AO principles course – Vizag 2016 Fracture fixation...
27
Fracture fixation using ‘LOCKED’ plates Ashok S Gavaskar AO principles course – Vizag 2016
Transcript of AO principles course – Vizag 2016 Fracture fixation...

Fracture fixation using ‘LOCKED’ plates
Ashok S Gavaskar
AO principles course – Vizag 2016

Learning outcomesWill discuss
•The need for locked plates based on mechano-biological characteristics•Advantages of locked plates •Technique of using locked compression plates using clinical case examples•Tips, tricks and shortcomings

Resist physiological loads
Ideal plate-screw-bone construct?
Sufficient stability
Minimal soft tissue dissection &
periosteal imprint
Avoid mechanical & biological failures

What happens in conventional plating?
Screw torque
Co-efficient of friction between plate & bone
OsteoporosisCancellous bone
ComminutionPathological host bone
Leaves a big periosteal footprint

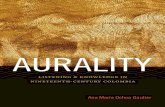
Conventional plate biomechanics
Fracture under compression
LOADSHARING
CONSTRUCT
Applied Load
1
2 3
Bone protects the plate

Fracture comminution
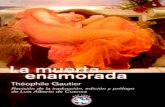
Conventional plate biomechanicsApplied Load
LOADBEARING
CONSTRUCT
When patient loads > co-efficient of friction
of the bone - plate
•Progressive screw loosening• Failure of the plate

Evolution of the locked plate designs
Pc - Fix LISS LCP
Internal fixator DCU + LISS

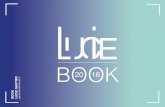
Locked plate biomechanics
SINGLEBEAM
CONSTRUCT
No motion occurs between individual components of the construct
4 times stronger than load sharing constructs
Gautier E, Perren SM, Cordey J. Effect of plate position relative to
bend- ing direction on the rigidity of a plate osteosynthesis. A
theoretical analy- sis. Injury. 2000;31(suppl 3):C14–C20.

Bone after plating with DCP Bone after plating with LCP
Locked plate – Biological advantages

LHS and the LCP – Basic concepts
POSITION SCREW
FIXATION SCREW
Fixes the plate to the bone
Keeps 2 fragments in position
LHS – provide angular and axial stabilityNever as a stand alone or a lag screw

Locked plate – Advantages
Osteoporosis
LHS cannot be over-tightenedNo secondary loss of reductionImproved resistance to bending

Short segment
Locked plate – Advantages
Axial and angular stabilityNo primary loss of reduction

MIPO
No contouringNo primary loss of reductionFavorable as a load bearing construct
Locked plate – Advantages

LCP – when to use?
Any fracture can be treated with a locked compression plate
Absolute stability
Relative stability
Compression Splinting•Articular fractures•Osteoporosis •Simple diaphyseal fractures (upper limb)
•Multi-fragmentary fractures•Open wedge osteotomy•Periprosthetic fractures
•Segmental fractures•C2 and C3 articular fractures

LCP – Preoperative planningType of stability
•Anatomical reduction•Good host bone – conventional screws•Exact PREBENDING•Inter-fragmentary compressioni) DCUii) Lag screw and neutralisation plate
LHS – in poor bone quality
Absolute stability

Closed radial shaft fracture, 22-A2 (
25-year-old man, fall on arm
Principle: absolute stability Method: interfragmentary compression Technique: conventional plating (ORIF)
Case from Michael Wagner, Wien

LCP – Preoperative planningType of stability
Relative stability
•Indirect reduction•Long plate •No pre-bending•LHS - in main fragments•No screw in # zone•Elastic fixation

Closed, 12 – C3 fracture (humeral shaft)48 years female, Fall from height, NV status - intact
Comminuted diaphyseal #Principle: Relative stability Method: BridgingTechnique: MIPO

Periprosthetic distal femur & proximal tibia #s81 years female, osteoporotic
Principle: Relative stability Method: Locked splintingTechnique: Less invasive

LCP – combination techniqueCombine two ‘principles’ in a single construct -only when two different types of fractures in the same bone
Segmental fracture C2, C3 articular fractures

Open grade IIIA 33 – C3 fracture (distal femur)19 years male, MVA
Articular componentPrinciple: Absolute stability Method: CompressionTechnique: ORIF
Metaphyseal componentPrinciple: Relative stability Method: BridgingTechnique: Less invasive

Locked plate – tips & tricks
Lag first & lock next
Cannot help in reduction
In a locked plate achieve reduction first•Distractor•Percutaneous clamps
In a LCP – correction of axial & fracture malalignments is possible

Locked plate – tips & tricks
Simple fractures(transverse & oblique fractures)
Use in compression mode(Use the DCU)LHS – only in osteoporosis

LCP - Technical pearls in bridging
Pre - dynamizeNon-union generators •Longer plate
•Leave 2 empty screw holes over the fracture gap•Screw ratio: 0.4 – 0.5
•Improves working length•Decreases bending stiffness•Improves axial stiffness
Gap strain < 10%
Gautier E, Sommer C. Guidelines for the clinical application of
the LCP. Injury. 2003;34 Suppl 2:B63-76.

Locked plate – tips & tricks
Interface failure
Uncommon•Perfect insertion (upto 5°)•Torque limiter
Respect the FIXED angle

Locked plate – Tips & tricks
Screws Bone quality Fracture location Working length Comments
Unicortical Normal Diaphysis ADEQUATE (Humerus)
Bicortical Normal & osteopenic
Diaphysis & metaphysis
ADEQUATE Avoid self drilling screws
Unicortical Normal Metaphysis INADEQUATE Short segment epi-metaphyseal #s
Unicortical Osteopenic Diaphysis & metaphysis
INADEQUATE contraindication
J Bone Joint Surg Am. 2007;89:2298-307
Unicortical screwsPullout strength = conventional screws & 70% of LHS
•Bone quality•Rotational forces

To conclude..
Using a LCP will depend on - bone quality - fracture personality - anatomical region - surgeon’s preference
•Compression•Bridging•Combined
Absolute/relative stability
For successful practical application..•Preoperative planning•Biological & mechanical considerations•Never mix principles/methods