Antibiotics Mechanisms of Action - 1994

of 10
-
Upload
camiloz666 -
Category
Documents
-
view
215 -
download
0
Transcript of Antibiotics Mechanisms of Action - 1994
-
7/30/2019 Antibiotics Mechanisms of Action - 1994
1/10
DOI:10.1542/pir.15-11-440
1994;15;440-447Pediatr. Rev.Kathleen A. Woodin and Susan H. Morrison
BACK TO BASICS: Antibiotics: Mechanisms of Action
http://pedsinreview.aappublications.orgthe World Wide Web at:
The online version of this article, along with updated information and services, is located on
Print ISSN: 0191-9601. Online ISSN: 1526-3347.Village, Illinois, 60007. Copyright 1994 by the American Academy of Pediatrics. All rights reserved.
trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Groveandpublication, it has been published continuously since 1979. Pediatrics in Review is owned, published,
Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
at Health Internetwork on July 29, 2008http://pedsinreview.aappublications.orgDownloaded from
http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/ -
7/30/2019 Antibiotics Mechanisms of Action - 1994
2/10
44 0 P ed iatrics in Rev iew V oL 15 No. 11 Novem ber 1994
Ant ib iot ics : M ech an ism s o f A ctionK ath leen A . W ood in , M D * and S usan H . M o rrison , M D tM edica l prac tice rests on the founda tion o f science . C lin icia ns are constan tly m ak ing p rac tica l dec isions and d ea lingw ith imm ed ia te situa tio ns tha t dem and so lu tion s. T im e should b e taken to fo cu s on th ose sc ien tific prin cip les tha tu nderlie o ur d iagnostic and therapeu tic m aneuvers. Th is sec tion o f Ped ia tric s in R ev iew presen ts se lected top ics tha ta re re levan t to pra ctice from the area s o f physio lo gy , p harm aco logy , b iochem is try, and o ther d isc ip lin es; c lar ifica tiono f these w ill a ugm ent the ped ia tric ia n s understand ing o f c lin ica l p rocedures.
In t roduct ionU n like p hys icians p rac tic ing in the19 40s, w ho had on ly su lfonam id esan d p en ic illin to trea t in fectio ns,p rac tition ers now choose from abroad (and som e tim es o ve rw he lm in g)n um ber o f an tib io tics . H ow eve r ,trend s in em erg in g an tim icrob ial re -sis tance m ay fo rce us to take a g ian tstep b ackw ard to tha t frig h ten ing sit-ua tion of the past o f h av ing b ac te riath at a re e ssen tia lly u n trea tab le byany of o ur av ailab le an tib io tics .
T h is a r ticle is an o ve rv iew o f som eof the m ic rob io logy , ph arm aco log y ,and physio logy c ritica l to the ratio na lu se o f an tib io tics in tod ay s p rac tice .I t summ arize s the basic m ech an ism sof ac tion of som e comm only u sedan tib io tic s an d b rie f ly d iscu sse s th eem ergence o f re sis tance to seve ra lcom mon pa tho gens.S truc tu res o f B ac te r iaIm po rtan t to A n tib io ticAct ionT he ou term os t com pon en t o f m o stbac ter ia is the cell w a ll, a m ultilay -e red s truc tu re lo ca ted ex terna l to thecy to p la sm ic m em bran e. Th e ce ll w a llis com po sed of an inn e r laye r o f pep -tido g lycan , a com plex in te rw oven lat-tic e o f linear sug ars (g lycan ) tha t a re
c ros s-lin ked b y pep tide cha ins. P ep -tidog lycan prov id es th e r ig id su ppo rtby w hich the ce ll m a in ta ins its cha r-acte r is tic sh ap e.
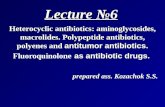
G ram -po sitive an d G ram -n eg a tivebac ter ia d iffe r in the ir cell w all s truc -tu res (F ig u re) . In G ram -pos itiv eo rgan ism s, the pep tid og ly can laye r isa th ick (1 5 to 80 nm ) m ultilaye r an dm ay hav e a th in laye r o f te icho icacid ou tside the pep tid og ly can . Incon tra st, G ram -neg ativ e o rg an ism shave a th in (2 nm ) sing le lay e r o fp ep tidog lycan cove red by a com plexou te r m em bran e lay er com po sed o flip opo lysacch arides, lipop ro te in s, andpho sph o lip ids . T he ou te r m em braneof G ram -nega tive bac ter ia con ta insporn pro te ins tha t ac t a s ch an ne ls totransp ort sm a ll m o lecu le s su ch assuga rs , m e tals , v itam in s, and an tib io t-ics in to th e b ac te ria l ce ll.
T he cy top lasm o f bac ter ia con tain san inn er nu c leo id reg ion com po sed ofsing le -strand ed c ircu la r D NA andm atrix th a t con ta ins r ibo som es, nu tr i-en t g ranu le s , m e tab o lite s , and p la s-m ids . P la sm ids are doub le -strandedc ircu lar D NA m olecu les th at can rep -lica te indep en den tly o f th e bac ter ia lch rom o som es . M o st p la sm id s are ex -trach rom osom a l, b u t som e a re in te -g ra ted in to th e b acte r ial ch rom osom e .
P la sm ids o ccur in bo th G ram -n ega -tiv e an d G ram -po sitive o rgan ism sand a re an im portan t sou rce o fgene tic in fo rm a tion th a t can conveyre sis tance to v ariou s an tib io tics .Se lec tive Tox ic ityA n id ea l an tim ic ro b ia l agen t w ou ldexh ib it s elec tive tox ic ity ; tha t is , thed rug w ou ld b e ha rm fu l to th e in fect-ing m ic roo rgan ism w ithou t h arm ingthe h ost. B ecause pep tido g lycan isp re sen t in b ac te ria bu t no t in h um ance lls , it is an exce llen t ta rg et fo r an ti-b io tic s . S im ila rly , an tib io tic s th at a f-fec t p ro tein syn thesis take advan tag eo f the d iffe rences in size and ch em i-ca l com position of r ibo som es frombac te ria an d euk aryo tic o rg an ism s (ie ,th ose hav ing a true nu c leu s su r-roun ded by a nuc lear m em b rane andm u ltip le ch rom o som es , as in hum ance lls). O th er m e tabo lic s tep s tha t oc -cu r in bac ter ia b u t n o t hum an s (eg ,syn th esis o f fo lic ac id fo r n uc leo -tid es ) a lso can b e inh ib ited se lec -tiv ely b y an tib io tic s .B ac te ric Id a l V ersusB ac te rlo s ta t lc P rope rt ies o fAnt ib iot icsA favo ra b le th erap eu tic ou tcom e fo l-low ing the adm in istra tion of a spe -
at Health Internetwork on July 29, 2008http://pedsinreview.aappublications.orgDownloaded from
http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/ -
7/30/2019 Antibiotics Mechanisms of Action - 1994
3/10
W E A K E N C E L L W A L L B YIN H IB IT IN G C R O S S -L IN K IN G O FP E P T I D O G L Y C A N
Pedi atr i cs i n Revi ew VoL 15 No. I i N ovember 1994 441
Icif ic antibiotic depends on multiplefactors, including those related to thebacteria (eg, resistance mechanisms),the antibiotic (eg, mechanism of ac-tion, ability to penetrate to the in-fected site, and spectrum of activity),and the host defenses (eg, phagocyto-sis, opsonization, complement pro-duction). W hen host defenses aremaximally effective, the contributionof the antibiotic may be less impor-tant. For example, a bacteriostaticagent (eg, chloramphenicol, erythro-mycin, clindamycin, tetracycline) thatslows or inhibits protein synthesismay be adequate when combinedwith the host s ability to opsonizeand phagocytize bacteria. In contrast,a patient whose host defenses are im-paired may require a bactericidalagent ( eg, penicillin, cephalosporin,aminoglycoside) that actually w ill killor lyse the bacteria. Bactericidalagents (T able 1) generally are used totreat bacterial endocarditis, meningi-tis, and osteomyelitis as well as anybacterial infections in neutropenicpatients.
A n t ib io t ic S u s c e p tib ilit yI f the concentration of an antibioticrequired to inhibit or kill the organ-ism can be achieved safely in the af-fected tissue or fluid, a micro-organism is considered sensitive to aparticular antibiotic. H owever, if theconcentration required is greater thanwhat can be achieved safely, the mi-croorganism is considered to be resis-tant to that antibiotic. M ost in vitrosensitivity tests are standardized onthe basis of drug concentrations thatcan be achieved safely in plasma andmay not take into account increaseddrug concentrations that may occur atspecif ic sites (eg, bladder) or any lo-cal conditions that may affect the ac-tivity of the antimicrobial agent.
Me c h a n is m s o f A c t io n o fA n t i b i o t i c sFor many antibiotics, the mechanismof action is not understood fully.However, it is known that antibioticscan act in the follow ing ways: 1) in-hibit cell wall synthesis, 2) alter thepermeability of the cell membrane,3) inhibit protein synthesis, and4) inhibit nucleic acid synthesis(Table 1).
Pe nicil lins a n d CephalosporinsPenicillins and cephalosporins (beta-lactam antibiotics) are among themost widely prescribed antibiotics be-cause of their safety profiles. The ba-sic structure of penicillin consists ofa five-member thiazolidine ring con-nected to a beta-lactam ring to whicha side chain is attached. In contrast,the cephalosporins have a six-mem-bered hydrothiazine ring connected tothe beta-lactam ring. An intact beta-lactam ring structure is an essentialrequirement for the biologic and anti-bacterial activity of both penicillinsand cephalosporins. N ew derivativesof the basic penicillin nuclei continueto be produced; each has unique ad-vantages. M odification of the variousside chains on these structures affectsthe specif ic antibacterial spectrum aswell as the pharmacokinetic profile ofthese drugs.
Beta-lactam antibiotics kill suscep-tible bacteria by interfering with cellwall synthesis. T hey are bactericidal,but only kill organisms undergoingactive cell wall synthesis. T he bio-synthesis of peptidoglycan in the cellwall occurs in three stages and in-volves about 30 different enzymes.Beta-lactam antibiotics inhibit trans-peptidases, the enzymes that catalyzethe final cross-linking step of pepti-dogl ycan sy nthesi s.
There also are receptors calledpenicillin binding proteins (PBPs) inthe bacterial cell membrane and cellwall for the beta-lactam antibiotics.Each bacterium has several types of
PBPs that vary in their affinity fordifferent penicillins and cephalospo-rins. Some PBPs are transpeptidasesresponsible for peptidoglycan cross-linking and necessary for bacterialshape; the function of others isunknown. I nhibition of PBPs causesabnormal cell shape, division, andeventual lysis. A ltering the PBPs isone mechanism by which bacteriacan develop resistance to penicillin.This resistance may be intrinsic be-cause of structural differences inPBPs or a previously sensitive strainmay acquire resistance follow ing amutation of PBPs. Resistance ofStr eptococcus pneumoni ae t o peni ci l-lin and cephalosporins, which hasbeen reported around the world aswell as in the U nited States, is due toalterations in PBPs (Table 2).
A ctivation of cell wall autolyticenzymes (ie, autolysins) is anotherfactor that is important in the degra-dation of the cell wall. The relation-ship between the inhibition of PBPactivity and the activation of autoly-sis is unclear and very complex. Tol-erance to penicillin occurs when theorganism is inhibited but not killedby an antibiotic that usually is bacte-ricidal. For example, the growth ofcertain tolerant strains of Staphylo-coccus aur eus can be arrested bybeta-lactam antibiotics, but autolyticenzymes are not activated.
Production of beta-lactamases, en-zymes that can cleave the beta-lactamring, is an important mechanism forthe inactivation of beta-lactam antibi-otics and development of resistanceby many bacteria (eg, S aur eus, N ei s-ser i a gonor r hoeae, Pseudomonas sp,B acter oi des fr agi l i s, and some enteric
at Health Internetwork on July 29, 2008http://pedsinreview.aappublications.orgDownloaded from
http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/ -
7/30/2019 Antibiotics Mechanisms of Action - 1994
4/10
442 Ped ia tric s in R eview VoL 15 No . 11 N ovember 1994
IT . IMECHAN IS M DRUGS ACT1 ON
W eaken bacter ial cell wall and cause cell death. In h ib it c ro ss- link in g of p ep tido g lycan P en ic illin s , ceph alo sporins B ac ter ic ida l. A ctiv ate au to ly tic enzym es (ie , au to ly sins). In h ib it o the r step s in pep tid og ly can syn th esis V ancom yc in B ac te ric ida l
In c rea se ce ll m em bran e pe rm eab ility. C ause leakage of cell con ten ts P o lym yx in NA
I nhibit protein synthesis. B ind to 5 05 ribosom e subun it C h lo ram ph en ico l B acte r io sta tic
E ry th rom yc in B acte r io sta ticC la rith rom yc in B acte r io sta ticC lin dam yc in B acte r io sta tic
. B ind to 3 05 ribosom e subun it Am in og ly co sides B acte r icid a lT e tracyc line s B acte r io sta tic
I nhibit nucleic acid synthesis. Inh ib it nuc leo tide syn th esis S u lfon am ides, tr im e thop rim B ac te rio sta tic. Inh ib it DNA -d ep en den t RNA polym erase R ifam pin B ac te ric ida l. Inh ib it D NA sup erco iling and DNA syn thesis Q u in o lon es B ac te ric ida l
* N ot e: B a ct er io st at ic agents m ay be bac ter ic id a l ag ains t som e o rganism s a t high concentration s.
DRUGS FO R WHICH RES IS TANCEORGAN IS M HAS B EEN REP ORTED RECOMMENDATiO NS
Strep to co ccu s pneum on iae #{149 }en icillin # {149}ondu ct o xac illin d isk su scep tib ility onIn te rm ed iate - lev el re sis tance is a ll iso la tes
in c rea sing #{149}f re sis tan t, check M IC s to p en ic illin ,H igh -leve l res is tan ce h as b een ce fo tax im e , ce f triaxo ne , vancom yin ,repo rted in va rious a rea s o r o the rs
w orldw ide an d is inc rea sing #{149}f sensitive , suscep tib le to a ll b eta -in the U nited S ta tes lac tam s
C luste rs o f ca se s m ay o ccu r (eg , #{1 49}f m en in g itis , trea t w ith v an com yc inch ildca re co n tac ts) PLU S th ird -gene ratio n ceph alo spo rin
#{149}ep ha lospo rin s O R ch lo ram phen ico l O R im ipen emT reatm en t failu re s h av e prom pted pend ing suscep tib ility te stin g
su scep tib ility te stingEnterococcus feca lis #{149 }m p icillin #{1 49}f invasiv e d isea se , ch eck M IC s an d treatEnterococcus faec ium # {149}ancom y in w ith am pic illin PLU S vancom yc in
R es is tan t s tra in s have been PLUS am inog lycoside (gen tam ic in )id en tified p en d ing suscep tib ility tes ting
Neisseria gonorrhoeae #{149 }en ic illina se -p ro duc ing s tra in s #{149 }en icillin o r d oxy cyc line a re n o tcomm on recom m ended em pir ic the rap ies
#{149}e tracyc line #{149}on ito r f luo roq u ino lone suscep tib ilityH ig h-lev el p la sm id -m ed ia ted pa tte rn and c lin ica l re sp onse
resis tan ce reported #{149}h ird -g en era tion cep ha losp orin s (eg ,#{149}lu o roqu ino lo nes ce ftr iax one ) still seem effectiv e
D ec reased su scep tib ility repo rted
at Health Internetwork on July 29, 2008http://pedsinreview.aappublications.orgDownloaded from
http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/ -
7/30/2019 Antibiotics Mechanisms of Action - 1994
5/10
Ped iatrics in Rev iew V oL iS No . ii No vem ber 1994 44 3
Gram-negati ve baci l l i ). T he inf orma-ti on f or producing beta- lactamasescan be coded in chromosomes or ona plasm id. T he beta-lactamases canbe consti tuti ve (produced al l thetime) or inducible (only produced atcertai n ti mes).
In the case of inducible resi stance,the organism ini ti al l y w i l l be suscep-ti ble to a certain antibioti c, but af tera short per iod of therapy , the organ-i sm w i l l become resistant because ofthe beta- lactamases that have beeninduced. Frequentl y , thi s i s signaledby only l im i ted improvement or cl i ni -cal deter iorati on of the patient af teran ini ti al improvement. Induciblebeta-lactamase production i s a partic-ular problem w i th some Gram-negati v e bacter ia (eg, Pseudomonas ,Enterobac ter, C itro bac ter, A c ine to -b ac ter , S erra tia sp) treated w i thbroad-spectr um cephal ospor ins.
B eta- lactamase production by bac-ter ia can be inhibi ted by the addi ti onof certain chem ical structures that aresim i lar i n structure to penici l l i n (eg,clavulanic acid, sulbactam). The in-hibi tors bind strongly to the beta-lac-tamases and prevent the subsequentinacti vati on of the penici l l i n nucleus.
Penici l l i ns have good acti v i tyagainst G ram-posi ti ve bacter ia andoral anaerobes and variable acti v i tyagainst G ram -negati v e baci l l i . T heyare the treatment of choice for syphi -l is, l eptospi rosi s, or Listeria infec-tions. Penici l l i ns general ly areclassi f i ed according to thei r spectrumof acti v i ty as determ ined by changesin thei r side chains relati ve to peni -ci l l i n: penici l l inase-resi stant penici l l i n(eg, methi ci l l i n, nafci l l i n, oxaci l l i n,cloxaci l l i n, and dicloxaci l l i n) ; am ino-penici l l i ns (am pici l l i n, amox ici l l i n) ;antipseudomonal penici l l i ns (eg, car-benici l l i n, ti carci l l i n, and azloci l l i n);and ex tended-spectrum penici l l i ns(eg, m ezl oci ll in, pi peraci ll in) .
The cephalosporins are div idedinto generations based on thei r an-ti mi crobi al acti vi ty . Fi rst-generati oncephalosporins (eg, cephalex in, cef a-drox i l , and cef azol i n) have good ac-ti v i ty against Gram-posi ti v e bacteria,i nc lu di ng p en ic il l in ase- pr od uc in g Saureus , group A beta-hem ol yti cstreptococci , group B streptococci ,and S p ne um o ni ae , and modest acti v -i ty against some Gram -negati v e or-gani sm s. T he second- generati on
cephalosporins (eg, cefaclor, cef urox-ime, cef urox ime axeti l , cefprozi l , cef -amandole, cefox i ti n, and cef otetan)retain acti v i ty against Gram-posi ti v eorganisms but have more acti v i tyagainst Gram-negati ve organisms, in-cluding most strains of Haemoph i lu sin f luenzae and some strains of enteri cbacter ia. The thi rd-generation cepha-lospor ins (eg, cef ix im e, cefoperazone,cefotax ime, cefpodox ime proxeti l ,cef tazidime, cef ti zox ime, and cef tr i ax -one) are more acti v e against G ram-negati ve organisms (includingEnterobac ter iaceae and beta- lac tamase -producing strains of H in fiu en za e,M oraxe lla ca ta rrha lL i, and N gonor -rhoeae), but they are less acti ve thanf i rst-generation cephalosporins againstG ram-posi ti v e organism s. Cef tazidim ei s acti ve agai nst Ps eudomona s sp andhas superior central nervous systempenetrati on compared w ith am inogly co-sides. Cef tri axone has a prolongedhal f - l i f e that al l ow s f or once-a-daydosing. N one of the cephalosporins i sef f ecti v e against anaerobes, entero-cocci , or L m o no c yt og en es .
B ecause of the structural sim i lar i tybetw een penici l l i n and f i rst- and sec-ond-generation cephalosporins, pa-ti ents may m ani fest cross-reacti v i tyw hen a member of the other class i sadm inistered. Immunologic studiesdem onstrate a 20% cross-reacti v i ty ;more recent cl i ni cal studies indicate af requency as low as 1% . Cross-reac-ti v i ty betw een penici l l i ns and cepha-losporins general l y occurs in about8% of patients w ho have a history ofan al l ergi c reaction to penici l l i n. A l -though side chains do not seem to bea f actor in al l ergi c reactions to peni -ci l l i ns, they may be important incephalosporin al l ergy . The patientw ho is al l ergi c to cephalosporins mayhave an al lergy to the beta- lactamring, the bulk y side chain, or both.T he ri sk of al l ergi c reaction w i th thenew er thi rd-generation cephalosporinsi s not known.WEAKEN C E L L WA L L B YIN HIB IT IN G P E P F ID OG LY CA NSYNTHESISVa n c o my c inV ancomycin i s a complex and unu-sual tri cycl i c gl ycopeptide that inhib-i ts cel l synthesis in sensi ti ve bacter iaby binding tightl y to precursor sub-uni ts of the cel l w al l and preventing
Ithei r i ncorporati on into the grow ingpeptidoglycan. The drug is rapidl ybacter i cidal f or di v iding m icroor-ganisms. B ecause vancomycin maybe only bacter iostati c f or some en-terococci , an am inoglycoside isadded to vancomycin therapy in se-ri ous inf ecti ons known to be causedby thi s organism (eg, infecti ve en-docarditis).
Earl y preparations of vancomycincontained impuri ties that probablycontri buted signi f i cantl y to the tox i c-i ty associated w i th i ts earl y use; thi sno longer i s a problem. I n recentyears, there has been renew ed interesti n the use of vancomycin for severalreasons. Fi rst, i t i s structural l y unre-lated to other antibioti cs, so i t i s use-f ul i n the patient w ho is al l ergi c topenici l l i n and cephalosporins. Sec-ond, i t i s acti ve primari l y againstG ram -posi ti ve bacteria and f orms themainstay of therapy for the treatmentof i nf ecti ons caused by methici l l i n-resistant S aureu s (M R S A ), coag u -l ase-negati ve staphy lococci that areresi stant to other penici l l i ns, and Spneumoniae strains that are resi stantto penici l l i n and cephalosporins (T a-ble 2). V ancomycin i s an importantantibioti c for use in immunocom -prom ised patients who have ev i -dence of catheter-related inf ecti ons.B ecause oral vancomycin i s ab-sorbed poorl y , high concentrati onsoccur in the stool . T hus, i t can beused as a more expensive al ternati veto metronidazole f or the treatment ofC lo strid ium diffic ile i nfecti ons; me-tronidazole i s not approved by theFood and D rug A dm inistrati on f oruse in chi l dren.
R ep or ts o f v ancom yci n- resi st antstrains of enterococci and S aureushave caused ex treme concern in themedical communi ty . Prudent use ofthi s drug is essential to m inim ize thedevelopment of further resi stance.M easurement of serum levels of van-comycin i s recommended to avoidpotential ototox i ci ty and nephrotox i c-i ty . The incidence of both tox i ci ti esi s increased w hen vancomycin i s ad-m ini stered simul taneously w i th anaminoglycoside.IN C R E A S E C E L L PERMEAB IL I TYPolymyx in BPolymyx in B is a basic peptide elab-orated by various strains of Bac il lus
at Health Internetwork on July 29, 2008http://pedsinreview.aappublications.orgDownloaded from
http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/ -
7/30/2019 Antibiotics Mechanisms of Action - 1994
6/10
G ram -positiv e an d G ram -negativ e b ac teria d if f e r in th e ir ce llw all s truc tu res; th e pep tid og ly can lay er is th ick in G ram -positiv eo rgan ism s and th in in G ram -negativ e o rgan ism s.
444 Pedi atr i cs i n Revi ew V ol . 15 No. 11 November 1994
sp . I t is a surf ace -ac tiv e ag en t con-tam ing both lipophilic and lipophob icgroups w ith in the m o lecu le that in ter-ac t strong ly w ith phospholip id s andd isrup t the in teg rity o f cell m em -branes. T h e perm eability o f the bac-terial m em brane changes im mediate lyaf ter contact w ith th e d rug . Poly -m y x in B is p rescrib ed p rim arily f orophthalm ic, o tic , or to p ical use incom binatio n w ith a v arie ty o f o thercom pound s (eg , b ac itrac in , neom yc in ,hydrocor t isone).IN H IB IT P R O T E IN S Y N T H E S ISR ibosom es are the site o f p ro teinsy n thesis in bo th bacterial and euk ar-y o tic ce lls , b u t bac terial and eu k ar-y o tic ribo som es d if f e r in bo th siz eand ch em ical com pos ition . B ac terialrib osom es are 70S in siz e (w ith 50Sand 30S subunits) com pared w ith80S (w ith 60S and 40S subunits) ineuk ary o tic ce lls . T hus, an tib io tic s that
ph en ico l usually is caused by ap lasm id acqu ired b y conjugatio n .O ther p lasm id s m ay tran sf er resis-tance to m u ltip le an tib io tics (eg ,ch lo ram phenico l, te tracy c lin e, andbeta-lac tam s). O nce acety lated , chor-am phenico l cannot attach to thebacterial riboso me .U se of ch loram phenico l m u st belim ited to in f ec tions fo r w hich th ebene f its o f th e d rug outw eigh the risko f th e poten tial tox ic itie s (eg , rev ersi-b le , dose -re lated bone m arrow sup-press ion , po ten tially f atal id iosy n-cratic ap las tic anem ia, and g raybaby sy ndrom e). W hen antim icro-b ials that hav e equiv alen t ac tiv ity bu tare poten tially les s to x ic are av aila-b le, they should b e used . In additio n ,it is necessary to m on itor serum lev -e ls w hen treatin g a patien t w ith ch lo-ramphenico l .C hloram phen ico l is a broad-spec-trum antib io tic that is ac tiv e against
R esistance to ery throm y cin can oc-cur by at least three p lasm id -m ed i-ated m echan ism s: f ailure o f the drugto p en etrate the cell, m odif icatio n o fthe targe t site s on the 505 ribo som eso that the drug fails to b ind , andproduc tion o f an esterase by the bac-teria to h y dro ly z e the d rug .G ram -positiv e bac teria accum ulateabout 100 tim es m ore ery throm y cinth an do G ram -negativ e organism s.A lth ough ery throm y cin generally isclassif ied as a bac teriostatic ag ent, itcan hav e bacteric id al ac tiv ity again sta sm all num ber o f rap id ly d iv id ingbac teria, especially in an alk alineenv ironment.
In patien ts w ho hav e p en ic illin al-lergy , ery th rom y c in is an ef f ec tiv e al-te rnativ e agent agains t G ram -positiv ebac teria such as group A s trep to-cocc i , S p n eu m on i a e, an d S a ur eu s.H ow ev er, the em ergence o f res istan tstrains m u st b e m on itored . E ry thro-m yc in also has good an tim icrob ialac tiv ity agains t Bor detel la per tussi s,B o rre l ia sp , Campylobacter sp , C h la -mydi a tr achomati s, C pneumoni ae(T W A R strain), M ycopl asma pneu-moniae, an d L egi onel la pneumophi la.Clanthromyc in
af f ec t pro te in sy n th es is can hav e ase lec tiv e e f f ec t o n sen sitiv e bac teriaw ithou t af f ec ting hum an ce lls .Ch lo r a mp h e n ic o lCh loram phenico l, a n itro benz enem o iety , pene trates bac terial cells byf ac ilitated d if f u sion and bind s rev ersi-b ly to th e bac terial 505 ribosom al sub-un it. T his drug (lik e te tracy clin ese f f ec t o n th e 305 ribosom e subunit)b lock s th e b ind ing of the am inoacy ltransf er R N A (tR N A ) to th e accep torsite on the ribosom e. C hlo ram pheni-co l h as less o f an e f f ect o n p ro te insy n th es is in eu k ary o tic cells than inbacterial cells . C hloram phen ico l isprim arily a bac terio static agent, bu t itm ay be bac teric idal to certain spec ies(eg , H i nfl uenzae, S pneumoni ae, Nmeningiditis).
M echanism s of res istan ce to ch lor-am phen ico l inc lud e productio n of anace ty ltransf erase by th e bac teria thatinac tiv ates ch lo ram phenico l and in-ab ility o f ch loram phen ico l to en terse lected bac teria. R esistance o fG ram -negativ e bacteria to ch lo ram -
m any G ram -po sitiv e and -negativ ebac teria as w ell as against rick e ttsiae .In particu lar, it is e f f ectiv e again stm ost anaerobic bac teria, inc lud ing B
fra g i l is , and the m ajo rity o f Salmo-nella sp and H i nf luenza e strains. I tis a recom m ended alternativ e therapyf or in f ec tion s cau sed by Brucella an dPasteurella sp as w e ll as fo r R ock yM ountain spo tted f ev er. C hloram -phenico l has b een e f f ec tiv e in som e Spneumoniae in f ec tions resistan t topen ic illins and cephalo spo rins .
Ery thromyc inEry throm y c in has a m acro lid e struc -ture com po sed o f a large 13 -carbonring to w hich tw o sugars are attachedby gly co sid ic link ag es. E ry throm ycinand o ther m acro lides inh ib it pro te insy n thesis by rev ers ib ly b ind ing to the50S ribo som e subunit o f sensitiv em icroorganism s. I t b lock s the tran slo-cation s tep in pro te in sy n thesis byprev en ting the re lease o f the tR N Afrom the accep to r to the donor siteon the rib osom e af ter the p ep tidebond is fo rm ed .
C larith rom y c in , recen tly appro v ed f orped iatric use , d if f e rs chem ically f romery throm y cin by hav ing a m ethy lsub stitu tion on the m acro lide ring . Itssp ec trum of ac tiv ity is sim ilar to thato f ery th rom y c in ex cep t f or enhancedH i nf luenzae ac tiv ity (in c lu d ing be ta-lactam ase-produc ing strains) , and itslonger half -lif e allow s fo r tw ice -a-daydosin g . C larithrom y c in and its ac tiv em etabo lite pene trate w e ll in to bodyf lu id s and tissues (eg , lung tissue ,to nsils) , resu lting in in trace llu lar andtissue concen tration s th at are h igherthan serum concentrations. G astro in-tes tinal s ide e f f ects o ccur less f re-quen tly in patien ts rece iv ingclarithrom y cin (8% to 16% ) than inthose treated w ith ery th rom y c in (20%to 40% ). B ecause it reaches ex ce llen tlev els in serum , alv eo li, m acrophages ,and lung tissue , o ther im portan t u seso f c larith rom y c in w ill b e in the ther-ap y o f M ycobacter i um avi um an d Cpnewnoniae (TW A R ) in f ec tion s.Cl in d a my c inC lindam y c in , a deriv ativ e o f anam ino ac id attached to a su lfu r-con-
at Health Internetwork on July 29, 2008http://pedsinreview.aappublications.orgDownloaded from
http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/ -
7/30/2019 Antibiotics Mechanisms of Action - 1994
7/10
In patien ts w ho hav e pen ic illin alle rgy , e ry th rom y c in is ane f f e c tiv e alte rnativ e agen t.
Pedi atr i cs i n Revi ew VoL 15 N o. i i N ovember 1994 445
I tam ing sugar, has rep laced its paren td rug lin com y c in in c lin ical use . C lin -dam y c in inh ib its pro te in sy n thesis byrev ersib ly b ind ing to th e 505 rib o-som e subunit o f sensitiv e m icrorgan-ism s . A lthough bactericid al fo r som eo rgan ism s, c lindam y c in generally isb ac terio static . M echan ism s o f resis-tance are sim ilar to th ose outlin ed f orery thromyc in .
C lindam y c in is ac tiv e againstp neum ococci and group A strep to-cocc i. I t h as ex ce llen t ac tiv ity againstS aur eus and m any anaerob ic bacte -ri a, p ar ti cu l ar ly B f rag il is. Clinda-m y c in is an im portan t an tib io tic f orth e treatm ent o f in tra-abdom inal orp elv ic in f ec tion s and as an alterna-tiv e th erapy in patien ts w ho are al-le rg ic to p en icillin . B ac terial s trainsth at are resistan t to c lindam y c in gen-erally are resistan t to ery th rom yc in .C lindam y c in p en etrates w e ll in tom ost bod y f lu id s, inc lud ing sputum ,p leural f lu id , and bone . H ow ev er, itshould not be used f or cen tral nerv -ous sy s tem in f ec tio ns becau se o f itsp oo r p ene tration in to cereb ro sp inalf lu id .
the inner cy to p lasm ic m em brane canbe reduced by acid ic or anaerobiccond itions , su ch as tho se presen t inan ab scess. Inac tiv ation b y m icrob ialenz ym es is an im portan t cau se o f theacquired resistan ce to am inogly co-sides that occurs f requently . T h e ge-ne tic in f orm ation f or th ese enz ym esis acqu ired p rim arily by conjugatio nand the tran sf er o f D N A as plasm id so r resistance f ac tors. S uch plasm id sare w idespread and m ay dissem inateresistance to o ther antib io tic s sim ulta-n eously . A m ik ac in m ay be less v u l-n erab le to these inactiv atin g en z y m esthan k anam y c in , gen tim ic in , and to-bram y c in becau se o f pro tec tiv e m o-lecu lar side chain s.
T h e an tibac terial activ ity o f am i-nogly co sides is d irec ted prim arilyagain st aerob ic G ram -negativ e bac illi;there is little ac tiv ity again st anaer-obes or G ram -positiv e bac teria.S trep tom y c in has b een used in th e
outer m em brane of bac teria. T hen itis transported in to the inner cy top las-m ic m em branes w here it is boundm ain ly to the 30S subunits o f th ebac terial ribosom es. T he tetracy c linesinh ib it pro te in sy n thesis b y b lo ck ingam inoacy l tR N A f rom enterin g theaccep tor site on the m R N A ribosom ecom p lex . T etracy clin es selec tiv e ac-tion on bac terial cells is b ased on itsgreatly in creased uptak e in su scep ti-b le bacterial ce lls com pared w ithhum an ce lls; the host cells lack theac tiv e transport sy stem presen t inbacteria.
R esistance to the te tracy c lines f re -qu en tly is m ediated by p lasm ids andis an indu cib le trait; that is , the bac-teria becom e res istan t fo llow ing ex -po sure to the drug . A num ber o ftran sf erab le resistance d eterm inantsf or te tracy clin e hav e been id en tif ied .M icrorganism s that dev e lop resis -tance to one te tracy c line u sually are
A minog ly c o s id e sT he am inog ly cosides (eg , am ik ac in ,gen tam icin , tobram y c in , and strep to -m y c in) contain am ino sugars link edto an am ino cy clito l ring b y gly co-sid ic bonds. A minogly cos ides d if f usethrough channels f orm ed by porinp ro tein s in the outer m em brane ofG ram -n egativ e bac teria and in to thep erip lasm ic space (Figure). T here theam inogly co sides b ind irrev ersib ly topoly som es, especially th e 305 rib oso -m al subunits , and prev en t pro te insy n thesis by inh ib iting th e initiationcom plex . In add ition , am inogly co -sid es cau se m isreading of th e m es-senger R N A (m R N A ) tem p late,w h ich resu lts in the incorporation o fin co rrect am ino ac ids in to the grow -in g pro te in chain . A s a resu lt, them em brane is dam aged and the bac te -ria d ie. U n lik e the o ther in h ib ito rs o fm icrob ial pro te in sy n th esis, the am i-nog ly cosides are bactericid al rathert ha n b ac te ri os ta ti c.
B ac teria m ay be res is tan t to th eantim icrob ial ac tiv ity o f am inog ly co-sides if th e d rug fails to pene trate thece ll, h as a low af f in ity f or the bac te -rial ribosom e , or is inactiv ated bym icrobial enz ym es . T ran sport acro ss
m ultip le drug therapy of resistan tpu lm onary tu bercu lo sis or d is sem i-nated m y cobacterial d isease. G enta-m ic in has been u sed in com b inationw ith o ther antib io tics fo r its sy n erg is-tic e f f ects again st certain bac teria (eg ,w ith pen ic illin agains t en tero cocci,w ith nafc illin against S a ur eu s, wi thp en ic illin against group B strep to-co cc i, w ith am pic illin against L mono-cytogenes, and w ith o ther drugsef f ec tiv e again st Pseudomonas sp).T he c lin ical use f u lness o f am inogly -co sides is lim ited by the po ten tial f oro to to x ic ity and nephro to x ic ity , poorcen tral n erv ous sy stem pene tration ,and the n eed f or m on itorin g serumleve ls .TetracyclineT he stru ctu re o f te tracy c lin e consistso f f o ur cy clic rin gs w ith d if f eren tsub stituen ts in three reg ions ; the lat-te r subs titu tions resu lt in d if f e ren tpharm acolog ic properties bu t s im ilaran tibac terial ac tiv ity . In itially , the te t-racy c line m oie ty passiv ely d if f usesth rough the po rn p ro te in s in th e
resistan t to th e congeners as w e ll.H igh-lev el p lasm id res istan ce to te tra-cy c line has in creased nationallyam ong strain s o f N g on or r ho ea e;consequently , m ono therapy w ith te t-racy c line o r dox y cy c line no longer isrecom m ended to treat a patien t w hohas both gono rrhea and ch iam y dialin f ec tio ns (T ab le 2).
T he te tracy c lines hav e bac terio -static ac tiv ity agains t a v ariety o fG ram -po sitiv e and G ram -negativ ebac teria. T etracy clin es are a recom -m ended treatm en t for early L ym ed isease , R o ck y M oun tain spo ttedf ev er, and in f ec tio ns caused b y Mpneumoni ae, C tr achomati s ( inc lud-ing p e lv ic in f lam m ato ry d isease ), andC p neu mo ni a e (TW A R strain ).
B ecause o f its in creased lipophilicp ropertie s, d ox y cy clin e attains h ighercen tral nerv ou s sy s tem concentrationsthan o ther te tracy c lines, w hich m aybe im portan t in th e treatm ent o f earlyL ym e disease . T e tracy c lines are no tg iv en routine ly to ch ild ren y oungerthan 9 y ears o f ag e becau se o f tox ic -ity to tee th and bones. H ow ev er, cx -
at Health Internetwork on July 29, 2008http://pedsinreview.aappublications.orgDownloaded from
http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/ -
7/30/2019 Antibiotics Mechanisms of Action - 1994
8/10
T he c lin ical u se f u lness o f am inog ly co sides is lim ited by thep o ten tial f o r o to tox ic ity and neph ro to x ic ity , poor c en tral ne rv oussy s tem pene tration , and the need fo r m on ito ring serum lev e ls .
446 Pedi atr i cs i n Revi ew VoL 15 N o. 11 N ovember 1994
I Icep tion s hav e been m ade to treaty ounger ch ild ren w ho hav e R ock yM ountain spo tted f ev er.
I N H I B I T NUCL E I C AC I DS Y N THE S I S
SulfonamidesS u lfo nam ide is a generic nam e fo rthe deriv ativ es o f p ara-am inobenz ene-su lf onam id e . S u lf onam id es are struc -tural analogs and com petitiv e inh ib i-tors o f th e bac terial en z y m e d ih y d rop -teroate sy n thase, w hich is responsib lef or in co rp orating para-am in oben zo icacid (PA BA ) in to d ihy d roptero icacid , th e p recursor o f fo lic acid . T h isresu lts in a decreased pool o f b ac te -rial nu cleo tides, w hich are th e build -ing b lock s f or DN A sy n th esis.M am m alian ce lls are not af f ec ted byth is m echanism because they requirep re fo rm ed f o lic ac id f rom th eir d ie t.
S ulf onam id es are bac terio staticag ents; thus, the f inal erad ication o fthe in f ec tion depend s on the ce llu larand hum oral de f ense m echanism s ofthe ho st.
S u lfo nam ides hav e a w id e range ofan tim icrob ial ac tiv ity agains t G ram -positiv e and G ram -n egativ e bac teria.T hey w ere th e f irst e f f ectiv e chem o-th erapeutic ag en ts used to cure bac te-rial d iseases (eg , pu erperal sep sis andm en ingo co ccal in f ectio ns) . S u lf ona-m ides f requently are used as chem o-p rophy lax is and also are recom -m ended f or the treatm ent o f Toxo-plasma in fec t ions .
Tnmethopr imT rim e thoprim , an antim e tabolite thataf f ec ts fo lic ac id sy n thesis, is ah igh ly se lectiv e in h ib ito r o f d ih y dro-fo late redu ctase in low er organism s.It prev en ts the reduc tion o f d ihy d ro -fo late to te trah y dro f o late , ano thercritical p recursor in purine sy n th esis .B y com bin ing trim e thoprim w ith su l-f am ethox az o le (T M P-SM Z ), tw o se-qu ential steps o f purine sy n thesis are
d isrup ted sy nerg istically and less re -s istan ce dev elo ps. T M P-SM Z is usedw ide ly f or th e treatm ent o f urinarytract in f ec tio ns, resp iratory in f ec tions,s inusitu s, o titis m ed ia, and gastro in-testin al in f ec tio ns (eg , salm one llosis,sh ige llo sis, trav e lers d iarrhea). TM P-SM Z also is the dr ug of choice forthe treatm ent and prophy lax is o fP neumocysti s car i ni i in fec t ions .
R i famp inR if am pin inh ib its DN A -d ep endentR N A poly m erase at the B subunit o fth is enz ym e , w hich p rev en ts chain in-itiation bu t no t e longatio n in R N Asy nthesis. R ifam p in is bactericid al fo rbo th in trace llu lar and ex tracellu larm icroorgan ism s. R esistan t strain s o fbac teria hav e altered R N A po lym er-ase that is no t in h ib ited by rif am p in .M icroo rgan ism s m ay dev e lop res is -tan ce to rif am p in rapid ly in v itro as a
one-s tep m utation ; th is also occurs inv iv o . Fo r th is reason , rif am p in shouldnot be adm in istered alone , ex cep t f orshort-te rm chem oprophy lax is (eg , in -f ectio ns cau sed by N m en in gi di ti s orH i nf lu en zae ty p e b ). R if am pin isused in com b ination w ith o therag en ts to treat tub ercu losis and per-sisten t group A strep tococcal orstaphy lococcal in f ec tions .
Quino lonesN alid ix ic ac id has been av ailab le forthe treatm ent o f u rinary tract in f ec -tions f or decades, b u t it h as lim iteduse f u lness becau se bacterial resis-tance d ev e lo ps rap id ly . N ew er sy n-the tic f luo roquino lon es (eg , n orf iox -acm , cip ro f lox ac in , eno x acin , f lerox a-cm , lom ef lo x acin , and of lox ac in)hav e broad-spec trum antim icrob ialac tiv ity and are a therapeutic ad -v an ce . T he ir u se in p ed iatric s hasb een lim ited by the poten tial risk o farth ropathy that has b een docum entedin sev eral sp ec ies o f im m ature ani-mals .
T h e quino lon es b ind to the A sub-
un its o f D N A gy rase , w h ich are re -spon sib le fo r cu ttin g DN A strand s,th us prev en ting sup erco iling , unrav e l-in g the DN A , and halting DN A rep li-cation . M ost qu ino lones are no t asac tiv e agains t G ram -pos itiv e bac teriaas they are agains t G ram -negativ ebac teria; th ey are only e f f ec tiv eagainst strep tococc i and enteroco cc iat lev e ls that can be reached in th eurine.
T he em ergence o f resistance tof lu oroqu ino lones has been p rob lem -atic fo r M R SA , m eth icillin -sens itiv eS aur eus, P aer ugi nosa, and som eSerratia in f ec tions. D ecreased suscep-tib ility o f N g on or r ho ea e to f lu oro -qu ino lones recen tly has been reported(T ab le 2 ). I t is be liev ed that w ide-spread and o f ten ind iscrim inate useo f f luo roquino lones has con tribu tedto th is resistance prob lem . H ow ev er,w hen u sed in se lec ted patien ts, th equ ino lones can be lif e -sav ing , m ayallow the patien t to av o id o r sho rtenho sp italiz atio n , and can be v ery cos t-e f fec t ive .
Fluo roquino lon es hav e been usedto treat patien ts w ho hav e py e lon e-ph ritis o r recurren t urinary trac t in -f ec tion s, prostatitis , gonorrh ea (sin g ledose ) and chlam y dia (7-day course)in f ectio ns, m alignant ex ternal o titis ,o steom y elitis cau sed by G ram -n ega-tiv e bacteria, resp iratory in f ec tion sinc lud ing ex acerbations o f cy stic f i-brosis, and gas tro in testinal in f ec tion s(eg , Shi gel l a, Sal monel l a, C ampyl o-bacter in f ec tions and trav e lers d iar-rhea).
Q uino lones are not approv ed bythe Food and D rug A dm in istrationfo r use in patien ts y ounger than 18y ears o f age o r in p regnant o r nu rs-ing w om en . C h ildren w ho hav e cy s-tic f ib ro sis and are y ounger than 18y ears o ld hav e b een treated w ithqu ino lones w ith out ad v erse e f f ec tsbecau se th e b en ef its w ere b eliev ed tooutw eigh the risk s.I m p l i c a t i o n sU nderstanding th e m any dif f e ren tm echanism s of ac tion f or av ailab lean tib io tic s m ay he lp practitio nersm ak e be tte r clin ical decis ions regard -ing th e u se o f an tib io tics . A lth oughthe increasing em ergence o f an tib i-o tic -res istan t p athogen s is alarm ing ,there are steps th at each phy sic iancan tak e to s low th is trend (T able 3).
at Health Internetwork on July 29, 2008http://pedsinreview.aappublications.orgDownloaded from
http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/ -
7/30/2019 Antibiotics Mechanisms of Action - 1994
9/10
P ed iatr ics in Review VoL 15 N o. ii N ovem ber 1994 44 7
IA dmittedly , some of these recom-mendatio ns are not easy o r popular.How ever, the alternative may be theemerg ence o f resistant bac teria thatcannot be treated w ith an y o f ourm any antibio tic s.
SUGGESTED READ INGGeneralBrook s O F , Bu te l JS , O rns ton LN , C t a l.
M e dic al M ic ro bio lo gy. No rwa lk , C onn :A pp le ton a nd Lange ; 1 991
C ra ft JC , S iepm an N . O verv iew o f the sa fe typ ro file o f c la rith rom yc in susp en s io n inp ed ia tric p atie nts . P ed ia tr I n fec t Di s J .1993;12 :S142 - .S147
O ilm an AG , Ra il 1 W , N ie s AS , e t a l. Th ePharm acolo gical B asis o f The rap eu tics .N ew Y ork , N Y : P erg am on P ress ; 1 99 0
Ku ce rs A , Benne tt N . Th e U se o f A nti bio tic s,4 th e d . P h ila de lph ia , P en n : JB L ipp inco ttC om pan y; 19 87
M u ll iga n M i, C obbs CO . Ba cte rio s ta tic ve rsusb ac te ric id al a ctiv ity . In fe ct D is Clin Nor thAm . 1989 ;3 :389 -397Pe tz LD . Im muno lo g ic a l re ac tion s betw eenpen ic illin s and ce pha lo sp o rin s : a re v iew . JIn fec t D is. 1978 ;137 ( s upp l ) :S74 -S79
R ee se RE , B e tts R F . H andbook of An tib io tics,2nd ed . B oston , M a ss : L ittle B rown andC om pany; 19 93
Rodriequ ez W i, W ie de rm ann V L . R o le o fn ew er o ra l cep ha lospo rin s, flu oroqu in olo nesa nd m acro lid es in the tre a tm en t o f p ed ia tricin fec tio ns . In : A ro no ff S C , e d . Advan ce s inPed iatric In fe ctious D isea ses , vo l 9 . S t.L ou is , M o : CV M osby ; 1 99 4 :1 25 -15 1
AntIbiot ic - res is tant PathogensB re im an R F , B u t le r JC , T eno ve r FC , E llio tt
JA , F ac k lam RR . Em ergence o f d rug -res is ta n t p ne um ococca l in fec t ion s in th e U S .J AMA . 1994 ;271 :1831-1835
C en te rs fo r D is ea se Con tro l. D ec re ase dsu sce p t ib il ity o f N eisse ria g on orrh oe ae toflu o ro qu ino lon es : O h io a nd Hawa ii, 1 99 2 -1 9 9 4 . MMWR . 1994 ;43 :325 -327
L egg ia d ro R J. Pe n ic illin a nd cep ha lospo rin -res is tant Str ep toco ccu s pn eu mon ia e: anem e rg ing m ic rob ia l th rea t. Pediatr ics . 1994 ;93 :500 -503
Sloas MM , Ba rre tt FF , Chesney P J, e t a t.C ep ha losp o r in trea tm en t fa ilu re in pen ic i llin -a n d c e p ha lo s p o ri n -r e s is t a n t S t r e p t o c o c c u spneumoniae men ing i t i s . Pedia tr In fect D is J .1 99 2; ! 1 :6 62 -6 66
Sm ith A L . An tib io tic re s is tan ce in pe d ia tricpa thogens . I n f e c t D is C lin N orth Am . 1992 ;6 :177 -195
Tab le 3 . W ha t P rac tftlo ne rs C an D o To Um ft th eEme rgenc e o f A n tib io tlc res ls tan t P a thogens
#{149}ash hands thor oughly to avoid spreading r esistant or ganisms to otherpatients.
# { 1 4 9 }top and think. Is this a bac terial disease and is an antibio tic needed?# { 1 4 9 }ducate your patients that v iral illnesse s do no t respond to antibio tics .# { 1 4 9 }lw ays use the narrow es t-spec trum antibio tic possible.# { 1 4 9 }ry to lim it the empiric use o f broad-spec trum ag ents.# { 1 4 9 }tay informed about your hospitals antibio tic resis tance patterns.# { 1 4 9 }ecognize that ho spitaiw ide antibio tic contro l prog rams may be
implemented in some cases to lim it access to certain antibio tic s .
ASS i SO JU Professor of P edia trics, D ivision sof Pedia tric In fe ctious D isease s and GeneralPedia tr ics , U n iver s ity of Ro ch este r , Ro ch ester ,NY .P rivate P ra ctic e, P edia tr ic In fec tiou sDiseases an d A lle rgy , B e llev ile , N J .
at Health Internetwork on July 29, 2008http://pedsinreview.aappublications.orgDownloaded from
http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/ -
7/30/2019 Antibiotics Mechanisms of Action - 1994
10/10
DOI:10.1542/pir.15-11-4401994;15;440-447Pediatr. Rev.
Kathleen A. Woodin and Susan H. MorrisonBACK TO BASICS: Antibiotics: Mechanisms of Action
& ServicesUpdated Information
http://pedsinreview.aappublications.orgincluding high-resolution figures, can be found at:
Permissions & Licensing
http://pedsinreview.aappublications.org/misc/Permissions.shtmlits entirety can be found online at:Information about reproducing this article in parts (figures, tables) or in
Reprintshttp://pedsinreview.aappublications.org/misc/reprints.shtml
Information about ordering reprints can be found online:
at Health Internetwork on July 29, 2008http://pedsinreview.aappublications.orgDownloaded from
http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/misc/Permissions.shtmlhttp://pedsinreview.aappublications.org/misc/Permissions.shtmlhttp://pedsinreview.aappublications.org/misc/reprints.shtmlhttp://pedsinreview.aappublications.org/misc/reprints.shtmlhttp://pedsinreview.aappublications.org/misc/reprints.shtmlhttp://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/misc/reprints.shtmlhttp://pedsinreview.aappublications.org/misc/Permissions.shtmlhttp://pedsinreview.aappublications.org/