Anticonvulsants Yacoub Irshaid MD, PhD, ABCP Department of Pharmacology.
74
Anticonvulsants Yacoub Irshaid MD, PhD, ABCP Department of Pharmacology
-
Upload
judith-clarke -
Category
Documents
-
view
221 -
download
0
Transcript of Anticonvulsants Yacoub Irshaid MD, PhD, ABCP Department of Pharmacology.
Anticonvulsants
Yacoub Irshaid MD, PhD, ABCP
Department of Pharmacology
Anticonvulsants
• ~ 1% of the world population has epilepsy.
• Standard therapy permits control of only ~ 80% of seizures (adequate in only 2/3rds).
• Epilepsy is a heterogeneous symptom complex, chronic disorder characterized by recurrence.
• Seizures are finite episodes of brain dysfunction resulting from abnormal discharge of cerebral neurons.

Anticonvulsants
• A fraction of epileptic population is resistant to all available drugs, which may be due to increased expression of the multidrug transporter P-glycoprotein.
• In children, some severe seizures associated with progressive brain damage are very difficult to treat.

Anticonvulsants

Anticonvulsants

Anticonvulsants
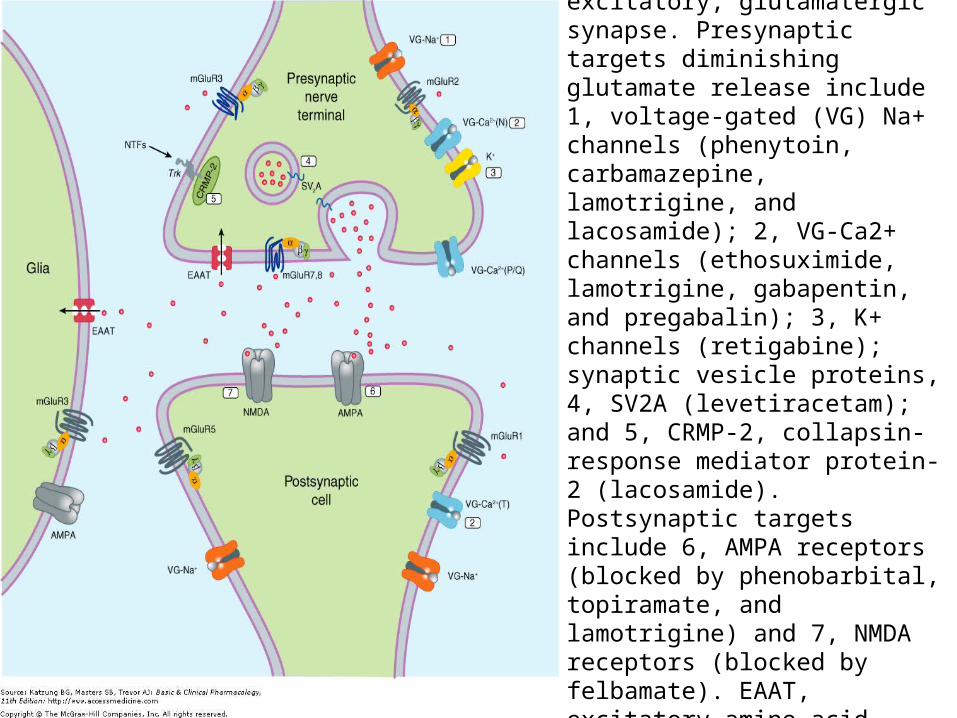
Molecular targets for antiseizure drugs at the excitatory, glutamatergic synapse. Presynaptic targets diminishing glutamate release include 1, voltage-gated (VG) Na+ channels (phenytoin, carbamazepine, lamotrigine, and lacosamide); 2, VG-Ca2+ channels (ethosuximide, lamotrigine, gabapentin, and pregabalin); 3, K+ channels (retigabine); synaptic vesicle proteins, 4, SV2A (levetiracetam); and 5, CRMP-2, collapsin-response mediator protein-2 (lacosamide). Postsynaptic targets include 6, AMPA receptors (blocked by phenobarbital, topiramate, and lamotrigine) and 7, NMDA receptors (blocked by felbamate). EAAT, excitatory amino acid transporter. Red dots represent glutamate.
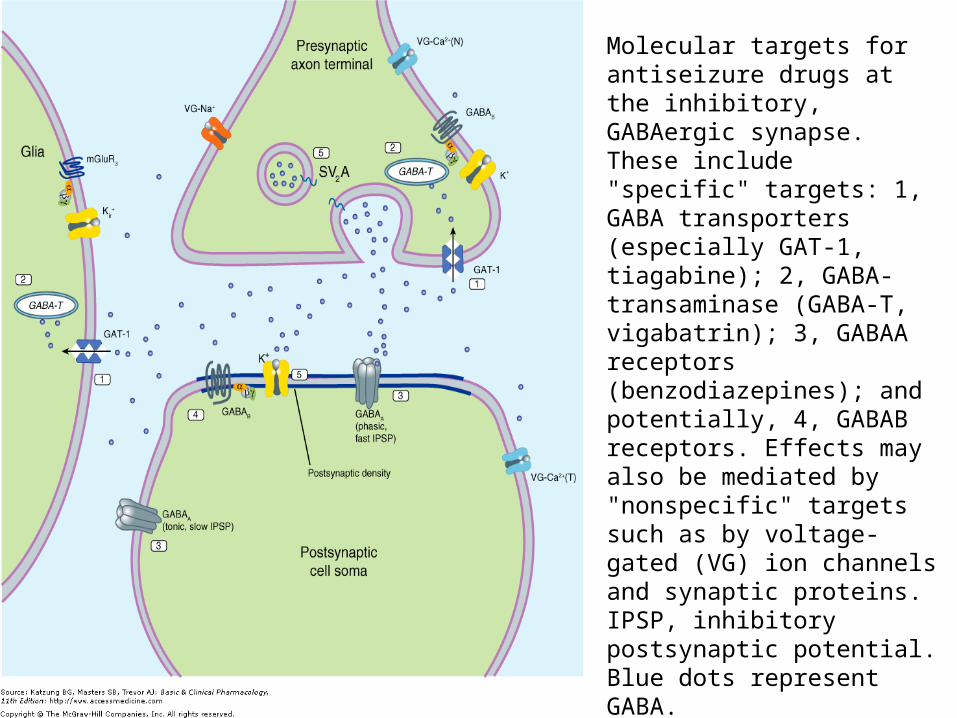
Molecular targets for antiseizure drugs at the inhibitory, GABAergic synapse. These include "specific" targets: 1, GABA transporters (especially GAT-1, tiagabine); 2, GABA-transaminase (GABA-T, vigabatrin); 3, GABAA receptors (benzodiazepines); and potentially, 4, GABAB receptors. Effects may also be mediated by "nonspecific" targets such as by voltage-gated (VG) ion channels and synaptic proteins. IPSP, inhibitory postsynaptic potential. Blue dots represent GABA.
Phenytoin
• The oldest nonsedative antiseizure drug (1938).
• Fosphenytoin is a soluble prodrug of phenytoin (phosphate ester).
Mechanism of Action:• At therapeutic concentrations, the major
action of phenytoin is to block sodium channels and inhibit the generation of rapidly repetitive action potentials.

Phenytoin
• Reduction of calcium permeability, with inhibition of calcium influx across the cell membrane may explain its ability to inhibit a variety of secretory processes, including release of hormones and neurotransmitters (glutamate, GABA, norepinephrine and acetylcholine).
• Pardoxically, phenytoin causes excitation in some cerebral neurons.

Phenytoin
Therapeutic uses:
1. Partial seizures
2. Generalized tonic-clonic seizures (1° or 2°).
Pharmacokinetics:
• Absorption is highly dependent on the formulation of the dosage form.
• Particle size and pharmaceutical additives affect both the rate and extent of absorption.

Phenytoin
• Absorption of phenytoin Na from the GIT is almost complete, although the time to peak ranges from 3-12 hours.
• Absorption after IM injection is unpredictable, since some drug precipitation in the muscle occurs (not recommended route).
• In contrast, fosphenytoin (a more soluble phosphate prodrug) is well absorbed after IM administration.
Phenytoin
• It is highly bound to plasma proteins.• The total plasma level decreases when the
percent bound decreases, as in uremia or hypoalbuminemia.
• Drug concentration in CSF is proportional to the free plasma level.
• It accumulates in brain, liver, muscle and fat
• It is metabolized to inactive metabolites.

Phenytoin
• The elimination of phenytoin is dose-dependent: At very low dose levels, phenytoin metabolism follows first-order kinetics. However, as blood levels rise within the therapeutic range, zero-order (saturation) kinetics prevail. Small increases in dosage may produce very large changes in phenytoin concentrations.

Phenytoin
In such cases, the half-life of the drug increases markedly, and steady state is not achieved.
• Half-life ranges from12-36 hours in patients with low to mid therapeutic range, and much higher at higher concentrations.
• At low levels it takes 5-7 days to reach steady-state. (At higher doses 4-6 weeks are needed to reach SS).

Nonlinear relationship of phenytoin dosage and plasma concentrations. Five patients (identified by different symbols) received increasing dosages of phenytoin by mouth, and the steady-state serum concentration was measured at each dosage. The curves are not linear, since, as the dosage increases, the metabolism is saturable. Note also the marked variation among patients in the serum levels achieved at any dosage.

Phenytoin
• Therapeutic total plasma level is between 10-20 μg/mL.
Drug Interactions:
1. Phenylbutazone and sulfonamides can displace phenytoin from binding sites to plasma proteins.
2. Hypoalbuminemia results in decreased total plasma drug concentration but not the free concentration.

Phenytoin
• In these 2 cases intoxication may occur if total drug levels are increased by increasing the dose.
3. The drug has affinity for thyroid-binding globulin which confuses some tests for thyroid function.
4. Phenytoin induces many drug metabolizing enzymes.
5. Phenobarbital and carbamazepine induce the metabolism of phenytoin.

Phenytoin
6. Isoniazid inhibits the metabolism of phenytoin.
Adverse effects:1. Nystagmus.2. Diplopia and ataxia are the most common
dose-related adverse effects, requiring dose reduction.
3. Sedation only occurs at high levels.4. Gingival hyperplasia.5. Hirsutism

Phenytoin
6. Long-term use is associated with:a. coarsening of facial featuresb. mild peripheral neuropathy (diminished deep tendon reflexes in the lower limbs).c. osteomalacia due to altered vitamin D metabolism.d. megaloblastic anemia secondary to low folate levels.

Phenytoin
7. Idiosyncratic reactions:
a. hypersensitivity reaction and skin rash.
b. fever.
c. exfoliative skin lesions.
d. lymphadenopathy.
e. agranulocytosis.
Carbamazepine
• A tricyclic compound related to imipramine.
Mechanism of Action:
• It blocks sodium channels, like phenytoin.
• It acts also presynaptically to decrease synaptic transmission.

Carbamazepine
Therapeutic uses:
1. Partial seizures
2. Generalized tonic-clonic seizures
3. Trigeminal neuralgia
4. Bipolar manic-depressive disorder
• Therapeutic drug level is ~ 4-8 μg/mL.

Carbamazepine
Pharmacokinetics:
• There is interindividual variation in oral absorption.
• Absorption is slowed if given after meals.
• Volume of distribution is low (1L/Kg).
• Clearance is also low.
• Binding to plasma proteins is ~ 70%.

Carbamazepine
• Induces microsomal drug metabolizing enzymes.
• Induces its own metabolism (autoinduction) t½ after initial dose is ~ 36 hours, and after continuous therapy becomes ~ 8-12 hours (dose adjustment is needed within 1 week of therapy).
• It is completely metabolized to several metabolites. One, carbamazepine-10,11-epoxide, has anticonvulsant activity.
Carbamazepine
Drug interactions:• It increases the metabolism of primidone,
phenytoin, ethosuximide, valproic acid, and clonazepam.
• Propoxyphene, troleandomycin, and valproic acid may inhibit carbamazepine clearance and increase its steady-state levels.
• Phenytoin and phenobarbital decrease SS concentration of carbamazepine by enzyme induction.

Carbamazepine
Adverse effects:1. The most common dose-related adverse
effects are diplopia and ataxia.2. Mild GIT upset.3. Unsteadiness and drowsiness.4. Hyponatremia and water intoxication.5. Idiosyncratic reactions: aplastic anemia
and agranulocytosis, leukopenia, erythematous skin rash and hepatic dysfunction.

Phenobarbital
• Is the oldest of the currently available antiseizure drugs.
• Has sedative effect (?).
• Some consider that it is the drug of choice for responsive seizures only in infants.
• A weak acid.

Phenobarbital
Mechanism of Action:• Recent data indicate that it selectively
suppresses abnormal neurons, suppressing firing from foci and inhibiting spread of impulses and thus seizures.
• It enhances GABA effects by prolonging opening of the chloride channels.
• It blocks excitatory responses induced by glutamate.

Phenobarbital
Therapeutic uses:
1. Partial seizures
2. Generalized tonic-clonic seizures
3. Febrile seizures
• It may worsen absence seizures, atonic attacks, and infantile spasms.
• Therapeutic level is ~ 10-40 μg/mL

Primidone
• It is 2-desoxyphenobarbital
• It is metabolized to phenobarbital and phenylethylmalonamide (PEMA).
• All 3 compounds are anticonvulsants.
• The mechanism of action of primidone may be more like phenytoin.
• Therapeutic uses are similar to phenobarbital.
Primidone
• Therapeutic range is ~ 8-12 μg/mL.
• Measure also phenobarbital concentration.
• After start of treatment with primidone the time to reach steady-state for primidone is 30-40 hours, phenobarbital 20 days and PEMA 3-4 days.

Primidone
Pharmacokinetics:• Primidone is completely absorbed.• Has a small volume of distribution
(total body water).• It is not highly bound to plasma
proteins• t½ is ~ 6-8 hours
Adverse effects are similar to phenobarbital.

Vigabatrin
• Is gama-vinyl-GABA• It is an irreversible inhibitor of GABA
aminotransferase, the enzyme responsible for the degradation of GABA increase in the amount of GABA at synapse.
• It is useful in the treatment of partial seizures.
• t½ is ~ 6-8 hours but activity is more prolonged and not well correlated to half-life.

Vigabatrin
Adverse effects:
• Drowsiness, dizziness and weight gain are typical toxicities.
• Less common but more troublesome adverse effects include agitation, confusion, and psychosis.
• Preexisting mental illness is a relative contraindication.

Vigabatrin
• Long-term treatment has been associated with visual field defects in up to one third of patients, which might not be reversible.
• Therefore, it is used only in patients refractory to other treatments (infantile spasm).
Lamotrigine
Mechanism of Action:Like phenytoin, it produces a voltage- and use-dependant inactivation of sodium channels.It suppresses sustained rapid firing of neurons.
• This explains its efficacy in focal epilepsy.• Other mechanisms include:

Lamotrigine
a. Possible actions on voltage-activated Ca2+ channels.b. Reduction in synaptic release of glutamate.
Clinical Uses:1. Monotherapy for partial seizures.
Therapeutic blood level ~ 3 µg/mL.2. Absence and myoclonic seizures in
children.
Lamotrigine
Pharmacokinetics:• Almost completely absorbed.• Vd ~ 1-1.4 L/Kg.• Protein binding ~ 55%.• Metabolized by glucuronidation.• t½ ~ 24 hours in normal volunteers, which
decreases to ~ 14 hours in patients taking enzyme inducers.
• Valproate causes a 2-fold increase in half-life.

Lamotrigine
Adverse Effects:
1. Dizziness, headache, diplopia, nausea, somnolence
2. Hypersensitivity reaction: skin rash.
3. A potentially life-threatening dermatitis in 1-2 % of pediatric patients.

Felbamate
Mechanisms of Action:1. It produces a use-dependent block of
NMDA receptor.2. It potentiates GABAA receptor responses.Pharmacokinetics:• t½ ~ 20 hours, which is shortened with
coadministration of phenytoin or carbamazepine.
• Partially metabolized by hydroxylation and glucuronidation and partially excreted unchanged in urine.
Felbamate
Clinical uses:1. Partial seizures (therapeutic
concentration 30-100 µg/mL). Third-line agent.
2. Lennox-Gastaut syndrome (Occurs in children and is characterized by tonic, atonic, and myoclonic seizures; and atypical absence seizures, that is associated with mental retardation).
Felbamate
Adverse Effects:
A high rate of
1. Aplastic anemia
2. Severe hepatitis
• It increases plasma phenytoin and valproic acid levels and decreases that of carbamazepine.

Gabapentin & Pregabalin
• Gabapentin is an amino acid analog of GABA, that is effective against partial seizures. It is a spasmolytic.
• Pregabalin is also an analog of GABA, which has antiseizure activity and analgesic properties.
Mechanism of Action:• They do not act directly on GABA receptors
despite structural resemblance to GABA.
Gabapentin & Pregabalin
• They may modify the synaptic and nonsynaptic release of GABA an increase in brain GABA concentration.
• They bind avidly to the voltage-gated Ca2+ channels.
• Decrease the release of glutamate presynaptically, which is probably dependent on reduced presynaptic entry of calcium via voltage activated channels.
Gabapentin & Pregabalin
Pharmacokinetics:• These drugs are not metabolized and do not
induce hepatic enzymes.• They are eliminated by the kidney unchanged.• Absorption is nonlinear and dose-dependent at
very high doses.• Elimination kinetics are linear.• Not bound to plasma proteins.• Gabapentin is transported to the brain by L-
amino acid transporter.• t½ is short (5-8 hours).• No significant drug interactions.
Gabapentin & Pregabalin
Clinical Uses:1. Adjunct against partial seizures and
generalized tonic-clonic seizures.2. Neuropathic pain, postherpetic
neuralgia, and painful diabetic peripheral neuropathy.
Adverse Effects:Somnolence, dizziness, ataxia, headache and tremor.

Levetiracetam
• Binds selectively to a synaptic vesicular protein (function is not understood). It is likely that the drug modifies synaptic release of glutamate and GABA.
• Used for partial seizures.• Oral absorption is complete, rapid and unaffected by
food.• Kinetics are linear.• Protein binding is low.• t½ ~ 6-8 hours.• Two thirds excreted unchanged, not metabolized by
P450.• Drug interactions are minimal.• Adverse effects include somnolence, asthenia,
dizziness and idiosyncratic reactions.

Tiagabine
Mechanism of Action:
• It is an inhibitor of GABA uptake in both neurons and glia, and increases extracellular GABA levels in the forebrain and hippocampus. It prolongs the inhibitory action of synaptically released GABA.
Tiagabine
Pharmacokinetics:• Very well absorbed, linear kinetics, highly
protein bound.• t½ ~ 5-8 hours, decreases in the presence of
enzyme inducers.• Food decreases the rate but not extent of
absorption.• Does not cause induction or inhibition of
hepatic enzymes.• Oxidized by CYP3A and metabolized are
excreted in bile (65%) and Urine (25%).
Tiagabine
Clinical Uses:Adjunctive treatment of partial seizures. Some patients do well with monotherapy.
Adverse Effects:• Nervousness, dizziness, tremor, difficulty
in concentrating, and depression.• Excessive confusion, somnolence, or
ataxia may require discontinuation.• Psychosis is rare.• Rash is uncommon idiosyncratic reaction.

Topiramate
• A substituted monosaccharide that is structurally different from all other anticonvulsants.
Mechanism of Action:1. Similar to phenytoin and carbamazepine. It may
involve blocking of voltage-gated sodium channel.
2. It may potentiate the inhibitory effect of GABA, acting at different site from that of benzodiazepine and barbiturates.
3. It depresses the excitatory action of kainate on glutamate receptors

Topiramate
Pharmacokinetics:
• It is rapidly absorbed and is 80% bioavailable.
• No food effect on absorption.
• Minimal plasma protein binding.
• Moderate metabolism (20-50%).
• t½ ~ 20-30 hours.
• Birth control pills may be less effective in the presence of topiramate.

Topiramate
Clinical Uses:
1. Monotherapy of partial and generalized tonic-clonic seizures
2. Lennox-Gestaut syndrome, West’s syndrome (infantile spasm).
3. Absence seizures.
4. Migraine headache.

Topiramate
Adverse Effects:• Somnolence, fatigue, dizziness,
cognitive slowing, paresthesias, nervousness and confusion – dose related.
• Acute myopia and glaucoma may require prompt drug withdrawal.
• Urolithiasis.• Teratogenic – hypospadius (?).
Zonisamide
• Is a sulfonamide derivative• The primary site of action appears to be the
sodium channel.• It may also act on the voltage-gated calcium
channels.• Effective against partial and generalized tonic-
clonic seizures.• May be effective against infantile spasms and
certain myoclonias.• Adverse effects include drowsiness, cognitive
impairment and potentially serious skin rashes.

Ethosuximide
Mechanism of Action:• It reduces the low-threshold (T-type)
Ca2+ currents in thalamic neurons. This current is thought to provide a pacemaker current in thalamic neurons responsible for generating the rhythmic cortical discharge of the absence attack. Thus, It has narrow spectrum of activity.

Ethosuximide
Pharmacokinetics:• Complete absorption.• Not protein bound.• Completely metabolized to inactive products.• t½ ~ 40 (18-72) hours.• Linear kinetics.• Therapeutic concentration is ~ 60-100 µg/mL.• Valproic acid inhibits its metabolism
decreased clearance.

Ethosuximide
Adverse Effects:
1. The most common is gastric distress – pain, nausea, and vomiting.
2. Transient lethargy and fatigue.
3. Headache, dizziness, hiccup, and euphoria.
4. Idiosyncratic reactions: skin rash, Stevens-Johnson syndrome.
5. Development of lupus erythematosus (?).
Valproic Acid & Sodium Valproate
• A fatty carboxylic acid.• The active form is the valproate ion.
Mechanism of Action:• Anticonvulsant activity appears to be
poorly correlated with blood or tissue level of the parent drug.
• Like phenytoin and carbamazepine, it blocks sustained high frequency repetitive firing of neurons, an effect on Na+ current.

Valproic Acid
• Blockade of NMDA receptor-mediated excitation may be important.
• It increases the levels of GABA in the brain due to (?):a. Increased synthesis by facilitating glutamic acid decarboxylase.b. Inhibition of an GABA transporter
• It is a broad spectrum anticonvulsant.
Valproic Acid
c. At high concentration, it blocks GABA degradation by GABA transaminase.
• GABA is not always increased at effective concentrations of the drug.
• It is a potent inhibitor of histone deacetylase and may change the transcription of many genes.

Valproic Acid
Pharmacokinetics:• Well absorbed after oral administration.• Food may delay absorption.• It is 90% bound to plasma proteins,
binding is saturable, and the free fraction is increased at plasma levels of > 150 μg/mL.
• It is distributed to extracellular water (Vd ~ 0.15 L/Kg) (why?).

Valproic Acid
• t½ ~ 9-18 hours.• 20% eliminated as a direct conjugate.• Clearance is low and dose-dependent.
Clinical uses:
1. Absence seizures. If they occur alone, ethosuximide is preferred, while if they occur in the presence of generalized tonic-clonic seizures, valproate is preferred.
Valproic Acid
2. Myoclonic seizures.
3. Tonic-clonic seizures.
4. Atonic attacks – few patients respond.
5. Partial seizures.
6. Bipolar disorders.
7. Migraine prophylaxis.
• Therapeutic levels ~ 50-100 μg/mL.

Valproic Acid
Drug Interactions:
1. It displaces phenytoin from plasma proteins.
2. It inhibits the metabolism of phenobarbital, phenytoin, carbamazepine, and other drugs.

Valproic Acid
Adverse Effects:1. The most common dose-related
adverse effects are nausea, vomiting, abdominal pain and heart burn. Gradual starting avoids them.
2. Sedation is uncommon with valproate alone but becomes striking when combined with phenobarbital.
3. Fine tremor.

Valproic Acid
4. Increased appetite and weight gain.5. Loss of hair.6. Hepatotoxicity (idiosyncratic). Can be
severe and fatal. Risk is more in patients under the age of 2 years, and those taking multiple medications. May be reversible in some patients if the drug is discontinued. Some clinicians recommend the use of L-carnitine (PO or IV) as soon as hepatotoxicity is suspected.

Valproic Acid
• VPA inhibits the biosynthesis of carnitine contributing to carnitine deficiency.
• Carnitine enhances the β-oxidation of fatty acids (including VPA), thereby limiting its omega-oxidation to hepatotoxic metabolites.
Valproic Acid
7. Thrombocytopenia (idiosyncratic).
8. Teratogenicity (spina bifida, cardiovascular, orofacial and digital abnormalities).
• Despite that valproate is popular, effective, since a small number of patients had severe adverse effects.

Other Drugs
Trimethadione:• For absence seizures, not popular
because of marked sedation.Diazepam, Lorazepam:• Are used to terminate continuous
seizure activity, especially generalized tonic-clonic status epilepticus. Lorazepam may be more effective and longer- acting.

Other Drugs
Clonazepam:
• Long-acting, with documented activity against absence seizures. It is also effective in some cases of myoclonic seizures. Sedation is prominent.
Nitrazepam:
• Used for infantile spasms and myoclonic seizures.
Other Drugs
Clorazepate dipottasium:• Adjunct treatment of complex partial
seizures in adults. Drowsiness and lethargy are common.
• Tolerance develop for anticonvulsant action of benzodiazepines and their efficacy is limited by the sedation they produce.

Effective Plasma Levels of Six Antiseizure Drugs
DrugEffective Level (mcg/mL)
High Effective Level1 (mcg/mL)
Toxic Level (mcg/mL)
Carbamazepine 4–127> 8
Primidone 5–1510< 12
Phenytoin 10–2018> 20
Phenobarbital 10–4035> 40
Ethosuximide 50–10080> 100
Valproate50–10080> 100