
Metabolic Complications of HIV Infection and Antiretroviral Therapy (ART)
Upload
jean-goodwinCategory
view
226download
0
Antiretroviral Therapy for HIV Infection in Adults and Adolescents in Resource-Limited Settings: Towards
Universal Access Recommendations for a public health approach
2006 revision

Principles and Objectives
• Standardized formulary for 1st and 2nd line ART– NNRTI-based for 1st line– PI/r-based for 2nd line
• Simplified patient management and standardized laboratory monitoring
• Considerations for women of child-bearing potential, TB and hepatitis coinfected patients, and IDU’s
• Advocacy for greater access to ART and wider availability of CD4 and viral load testing
• Free drugs at point-of-care• Recommendations based on scientific evidence• Utility for program managers and clinicians

Grading of recommendations and levels of evidence
Strength of recommendationLevel of evidence to make for
recommendation
A. Recommended - should be followed
B. Consider - applicable in most situations
C. Optional
I. At least one randomized controlled trial with clinical, laboratory or programmatic endpoints
II. At least one high quality study or several adequate studies with clinical, laboratory or programmatic endpoints
III. Observational cohort data, one or more case controlled or analytic studies adequately conducted
IV. Expert opinion based on evaluation of other evidence

Recommendations for initiating ART in adults and adolescents based on clinical stage and availability of immunological markers
WHO Clinical Staging
CD4 testing not available
CD4 testing available
1Do not treat
[A-III] Treat if CD4 cell count <200/mm3[A-III]
2Do not treat
[B-III]
3 Treat [A-III]
Consider treatment if CD4 cell count <350/mm3 and initiate ART
before CD4 cell count drops below 200/mm3 [B-III]
4 Treat [A-III]Treat irrespective of CD4 cell
count [A-III]

First Line ARV Drugs in Adults and Adolescents
TDF or ABC
AZT or d4T*
NVP
EFV3TC or FTC
Triple NRTI alternative approach
Preferential 2 NRTI/NNRTI approach
*Programs encouraged to begin to move away from d4T.

Clinical, CD4 Cell Count, and Virological Definitions of Treatment Failure for Patients on a First-Line Antiretroviral
Regimen
Clinical failure Occurrence of new or recurrent WHO stage 4 condition
CD4 cell failure Fall of CD4 count to pre-therapy baseline (or below); or 50% fall from the on-treatment peak value (if known); or Persistent CD4 levels <100 cells/mm3
Virological failure
Plasma viral load >10,000 copies/ml

Clinical staging events to guide decision-making on ART switching
New or recurrent event on ART
Recommendations Additional management options
Asymptomatic(T1)
Do not switch regimen
• Maintain scheduled follow up visits including CD4 monitoring (if available) • Continue to offer adherence support
Stage 2 event(T2 )
Do not switch regimen
• Treat and manage staging event• Assess and offer adherence support • Check if on treatment at least 6 months • Assess continuation or reintroduction of OI prophylaxis • Schedule earlier visit for clinical review and consider CD4 (if available)
Stage 3 event(T3)
Consider switchingregimen
• Treat and manage staging event and monitor response• Assess and offer adherence support• Check if on treatment at least 6 months • Check CD4 cell count (if available)• Assess continuation or reintroduction of OI prophylaxis• Institute more frequent follow up
Stage 4 event(T4)
Switch regimen
• Treat and manage staging event and monitor response• Check if on treatment at least 6 months • Assess continuation or reintroduction of OI prophylaxis• Check CD4 cell count (if available)• Assess and offer adherence support
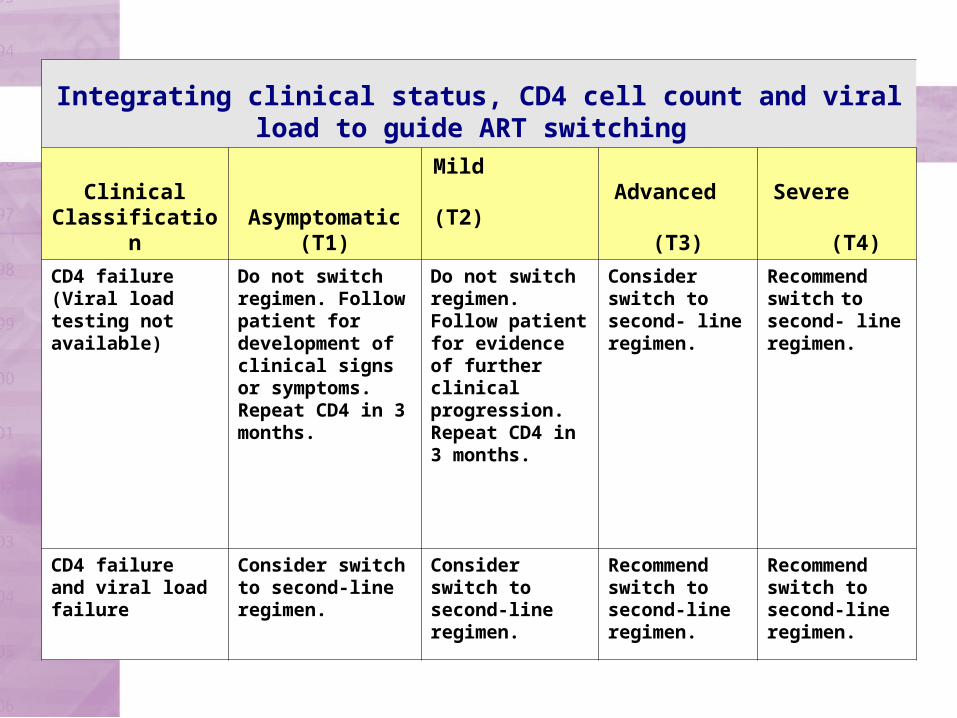
Integrating clinical status, CD4 cell count and viral load to guide ART switching
Clinical Classification
Asymptomatic(T1)
Mild (T2)
Advanced
(T3)Severe (T4)
CD4 failure(Viral load testing not available)
Do not switch regimen. Follow patient for development of clinical signs or symptoms.Repeat CD4 in 3 months.
Do not switch regimen. Follow patient for evidence of further clinical progression.Repeat CD4 in 3 months.
Consider switch to second- line regimen.
Recommend switch to second- line regimen.
CD4 failureand viral load failure
Consider switch to second-line regimen.
Consider switch to second-line regimen.
Recommend switch to second-line regimen.
Recommend switch to second-line regimen.
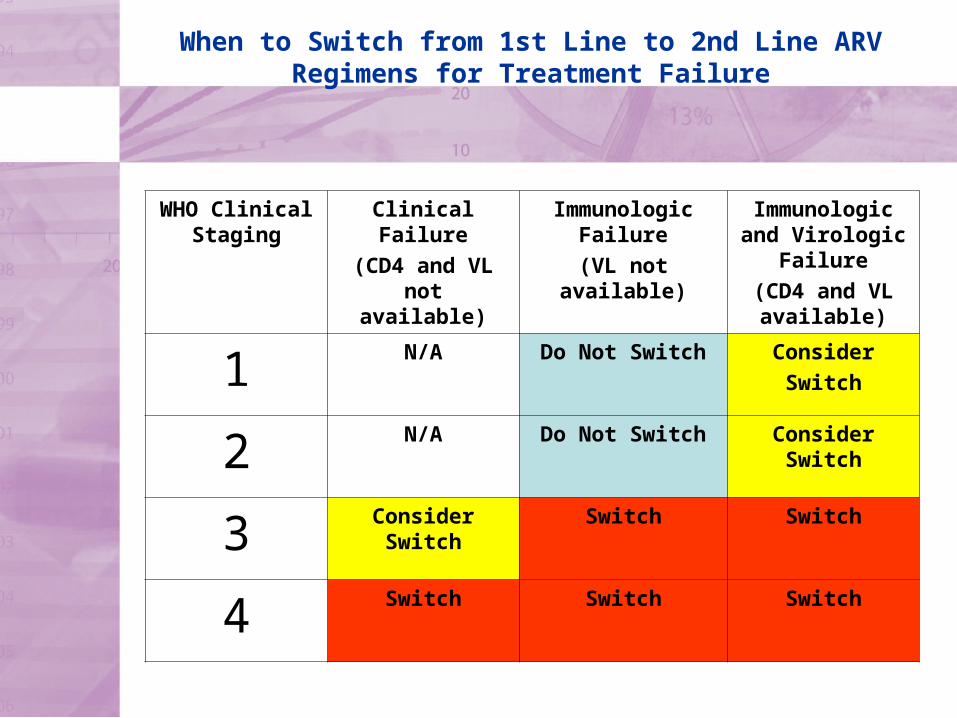
When to Switch from 1st Line to 2nd Line ARV Regimens for Treatment Failure
WHO Clinical Staging
Clinical Failure
(CD4 and VL not available)
Immunologic Failure(VL not
available)
Immunologic and Virologic
Failure(CD4 and VL available)
1 N/A Do Not Switch ConsiderSwitch
2 N/A Do Not Switch Consider Switch
3 Consider Switch
Switch Switch
4 Switch Switch Switch

Second line ARV drugs in adults and adolescents
ABC or 3TC (±AZT)
ddI or TDF
EFV or NVPNRTI sparing option if the triple NRTI approach used in first-line therapy
Standard second-line option if NRTI/NNRTI approach used in first-line therapy
PI/r

Detailed recommendations for switching to second line ARV regimens in adults and adolescents
First Line Regimen
Second Line Regimen
RTI ComponentPI
Component
Standard Strategy
AZT or d4T + 3TC + NVP or EFV
ddI + ABC orTDF + ABC orTDF + 3TC (± AZT)
PI/rTDF + 3TC + NVP or EFV
ddI + ABC orddI + 3TC (± AZT)
ABC + 3TC + NVP or EFV
ddI + 3TC (± AZT) orTDF + 3TC (± AZT)
Alternative Strategy
AZT or d4T + 3TC + TDF or ABC
EFV or NVP ± ddI

Initiating first line ART in relationship to starting anti-TB therapy
CD4 Cell CountART recommendations
Timing of ART in relation the start of TB treatment
CD4 200 cells/mm3 Recommend ART Between 2-8 weeks
CD4 between 200-350 cells/mm3 Recommend ART After 8 weeks
CD4 350 cells/ mm3 Defer ART
Re-evaluate patient at 8 weeks and at the end of
TB treatment
CD4 not available Recommend ART Between 2-8 weeks
Guidelines Development Group
Scott Hammer, Columbia University, USAAyce Riley, MASA National ARV Programme, BotswanaAlexandra Calmy, MSF and St. Vincent’s Hospital, SydneyAnthony Harries, National TB Programme, MalawiChris Duncombe, HIV-NAT, ThailandDiane Havlir, UCSF, USAElly Katabira, Makerere University, UgandaFabio Scano, WHO/HTM/STB, SwitzerlandJean-Elie Malkin, ESTHER, FranceJoep Lange, IATEC, NetherlandsJoia Murkerjee, Partners in Health, USAJudith Currier, UCLA, USALynne Mofenson, NICHD, NIH, USAMark Harrington, Treatment Action Group, USAMauro Schechter, Universidade Federal do Rio De Janeiro, BrazilN. Kumarasamy, YRG Centre for AIDS Research and Education, IndiaPapa Salif Sow, University of Dakar, SenegalPaula Munderi, Uganda Virus Research Institute, UgandaSylvia Ojoo, National AIDS and STI Control Programme, KenyaPedro Cahn, Fundacion Huesped, ArgentinaPraphan Phanuphak, Thai Red Cross AIDS Centre, ThailandSergie Eholie, Treichville Hopital, Cote D’IvoireWafaa El-Sadr, Columbia University, USAWilliam Rodriguez, Clinton Foundation, USA

Acknowledgements
Comments and Contributions:
Annette Verster, WHO/HTM/HIV, SwitzerlandDiane Bennett, WHO/HTM/HIV, SwitzerlandDonald Sutherland, WHO/HTM/HIV, SwitzerlandGerald Friedland, Yale University, USAIgor Olyinik, University of Berlin, GermanyJeroen van Gorkorn, KNCV TBC, NetherlandsMonica Alonso, WHO/AMRO, USASilvia Bertagnolio, WHO/HTM/HIV, SwitzerlandSiobhan Crowley, WHO/HTM/HIV, SwitzerlandPaula Fujiwara, IUATLD, FranceRamzi Asfour, WHO/HTM/HIV, SwitzerlandYing Ru-Lo, WHO/SEARO, India
Acknowledgements
Coordinated by (and special thanks to):
Charles Gilks, WHO/HTM/HIV, Switzerland
Marco Vitoria, WHO/HTM/HIV, Switzerland

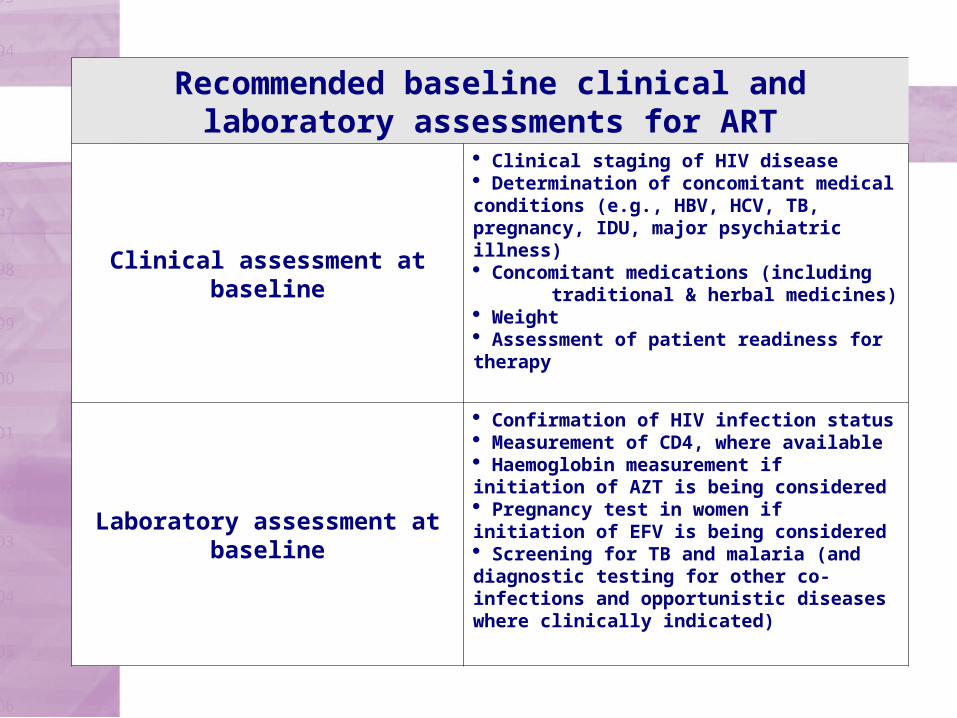
Recommended baseline clinical and laboratory assessments for ART
Clinical assessment at baseline
Clinical staging of HIV disease Determination of concomitant medical conditions (e.g., HBV, HCV, TB, pregnancy, IDU, major psychiatric illness) Concomitant medications (including traditional & herbal medicines) Weight Assessment of patient readiness for therapy
Laboratory assessment at baseline
Confirmation of HIV infection status Measurement of CD4, where available Haemoglobin measurement if initiation of AZT is being considered Pregnancy test in women if initiation of EFV is being considered Screening for TB and malaria (and diagnostic testing for other co-infections and opportunistic diseases where clinically indicated)
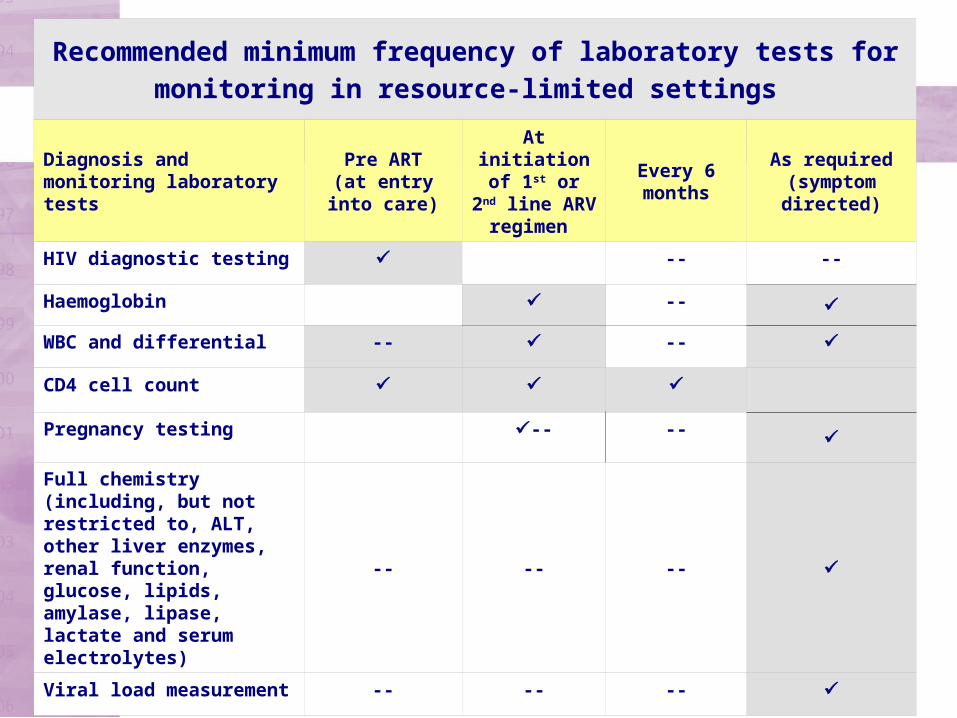
Recommended minimum frequency of laboratory tests for monitoring in resource-limited settings
Diagnosis and monitoring laboratory tests
Pre ART(at entry into care)
At initiation of
1st or 2nd line ARV regimen
Every 6 months
As required(symptom directed)
HIV diagnostic testing -- --
Haemoglobin --
WBC and differential -- --
CD4 cell count
Pregnancy testing -- --
Full chemistry (including, but not restricted to, ALT, other liver enzymes, renal function, glucose, lipids, amylase, lipase, lactate and serum electrolytes)
-- -- --
Viral load measurement
-- -- --
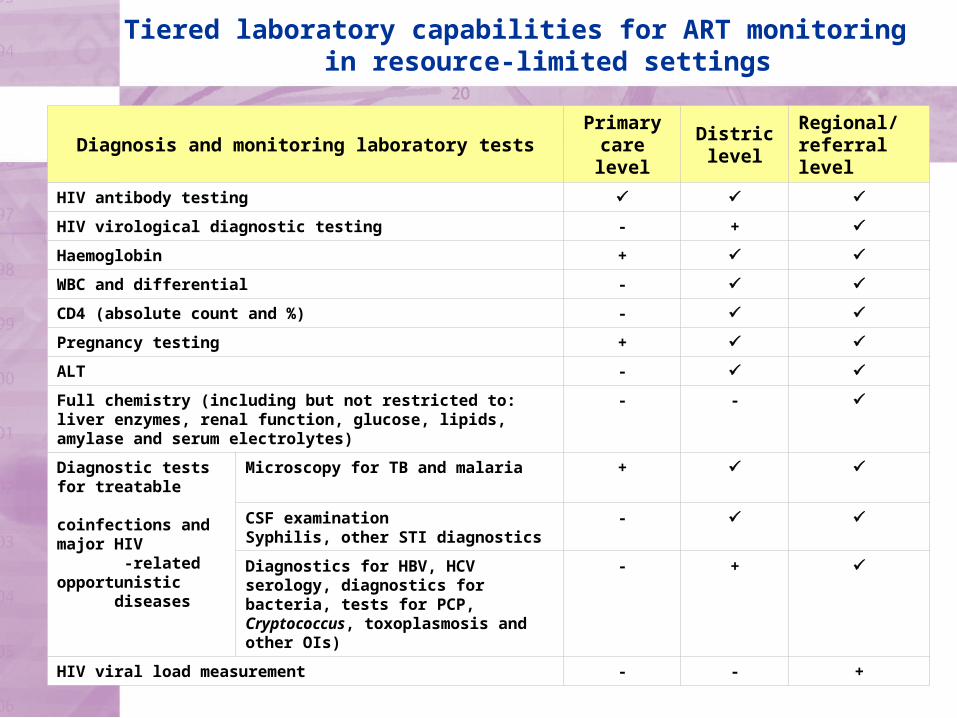
Diagnosis and monitoring laboratory testsPrimary
care level
Distric level
Regional/ referral level
HIV antibody testing
HIV virological diagnostic testing - +
Haemoglobin +
WBC and differential -
CD4 (absolute count and %) -
Pregnancy testing +
ALT -
Full chemistry (including but not restricted to: liver enzymes, renal function, glucose, lipids, amylase and serum electrolytes)
- -
Diagnostic tests for treatable coinfections and major HIV -related opportunistic diseases
Microscopy for TB and malaria +
CSF examinationSyphilis, other STI diagnostics
-
Diagnostics for HBV, HCV serology, diagnostics for bacteria, tests for PCP, Cryptococcus, toxoplasmosis and other OIs)
- +
HIV viral load measurement - - +
Tiered laboratory capabilities for ART monitoring in resource-limited settings


















