Aspiration/Injection & Crystalline Arthritis Kathryn Dao, MD Arthritis Consultation Center July 26,...
56
Aspiration/Injectio n & Crystalline Arthritis Kathryn Dao, MD Arthritis Consultation Center July 26, 2007
-
Upload
gwendoline-owens -
Category
Documents
-
view
227 -
download
1
Transcript of Aspiration/Injection & Crystalline Arthritis Kathryn Dao, MD Arthritis Consultation Center July 26,...

Aspiration/Injection
& Crystalline Arthritis
Kathryn Dao, MD Arthritis Consultation Center
July 26, 2007

Outline• General Principles
• Technique
• Fluid Analysis
• Crystalline Diseases
General Principles• Almost any articular/peri-articular structure
(e.g.,bursa) can be aspirated/injected
Intern question: Why should you do an aspiration/injection?
• Primary goals of arthrocentesis/injection:
1. Aid in diagnosis
2. Provide therapy
(relieve pressure/inject medicine)

Indications for Arthrocentesis• Undiagnosed acute or chronic monoarthritis with
effusion• Suspected infection or crystalline arthritis• Unexplained exacerbation of pre-existing polyarthritis• Joint effusion after trauma• Osteoarthritis• Focal pain/swelling in RA, seronegative
spondyloarthritis, gout• Early adhesive capsulitis• Bursitis, tendonitis

Why do steroid injections work in OA?
3rd year resident question:

Why steroid injxs work in OA
• OA is not entirely “non-inflammatory”• Steroids work to alter levels of
cytokines/enzymes involved in leukocyte trafficking
• They inhibit phospholipase A2; therefore, decrease arachidonic acid derivatives
• They decrease production of MMPs/chondrocyte stromelysin
• Placebo effect
Creamer P. Ann Rheum Dis 1997;56:634-6.

Name at least 5 non-financial reasons not to
inject.
2nd year resident question:

Relative Contraindications for Steroid Injections
• Overlying cellulitis/psoriasis
• Known bacteremia
• Prosthetic joints
• Thrombocytopenia/coagulopathy (INR>4, Plt <50,000)
• Lack of response to previous injection
• Charcot/neuropathic joint

Cautions About Injections• Possible adverse effects from injections:
– Systemic absorption of the steroid can worsen CHF, HTN, and DM; HPA suppression, facial erythema
– Steroid arthropathy; osteonecrosis (0.1-3%)
– Iatrogenic infection (1 in 5,000-15,000)
– Tendon rupture due to atrophy
– Fat necrosis or calcification
– Nerve atrophy
– Postinjection flare
– Vitiligo/skin atrophy

Cautions About Injections• Obtain informed consent• Wear gloves for your own protection• Disinfect injection site• Use a large-gauge needle to aspirate an inflamed or
infected joint• Use small-gauge needle and hold pressure over injection
site if patient is anticoagulated• Do not inject the same joint more than 3 to 4 times a year• No more than a total of Depo-Medrol 120 mg in 24 h
period

Steroid PreparationsTrade name Generic name Equivalent
doses*Water solubility
Depo-Medrol Methylprednisolone acetate
4 Insoluble
Aristospan Triamcinolone hexacetonide
4 Insoluble
Kenalog, Aristocort
Triamcinolone acetonide
4 Soluble
Celestone Betamethasone acetate
0.6 Insoluble
Hydeltrasol Prednisolone tebutate
5 Soluble
* Compared to hydrocortisone

DosingTarget Needle length Gauge Dose of
Depo-Medrol
Large:-Troch. Bursa
-Knee
-Shoulder/SAB
1.5 inches 18-21 40-80 mg
Medium:-SI joint
-Elbow
-Ankle
-Wrist
1-1.5 inches 19-23 20-40 mg
Small:-fingers
-toes
½ - 1 inch 23-25 5-10 mg

Contents of Arthrocentesis Tray
- Gloves - Ballpoint pen- Iodine (or other
antiseptic)- Alcohol swabs- Gauze/ Band-Aids- Ethyl chloride (optional)- Hemostat- Syringes (3,10, 20cc)
- Needles (1”, 1.5”, 18-25 gauge)
- Tubes: EDTA (lavender-cell count), Heparin (green-crystals), blank (red-microbiology)
- 1% lidocaine- Corticosteroid - Glass slides/cover slip

Aspiration/Injection
Identify landmarks
Position patient
Obtain informed consent
Mark entry site
Clean skin
Apply topical anesthetics
Aspirate/ Inject
Send specimen Clean up

Commonly injected sites
• Shoulder• Subdeltoid bursa• Olecrenon bursa• Trochanteric bursa• Knee• Ankle
(Injected structures not reviewed in this lecture: hip, pes anserine bursa, elbow, wrist, PIPs, MCPs, MTPs, carpal tunnel, sacroiliac joints)

Anterior Shoulder Exam• Sternoclavicular
joint
• Acromioclavicular joint
• Glenohumeral joint
• Biceps tendon

• Insert needle 1 cm below coracoid process
• Medial to humeral head
Shoulder Joint Injection
ANTERIOR APPROACH POSTERIOR
APPROACH

• Localize lateral midpoint of acromion
• Insert 1 cm distal
• Angle needle upward
Subdeltoid Bursa Injection

Olecrenon Bursa
• Do not approach the bursa at the vertex
• Approach from above or below
• Risk for persistent drainage/infection

Trochanteric bursa
•Lay patient with painful side up
•Palpate point of maximal tenderness
•Insert needle 90 degrees until it touches the greater trochanter
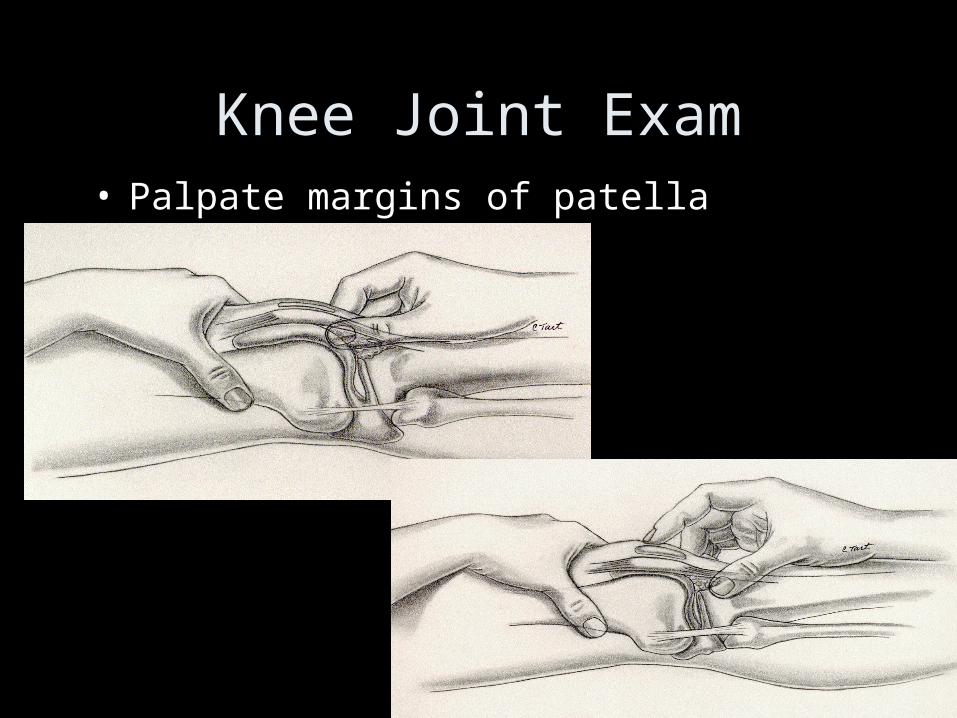
Knee Joint Exam• Palpate margins of patella

Knee Injection
• Knee fully extended
• Junction upper third and lower two thirds of the patella
• Insert needle under patella and aim superiorly
© ACR

Ankle Joint Injection• Plantar flex foot• Insert needle 1 cm
anterior to distal medial malleolus, just medial to dorsalis pedis pulse and extensor tendon of great toe

Synovial Fluid Analysis
Document:
Site
Volume
Viscosity
Color
Clarity

Synovial Fluid Analysis
Synovial fluid should usually be tested for the following EXCEPT:
a) Cell count
b) Protein
c) Gram stain & cultures
d) Crystals
e) Glucose

Synovial Fluid AnalysisAnalysis Non-
inflammatoryInflammatory Septic Hemorrhagic
Appearance Yellow Yellow Purulent Bloody (does NOT clot)
Clarity Clear Cloudy Opaque Opaque
Viscosity High Decreased Decreased Variable
Cell Count 200-2,000 2,000-75,000 >50,000 RBCs>WBCs
%PMNs <25% >50% >80% -----
Example OA, trauma, AVN, SLE
RA, reactive arthritis, crystalline dz, SLE, fungal, TB, viral arthritis
Bacterial arthritis, crystalline dz.
Trauma, fracture, ligamentous tear, coagulopathy, Charcot, PVNS
3 4 5
1 2
Intern question:
How viscous is normal viscosity?
2nd year resident question:
What makes joint fluid viscous? Hyaluronan
>10 cm string
3rd year resident question: What common condition can yield very viscous fluid? hypothyroidism

Wet Prep: Crystal Analysis

Wet Prep: Crystal Analysis
PSEUDOGOUT
GOUT

Types of Crystals
•Monosodium urate•Calcium pyrophosphate dihydrate•Calcium phosphate (hydroxyapatite)•Calcium oxalate•Cholesterol•Corticosteroid•Starch

Crystalline Arthritis: GoutDefinition: An inflammatory disorder due to tissue
deposition of monosodium urate crystals (MSU).
• Uric acid, synthesized by the liver, is a normal end-product of purine degradation
• Hyperuricemia is a result of over-production or under-excretion (90%)
• Excretion of uric acid : 2/3 kidney, 1/3 gut
• Hyperuricemia = 2 SD above the mean
-Men >7.0 mg/dL -Women >6.0 mg/dL
• Solubility of MSU is approx 6.7 mg/dL at 37o C
Gout is the only enemy that I do not wish to have at my feet. — Reverend Sydney Smith, 1841

Gout: uric acidOverproduction:• Idiopathic• Inherited enzyme defects
(HGPRT/PRPP)• Lymphoproliferative/
malignant d/o• Hemolytic d/o• Obesity• Drugs/diet (EtOH,
Cytotoxic drugs, warfarin, purine-rich diets)
Underexcretion:• Idiopathic
• CRF
• HTN
• Dehydration
• Obesity
• HyperPTH
• Hypothyroidism
• Drugs (EtOH, diuretics, low dose salicylates, PYZ, Ethambutol, Levodopa, cyclosporine)

Gout
• The inflammation is secondary to the response of the leukocytes to the MSU crystals.
• Acute gout is most likely secondary to the formation of new crystals (not from release of crystals from pre-formed tophi)
• Common sites of MSU deposition: cartilage, epiphyseal bone, peri-articular structures, kidneys
• Demographics: – hyperuricemia: 5-8% in USA– Gout: men 13/1000; women 6.4/1000– peak incidence 30-40’s in men, 50-70’s in women

Stages of Gout
Asymptomatic hyperuricemia
Acute intermittent gout
Intercritical period
Chronic tophaceous gout

Hyperuricemia
SO Am J Med 1987 Mar;82(3):421-6.
Creatinine (mg/dL)
Uric acid level (mg/dL)
Normal 8-8.5 mg/dL*
1.5 mg/dL 9 mg/dL
1.5-2.0 10 mg/dL
>2.0 or HD 12 mg/dL
*lab ref range

Hyperuricemia• 2/3 pts will remain asymptomatic• Assc. with hypertension, chronic kidney disease, cardiovascular
disease, and components of the insulin resistance syndrome (no causal relationship has been established)
• Incidence of gout increases with uric acid level• 2046 men in the Normative Aging Study followed 14.9 years
urate levels >9 mg/dL, 7.0-8.9 mg/dL, <7.0 mg/dL; annual incidence rate gout 4.9%, 0.5%,0.1%
• strongest predictors of gout were age, body mass index, hypertension, and cholesterol level, and alcohol intake
• Vast majority never developed gouty arthritis, gouty nephropathy, or tophi
SO Am J Med 1987 Mar;82(3):421-6.

Gout Acute gout:
– Abrupt onset of severe joint inflammation, often with onset in the night
– 75% of initial attacks in first MTP joint (podagra)
– Usually monarticular, may be polyarticular
– Attack subsides in 3-10 days
– Urate crystals present in synovial fluid
– Postinflammatory desquamation can occur

Gout Intercritical gout:
– The interval between acute attacks
– Duration variable
– Untreated individuals will experience a 2nd episode within 2 years
– Clinical picture can be confused with RA (if tophi are mistaken for rheumatoid nodules) *** gout and RA rarely co-exist ***

Gout Chronic Tophaceous gout:
– Tophi = aggregrate of MSU crystals in a proteoglycan-rich matrix surrounded by fibrous tissue
– Usually develops after 10 years of acute intermittent gout
– Common sites for tophi development: olecranon, prepatellar bursa, ulnar surface of forearm, helix of the ear, Achilles tendon, fingers

Gout
• Diagnostic Tests:– During an attack, labs may show: elevated ESR/CRP,
uric acid, leukocytosis, thrombocytosis– Joint fluid: WBC >2000 with >75% NO, intracellular
crystal needle-shaped, neg. birefringent 5-25 um– Always send fluid for cultures as septic arthritis may
coexist with gout– Serum Cr and 24 hour urine for uric acid useful to
assess risk for renal stones and for planning therapy• Urinary levels are normal below 750 mg/ 24h; > 1100 mg/dl
increase risk for nephrolithiasis by 50%

Intern question:A 40 y.o obese male patient presents acutely with 1st MTP joint swelling, redness and pain. He cannot put a sheet over his foot. You evaluated him and thought it looked like podagra, but on labs his uric acid level is 3.1 mg/dL.
Does he have gout?
Yes. 40% of patients will have a normal uric acid level during an acute attack.
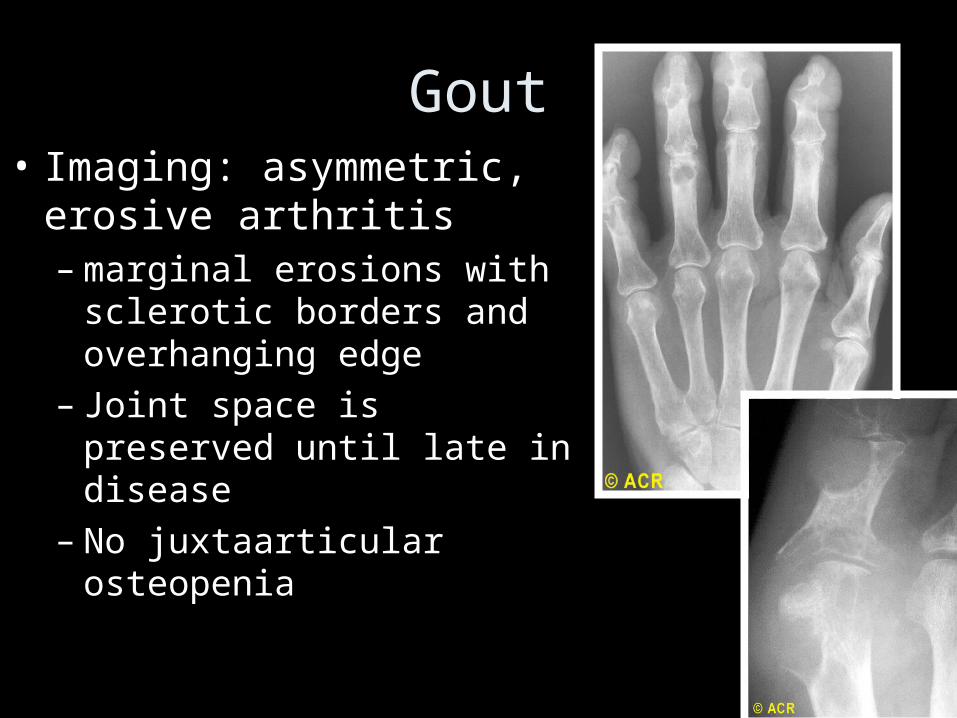
Gout• Imaging: asymmetric,
erosive arthritis – marginal erosions with
sclerotic borders and overhanging edge
– Joint space is preserved until late in disease
– No juxtaarticular osteopenia

Gout or RA??a) b)

DDx
• Acute Gout: septic arthritis, pseudogout, reactive arthritis, acute rheumatic fever and other crystalline arthropathies.
• Chronic tophaceus gout: rheumatoid arthritis, pseudogout, seronegative spondyloarthropathies and erosive osteoarthritis.

Gout Therapy
Goal: treat acute attack and prevent recurrence & complications of untreated gout

Gout TherapyCondition Treat Comments
Asymptomatic Hyperuricemia
???? Weigh risks/ benefits; treat if 24h Urine uric acid >1100 mg/dL, malig. d/o rx to prevent tumor lysis syndrome, possible role to decrease risk in pts with CRI progressing to RF
Acute gout Yes NSAIDS, steroids (po/injx), colchicine
Intercritical period
Yes (in cases of recurrent attacks) Goal for prevention & prophylaxis
Tophaceous gout
Yes Uricosuric agents, uric acid production inhibitors
Am J Kidney Dis. 2006 Jan;47(1):51-9. Ann Rheum Dis. 2006 Oct;65(10):1312-24.

Gout therapyAcute Gout
Intercritical gout
Steroids ok?
NSAIDS ok?
Treat with po colchicine
No
No
Yes
Yes
NSAIDs
Monarticular?
Yes
Rx: Intra-articular injx
No
PO/IM steroids
1st time/ infrequent?
YesObserve, educate
Renal stones/ Tophi?
YesAllopurinol
Uric acid >9 mg/dL Cr > 2 mg/dL?
No
No
No
24h U Uric acid >800 mg?
uricosuric
No
Yes
Yes
Cush J. Rheumatology: Diagnostics/Therapeutics, 2005.
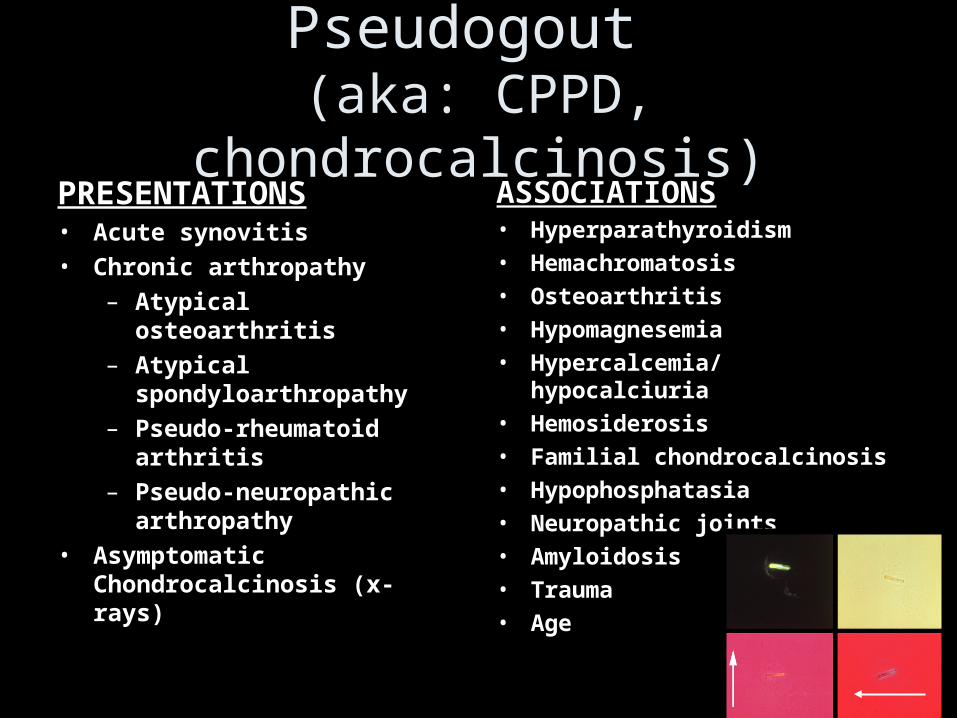
Pseudogout (aka: CPPD, chondrocalcinosis)
PRESENTATIONS• Acute synovitis
• Chronic arthropathy
– Atypical osteoarthritis
– Atypical spondyloarthropathy
– Pseudo-rheumatoid arthritis
– Pseudo-neuropathic arthropathy
• Asymptomatic Chondrocalcinosis (x-rays)
ASSOCIATIONS• Hyperparathyroidism
• Hemachromatosis
• Osteoarthritis
• Hypomagnesemia
• Hypercalcemia/hypocalciuria
• Hemosiderosis
• Familial chondrocalcinosis
• Hypophosphatasia
• Neuropathic joints
• Amyloidosis
• Trauma
• Age

Pseudogout
• Demographics: peak age 65-75 y.o F>M 2-7:1• Prevalence: 5-8% in gen. pop.; 15% by 9th decade• Presentations:
– Acute arthritis: • resembles gout, self-limiting (lasts 1day to 4 weeks); Knee ( 50%
cases)>wrist > shoulder > ankle > elbow
• 20% can have concurrent hyperuricemia
• Can co-exist with gout, RA, infection
– Chronic CPPD deposition disease:• Chronic progressive polyarthritis; mimics RA
– Chondrocalcinosis: • Incidental finding on x-ray

Pseudogout• Diagnostic tests: ESR/CRP/WBC elevation, SF shows
WBC >20,000 >90% NO
• Screen for underlying metabolic abnormalities in pts. age < 55 y.o., florid polyarticular dz., recurrent acute attacks:– Phosphorus -- Magnesium
– Alkaline phosphatase -- Ferritin
– Iron -- Transferrin
– Thyroid-stimulating hormone -- LFTs
• Imaging: Ca++ articular fibrocartilage (menisci, triangular fibrocartilage, symphysis pubis, glenoid and acetabular labra, annulus fibrosus intervertebral discs); degenerative changes (subchrondral cysts, sclerosis, osteophytes, JSN)

Pseudogout• Diagnostic tests: ESR/CRP/WBC elevation, SF shows
WBC >20,000 >90% NO
• Screen for underlying metabolic abnormalities in pts. age < 55 y.o., florid polyarticular dz., recurrent acute attacks:– Phosphorus -- Magnesium
– Alkaline phosphatase -- Ferritin
– Iron -- Transferrin
– Thyroid-stimulating hormone -- LFTs
• Imaging: Ca++ articular fibrocartilage (menisci, triangular fibrocartilage, symphysis pubis, glenoid and acetabular labra, annulus fibrosus intervertebral discs); degenerative changes (subchrondral cysts, sclerosis, osteophytes, JSN)

Pseudogout

Pseudogout Rx
• Steroid injection
• NSAIDs
• Colchicine (in acute Rx and for prophylaxis)
• PO steroids (no controlled trials)
• Identify and treat underlying metabolic disorder

Conclusions
• Most joints can be aspirated and injected
• Always obtain informed consent
• Use good techniques
• Gout and pseudogout are common causes
of inflammatory arthritis,
but can easily
be treated.

Review Video