinical judgment and experience in determining amount of exudate; levels have not been quanAfied in the literature

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
DocumentaAon: Wound Margin
Wound margins-‐ the area immediately adjacent to the wound bed where epithelizaAon typically occurs.
Describe integrity and appearanceEpithelialized-‐complete, epithelializing, rolled epithelium or epiboly, callus or hyperkeratoAc Assue (thickening of stratum corneum), other…
16

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Wound Margin Examples
17
Epiboly-‐ edges rolledover (invaginated)
Rough and raggededges due to fric<onand shear
Thickened, hyperkerato<c<ssue; callus-‐like rim
Complete re-‐epitheliza<on wound has resurfaced and is considered closed*
*A wound is sAll “healing” even ajer it closes/resurfaces. Scar maturaAon (full thickness wounds) can take up to two years. Once the scar Assue is mature, then the wound is considered “healed”.Immature scar Assue is red, raised and rigid.Mature scar Assue is pale, planar and pliable.
Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
DocumentaAon: Periwound
Observe for color and temperature Note if skin is intact, open, moist or weepyA red ring, streaking or significant alteraAons in color may indicate infecAonEvaluate epithelial edge for conAnuity
EpithelializaAon may be delayed if:Eschar or necroAc Assue is presentWound is draining excessivelyEdges are rolled or traumaAzed
18

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Periwound Examples
19
Evidence of re-‐epitheliza<on,thin silvery epithelial <ssue
Evidence of deep<ssue injury, purplebruised appearance
Atrophic and fibro<c <ssue changes
Note: in darker pigmented individuals, the area of re-‐epithelializaAon ojen appears pink and/or hypopigmented. Over Ame, the residents more natural skin color/pigmentaAon will return.

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Wound Care RaAonale
Manage original eAologyRemove pressure from wound and involved area via complete offloading and pressure redistribuAonControl inconAnence, excessive moisture
Use barriers as neededAssess for adequate blood flow
Assess for venous and arterial insufficiencies*– UAlize ankle brachial index– Consider referral to vascular surgeon
Reduce venous hypertension– UAlize compression bandages/garments when appropriate
20
If wound is venous in nature, address underlying VI. If arterial, refer for vascular consult before implemenAng aggressive wound management. If the wound is related to or complicated by diabetes, address and manage underlying disease process.* Determine vascular status by doing an Ankle Brachial Index (ABI). This will determine the status of the paAent’s arterial system and ability to tolerate compression.

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Wound Bed PreparaAon (WBP)
Remove necroAc Assue & reduce bacterial bio-‐burdenDecrease infecAon risk and promote healing Select appropriate form of debridement for resident/pt and wound
Maintain moist wound environment Add moisture to dry woundsControl moisture with wet wounds
*EXCEPTION: in cases of very poor arterial flow with intact dry black eschar: keep dry, protect, prevent infecAon or with stable dry eschar
Assess for other systemic/resident/pt issuesMalnutriAon, disease processes, pharmaceuAcal
21

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
WBP: Debridement
AutolyAcUse of moist environment to allow the body to naturally cleanse wound of necroAc AssueSlowest and most pain-‐free method
EnzymaAcUse of topical ointments to remove necroAc AssueFaster processRequires prescripAon.
Other forms of debridement
22
The type/form of debridement selected will be dependent upon the clinical presentaAon of the wound as well as the resident.

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
WBP: Reduce Bioburden
Bioburden vs. InfecAonALL wounds are contaminated with bacteria (MRSA very prevalent)Some degree of bacterial balance is necessary for healingWounds may not be clinically “infected” (determined by culture, # of bacteria present) but can have a high bacterial load that slows healingIf a high bioburden is suspected based on wound characterisAcs, culturing the wound is NOT necessary
23

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
WBP: Reduce Bio-‐burden
Deep InfecAonRecommend use of systemic anAbioAcsClinical systemic wound infecAon is indicated by:
Elevated WBC countFeverMarked erythemaEdemaPainCelluliAs at periwound/extremity
24
Systemic anAbioAcs will not reach granulaAon Assue due to large molecular size, so topical anAmicrobials are also helpful

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
InflammaAon Vs. InfecAon
Rubor
Calor
TumorDolor
FuncAo laesa
25
How can you tell thedifference? Both present with…
Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Classic Signs/Symptoms of InfecAon
Acute Wound InfecAon
Chronic Wound InfecAon
26
Dolor (pain)Rubor (erythema)Calor (warmth)Edema/swellingPurulenceFever
From: Vazquez J, Keast D. Contemporary Issues in Wound InfecAon: Managing Risks, TreaAng the Problem. Wounds. November 2006 Supplement.

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
InfecAon vs. InflammaAon
InflammaAonWell defined erythemal
InfecAon•Poorly defined border
27

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Secondary Signs/Symptoms of InfecAon
CriAcally colonized
Bacterial burden
Local wound infecAon
28
Delayed healingChange is wound bed colorFriable granulaAon AssueAbsent/abnormal granulaAon AssueAbnormal colorSerous drainagePain at wound site
From: Vazquez J, Keast D. Contemporary Issues in Wound InfecAon: Managing Risks, TreaAng the Problem. Wounds. November 2006 Supplement.
*Friable granulaAon Assue…In a chronic nonhealing wound, the prolonged inflammatory state interferes with normal healing; the new matrix is broken down by inflammatory products as quickly as it is constructed. This can make the granulaAon Assue produced, defecAve.For example: a high bacterial burden triggers the release of excess vascular endothelial growth factor (VEGF) producing excessive but abnormally weak vascular endothelial buds. The subsequent granulaAon Assue can easily be digested by the MMPs and it appears very friable.

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
WBP: Reduce Bio-‐burden
AnAmicrobial Rinses (excellent alternaAve to saline)Commercially prepared with non-‐cytotoxic levels of anAmicrobial chemicals
Anasept: 0.057% Sodium HypochloriteMicro-‐Klenz (Carrington), SepAcare (Sage), Remedy (Medline) – Benzalkonium chloride as acAve ingredient
Topical AnAbioAcsTAO, Bacitracin, Neosporin, etc.Fallen out of favor for standard treatment due to recent development of “super bugs” and resistant organisms
Topical AnAmicrobialsNewest area of wound technology and incorporated into advanced dressings
Silver
29

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
WBP: Moisture Management
Moisture-‐RetenAve Dressings vs. Gauze/Tape Moist wound healing is the current STANDARD. Semi-‐occlusive dressings ensure moisture retenAon whereas gauze dressings can dry out rapidlyBacterial barrier is inherently provided with semi-‐occlusive dressings: studies show that bacteria can penetrate 64 layers of gauze 4x4sNormothermia increases metabolic funcAon and expedites healing
Cooling of wounds with frequent dressing changes slows healing
Chronic wounds are hypothermic and are about 6 degrees below body temperature
Atrauma<c removal preserves granulaAon Assue and decreases pain during dressing changesFewer dressing changes decreases nursing Ame, reduces wound bed trauma, and saves money
30
Moisture retenAve dressings are ojen called “advanced”, “acAve”, or “interacAve” in that the interact with the wound bed and do not just sit passively on the wound like gauze.
Lawrence JC. Dressings and wound infecAon. Am J Surg; 1994;167:(Suppl 1A):21S–24S.
Lawrence JC, Lilly HA, Kidson A. Wound dressings and airborne dispersal of bacteria. Lancet 1992;339:807.

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
H = HypoxiaE = Excessive tension on wound edgesA = Another woundL = Low temperature
31
D = DiabetesI = InfecAonD = DrugsN = NutriAonal problemsT = Tissue necrosis
. D = Diabetes: The long-‐term effects of diabetes impair wound healing by diminishing sensaAon and arterial inflow. In addiAon, even acute loss of diabeAc control can affect wound healing by causing diminished cardiac output, poor peripheral perfusion, and impaired polymorphonuclear leukocyte phagocytosis.I = InfecAon: InfecAon potenAates collagen lysis. Bacterial contaminaAon is a necessary condiAon but is not sufficient for wound infecAon. A suscepAble host and wound environment are also required. Foreign bodies (including sutures) potenAate wound infecAon.D = Drugs: Steroids and anAmetabolites impede proliferaAon of fibroblasts and collagen synthesis.N = NutriAonal problems: Protein-‐calorie malnutriAon and deficiencies of vitamins A, C, and zinc impair normal wound-‐healing mechanisms.T = Tissue necrosis, resulAng from local or systemic ischemia or radiaAon injury, impairs wound healing. Wounds in characterisAcally well-‐perfused areas, such the face and neck, may heal surprisingly well despite unfavorable circumstances. Conversely, even a minor wound involving the foot, which has a borderline blood supply, may mark the onset of a long-‐term, nonhealing ulcer. Hypoxia and excessive tension on the wound edges also interfere with wound healing because of local oxygen deficits. See, for example, the pressure ulcers shown in the image below. = Hypoxia: Inadequate Assue oxygenaAon due to local vasoconstricAon resulAng from sympatheAc overacAvity may occur because of blood volume deficit, unrelieved pain, or hypothermia, especially involving the distal extent of the extremiAes.E = Excessive tension on wound edges: This leads to local Assue ischemia and necrosis.A = Another wound: CompeAAon between several healing areas for the substrates required for wound healing impairs wound healing at all sites.L = Low temperature: The relaAvely low Assue temperature in the distal aspects of the upper and lower extremiAes (a reducAon of 1-‐1.5°C [2-‐3°F] from normal core body temperature) is responsible for slower healing of wounds at these sites.

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Wound EAologies
RadiaAon damageAnAcoagulant-‐induced skin necrosisAcAnomycosisYawsMucomycosisCutaneous anthrax Pyoderma gangrenosumSickle cell
32
Arterial insufficiencyAtheroembolism Venous insufficiency Lymphedema Neuropathy Pressure Neoplasms Necrobiosis lipoidica VasculiAc wounds
venous insufficiency PaAents with varicose veins or nonfuncAonal venous valves ajer deep vein thrombosis develop ambulatory venous hypertension, that is, distal venous pressure remains elevated despite ambulaAon. This constant venous hypertension seems to cause white cell and fibrin buildup, which impairs capillary blood flow or traps growth factors. Macromolecules pass into the dermis and eventually cause the hemosiderin deposiAon and brawny induraAon in the distal leg (gaiter area) characterisAc of chronic venous insufficiency.LymphedemaAlthough not typically a cause of ulceraAon, extremity ulcers may fail to heal because of untreated lymphedema. Nocturnal leg elevaAon and elasAc wraps or support hose are appropriate adjuncts to the treatment of recalcitrant wounds in edematous extremiAes. For advanced and nonresponsive lymphedema, complex decongesAve physiotherapy is a useful treatment opAon.NeuropathySensory neuropathy involving the feet may lead to unrecognized episodes of trauma caused by ill-‐fi�ng shoes. This is compounded by motor neuropathy causing intrinsic muscle weakness and spaying of the foot on weight bearing. The result is a convex foot with a rocker-‐boGom appearance. MulAple fractures go unnoAced, unAl bone and joint deformiAes become marked. This is termed a Charcot foot (ie, neuropathic osteoarthropathy) and is observed most commonly in people with diabetes mellitus, affecAng approximately 2% of persons with diabetes. Pressure (decubitus) ulcers Pressure (decubitus) ulcers occur because of prolonged ischemia-‐producing external pressure, usually to a soj Assue region overlying a bony prominence. Tissue ischemia results when external pressure exceeds capillary closing pressure (ie, 25-‐32 mm Hg in healthy individuals), the minimum pressure that causes collapse of the capillary when applied to a capillary bed. Shearing forces, exposure to constant moisture, and heat buildup also are major contribuAng factors. For example, the stratum corneum, the outer layer of skin, becomes 25 Ames more fragile at a relaAve humidity of 100% than at a relaAve humidity of 25% and becomes 4 Ames more fragile at 95°F (35°C) than at 86°F (30°C).NeoplasmsNeoplasms strongly suggest malignancy in any chronic nonhealing wound, parAcularly if the wound appears to have occurred spontaneously.[11 ]Basal cell carcinoma appears smooth, pearly, and elevated above the skin surface, as illustrated in the image below, whereas squamous cell cancer is ojen somewhat erythematous and scaly and almost always occurs on sun-‐exposed areas. ParAcularly perAnent in wound care is the so-‐called Marjolin ulcer, a squamous cell carcinoma originaAng in a chronic wound, such as a burn scar or sinus tract.[12 ]This implies that even a wound that is decades old is not necessarily benign. PaAents with Kaposi sarcoma typically present with mulAfocal violaceous lower extremity lesions. PaAents with cutaneous lymphoma present with a single nodule or a group of papules from one to several cenAmeters in diameter, and these almost always occurs above the waist.adiaAon damage The adverse effects of prolonged or excessive electromagneAc radiaAon vary with the wavelength. Wavelengths of electromagneAc radiaAon are as follows: Gamma rays -‐ Less than 0.01 nmX-‐rays -‐ 0.01-‐10 nmUltraviolet C -‐ 10-‐280 nmUltraviolet B -‐ 280-‐320 nmUltraviolet A -‐ 320-‐400 nmVisible light -‐ 400-‐760 nmInfrared -‐ 760 nm to 1 mmMicrowave -‐ 1 mm to 30 cmRadio waves -‐ CenAmeters to metersGamma radiaAon and x-‐ray exposure cause a zone of stasis, in which local blood supply is impaired by coagulaAve necrosis due to thromboAc occlusion of smaller arteries. Gamma and x-‐ray radiaAon also spawn ionized oxygen that adversely affects DNA. The long-‐term result is inhibiAon of regeneraAon of skin cells from dividing basal cells. This may cause recalcitrant painful skin ulcers. The surrounding skin is atrophic, with atrophy of hair follicles and a paucity subcutaneous fat.Ultraviolet radiaAon exposure, parAcularly ultraviolet B, causes sunburn iniAally and subsequently conveys a conAnuing risk of skin malignancy (eg, basal cell carcinoma, squamous cell carcinoma, melanoma). Excessive exposure to infrared radiaAon, which induces repeated or persistent skin hyperthermia of 43-‐47°C, may cause erythema ab igne. PaAents with this skin condiAon present with telangiectasia, erythematous patches, and hyperpigmentaAon.Atheroembolism syndromePatchy areas of ischemia involving the feet, especially in the presence of palpable pedal pulses, suggest the possibility of atheroembolism of plaque fragments from ulcerated, although nonocclusive, proximal atheroscleroAc plaques or from thrombi lining the wall of an infrarenal aorAc aneurysm.Pyoderma gangrenosumPyoderma gangrenosum usually starts as a small painful papule or nodule, which is ojen erroneously presumed to be the result of an insect bite. The lesion enlarges, becomes ulcerated, and develops overhanging, violaceous borders, as shown in the image below. The histologic findings ojen are nonspecific. Associated underlying systemic problems, which occur in one half of paAents with pyoderma gangrenosum, are ojen the best clues to the diagnosis. Examples of such systemic diseases include various arthriAdes, inflammatory bowel disease, hepaAAs, myeloproliferaAve disorders, myeloma, primary biliary cirrhosis, systemic lupus erythematosus, and Sjögren syndrome. An important clue is a paradoxical response in which debridement exacerbates the wound, parAcularly near the areas debrided. When myofascial and osseous Assues become involved, the only choice may be surgical debridement to try to save the extremity.[13,14 ]Sickle cellPaAents with sickle cell–associated leg ulcers typically present with painful small ulcers that start as crusAng nodules in the distal one third of the leg, ojen near the malleoli. The surrounding skin demonstrates absence of hair follicles, hyperpigmentaAon, and atrophy of subcutaneous fat. Radiograph findings may reveal periosteal thickening of underlying bone; true osteomyeliAs is rare. Sickle cell ulcers are more common in males than in females and occur predominantly in persons aged 10-‐50 years. PaAents with sickle cell anemia can also develop leg ulcers because of other eAologies; the physical examinaAon should exclude arterial and venous insufficiency.CalciphylaxisCalciphylaxis is an unusual and ojen fatal syndrome of cutaneous necrosis that tends to develop in paAents with chronic renal failure, parAcularly those with diabetes. The average Ame of onset is 3 years ajer the start of dialysis. The female-‐to-‐male raAo is 3:1. The iniAal finding of calciphylaxis may be that of livedo reAcularis, followed by painful erythematous areas of thickening of the skin and subcutaneous Assues. The most common site is the thigh, though the condiAon may also occur in the legs or the upper extremiAes.[15,16 ]PanniculiAs signaling the onset of calciphylaxis may be precipitated by trauma, such as the site of an injecAon. Proximal painful myopathy, muscle weakness, and elevated serum creaAne kinase (CK) levels may occur. Laboratory tesAng may demonstrate a high serum phosphate level and an elevated parathyroid hormone level. Skin biopsy reveals calcificaAon of the arterial media and luminal stricture of small-‐to-‐medium blood vessels in the subcutaneous fat. Muscle biopsy shows patchy necrosis and atrophy.[17 ]Necrobiosis lipoidicaNecrobiosis lipoidica usually involves the anterior Abial areas, though it can also occur in the face, arms, and chest. PaAents present with well-‐circumscribed, shiny, reddish-‐brown, oval, painless nodules or papules that have a thick shiny surface. Over several months or a year, the lesions may gradually expand and develop a waxy yellow color. Trauma may lead to infected ulceraAons, and involvement of adjacent cutaneous nerves may precipitate considerable pain. Necrobiosis lipoidica is more common in women and in persons with diabetes than in others, but it may also occur in persons without diabetes and before the diagnosis of diabetes.[18 ]Long-‐standing necrobiosis lipoidica may harbor a squamous cell carcinoma.VasculiAc woundsVasculiAc wounds tend to occur throughout the lower legs as mulAple, small, painful, erythematous nodules. Scars resulAng from previous vasculiAc lesions may be a useful clue. Any of the disparate systemic manifestaAons of the diseases of cellular immunity associated with atypical skin lesions, including unexplained fevers, jaw claudicaAon, malaise, Raynaud phenomenon, myalgias, neurologic abnormaliAes, and craniofacial pain syndromes, suggest the possibility of vasculiAs. These lesions are rare.The differenAal diagnosis of wounds with these features includes other uncommon problems, such as anAcoagulant-‐induced skin necrosis, atheroembolism syndrome (ie, trash foot), and Buerger disease. LeukocytoclasAc vasculiAdes represent a disparate group of acquired connecAve Assue problems; paAents present with palpable purpuric skin lesions, petechiae, and ecchymoses, usually involving the lower extremiAes. These syndromes include Wegener granulomatosis, Sjögren syndrome, cryoglobulinemia, systemic lupus erythematosus, rheumatoid arthriAs, dermatomyosiAs, and hepaAAs B. The common factor among these syndromes is a hypersensiAvity angiiAs.[19 ]Skin biopsy demonstrates cuffing of the dermal microcirculaAon by granulocytes, which are found in diverse stages of viability, including complete cellular disintegraAon (ie, nuclear dust). The various disorders in this group are differenAated by clinical and serologic criteria. The presence of asymptomaAc palpable purpura without thrombocytopenia suggests a drug adverse effect, such as those caused by iodides, penicillin, aspirin, chlorothiazides, oxytetracycline, isoniazid, or benzoic acid.AnAcoagulant-‐induced skin necrosisAnAcoagulant-‐induced skin necrosis is an unusual complicaAon of anAcoagulant therapy.[20 ]It may occur with heparin or warfarin, though it is more common with warfarin. Warfarin-‐induced skin necrosis manifests as painful hemorrhagic skin lesions, usually in an area having abundant adipose Assue, such as the thighs, abdomen, or breasts. The female-‐to-‐male raAo is 4:1.This complicaAon is ojen aGributable to hereditary coagulaAon abnormaliAes. Warfarin (Coumadin) depletes vitamin K–dependent coagulaAon factors, such as protein C. Therefore, during the first several days of warfarin therapy, a period of transient hypercoagulability may occur, parAcularly in paAents with hereditary coagulaAon abnormaliAes, such as protein C deficiency or protein S deficiency, anAthrombin 3 deficiency, or acAvated protein C resistance.[20 ]AcAnomycosisAc#nomyces israelii is a fas#dious anaerobic bacterium that is rela#vely common and usually nonpathogenic. In rare individuals, par#cularly hosts who are immunocompromised, the bacterium can become pathogenic and cause chronic, draining, painless skin ulcers and sinuses, usually in the head and neck. False-‐nega#ve #ssue cultures are common because the organism is o?en difficult to culture in vitro. However, microscopic examina#on of wound exudates may demonstrate characteris#c sulfur granules. Ac#nomycosis is responsive to penicillin but requires long-‐term therapy.YawsYaws is a treponematosis caused by Treponema pertenue, which is endemic in humid regions near the equator. Approximately 3-‐4 weeks a?er exposure, a pruri#c sore that resembles a raspberry (the mother yaw) develops at the site where the spirochete enters the skin. This lesion eventually opens to form an ulcer. Scratching spreads the organism and results in mul#ple tubercles and ulcera#ons elsewhere, including the hands, feet, and genitals. These ulcers may have a caseous crust. Results of serologic tes#ng for syphilis may be posi#ve.Treatment is with a single large dose of penicillin. Untreated yaws can erode to bone and joints and can become deforming and crippling. The lesions of pinta, caused by Treponema carateum, are similar to those of yaws, but, unlike yaws, no ulcera#on is present. Pinta typically begins as a papule on the dorsum of the foot or leg. The papule enlarges and becomes a pruri#c plaque, which changes from a copper to gray to bluish color over #me. Regional lymphadenopathy may occur. Pinta is also responsive to penicillin.MucormycosisMucormycosis is an acute and some#mes rapidly progressive, even fatal, fungal infec#on that may occur in pa#ents who are immunocompromised, especially following a burn. The primary lesions are plaques, ulcera#ons and abscesses, or painful ecchymo#c nodules, which may ulcerate and then become necro#c and form eschars. The diagnosis is confirmed by demonstra#ng fungal elements of the black discharge in KOH prepara#ons and by culturing on standard laboratory media.Cutaneous anthraxCutaneous anthrax results from skin exposure to Bacillus anthracis, a gram-‐posi#ve bacillus. Cutaneous anthrax evolves from a pruri#c papule to an ulcerated wound in 1 or 2 days and then into a black eschar over the next week or so. Associated regional lymphadenopathy may be present. Findings on special stains and cultures of the wound exudate are diagnos#c.Anthrax is transmissible from specimens; therefore, so laboratory personnel should be warned in the event of clinical suspicion of this disease. Of course, appropriate public health authori#es must be no#fied. See Anthrax for details.

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Leg Ulcers
Cost to heal can be as high as $10,000Of the more than 16 million diabeAcs in the US, more than 30 percent will develop foot ulceraAonThe average cost of healing a single diabeAc ulcer is $20,000
Common cause circulatory issues (venous, arterial, and neuropathicLeg ulcers affect more individuals than pressure ulcers: one in four Americans over the age of 65 will develop a leg ulcer in their lifeAmeRecurrence rate is as high as 70%, conservaAvely
33
Primary prevenAon is the key to leg ulcer management. Appropriate educaAon, monitoring and prophylacAc foot and nail care have been shown to prevent ulceraAon and the resulAng sequelae in the majority of paAents. For paAents who have already developed a leg ulcer, the criAcal issue is accurate assessment of causaAve factors with iniAaAon of appropriate correcAve care. It is also essenAal to provide cost-‐effecAve and research-‐based wound care. Since leg ulcers are associated with a very high recurrent rate, paAent educaAon regarding follow-‐up care is another crucial component of management. • Leg ulcers are most commonly caused by circulatory problems (venous ulcers and arterial ulcers) or by damage to nerves(neuropathic ulcers, common in diabeAc paAents). • Leg ulcers affect more individuals than pressure ulcers. One in four Americans over the age of 65 will develop a leg ulcer in their lifeAme. • The recurrence rate for venous ulcers is as high as 70 percent. The cost to heal a single venous ulcer can be close to$10,000. The medical grade compression stockings used to treat this life-‐long condiAon cost $40-‐100 per pair. They must be replaced every six months and are an out-‐of-‐pocket expense to the paAent. • Arterial ulcers and neuropathic ulcers are parAcularly common among individuals with diabetes. Of the more than 16million diabeAcs in the US, more than 30 percent will develop foot ulceraAons. These ulcers are notoriously difficult to resolve. The average cost of healing a single diabeAc ulcer is $20,000. The average out-‐of-‐pocket expense for custom-‐ molded diabeAc shoes used to prevent further complicaAons is $143 per pair. Many of these individuals require surgical intervenAon, and some will require amputaAon. The cost of amputaAon and subsequent rehabilitaAon averages $62,000 for the first year. AmputaAon can frequently be prevented by appropriate prevenAve care and early intervenAon

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Venous
HistoryMalleolusMedial aspect of leg superior to medial malleolus
LocaAon Advanced AgeCHFLymphedemaObesityOrthopedic ProceduresPain reduced by elevaAonPulmonary EmbolusReduced mobilitySedentary LifestyleTraumaAc Injury Vascular UlcersWork History
34

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Venous
Assessment of WoundBase: ruddy red, yellow adherent or loose slough granulaAon Assue present, undermining or tunneling are uncommonDepth: usually shallowMargins: irregular Exudate: moderate to heavyInfec<on: less common
Assessment of Surrounding SkinVenous dermaAAs (erythemaAc, weeping, scaling, crusAng)Hemosiderosis (brown staining)Lipodermatosclerosis: Atrophy BlancheTemperature: normal, warm to touchEdema: pi�ng or non-‐pi�ng, possible induraAon and celluliAsScarring from previous ulcers, ankle flare, Anea pedisInfecAon: induraAon, celluliAs, inflamed, tender bulla
35

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Venous
Perfusion Pain
Minimal unless infected or dessicatedDescribed as throbbing, sharp, itchy, sore, tender, heavinessWorsens with prolonged dependency
Peripheral Pulses = Present/palpableNon-‐Invasive Vascular TesAng
Capillary Refill: normal (less than 3 seconds)ABI to rule out arterial componentMeasures to Improve Venous ReturnProvided vascular studies have ruled out significant arterial disease)Surgical obliteraAon of damaged veinsElevaAon of legsMedicaAonsExcercise EducaAon
Topical TherapyGoals:
Absorb exudates Maintain moist wound surface
36

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Arterial Insufficiency
HistoryArterial disease Cardiovascular diseaseDiabetesDyslipidemiaHypertensionIncreased pain with acAvity and/or elevaAon IntermiGent claudicaAonObesityPainful ulcerSickle Cell AnemiaSmokingVascular procedures/surgeries
Loca<onAreas exposed to pressure or repeAAve trauma, or rubbing of footwear Lateral malleolus Mid-‐Abial Phalangeal heads Toe Aps or web spaces
37

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Arterial Insufficiency
Assessment of WoundAssessment of WoundBase: Pale; granulaAon rarely present; necrosis, eschar, gangrene (wet or dry) may be presentDepth: may be deepMargins: edges rolled; punched out, smooth and undermining Exudate: minimal InfecAon: frequent (signs may be subtle)
Assement of Surrounding SkinAssessment of Surrounding SkinPallor on elevaAon Dependant rubor Shiny, taut, thin, dry, Hair loss in lower extremiAes Atrophy of subcutaneous Assue Edema: variable; atypicalTemperature: decreased/coldInfecAon: CelluliAs Necrosis, eschar, gangrene may be presentNails-‐Dystrophic
38
Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Arterial InsufficiencyPain
IntermiGent claudicaAonResAng, posiAonal, nocturnalPainful ulcer Paresthesias
Peripheral PulsesAbsent or diminished
Non-‐Invasive Vascular Tes<ngCapillary refill: Delayed (more than 3 seconds)ABI < 0.9 TCPO2 < 40 mm Hg TP > 30 mm Hg
Measures to Improve Tissue PerfusionRevascularizaAon, if possibleMedicaAons to improve RBC transit through narrowed vesselsLifestyle changes (avoid tobacco, caffeine, restricAve garments, cold temperatures) HydraAonMeasures to prevent trauma to Assues (appropriate foot wear)Maintain legs in neutral or dependent posiAon Pressure reducAon for heels and toes
39

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Topical TherapyDry, Non-‐Infected, NectroAc Wound
Keep dry
Infected Wound / Dry or Moist NecrosisReferral for potenAal surgical debridement/anAbioAc therapy
Open Wound / Non-‐NectroAcMoist wound healing Non-‐occlusive dressingsAggressive treatment if any infecAon
40

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Peripheral Neuropathy
HistoryAdvanced ageAlcoholismChemotherapyDiabetes Hansen’s diseaseHeredityHIV, AIDS and related drug therapiesHypertensionImpaired glucose toleranceObesityRaynaud’s disease, SclerodermaSmokingSpinal cord injury and neuromuscular
Loca<onAltered pressure points/sites of painless trauma/repeAAve stress Dorsal and distal toesHeelsInter-‐digital Metatarsal heads Mid-‐foot (dorsal and plantar) Toe interphalangeal joints
Assessment of WoundBase: pink/pale, necroAc Assue variableDepth: variableEdges: well defined Exudate: usually small to moderate Wound shape: usually rounded or oblong and found over bony prominence
41

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Peripheral NeuropathySurrounding Skin
Normal skin tones Trophic changes Fissuring or callus formaAon u Edema: with erythema may indicate high pressureTemperature: warm
NailsOnychomycosis, dystrophic nails, paronychia, hypertrophy
PainDecreased sensi<vity to touch; if present, pain may be superficial, deep, aching, stabbing, dull, sharp, burning or coolAltered sensaAon not described as pain (numbness, warmth, prickling, Angling)
Peripheral Pulses Palpable/present
Non-‐Invasive Vascular Tes<ngCapillary refill: Normal
Measures to Eliminate TraumaReducAon of shear stress and offloading of neuropathic wounds (bedrest, contact casAng, orthopedic shoesUse of assisAve devices to provide support, balance and addiAonal off loading Appropriate footwear Tight glucose/glycemic control Aggressive prevenAon/treatment of infecAon (debridement of callus and necroAc Assue; pharmacologic treatment when appropriate)Revascularizaton if ischemicComplicaAons: CelluliAs, osteomyeliAs, gangrene, Charcot fracture
Topical TherapyUse dressings that maintain a moist surface,
42

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Pressure Ulcers
More than 1 million new cases each year60,000 deaths each year associated with pressure ulcersAccording to the NPUAP prevalence in acute hosp is as high as 17%, LTC faciliAes 28% and home 28%Management of pressure ulcers esAmated to be $6.4 billion annually
43
Pressure Ulcers Pressure ulcers represent a significant health care problem, therefore preven<ng them is vitally important. Pressure ulcer preven<on can best be accomplished by iden<fying individuals who are at risk for the development of pressure ulcers and the ini<a<on of early preven<ve measures. This requires an understanding of risk factors, the u<liza<on of research-‐based risk assessment tools, knowledge of appropriate preven<ve strategies and access to essen<al medical equipment such as therapeu<c support surfaces. Pa<ents who have already developed pressure ulcers require assessment and interven<ons to iden<fy and correct the causa<ve factors and treatment modali<es to assure op<mal wound healing. Regular follow-‐up assessment and modifica<ons of the treatment plan when indicated are also necessary to assure op<mal wound repair and efficient use of resources, including supplies.• There are more than one million new cases of pressure ulcers (also referred to as bedsores) each year. • 60,000 deaths each year are associated with pressure ulcers. • According to the Na<onal Pressure Ulcer Advisory Panel, pressure ulcer prevalence in acute care hospitals is as high as 17percent, long term care facili<es at 28 percent and home care at 29 percent. • The cost involved in management of pressure ulcers is es<mated to be $6.4 billion annually in US health care dollars. One severe pressure ulcer can cost as much as $50,000 to heal or repair.

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Pressure Ulcer – Stage I
Presents as intact skin with non-‐blanchable redness of a localized areaUsually occurs over a bony prominenceDarkly pigmented skin may not have visible blanching: its color may differ from the surrounding area
44
Further descripAon. The area may be painful, firm, soj, and warmer or cooler as compared to adjacent Assue. Stage I ulcers may be difficult to detect in individuals with dark skin tones and may indicate “at risk” persons (a heralding sign of risk).

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Characterized by parAal-‐thickness loss of dermis presenAng as a shallow open ulcer with a red-‐pink wound bed without sloughIt also may present as an intact or open/ruptured serum-‐filled blister
45
Pressure Ulcer – Stage II
Further descrip#on. A Stage II ulcer a may present as a shiny or dry shallow ulcer without slough or bruising.* This stage should not be used to describe skin tears, tape burns, perineal derma##s, macera#on, or excoria#on. * Bruising indicates suspected deep #ssue injury.

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Pressure Ulcer – Stage III
Characterized by full-‐thickness Assue lossSubcutaneous fat may be visible but bone, tendon, or muscle is not exposedSlough may be present but does not obscure the depth of Assue lossMay include undermining and tunneling
46
Further descrip#on. The depth of a Stage III pressure ulcer varies by anatomical loca#on. The bridge of the nose, ear, occiput, and malleolus do not have subcutaneous #ssue; Stage III ulcers in these loca#ons can be shallow. In contrast, areas of significant adiposity can develop extremely deep Stage III pressure ulcers. Bone Tendon is not visible or directly palpable

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Full-‐thickness Assue loss with exposed bone, tendon, or muscleSlough or eschar may be present on some parts of the wound bedThese ulcers ojen include undermining and tunneling
47
Pressure Ulcer – Stage IV
. further descrip#on. The depth of a Stage IV pressure ulcer varies by anatomical loca#on. The bridge of the nose, ear , occiput, and malleolus do not have subcutaneous #ssue; StageIV ulcers in these loca#ons can be shallow. Stage IV ulcers can extend into muscle and/or suppor#ng structures (eg, fascia, tendon, or joint capsule) ;osteomyeli#s is possible. Exposed bone/tendon is visible or directly palpable

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Full-‐thickness Assue loss in which the base of the ulcer is covered by slough (yellow, tan, gray, green or brown) and/or eschar (tan, brown or black) in the wound bed may render a wound unstageable
48
Pressure Ulcer – Unstageable
Further descrip#on. Un#l enough slough and/or eschar is removed to expose the base of the wound, the true depth (and therefore ,the stage) cannot be determined. Stable (dry, adherent, intact without erythema or fluctuance) eschar on the heels serves as “the body’s natural biological) cover” and should not be removed

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Deep Assue injury may be characterized by a purple or maroon localized area of discolored intact skin or a blood-‐filled blister due to damage of underlying soj Assue from pressure and/or shearPresentaAon may be preceded by Assue that is painful, firm, mushy, boggy, and warmer or cooler as compared to adjacent Assue
49
Suspected Deep Tissue Injury
. Further descrip.on. Deep .ssue injury may be difficult to detect in individuals with dark skin tones. Evolu.on may include a thin blister over a dark wound

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Wound Classifica<on
Wagner Classifica<on of Diabe<c Foot Ulcers
Grade 0: No ulcer is a high risk for foot ulceraAonGrade 1: Superficial ulcer involving the full skin thickness but not
underlying AssuesGrade 2: Deep ulcer, penetraAng down to ligaments and muscle, but
no bone involvement or abscess formaAonGrade 3: Deep ulcer with celluliAs or abscess formaAon, ojen with
osteomyeliAsGrade 4: Localized gangreneGrade 5: Extensive gangrene involving the whole foot
50

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Wound Classifica<on System
University of Texas Wound Classifica<on System of Diabe<c Foot Ulcers
GradingGrade 0: Epithelialized wound
Grade 1: Superficial woundGrade 2: Wound penetrates to tendon or capsuleGrade 3: Wound penetrates to bone or joint
StagesStage A: No infecAon or ischemiaStage B: InfecAon present
Stage C: Ischemia presentStage D: InfecAon and ischemia present
51

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Wound Classifica<on
By Depth: common classificaAon for non-‐pressure related wounds
Par<al-‐Thickness: extends through epidermis down into, but not through, the dermisFull-‐Thickness: extends through epidermis and dermis, may involve subcutaneous Assue, muscle or bone
52
For wounds that are not pressure ulcers, you can classify those wounds into parAal and full thickness. It is very important that those wounds are correctly classified because paAents with full thickness wounds ill have access to treatments from Medicare that those with parAal thickness wounds will not have. A stage II pressure ulcer is a parAal thickness Whereas a stage III and IV are both full thickness wounds They can further be classified into Superficial and deep parAal thickness wounds

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
Summary
IdenAfy and manage the proper wound eAologyDocumentaAon should be objecAve, descripAve, legible and thoroughMatch the intervenAons with the clinical presentaAon of the wound as well as the clinical presentaAon of the resident/paAent
53

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
AddiAonal Resources
54
Agency for Healthcare Research and Quality: www.ahrq.govAmerican AssociaAon of Diabetes Educators: www.aade.orgAmerican Medical Directors AssociaAon: www.amda.comAmerican Academy of Wound Management: www.aawm.comAmerican Physical Therapy AssociaAon: www.apta.orgAmerican College of CerAfied Wound Specialists (ACCWS): www.thecws.orgCenters for Medicare and Medicaid Services: www.cms.hhs.gov/medicaid/survey-‐cert/siqhome.aspEvidence Informed PracAce: www.woundpedia.comExtended Care News: www.extendedcarenews.comMedicare InformaAon: www.Medicare.govNaAonal Pressure Ulcer Advisory Panel: www.npuap.orgOstomy and Wound Management (magazine): www.o-‐wm.com/Texas Diabetes Council: www.dshs.state.tx.us/diabetes/The Wound Healing Society: www.woundheal.orgThe Wound InsAtute (CEU’s): www.thewoundinsAtute.com/US Dept. of Health & Human Services, Lower Extremity AmputaAon PrevenAon Program: www.hrsa.gov/leap/Wound Ostomy ConAnence Nurse AssociaAon: www.wocncenter.com/public/member_directory.cfmWounds (magazine): www.woundresearch.com/

Copyrighted 2011 Confidential and Proprietary Information. Do Not Copy or Redistribute Without Written Permission From Electrochemical Oxygen Concepts, Inc. 12500 Network Blvd. Suite 310 San Antonio, Texas 78249 (210) 338-7300
QuesAons?
55







![AnOverviewof TransferLearning - Nanjing Universitylamda.nju.edu.cn/conf/mlss2014/(X(1)S(kcfwaxyqgaqzl2...JMLR 2009] • Transfer$learning$for$ classificaon,$and$ regression$problems.$](https://static.fdocuments.us/doc/165x107/5b05aa8b7f8b9ad1768bb2ef/anoverviewof-transferlearning-nanjing-x1skcfwaxyqgaqzl2jmlr-2009-transferlearningfor.jpg)










