Antaabuse med
1
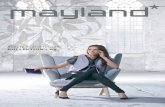
TABLE 17-2 DISULFIRAM ADVERSE EFFECTS: ACETALDEHYDE SYNDROME BODY SYSTEM AFFECTED RESULT Cardiovascular Vasodilation over the entire body, hypotension, orthostatic syncope, chest pain Central nervous Intense throbbing of the head and neck leading to a pulsating headache, sweating, marked uneasi- ness, weakness, vertigo, blurred vision, confusion Gastrointestinal Nausea, copious vomiting, thirst Respiratory Difficulty breathing
-
Upload
subbie-outlier -
Category
Documents
-
view
12 -
download
0
description
Antaabuse med
Transcript of Antaabuse med

288 CHAPTER 17 Substance Abuse
When consumed on a regular basis in large quantities, etha-nol produces a constellation of dose-related negative effects such as alcoholic hepatitis or its progression to cirrhosis. Teratogenic effects can be devastating and are caused by the direct action of ethanol, which inhibits embryonic cellular proliferation early in gestation. This often results in a condition known as fetal alco-hol syndrome, which is characterized by craniofacial abnormali-ties, CNS dysfunction, and both prenatal and postnatal growth retardation in the infant. Pregnant women need to be strongly advised not to consume alcohol during pregnancy, and appro-priate treatment and counseling need to be arranged for preg-nant women addicted to alcohol or any other drug of abuse.
Interactions Alcohol can intensify the sedative effects of any medications that work in the CNS (e.g., sedative-hypnotics, benzodiazepines, antidepressants, antipsychotics, opioids). It can interact with the antibiotic metronidazole, causing a disulfi ram reaction. Alcohol can also cause severe hepatotoxicity when taken with acetaminophen. Acute ingestion of alcohol can increase the bioavailability of the blood thinner warfarin, which increases the chances of bleeding. Chronic ingestion can cause warfarin to be less effective, leading to increased risks of clots.
Management of Withdrawal, Toxicity, and Overdose Box 17-6 lists the common signs and symptoms of ethanol withdrawal. Signs and symptoms may vary depending on the individual’s usage pattern, the preferred type of ethanol, and the presence of comorbidities. Treatment of ethanol toxicity is supportive and strives to stabilize the patient and maintain the airway. Ethanol withdrawal can be life threatening.
One pharmacologic option for the treatment of alcohol-ism is disulfi ram (Antabuse). Disulfi ram works by altering the metabolism of alcohol. It is not a cure for alcoholism, but it helps patients who have a sincere desire to stop drinking. The rationale for its use is that patients know that if they are to avoid the devastating experience of acetaldehyde syndrome, they can-not drink for at least 3 or 4 days after taking disulfi ram. Table 17-2 outlines acetaldehyde syndrome. These adverse effects are obviously very uncomfortable and potentially dangerous for someone with any other major illnesses. For this reason, disul-fi ram is usually reserved as the treatment of last resort for “hard core” alcoholic patients for whom other treatment options (e.g., Alcoholics Anonymous, psychotherapy) have failed but who still hope to avoid continued alcohol abuse. When ethanol is ingested by an individual previously treated with disulfi ram, the blood acetaldehyde concentration rises 5 to 10 times higher than in an untreated individual. Within about 5 to 10 minutes of alcohol ingestion, the individual’s face feels hot, and soon afterward it is fl ushed and scarlet. After this, throbbing in the head and neck, nausea, copious vomiting, diaphoresis, dyspnea, hyperventila-tion, vertigo, blurred vision, and confusion occur. As little as 7 mL of alcohol will cause mild symptoms in a sensitive per-son. The effects last from 30 minutes to several hours. After the symptoms wear off, the patient is exhausted and may sleep for several hours. Most of the signs and symptoms observed after the ingestion of disulfi ram plus alcohol are attributable to the
resulting increase in the concentration of acetaldehyde in the body. There have even been a few published reports of localized disulfi ram-alcohol skin reactions when alcohol preparations—even beer-containing shampoo—were placed on the skin. The usual dosage of disulfi ram is 250 mg/day, or 125 mg/day in patients who experience adverse effects such as sedation, sexual dysfunction, and elevated liver enzyme levels.
A less noxious drug therapy option is the use of naltrexone, as mentioned previously in the section on opioids earlier in
TABLE 17-2 DISULFIRAM ADVERSE EFFECTS: ACETALDEHYDE SYNDROME
BODY SYSTEM
AFFECTED RESULT
Cardiovascular Vasodilation over the entire body, hypotension, orthostatic syncope, chest pain
Central nervous Intense throbbing of the head and neck leading to a pulsating headache, sweating, marked uneasi-ness, weakness, vertigo, blurred vision, confusion
Gastrointestinal Nausea, copious vomiting, thirst Respiratory Diffi culty breathing
Mild Withdrawal
Signs and Symptoms
Systolic blood pressure higher than 150 mm Hg, diastolic blood pressure higher than 90 mm Hg, pulse rate higher than 110 beats/min, temperature above 100° F (37.7° C), tremors, insomnia, agitation
Moderate Withdrawal
Signs and Symptoms
Systolic blood pressure 150 to 200 mm Hg, diastolic blood pressure 90 to 140 mm Hg, pulse rate 110 to 140 beats/min, temperature 100° to 101° F (37.7° to 38.3° C), tremors, insomnia, agitation
Severe Withdrawal (Delirium Tremens)
Signs and Symptoms
Systolic blood pressure higher than 200 mm Hg, diastolic blood pressure higher than 140 mm Hg, pulse rate higher than 140 beats/min, temperature above 101° F (38.3° C), tremors, insomnia, agitation
Treatment
Benzodiazepines are the treatment of choice for ethanol withdrawal. The dosages are variable and differ from institution to institution. Lower dosages are used for mild symptoms, and higher dosages are needed for severe with-drawal. The oral route is preferred; however, it is often necessary to use the intravenous route for patients experiencing severe withdrawal. Patients who are experiencing severe withdrawal often require monitoring in an intensive care unit for cardiac and respiratory function, fl uid and nutrition replacement, vital signs, and mental status. Restraints are indicated for a patient who is confused or agitated to protect the patient from self and to protect others (delirium tremens can be a terrifying and life-threatening state). Thiamine administration, hydration, and magnesium replacement may be indicated depending on the severity of the withdrawal state.
BOX 17-6 SIGNS, SYMPTOMS, AND TREATMENT OF ETHANOL WITHDRAWAL