
Anticonvulsants Yacoub Irshaid MD, PhD, ABCP Department of Pharmacology.

EPILEPSY AND
ANTICONVULCSANT (ANTIEPILEPTIC) DRUGS

Pharmacotherapy of the epilepsies
• Seizure: Transient alteration of behaviour Due to Disordered synchronous rhythmic of Brain neurones
• Epilepsy: Disorder of brain function characterized by periodic, unpredictable occurrence of seizures
• Seizures “ Non-epileptic”- Evoked in normal brain by electroshock or chemical convulsants
• Seizures “ Epileptic”- When occuring without provocation*
CAUSES OF EPILEPSY
- Genetic Factors - Antenatal and birth factors – congenital abnormalities - Infection – meningitis, viral encephalitis - Toxic factors – lead and mercury poisoning - Drug withdrawal – abrupt cessation of CNS
depressants - Cerebral injury - Metabolic disorders - Hypoxia, hyperpyrexia, hypoglycemia

CLASSIFICATION of Epipepsy : Major Seizure Types
I. Partial (focal, local) seizures
A. Simple partial seizures - Seizures may be limited to a single limb or muscle group, may show
sequential involvement of body parts. Consciousness is usually preserved;
B. Complex partial - seizures (psychomotor epilepsy,
temporal lobe epilepsy) Impairment of consciousness, may have autonomic
activity such as pupil dilation, flushing, piloerection, etc.
C. Partial seizures (evolving to secondary generalized seizures) – May generalize to tonic, clonic, or tonic-clonic

II. Generalized seizures
A. Absence seizures (Petitmal epilepsy) - Brief loss of consciousness, with or without motor
involvement; occurs in childhood with a
tendency to disappear following adolescence
B. Myoclonic seizures (Myoclonus)
• Sudden, brief, shock like contractions of musculature (myoclonic jerks) usually of the upper extremities.
C. Clonic seizures - Repetitive muscle jerks
D. Tonic seizures - Rigid, violent muscular contraction with limbs fixed
TONIC-CLONIC - Generalized seizures usually start with tonic and thereafter progress to clonic rhythmic contractions. Clonic subsides after several min. Regain consciousness.

E. Tonic-clonic seizures (grand mal epilepsy)-
Loss of consciousness; sudden sharp tonic contractions of muscles, falling to ground, followed by clonic convulsive movements; depression and incontinence
F. Atonic seizures (astatic) - Sudden diminution in
muscle tone affecting isolated muscle groups, or
loss of all muscle tone; may have extremely brief
loss of consciousness
STATUS EPILEPTICUS- dogs
II. Generalized seizures

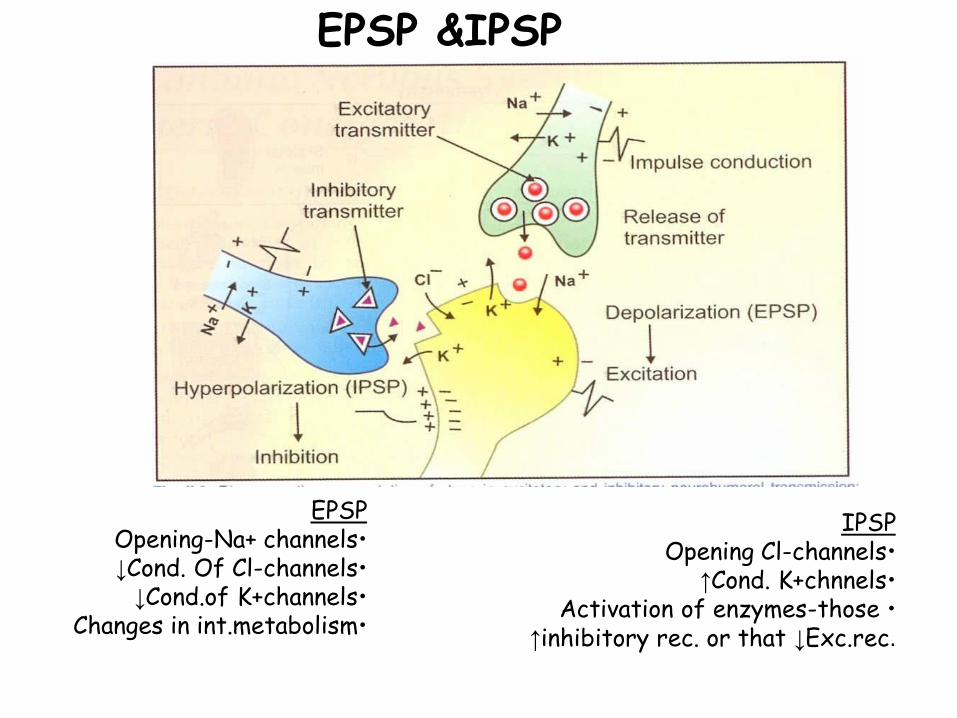
EPSP &IPSP
EPSP •Opening-Na+ channels •↓Cond. Of Cl-channels •↓Cond.of K+channels •Changes in int.metabolism
IPSP •Opening Cl-channels •↑Cond. K+chnnels •Activation of enzymes-those
↑inhibitory rec. or that ↓Exc.rec.

ANTICONVULSANT DRUGS
Mechanism of action of anticonvulsant drugs
1. Reduce excitability of cell membranes via use- dependent block of sodium channels
2. Enhance inhibitory GABAergic transmission
3. Inhibition of calcium channels

CNS DEP: Sedation Sleep Unconciousness SA Dep. Of CVS & RS Death
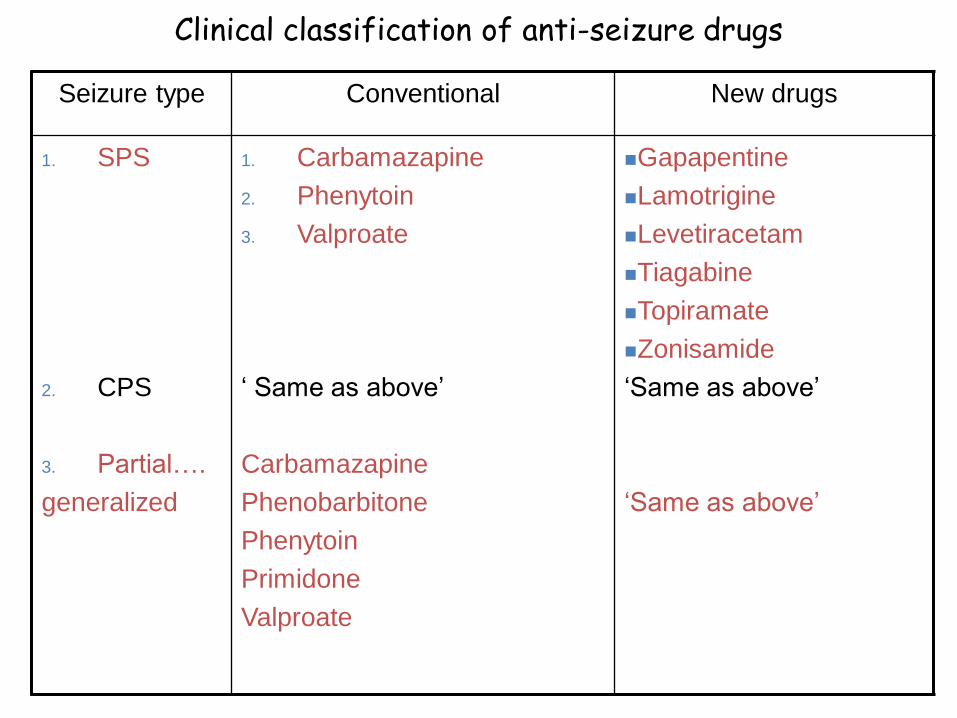
Clinical classification of anti-seizure drugs
Seizure type Conventional New drugs
1. SPS
2. CPS
3. Partial….
generalized
1. Carbamazapine
2. Phenytoin
3. Valproate
‘ Same as above’
Carbamazapine
Phenobarbitone
Phenytoin
Primidone
Valproate
Gapapentine
Lamotrigine
Levetiracetam
Tiagabine
Topiramate
Zonisamide
‘Same as above’
‘Same as above’
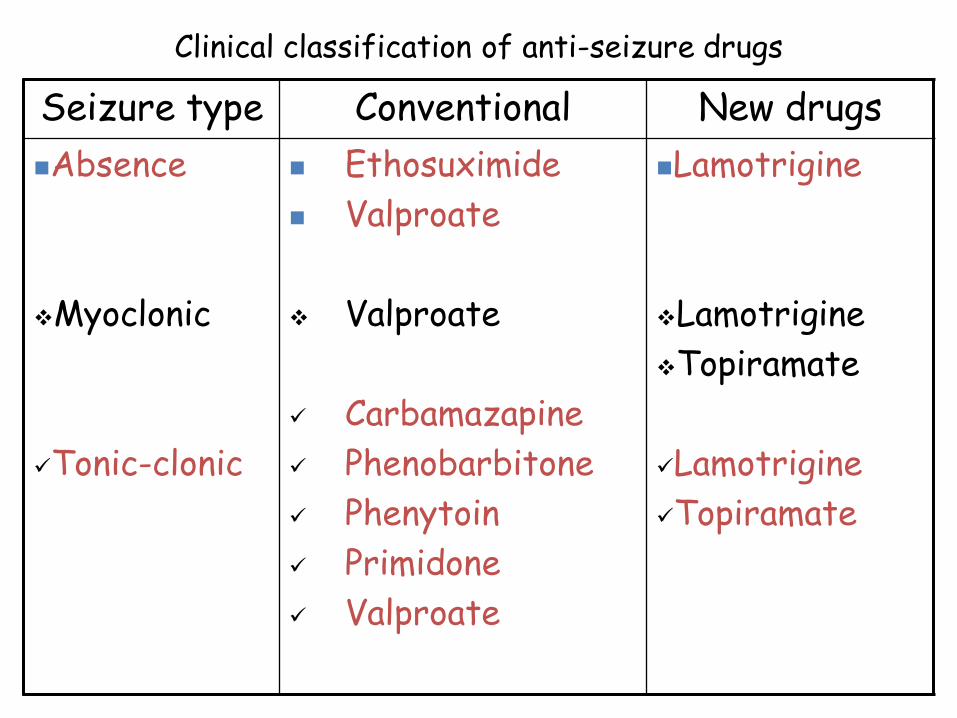
Clinical classification of anti-seizure drugs
Seizure type Conventional New drugs
Absence
Myoclonic
Tonic-clonic
Ethosuximide
Valproate
Valproate
Carbamazapine
Phenobarbitone
Phenytoin
Primidone
Valproate
Lamotrigine
Lamotrigine
Topiramate
Lamotrigine
Topiramate

Clinical classification of anti-seizure drugs
Seizure Drugs Second choice
Febrile
Status
epilepticus
Diazepam rectal
Diazepam i.v.
Lorazepam i.v.
Fosphenytoin i.v.
Pheno i.v.
Movie!

MOA of antiseizure drugs
• Reduce excitationReduce EPSP Enhance Na or Ca channel inactivation
Carbamazapine Lamotrigine
Phenytoin Valproate
Topiramate Zonisamide
Valproate
Ethosuximide
Trimethadione

MOA of antiseizure drugs
• Promote inhibition Promote IPSP Enhance GABA transmission [Cl channels]
BZD
GABA
binding sites
Barbiturates
GABA
↓ GABA-T
Succinic semialdehyde
↓ Dehydrogenase
Metabolites
GAT-1 GABA
Vigabatrine
Valproate Tiagabine
Guidelines to drug therapy
• Start with single, well tried safe drug
• According to type of seizure
• Age, sex-Hirsutism, terratogenicity, hepatitis
• Single drug Failure SUBSTITUTE with second[difft.MOA] withdrawal of First gradual
• Three drug hardly useful
• Dosage increased at particular time*

BARBITURATES and BENZODIAZEPINES
• Phenobarbitione, pentobarbitone, Mephobarbitone, Secobarbitone
• Potentiate inhibitory GABAergic transmission increasing the duration or frequency of chloride channel opening.
• used for the treatment of status epilepticus. Treatment must be initiated rapidly.
• Intravenous diazepam is the treatment of choice
• Other possibilities if benzodiazepines fail include intravenous phenytoin, Phenobarbital or general anaesthesia.
Benzodiazepines
• Clonazepam Absence & Myoclonic
• Diazepam & Lorazepam S tatus epilepticus
• Clobazam, Clorazepate + Other drugs Partial seizures
Diazepam:
Not used in long term[Sedation, tolerance]
Control of convulsions[Epilepsy & others]
0,2-0.5mg/kg slow i.v. 100mg/day
ADE-Fall of BP, Resp.dep.,
Rectally in children-Febrile
Lorazepam: 0.1mg/kg-i.v.-Long duration*

PHENYTOIN
This is the oldest non-sedative anticonvulsant drug
and is still one of the most widely used.
Mechanism of action: At therapeutic levels, the
main action of phenytoin is to block sodium
channels and inhibit the generation of repetitive
action potentials.

Pharmacokinetics: Effective after oral administration.
Absorption is almost complete in most patients. It is
highly bound to plasma proteins. Metabolism in
the liver is by hydroxylation followed by conjugation
with glucuronic acid. The metabolites are
excreted in the urine.
PHENYTOIN
Drug Interactions-Phenytoin
• Pheno & Phenytoin: Both induce enzymes metabolism of each other Result unpredictable
• CBMZP & Phenytoin Induce each others metabolism
• Valproate Displaces phenytoin Also decreases metabolism! Phenytoin toxicity
• Chloromphenicol, Cimetidine etc. inhibit Phenytoin metabolism
• Phenytoin inhibits Warfarin metabolism
• OCP and Phenytoin*

Uses:
1. Treatment of generalized tonic-clonic seizures
and partial seizures
2. Treatment of disturbed psychotic patients
without epilepsy
3. Cardiac arrhythmias
Side effects:
These are usually dose-related.
1. Gingival hyperplasia, hirsutism, nystagmus, ataxia
2. Coarsening of facial features and osteomalacia
3. Blood dyscrasias eg aplastic anaemia
PHENYTOIN

PRIMIDONE
• 2-deoxy analogue of phenobarbitone
• hepatotoxic – withdrawn
BROMIDES
• Sodium, Potassium, Ammonium bromide salts
• Bromism- bromide accumulation toxicity – adverse effect

Ethosuximide
• Reduces Ca flow in ‘T’ type Ca channels
• Reduces 3Hz spikes[EEG] from thalamus neurones
• Effective in absence seizures only[ No action on Na and GABA]
• ADE- GI, Behavioral effects[Anxiety, inability to concentrate)
CARBAMAZEPINE • Acts by blocking voltage-gated sodium channels (binds to
sodium channels in the inactive state). • orally active and bound (75%) to plasma proteins. It has
antidepressant properties. Slows rate of recovery of inactivated Na channels Prevents
repetitive firing of AP. • Ph.effects: Similar to phenytoin Antidiuretic effect* Uses: Carbamazepine is used for tonic-clonic and partial
seizures. It is also used in pain and manic depression.
Side effects include:
1. induction of liver enzymes 2. ataxia 3. diplopia 4. aplastic anaemia (not very common)

VALPROIC ACID
Valproic acid acts by:
1. Hyperpolarizing neuronal membranes through an action on potassium channels.
2. Blocking sodium channels (in the inactive state).
3. Increasing GABA levels by inhibiting GABA-T It is used for tonic-clonic and partial seizures
Side effects include: 1. ataxia 2. diarrhea 3. induction of liver enzymes and hepatic failure 4. Gastric irritation 5. teratogenicity

NEWER ANTICONVULSANT DRUGS
Lamotrigine:
• Developed as antifolate agent, Anticonvlsant axction-not related to antifolate
• Suppresses repetitive action potentials by blocking sodium channels in a use-dependent manner.
• inhibits the release of glutamate.
• used for tonic-clonic and partial seizures.
• Side effects- blurred vision and GIT upset.
Tiagabine:
• prevents reuptake of GABA thus raising GABA levels.
• used for partial Seizures.
Others: Levetiracetam, Topiramate, Felbamate, Zonisamide
NEWER ANTICONVULSANT DRUGS
Vigabatrin:
• Acts as an irreversible inhibitor of GABA-T and therefore prevents degradation of GABA leading to elevated levels of GABA.
• It is used for Partial and infantile seizures.
Gabapentin:
• Increases neuronal release of GABA.
• It is used as an adjunct in patients with partial seizures. Side effects include ataxia, dizziness and fatigue.














![HIGHLIGHTS OF PRESCRIBING INFORMATION ...3 Interactions (7.2), and Clinical Pharmacology (12.3)].These drugs include, but are not limited to, the following: - the anticonvulsants carbamazepine,](https://static.fdocuments.us/doc/165x107/5f10dda97e708231d44b30f6/highlights-of-prescribing-information-3-interactions-72-and-clinical-pharmacology.jpg)


