Antimicrobial Prophylaxis for Prevention of Meningitis in Traumatic ...
20
To Trick or Treat: Antimicrobial Prophylaxis for Prevention of Meningitis in Traumatic Skull Fractures Associated with CSF Leak Hannah J. Davis, Pharm.D. PGY1 Pharmacy Resident University Health System, San Antonio, Texas Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy Pharmacotherapy Education and Research Center University of Texas Health Sciences Center at San Antonio October 31, 2014 Learning Objectives: 1. Recall anatomy and physiology of skull bones and intracranial components 2. Describe pathophysiology of skull fractures with associated cerebrospinal fluid (CSF) leak 3. Evaluate role of antibiotic prophylaxis in the setting of CSF leak 4. Indicate appropriate use of antibiotic prophylaxis with CSF leak
-
Upload
phungtuyen -
Category
Documents
-
view
217 -
download
0
Transcript of Antimicrobial Prophylaxis for Prevention of Meningitis in Traumatic ...

To Trick or Treat: Antimicrobial Prophylaxis for Prevention of Meningitis in
Traumatic Skull Fractures Associated with CSF Leak
Hannah J. Davis, Pharm.D.
PGY1 Pharmacy Resident
University Health System, San Antonio, Texas
Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy
Pharmacotherapy Education and Research Center
University of Texas Health Sciences Center at San Antonio
October 31, 2014
Learning Objectives:
1. Recall anatomy and physiology of skull bones and intracranial components
2. Describe pathophysiology of skull fractures with associated cerebrospinal fluid (CSF) leak
3. Evaluate role of antibiotic prophylaxis in the setting of CSF leak
4. Indicate appropriate use of antibiotic prophylaxis with CSF leak

Davis 2
Background
I) Why do we care?
A) CNS infections including meningitis can be associated with cerebrospinal fluid (CSF) leaks
B) Overall incidence is low
C) Associated with morbidity, mortality, and increased cost
D) Controversial role for antibiotic prophylaxis
Figure 1. Severity of Injuries
II) Traumatic skull fractures
A) Incidence
i) 1.7 million traumatic brain injuries (TBI) annually1
(a) 275,000 hospitalizations for nonfatal TBI2
(b) 52,000 TBI-related deaths
(c) 80,000-90,000 experience long-term disability
(d) Mechanism of injury1
(1) Fall – 28%
(2) Motor vehicle accident – 20%
(3) Blunt force – 19%
(4) Assault – 11%
(5) Blast injuries
(e) Severity of TBI based on Glasgow Coma Scale (GCS)
(1) Presence of skull fractures is a prognostic factor for worse outcome3
(i) Greater force of impact with trauma
ii) 30% of patients with TBI have associated skull fractures
(a) Incidence of fracture by type
(1) Basal skull fractures (BSF) 3.5-25%4,5
(i) Incidence lower in pediatric patients
1. Increased flexibility of skull base
2. Underdevelopment of ethmoid, frontal, and mastoid air cells
(2) Maxillofacial fractures 23%5
(3) Cranial vault fractures 1%5
Traumatic brain injury
(TBI) Skull fractures CSF fistula
Central nervous
system (CNS) infections

Davis 3
B) Morbidity
i) Severe TBI with skull fractures is associated with a moderate or poor outcome6,7
(a) Intensive care unit admission, ventilator support during recovery, increased risk for
prolonged hospital length of stay8
ii) Permanent neurologic disorders6
(a) Epilepsy, blindness, deafness, diplopia, facial paralysis, other cranial nerve deficits9,10
iii) Traumatic encephalocele
(a) Herniation of brain tissue
iv) Pneumocephalus4,11
(a) Entrapment of air under pressure in intracranial cavity
v) Cerebrospinal fluid leaks
(a) Escape of fluid that surrounds the brain and spinal cord
vi) Infectious complications12
(a) Meningitis, encephalitis, intracranial abscesses, subdural empyema
(b) Head trauma is the most common cause of recurrent bacterial meningitis
C) Mortality
i) Early mortality has substantially declined over time7
ii) 7% mortality in mild TBI with BSF13
iii) 22% mortality in patients with penetrating injury and CSF leak14
iv) 65% mortality in severe TBI with skull fractures3
(a) 30-54% mortality in severe TBI
D) Cost5
i) Average cost of hospital stay in TBI cohorts from 2005-2009
(a) Without meningitis: $32,319
(b) With meningitis: $42,808
ii) Independent risk factors for escalating cost of hospitalization
(a) Rhinorrhea OR 2.0 (CI 1.6-2.7) and otorrhea OR 2.3 (1.9-2.7)
(b) Posttraumatic meningitis OR 3.1 (CI 2.5-3.8)
(c) Surgical intervention
E) Fracture classifications1
i) Characteristics
(a) Linear
(b) Depressed
(c) Compound
(d) Open
(e) Closed
(f) Penetrating

Davis 4
ii) BSF
(a) Characteristics
(1) Thin and more vulnerable to trauma
(2) Air-filled sinuses and multiple foramen render skull base more vulnerable to trauma
(b) Anterior BSF
(1) Type I, cribriform
(2) Type II, frontoethmoidal
(3) Type III, lateral frontal
(4) Type IV, complex
(c) Middle BSF
(1) Longitudinal - parallel to petrous portion of temporal bone
(2) Transverse - perpendicular to petrous portion of temporal bone
(3) Sella turcica fractures
(d) Posterior BSF
(1) Clivus
(i) Transverse, oblique, longitudinal
(2) Occipital
(i) Ring fracture- encircles foramen magnum at skull base
(ii) Occipital condyle- type I – IV
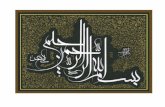
iii) Facial fractures15
(a) Le Fort I
(1) Horizontal maxillary fracture, separating the teeth from upper face, fracture line
passes through alveolar ridge, lateral nose and inferior wall of maxillary sinus
(b) Le Fort II
(1) Pyramidal fracture, passes through posterior alveolar ridge, lateral walls of maxillary
sinuses, inferior orbital rim and nasal bones
(c) Le Fort III
(1) Craniofacial disjunction, fracture line passes through nasofrontal suture, maxillo-
frontal suture, orbital wall and zygomatic arch
Figure 2. Le Fort Fracture Classifications
www.hakeem-sy.com/main/node/26408
Le Fort I Le Fort II Le Fort III

Davis 5
III) CSF
A) Function16
i) Provide physical support and buoyancy for brain/spinal elements
ii) Remove by-products of metabolism from neural tissues and regulates chemical
environment of brain
B) Production and circulation16,17
i) Produced by choroid plexus in the lateral, third, and fourth ventricles at a rate of 20-30
mL/h
(a) Approximately 90-150 mL total volume
ii) Flows from: lateral ventricles to third ventricle to fourth ventricle through subarachnoid
space and circulates through meninges before being reabsorbed via arachnoid granulations
IV) CSF leaks
A) CSF fistula5
i) A fracture involving skull or facial structures may produce a breach in dura
ii) Abnormal passageway allowing escape of CSF from subarachnoid space
iii) Can be associated with CSF leak
B) Types of CSF leaks
i) Rhinorrhea18,19
(a) 72% of CSF leaks
(b) CSF leak through nares
(c) Origins of leak19,20
(1) Fistula of anterior cranial fossa
(2) Fistula of temporal bone
(3) Fistula of middle cranial fossa through sphenoid sinus
(d) Presentation19,20
(1) Fluid initially may appear sanguineous
(2) Unilateral or bilateral clear fluid
(3) Discharge amount varies from drops to stream-like flow
(4) Reserviour sign
(i) Rush of fluid when patient brought from supine to upright with neck flexed
(ii) Useful for collection of diagnostic samples
(5) Anosmia19
(i) Inability to perceive odor
(ii) Present in 80% of cases or rhinorrhea and only 5% in TBIs
(6) Target sign or halo effect19,21
(i) CSF will migrate further when CSF/blood applied to filter paper
1. Apparent on pillowcase or sheets
(ii) Bull’s eye stain appearance
(7) Battles sign
(i) Periorbital ecchymosis

Davis 6
ii) Otorrhea
(a) 28% of CSF leaks18
(b) CSF leak through ear
(1) Typmpanic membrane may be intact or ruptured22
(i) Healing of tympanic membrane occurs within 1 week in ~80%23
(c) Origins of leak
(1) BSF involving temporal bone22
(d) Presentation21,23
(1) Clear fluid draining from ear
(2) Conductive hearing loss
(i) 20% still present 7 years post trauma
(3) Sensation of fluid or bubbles in ear
(4) Hemotympanum
(i) Presence of blood in tympanic cavity of middle ear
(5) Battles sign
(i) Retroauricular ecchymosis
C) Diagnosis of CSF leaks
i) High clinical suspicion of CSF leak in patients with skull fractures24
(a) Prompt recognition is key for instituting treatment and preventative measures9,21
(b) Potential to be overlooked due to nature of concomitant issues
ii) Diagnostic markers can confirm presence of CSF leak25
(a) Produced in CSF and when present in sample indicate presence of CSF
(1) Beta-2 transferrrin
(2) Beta-trace protein
iii) Confirm presence of concomitant fractures with imaging
(a) Computed tomography (CT) scan
(b) Formerly, X-ray
D) Incidence of CSF leak
i) 1-3% of all TBIs5,16,22
ii) 9 - 11% of penetrating head injuries4,20
iii) 10-30% of BSF6,25
iv) 36% of Le Fort fractures20
E) Time to presentation of CSF leak25
i) Acute
(a) Within 2 days following injury – 50%
ii) Delayed
(a) Within 1 week – 70%
(b) Within 3 months – 99%
iii) Sources of delayed presentation19,20
(a) Edema, inflammation, hematoma obstructing flow
(b) May appear in times of increased intracranial pressure (ICP)

Davis 7
F) Duration of CSF leak
i) Temporary
(a) Less than 24 hours
ii) Persistent
(a) Present greater than 7 days
(b) Characteristics of injury which prevent arachnoid mesh from sealing to dura21,26,27
(1) Fracture site mobility
(2) Disrupted blood supply
(3) Infections
iii) Intermittent
(a) Soft tissue or brain can obstruct flow
G) Treatment of CSF leak with skull fractures
i) Reduction and fixation of facial fractures as appropriate20
(a) Stabilize fracture and prevents disruption of dura by reducing movement of facial
skeleton
(b) Facilitate body’s natural repair of anterior fossa CSF leak
ii) Conservative treatment16,20
(a) Facilitate spontaneous resolution of CSF leak
(1) Adhesion formation and granulation from local inflamed meninges
(2) Mucosal swelling, local fibrosis, regenerated nasal mucosa
(3) Dura mater dose not regenerate
(b) Strict CSF precautions20,25
(i) Bed rest
(ii) Avoid: nose blowing, Valsalva maneuvers, straws, incentive spirometer
1. To prevent increase intracranial pressure
(2) Head elevation16,25
(i) At least 15º
(ii) To prevent negative gradient allowing ascending path for bacteria between
intracranial and paranasal sinus cavities
(c) Duration of treatment is controversial
(1) Typically pursued for 1 week
(d) Spontaneous resolution outcomes
(1) Within 3 days in 40% of all cases22
(2) Within 1 week in 70% of rhinorrhea16,22,28
(3) Within 10 days in 85% of rhinorrhea16
(4) Ultimately in 98% of rhinorrhea
(5) Otorrhea ceases spontaneously in nearly all cases
(6) Spontaneous closure higher with temporal bone fractures than BSF

Davis 8
iii) CSF diversion
(a) If conservative treatment fails25
(i) Typically after 1 week29
(b) Treatment options
(1) Temporary CSF drainage device placed
(i) Lumbar drain
(ii) External ventricular drain (EVD)
(iii) Duration less than 7 days due to increased infection risk
iv) Surgical management4,16
(a) Employed for definitive closure of CSF leak
(1) Failure of conservative management and CSF diversion
(b) Approaches
(1) Advances in neurosurgical approaches from open craniotomies to endoscopic
procedures
(2) Surgical approach and graft type used to repair leak depends on individual clinical
scenario
(i) Based on force of impact, location of fistula, temporal relationship between the
leak and traumatic event
(ii) Endoscopic endonasal approach preferred
(iii) Transcranial approach, extracranial approach, suprasinus transfrontal approach
also available
(c) Outcomes25
(1) 75-100% success rate
V) CNS Infections4,20,22,30
A) CSF fistulas allow direct access of nasophyaryngeal and middle ear flora to the subarachnoid
space
B) Pathogens30,31
i) Most common: Streptococcus pneumoniae, Haemophilus influenzae
ii) Less common: gram-negative, more resistant pathogens
C) Can appear within hours or up to years after injury4,19,24
i) Median onset 5-13 day
D) Risk factors for meningitis
i) CSF leaks
(a) Not associated with severity of leak or size of dural tear19,20
(b) Rhinorrhea increases risk 23-fold5
(c) Otorrhea increases risk 9-fold
(d) Persistent leaks increase risk 9-fold16,24,28,32,33
(1) Improper healing or traumatic encephaloceal
ii) Pneumocephalus increase risk up to 4-fold11,16

Davis 9
iii) Fracture types
(a) Penetrating fractures14
(1) Compound fractures with skull depressed deeper than thickness of cranium12
(2) Incidence of infection ~ 10%34
(b) Frontobasilar fractures proximal to midline33
(c) Fracture displacement > 1 cm
iv) GCS < 829
(a) Associated with severity of injury and increased utilization of invasive interventions
v) Surgical interventions are associated with a 5-fold increase risk retrospectively5
(a) Craniotomies12
(1) Incidence 0.8-1.5%
(i) Risk associated with concomitant infection at site of incision and duration of
surgery greater than 4 hours
(b) EVDs
(1) Incidence 4-17%
(i) Increased risk associated with colonization of catheter at time of surgery
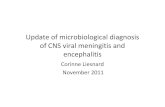
Figure 3. Incidence of Meningitis Associated with CSF Leaks in Literature10,17,22,24, 26,27,30-
43,46,49,50
52.4% (11 / 21)
19% (16 / 84)
3% (1 / 33)
22.2% (12 / 54)
8.7% (13 / 149)
4.7% (2 / 43)
1.9% (1 / 52)
3.4% (2 / 58)
0% (0 / 7)
6.1 % (2 / 33)
8.3% (3 / 36)
1.4% (2 / 138)
4% (2 / 50)
3.6% (1 / 28)
9.8% (21 / 215)
4% (2 / 50)
6.8% (6 / 88)
10.3% (10 / 97)
0% (0 / 12)
0% (0 / 34)
18.5% (15 / 81)
0% (0 / 9)
4.3% (2 / 47)
0% 10% 20% 30% 40% 50% 60% 70%
1942
1954
1966
1966
1973
1975
1976
1976
1978
1983
1986
1988
1991
1992
1993
1995
1995
1996
2004
2004
2004
2009
2010

Davis 10
E) Incidence
i) 0.2- 17.8% of TBI 5,11
ii) When CSF leak is present5,25
(a) Range: 0-52%
(b) Median: 4.24%,
(c) Rhinorrhea: 7-38%
(d) Otorrhea: 2.6%
iii) Penetrating injury with CSF leak: 36%22
(a) 1.7% without CSF leak
iv) 12- 50% of cases are associated with recurrence35
F) Mortality6,20
i) Early studies found morbidity and mortality rates of 50% and 25% respectively for
intracranial infections following CSF rhinorrhea
ii) Recent literature suggests posttraumatic meningitis is associated with ~10% mortality rate
VI) Role of antibiotic prophylaxis24
A) Early publications emphasized importance of antibiotic use as a means of reducing meningitis
i) Advocated for patients who presented with CSF leak or pneumocephalus
ii) Recommended duration of prophylaxis 5-7 days after cessation of CSF leak
iii) Recommendation was based on perceived or theoretical risk of infection and experience of
authors
B) Proposed mechanism of benefit48,49
i) Antibiotics maintain sterility of CSF until defect in dura closes spontaneously or is
surgically corrected
ii) Antibiotics may eradicate bacterial colonization in nasopharynx, nasal sinuses, and aural
canal
Literature Review
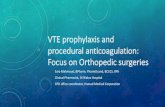
C) 24 studies evaluating incidence of meningitis in patients with CSF leak
i) 19 evaluate the role of antibiotic prophylaxis
ii) Literature dating back to 1942
Figure 4. Role of Antibiotics
16%
31%
53%
Position on Antibiotic Prophylaxis in Literature
Supportive
Neutral stance
Does not support

Davis 11
D) Conflicting meta-analysis published18,49
i) Brodie et al. 1997
(a) Objective: determine efficacy of antibiotic prophylaxis in CSF leaks
(b) Population: 6 studies involving 324 patients
(1) Included all articles with case series and sufficient data to allow evaluation
(2) Findings
(i) 237 patients received prophylactic antibiotics and 87 did not
(ii) Overall incidence of meningitis: 15/234 (6.4%)
1. Antibiotic prophylaxis: 6/237 (2.5%)
2. Inadequate/no antibiotic prophylaxis: 9/87 (10%)
3. Associated with p value=0.006
(3) Conclusion: meningitis rate was significantly lower in patients who received
antibiotic prophylaxis
ii) Villalobos et al. 1998
(a) Objective: determine efficacy of antibiotic prophylaxis in patients with BSF
(1) Evaluated CSF leaks as a secondary endpoint
(b) Population: 12 studies involving 1241 patients
(1) CSF leak: 9 studies involving 547 patients
(c) Findings in patients with CSF leaks
(1) 297 received prophylactic antibiotics and 250 did not
(i) 6 studies with 179 patients with either rhinorrhea or otorrhea were evaluated
(ii) Overall incidence of meningitis 63/547 (11.5%)
1. Antibiotic prophylaxis: 29/297 (9.7%)
2. Inadequate/no antibiotics: 34/250 (13.6%)
3. Common OR 1.34 (CI 0.75-2.41)
(d) Concluded antibiotic prophylaxis after BSF does not appear to decrease risk of
meningitis
VII) Primary Literature
Leech PJ et al. The Lancet. 1973;1:1013-101624
Objective Investigate incidence of meningitis, morbidity and mortality with adequate and inadequate
antibiotic prophylaxis
Trial design Retrospective, single center review at teaching hospital in Glasgow
Patients Inclusion: skull fracture with associated CSF leak from 1943-1972
Exclusion: not specified
Outcomes Incidence of meningitis, morbidity and mortality
Methods
Adequate prophylaxis: penicillin 500 mg PO QID and sulfadimidine 500 mg PO Q6H from time
of injury until 1 week after CSF leak cessation
Inadequate prophylaxis: those not meeting above criteria
Diagnostic criteria: not specified for skull fractures, CSF leak, or meningitis
Follow up: clinic visits, postal query, reviewing cases of meningitis at hospital; for up to ten years

Davis 12
Statistics Not specified
Results
n=155
Referred for neurosurgical care: 141/155
CSF leak associated with fracture: 108/155
Surgical repair of rhinorrhea: 65/118
Le Fort fractures: all received antibiotic prophylaxis, incidence not specified
* p ≤0.05
Increased incidence of meningitis associated with otorrhea if fracture was associated with
middle fossa (p=0.01)
All patients with meningitis recovered satisfactorily
Adequate
Prophylaxis
n=95
No Adequate
Prophylaxis
n=54
Rhinorrhea Number 76 42
Meningitis
leak < 1 week
0 (0%)
7 (17%)*
Otorrhea Number 19 12
Meningitis 1 (5%) 5 (41.7%) *
Mortality Overall 2/155 (3%)
Attributable 0/15 (0%)
Morbidity Anosmia Majority
Recurrent rhinorrhea 4/124
Pathogens Streptococcus pneumonia n=5, coliforms n=1, no growth n= 5
Authors’
conclusions
The inference is clear: all cases of CSF otorrhea should receive adequate antibiotic
prophylaxis from time of injury until 1 week after the leak has ceased.
The benefit of adequate chemotherapy in protecting patients from meningitis in patients with
rhinorrhea has been demonstrated.
Critique
Strengths
Large patient population
Majority of fractures associated with middle or anterior fossa
Morbidity and mortality were examined as endpoints
Limitations
Temporal bias: variations in surgical procedures, CSF precautions, antibiotic selection,
prevalence of resistant organisms
Included pre-existing cases of meningitis
High incidence of meningitis with otorrhea
Unknown exposure to antibiotics in patients receiving inadequate prophylaxis
Incidence of meningitis in rhinorrhea arm no longer associated with adequate or inadequate
prophylaxis following first week
Extensive referral from outside hospitals
Unknown baseline characteristics
Statistical analysis used not specified
Lack of specification of diagnostic techniques for fractures, CSF leak, meningitis
Take home
points
Results favored use of antibiotic prophylaxis
Questionable validity
Broad spectrum of antibiotics and extended duration of treatment

Davis 13
Ignelzi RJ et al. J Neurosurg. 1975;43:721-72650
Objective Primary: determine efficacy of antibiotic prophylaxis in treatment of BSF
Post hoc: determine effect of prophylactic antibiotics on nasopharyngeal flora
Trial design
Combined retrospective and observational prospective at Denver General Hospital
Retrospective arm: patients admitted with BSF, initiated on antibiotic prophylaxis (ampicillin,
cephalothin, or other)
Prospective arm: withheld antibiotic prophylaxis for BSF; antibiotic treatment was indicated if
fever, neck stiffness, clinical deterioration
Patients Retrospective arm: Adult patients with traumatic BSF who survived > 10 days
Prospective arm: Adult patients with BSF admitted for 10 day observation, excluded patients who
received antibiotics for other indications
Outcomes Rates of CNS and other other infections, nasopharyngeal cultures on admission, day 5 and 10
Methods
First year: Antibiotic prophylaxis (ampicillin or cephalothin 1 g Q6H IV x 3 days or until 2 days
after cessation of CSF leak then IM or PO antibiotics for duration of hospitalization
Posterior nasopharynx cultures: Post hoc endpoint, randomized to receive either no antibiotic,
ampicillin or cephalothin; obtained at hospital admission, day 5 and day 10
Follow up: method unspecified
Statistics
ANOVA
Fisher’s exact test
Chi-square
Results
n=129 with 136 BSF
n=40 with CSF leak
Follow up: 3-24 months
Baseline characteristics
Treated group had increased incidence facial fractures and one compound depressed fracture
No antibiotic prophylaxis group had more patients unconscious for > 24 hours, CNS
operations, prior medical illness
Prophylaxis: ampicillin: n=41 cephalothin: n=9 other: n=4
Prophylaxis
(Retrospective)
CSF leak n=17
No Prophylaxis
(Prospective)
CSF leak n=26
CNS infections 2 (12%) 0 (0%)
Pathogens isolated Resistant E. coli n=1,
no growth n=1
N/A
Attributable mortality 1 (50%) N/A
Attributable morbidity 1 (50%) N/A
Mortality, overall 7.2% 7.4%

Davis 14
Nasopharyngeal Cultures Results
Antibiotic Exposure Day 0 Day 5 Day 10
None (n=5) Normal Unchanged Unchanged
Cephalothin (n=3) Normal Gram-negative (n=2)
Increased normal (n=1)
Gram-negative (n=2)
Increased normal (n=1)
Ampicillin (n=2) Normal Gram-negative Gram-negative
Normal- Streptococcus and Staphylococcus sp.
Gram negative- resistant to antibiotic therapy
Outcomes Associated with Antibiotic Administration
Authors’
conclusions
Antibiotics are ineffective in preventing CNS infections and in some cases, harmful.
Antibiotics associated with more resistant, invasive and potentially pathogenic organisms in
nasopharynx.
Recommend close observation for early signs of meningitis and if present, start appropriate
antibiotics.
Critiques
Strengths
Included observational prospective arm
Post hoc investigation of antibiotic impact on nasopharyngeal flora
Limitations
Not specific to those with CSF leak, x-ray confirmation of fracture was present in 14/129
patients
Not adequately powered to determine no difference exists or more harm associated with
antibiotics, limited number of patients with CSF leak in 2 year time frame
Unknown demographic information; epidemiologic, fracture specific, time to onset/duration
of CSF, role of CSF precautions, duration of leak, duration of antibiotics or length of
hospitalization
More selective criteria for the prospective portion
Take home
points
No benefit demonstrated with antibiotic prophylaxis
Nasopharyngeal cultures demonstrated no sterilization of site
Change from usual nasopharyngeal flora to gram-negative/resistant bacteria
Alteration of potential pathogen
Alteration of flora to resistant bacteria
Nasopharyngeal flora not sterilized
Antibiotic administered

Davis 15
Eljamel MS. Br J Neurosurg. 1993;7:501-50535
Objective Evaluate efficacy of antibiotic prophylaxis in patients with CSF leak prior to surgical dural repair
Trial design Retrospective analysis of patients with CSF leaks who received adequate or inadequate antibiotic
prophylaxis prior to surgical dural repair at Mersey Regional
Patients Inclusion: adult patients with CSF fistula
Exclusion: patients who received antibiotics for reasons other than CSF leak, from time of surgical
dural repair forward
Outcomes Meningitis, mortality, and pathogens isolated
Methods
Similar age, CSF leak type, duration of leak, presence/absence of skull fractures
Adequate antibiotic prophylaxis: if started within 3 days of onset of CSF leak; penicillin 500 mg
Q6H and sulponamide 500 mg Q6H and continued for at least one week after CSF leak cessation
Meningitis diagnosis: based on clinical signs and symptoms, confirmed by isolating pathogen or
cytology of CSF
CSF leak: confirmed surgically or post-mortem
Follow-up: until surgical dural repair, death or 1990
Statistics
Chi-square test with Yate’s correction
Two-tailed p values
Log rank
Kaplan-Meier
Results
n= 253
Excluded= 38 patients for receiving antibiotics for other indications (pneumonia, facial
fixation) or were receiving antibiotics other than penicillin and sulponamide
Baseline characteristics
Mean age 35 years old, majority male, with rhinorrhea and skull fractures
More patients in the prophylaxis arm had facial fractures and pneumocephalus
Majority of patients received antibiotic prophylaxis within 24 hours of injury
Mean follow-up 2.5 years
Adequate Prophylaxis
n=106
Inadequate Prophylaxis
n=109
Facial fractures 52 26
Skull fractures 76 75
Rhinorrhea 99 97
Duration CSF leak, mean 17 days 20 days
Pneumocephalus 31 (29%) 12 (11%)*
Meningitis, first week 7 (6%) 10 (9%)
Meningitis, per year 8 (8%) 13 (12%)
Meningitis, total 20 (19%) 36 (33%)
Streptococcus pneumoniae 6 22
Gram-negative 3 0*
No pathogen isolated 11 14
Survival free from meningitis,
1 month
86 (81%) 84 (77%)*
Mortality 20 (19%) 25 (22%)
*p value <0.05

Davis 16
Critiques
Strengths
Large population
Specific to CSF leaks
Fracture type specified
Primary endpoint examining efficacy of antimicrobial prophylaxis
Excluded patients receiving antibiotics for other indications
Limitations
More pneumocephalus and facial fractures in antibiotic prophylaxis arm
Mean duration of CSF leak 17-20 days
Broad antibiotic coverage and extended duration of prophylaxis
Unknown demographic information, mode of injury, incidence of penetrating or other fracture
characteristics, number of patients receiving CSF diversion
Authors’
conclusions
These data do not support routine use of antibiotic prophylaxis in patients with CSF leak
It is ethically justifiable to withhold antibiotic prophylaxis in patients with CSF fistula until a
prospective controlled double-blind trial has settled the question
Take home
points No statistically significant in incidence of meningitis in a well-designed retrospective review
VIII) Limitations in literature
A) Lack of power of individual studies
i) Infrequent incidence of CSF leaks
ii) Even lower incidence of post-traumatic meningitis
B) Confounding factors in studies
i) Retrospective
ii) Lack of randomization
C) Temporal bias
i) Treatment of CSF leak
(a) CSF precautions
(b) CSF diversions and surgical management
ii) Antibiotic availability
iii) Alteration in pathogens
IX) Conclusions
A) Overall the data supporting the use of antibiotic prophylaxis to prevent meningitis in post
traumatic CSF leaks is of poor quality
B) Convincing evidence to support antibiotic prophylaxis is lacking
C) Randomized, prospective, multicenter trials are needed to provide further evidence
D) Harm has been demonstrated with administration of prophylactic antibiotics

Davis 17
X) Recommendation
i) Antibiotic prophylaxis in skull fractures with CSF leak not recommended to prevent
meningitis
(a) Closed fractures of basilar skull or skull vault
ii) Concomitant conditions may benefit from antibiotic prophylaxis
(a) Le Fort facial fractures, open/penetrating fractures, compound/depressed skull fractures
(b) Potential benefit in high-risk subsets of patients with multiple risk factors cannot be fully
excluded based on current level of evidence
(1) Lack of randomization
(2) High risk patients typically received antibiotic prophylaxis
(c) Antibiotic prophylaxis when selected should cover pathogens most likely to colonize
patient’s nasopharynx
(d) Duration should be one week after CSF leak resolution
iii) Regardless of presence of antibiotic prophylaxis, patients should be monitored for signs
and symptoms associated with meningitis
(a) If suspected, empiric treatment of meningitis should be promptly initiated
(1) Obtain cultures
(2) Vancomycin + cefepime

Davis 18
References
1. Head trauma. In: Advanced Trauma Life Support. 9th ed. American College of Surgeons. 2012;148-174.
2. Corrigan J, Selassie A, Orman J. The epidemiology of traumatic brain injury. J Head Trauma Rehabil. 2010; 25:
72-80.
3. Tseng W, Shih H, Su Y, et al. The association between skull bone fractures and outcomes in patients with severe
traumatic brain injury. The Journal of Trauma. 2011; 71: 1611-1614.
4. Tasdemiroglu E, Patchell R. Classification and management of skull base fractures. Neurosurgery Quarterly. 2002;
12: 42-62.
5. Sonig A, Thakur J, Chittiboina P, et al. Is posttraumatic cerebrospinal fluid fistula a predictor of posttraumatic
meningitis? A US nationwide inpatient sample database study. Neurosurg Focus. 2012; 32: 1-7
6. Perheentupa U, Kinnunen I, Grenman R, et al. Management and outcome of pediatric skull base fractures.
Otorhinolaryngology. 2010; 74: 1245-1250.
7. Maas A, Stocchetti N, Bullock R. Moderate and severe traumatic brain injury in adults. Lancet. 2008; 7: 728-741.
8. Helling T, Evans L, Fowler D. Infectious complications in patients with severe head injury. The Journal of Trauma.
1988; 28: 1575-1577.
9. Katzen J, Jarrahy R, Eby J, et al. Craniofacial and skull base trauma. The Journal of Trauma Injury, Infection, and
Critical Care. 2003; 54: 1026-1034.
10. Fishman G, Fliss D, Benjamin S, et al. Multidisciplinary surgical approach for cerebrospinal fluid leak in children
with complex head trauma. Childs Nerv Syst. 2009; 25: 915-923.
11. Eftekhar B, Ghodsi M, Nejat F, et al. Prophylactic administration of ceftriaxone for the prevention of meningitis
after traumatic penumocephalus: results of a clinical trial. J Neurosurg. 2004; 101: 757-761.
12. Van de Beek D, Brouwer C, Thwaites G, et al. Advances in treatment of bacterial meningitis. 2012; 380: 1693-
1702.
13. Koonsman M, Dunn E, Hughes K, et al. How much monitoring is needed for basilar skull fractures? The American
Journal of Surgery. 1992; 164: 487-490.
14. Management of cerebrospinal fluid leaks. J Trauma. 2001; 51: 29-33.
15. Noffze M, Tubbs S. Rene Le Fort 1896-1951. 2011; 24: 278-281.
16. Prosser J, Vender J, Solares C. Traumatic cerebrospinal fluid leaks. Otolaryngol Clin N Am. 2011; 44: 857-873.
17. Schlosser R, Bolger W. Nasal cerebrospinal fluid leaks. The Journal of Otolaryngology. 2002; 31: 28-36.
18. Brodie H. Prophylactic antibiotics for posttraumatic cerebrospinal fluid fistulae: a meta-analysis. Arch Otolaryngol
Head Neck Surg.1997; 123: 749-752.
19. Lewin W. Cerebrospinal fluid rhinorrhea in closed head injury. The British Journal of Surgery. 1954; 171: 1-18.
20. Marentette L, Valentino J. Traumatic anterior fossa cerebrospinal fluid fistulae and craniofacial considerations.
Current Issues in Head and Neck Trauma. 1991; 24: 151-163.
21. Chandler J. Traumatic cerebrospinal fluid leakage. Otolaryngologic Clinics of North America. 1983; 16: 623-631.
22. Davies M, Teo C. Management of traumatic cerebrospinal fluid fistula. The Journal of Cranio-Maxillofacial
Trauma. 1995; 1: 9-17.
23. Tos M. Course of and sequelae to 248 petrosal fractures. Acta Otolaryng. 1973; 75: 353-354.
24. Leech P, Paterson A. Conservative and operative management for cerebrospinal-fluid leakage after closed head
injury. The Lancet. 1973; 1: 1014-1015.
25. Ziu M, Savage J, Jimenez D. Diagnosis and treatment of cerebrospinal fluid rhinorrhea following accidental
traumatic anterior skull base fractures. Neurosurg Focus. 2012; 32: 1-17.
26. Choi D, Spann R. Traumatic cerebrospinal fluid leakage: risk factors and the use of prophylactic antibiotics. British
Journal of Neurosurgery. 1996; 10: 571-575.
27. Marentette L, Valentino J. Traumatic anterior fossa cerebrospinal fluid fistulae and craniofacial considerations.
Current Issues in Head and Neck Trauma. 1991; 24: 151-163.
28. Bell R, Dierks E, Homer L, et al. Management of cerebrospinal fluid leak associated with craniomaxillofacial
trauma. J Oral Maxillofac Surg. 2004; 62: 676-684.

Davis 19
29. Yilmazlar S, Arslan E, Kocaeli H, et al. Cerebrospinal fluid leakage complicating skull base fractures: analysis of
81 cases. Neurosurg. 2006; 29: 64-71.
30. Matschke J, Tsokos M. Post-traumatic meningitis: histomorphological findings, postmortem microbiology and
forensic implications. 2001; 115: 199-205
31. Ioannis B, Soultana T, Pavlos S. Posttraumatic meningitis: bacteriology, hydrocephalus, and outcome.
Neurosurgery. 1994; 35: 422-427.
32. Mincy E. Posttraumatic cerebrospinal fluid fistula of the frontal fossa. The Journal of Trauma. 1966; 6: 618-623.
33. Sakas D, Beale D, Ameen A, et al. Compound anterior cranial bas fractures: classification using computerized
tomography scanning as a base for selection of patients for dural repair. J Neurosurg. 1998; 88: 471-477.
34. Dunn L, Foy P. Anticonvulsant and antibiotic prophylaxis in head injury. Ann R Coll Surg Engl. 1994; 76: 147-
149.
35. Eljamel M. Antibiotic prophylaxis in unrepaired CSF fistulae. British Journal of Neurosurgery. 1993; 7: 501-506.
36. Adeleye A, Basilar skull fracture: outcome of acute care without antibiotic prophylaxis in a Nigerian neurosurgical
unit. Turkish Neurosurgery. 2010; 20: 430-436.
37. Clemenza J, Kaltman S, Diamond D. Craniofacial trauma and cerebrospinal fluid leakage: a retrospective clinical
study. J Oral Maxillofac Surg. 1995; 53: 1004-1007.
38. McGuirt W, Stool S. Cerebrospinal fluid fistula: the identification and management in pediatric temporal bone
fractures. Laryngoscope. 1995; 105: 359-364.
39. Demetriades D, Charalambides D, Lakhoo M. Role of prophylactic antibiotics in open and basilar fractures of the
skull: a randomized study. Injury. 1992; 5: 377-380.
40. Ash, G. Antimicrobial prophylaxis for fractured base of skull in children. Brain Injury. 1992; 6: 521-527.
41. Frazee R, Mucha R, Farnell M, et al. Meningitis after basilar skull fracture: does antibiotic prophylaxis help?
Postgraduate Medicine. 1988; 83: 267-270.
42. Dagi F, Meyer F, Poletti C. The incidence of and prevention of meningitis after basilar skull fracture. American
Journal of Emergency Medicine. 1983; 3: 295-298.
43. Einhorn A, Mizrahi E. Basilar skull fractures in children: the incidence of CNS infections and the use of antibiotics.
Am J Dis Child. 1978; 132: 1121-1124.
44. MacGee E, Cauthene J, Brackett C. Meningitis following acute traumatic cerebrospinal fluid fistula. J Neurosurg.
1976; 33: 312-317.
45. Klastersky J, Sadeghi M, Brihaye J. Antimicrobial prophylaxis in patients with rhinorrhea or otorrhea: a double-
blind study. Surg Neurol. 1976; 6: 111-114.
46. Calvert C, Cairns, H. Discussion on injuries of the frontal and ethmoidal sinuses. Proceedings of the Royal Society
of Medicine. 1942; 35: 805-810.
47. Yilmazlar S, Arslan E, Kocaeli H, et al. Cerebrospinal fluid leakage complicating skull base fractures: analysis of
81 cases. Neurosurg Rev. 2006; 29: 64-71.
48. Zrebeet H, Huang P. Prophylactic antibiotics in the treatment of fractures at the base of the skull. Del Med Jrl.
1986; 58: 741-748.
49. Villalobos T, Arango C, Kubilis P. Antibiotic prophylaxis after basilar skull fractures: a meta-analysis. 1998; 27:
364-369.
50. Ignelzi R, VanderArk G. Analysis of the treatment of basilar skull fractures with and without antibiotics. J
Neurosurg. 1975; 43: 721-726.

Davis 20
Appendix A
Glasgow Coma Scale (GCS)
Score Eye opening Verbal response Motor response
1 None None No movements
2 Open to painful stimulation
Incomprehensible sounds Extends to pain
3 Open to voice Inappropriate words Abnormal flexion to pain
4 Open spontaneously Confused, disoriented Withdrawals to pain
5 - Oriented, converses Localizes to painful stimulus
6 - - Obeys commands
Severity of TBI based on GCS
Severity GCS Score
Mild 13-15
Moderate 9-12
Severe <8