
Analgésie multimodale postopératoire et place des AINS ... · PDF fileanti-COX 2...
60
1 Analgésie multimodale postopératoire et place des AINS anti-COX 2 Professeur Eric J.VIEL, M.D., Ph.D. Centre d‟Evaluation & Traitement de la Douleur
Transcript of Analgésie multimodale postopératoire et place des AINS ... · PDF fileanti-COX 2...

1
Analgésie multimodale
postopératoire
et place des AINS
anti-COX 2
Professeur Eric J.VIEL, M.D., Ph.D.
Centre d‟Evaluation & Traitement de la Douleur

2
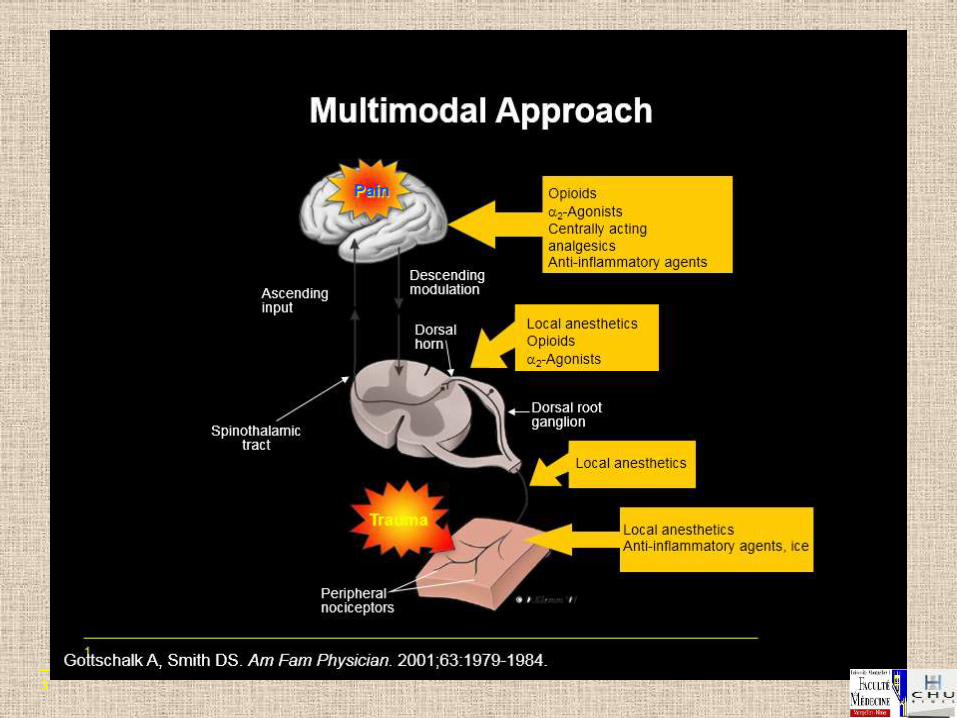
Analgésie multimodale: Les
Echelles de l’OMS
Crews JC. JAMA. 2002;288:629-632.
Severe Postoperative Pain Step 1 and Step 2 Strategies
AND
Local Anesthetic Peripheral Neural Blockade (with or without catheter)
AND
Use of Sustained Release Opioid Analgesics
Nonopioid Analgesic Acetaminophen, NSAIDs, or COX-2 Selective Inhibitors
AND
Local Anesthetic Infiltration
Moderate Postoperative Pain
Mild Postoperative Pain
Step 1 Strategy
AND
Intermittent Doses of Opioid Analgesics
Palier 3
Palier 2
Palier 1
3

4
2016

5
QUEL BESOIN DES AINS EN POSTOPERATOIRE ?
Les morphiniques ont longtemps été considérés agents de référence de l’analgésie postopératoire
MAIS…
• Ils provoquent des effets secondaires
• Ils imposent une surveillance particulière des patients
• Ils interfèrent avec les suites opératoires (NVPO)
• Ils sont peu efficaces sur la composante dynamique de la douleur
• Ils sont incomplètement efficaces sur les DPO à forte composante
inflammatoire : ORL, orthopédie-traumatologie
. Ils comportent un risque d’hyperalgésie pouvant favoriser le développement de
douleurs chroniques post-chirurgicales.
. Ils portent un risque de mésusage
Anti-COX2 péri-opératoires

6
AINS : La question ne se pose plus
les AINS figurent dans la plupart des protocoles d’analgésie postopératoire,
tous types de chirurgie confondus
les AINS sont recommandés pour l’analgésie postopératoire
Conférence de Consensus SFAR 1999
Recommandations SFAR 2016
comme alternative aux morphiniques
en association aux morphiniques :
* pour renforcer l’analgésie
* pour diminuer l’incidence des effets collatéraux
de manière indispensable en chirurgie orthopédique
Anti-COX2 péri-opératoires

7
LES AINS POSTOPERATOIRES SONT EFFICACES
… MAIS INDUISENT DES EFFETS SECONDAIRES
• Risque d’ulcèration gastro-duodénale
• Risque hémorragique
– Modification réversible hémostase primaire ( TxA2)
– En chirurgie digestive chez les patients de moins de 75 ans, la prescription d’AINS en postopératoire pendant moins de 5 jours n’augmente ni le risque hémorragique périopératoire, ni l’incidence des reprises chirurgicales pour hémostase (CE SFAR 2001)
– CI ALR périmédullaires
• Risque rénal
– diminution pression de perfusion glomérulaire ( PgE2)
– Accru par hypovolémie et terrains (athérosclérose)
Anti-COX2 péri-opératoires

8
. Très large utilisation (2ème rang mondial) . Large utilisation pour l’A.P.O. (kétoprofène, kétorolac…) . 1ère cause accidents iatrogènes rapportés à la F.D.A. Nuki Br Med J 1990 Fries et al Gastroenterology 1989
. Effets gastroduodénaux : hémorragies / perforations 20000 hospitalisations / an 2600 décès / an Source F.D.A. 1996
. Prévention ? EFFICACITE CONNUE ---> ENJEU : EFFETS ADVERSES
Coxibs
Anti-COX2 péri-opératoires

9
AINS : LES COMPLICATIONS SONT RARES mais LES CONTRE-INDICATIONS SONT FREQUENTES
• Audit of ketoprofen prescribing after orthopedic and general surgery. Benhamou et al Can J Anaesth 1999;46:109
– 22 % de contre-indications
– 11 % de prescriptions sur contre-indication
S
H2N
O
O
N
Anti-COX2 péri-opératoires

10
Utilisation du parecoxib pour l’analgésie postopératoire
agent unique
en association / analgésie multimodale
Très large utilisation des AINS en période postopératoire
kétoprofène en France
kétorolac aux E-U.
2003 : Mise à disposition du parecoxib, 1er AINS anti-cox2 injectable
Anti-COX2 péri-opératoires

11
AINS
Mécanismes d’action :
les molécules…

12
Moelle
AA K+ H+ BK
PG
Nocicepteur
CGRP, SUBSTANCE P
HISTAMINE
SÉROTONINE
Mastocyte
Plaquette
AAE
SP
Lésion tissulaire
Cerveau
Inflammation
Sensibilisation
Douleur
IL-1, TNF-
LPS, NGF
Cox

13
PLAQUETTES
Phospholipides membranaires ACIDE ARACHIDONIQUE
HPETE
HETE
5 HPETE
5 HETE LTA4
LTB4
PG G2
PG H2
PG E2 PG F2
Tx A2 PG I2 6CÉTOPG F1
LTC4 LTD4 LTE4
Radicaux superoxydes
LEUCOCYTES VAISSEAUX
Phospholipase A
Cyclo oxygénases Lipo oxygénases
CORTICOIDES INDOMETACINE Inhib. calciques
A I N S
PG : Prostaglandines LTC : Leucotriènes Tx : Thromboxane
phospholipide A

14
Interaction cyclo-oxygénase - substrat
N-terminal
Arginine
at 120
C-terminal
containing
active sites
Kurumbail et al Nature 1996
COOH
Ac. arachidonique
AINS

15
cyclooxygénase 2 ?
• 1971 : Inhibition de le cyclo-oxygénase / action AINS
Vane et al Nat New Biol 1971
• 1989 : Induction de la cyclo-oxygénase / inflammation
Raz et al Proc Natl Acad Sci USA 1989
• 1990 : Facteurs d’induction : cytokines
Fu et al J Biol Chem 1990
• 1991 : détermination du gène de la cyclo-oxygénase 2
Xie et al Proc Natl Acad Sci USA
Anti-COX2 péri-opératoires

16
COX-2 Induction
in Spinal Cord
COX-2 Induction
in Inflamed Paw
Acute Inflammation-Based Pain: Hargreaves Model
Hyperalgesia
Swelling &
Hyperalgesia
Carrageenan injection
COX-2 induction
Swelling
Thermal sensitivity
(Maximal by 3 hours)
oral

17
Smith et al Proc Natl Acad Sci U S A 1998
prophylactique
thérapeutique
0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
Normal Sham
PG
E2 (
ng
/mL
) L’inhibition COX-1 ne réduit pas l’induction de PGE2 dans le LCR
Inh Cox 1 Inh Cox 2
Anti-COX2 péri-opératoires

18
COX 1 constitutive COX 2 inductible
Localisation Plaquettes, cell.endothéliales
Cerveau, Poumon, Prostate
Estomac, rein, prostate
Monocytes, fibroblastes
# tous tissus (+)
Chondrocytes + tous tissus
Rôle Production basale PG
Production stimulée PG
Réponse cell / hormones
Processus inflammatoires
Physiologie rénale
Croissance cellulaire
Physiologie vasculaire ENZYME de REGULATION
ENZYME d'ADAPTATION
Smith Drugs 1994
AINS et COX

19
COX-2: une cible pour les agents analgésiques et anti-inflammatoires
Acide arachidonique
COX-1 (Constitutive)
COX-2 (Inductible)
Estomac
Intestin
Rein
Plaquettes
Sites inflammatoires
Macrophages
Synoviocytes
Glucocorticoïdes Bloquent expression mRNA (–)
•
•
X CIBLE de l’INHIBITEUR
SPECIFIQUE
ANTICOX-2
(–)
AINS
classiques
Anti-COX2 péri-opératoires
20
Mécanismes d'action
• AINS classiques anti COX 1 et anti COX 2 : inhibition physiologique ---> effets adverses (rein, estomac, hémostase) inhibition inflammation ---> effets thérapeutiques • AINS anti COX 2 : pas ou peu d'inhibition physiologique ---> pas d'effets adverses (???) inhibition inflammation ---> effets thérapeutiques ---> développement Anti-COX 2 préférentiels et sélectifs
AINS anti COX2

21
AINS classiques : Liaison non-spécifique à COX-1 et COX-2
Terminal Carboxylic Acid Plays an Important Role
COX-1
N-terminal
Carboxylic
group
of NSAID
forms
“salt bridge”
with
Arginine
at 120
C-terminal
containing
active sites
NSAID
(flurbiprofen)
phenyl group
sits in
hydrophobic
channel
COX-2
N-terminal
Carboxylic
group
of NSAID
forms
“salt
bridge”
with
Arginine
at 120
C-terminal
containing
active sites
NSAID
(flurbiprofen)
phenyl group
sits in
hydrophobic
channel
Kurumbail et al Nature 1996
22
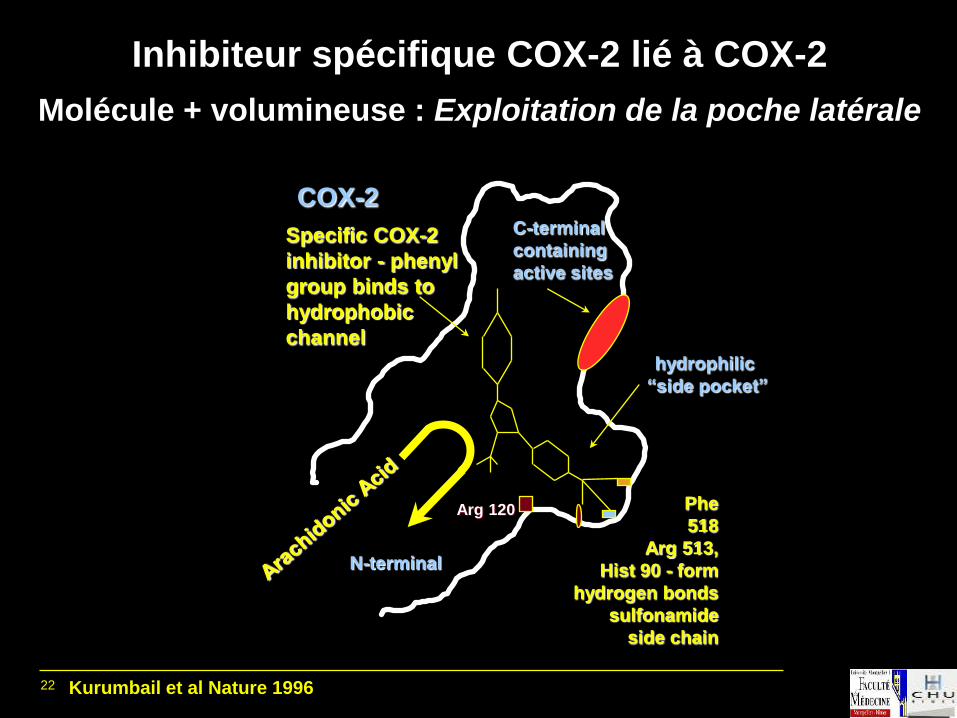
Inhibiteur spécifique COX-2 lié à COX-2
Molécule + volumineuse : Exploitation de la poche latérale
Kurumbail et al Nature 1996
COX-2
hydrophilic
“side pocket”
N-terminal
C-terminal
containing
active sites
Phe
518
Arg 513,
Hist 90 - form
hydrogen bonds
sulfonamide
side chain
Specific COX-2
inhibitor - phenyl
group binds to
hydrophobic
channel
Arg 120

23
COX-1 active site
Flurbiprofen
COX-2 active site
Celecoxib Prototype
Kurumbail et al. Nature 1996; 384: 644-8 Picot et al. Nature 1994; 367: 243-49
X-Ray Crystallography

24
Inhibiteur COX-2 spécifique et enzyme COX-1 Chaîne latérale encombrante empéchant la pénétration du
canal COX-1 trop étroit
N-terminal
COX-1
C-terminal
containing
active sites
Molecule
has no
carboxylic
group to
bind with
Arginine
at 120
Bulky side chains inhibit entry
into the narrower COX-1 channel
Kurumbail et al Nature 1996

25
AINS traditionnels : Nonselective because terminal carboxylic acid or
enolic acid interacts with Arg 120 in COX-1
OH H 3 C
F
O
S
N
HO
C
NH
O
N
O
O
CH 3
carboxylic acid enolic acid
indomethacin flurbiprofen piroxicam
O
Cl
N
COOH
O

26
Premier exemple de création ciblée d’une molécule
“Purpose Designed” Specific COX-2 Inhibitor:
• Favoriser liaison au pôle hydrophile de la poche latérale spécifique de l’enzyme COX-2 Incorporation d’une chaîne latérale hydrophile
• Empécher liaison au site actif de l’enzyme COX-1
– Elimination ac. carboxylique ou chaîne latérale enolique
– Chaîne latérale encombrante empéchant l’entrée dans le canal COX-1 étroit
• Résultat : sélectivité grâce à un nouveau mécanisme :
– Faible affinité pour inhibition compétitive COX-1
– Affinité élevée pour inhibition non-compétitive COX-2
– réversibilité très lente durée action >> T1/2 pharmacocinétique

27
celecoxib: A “Purpose Designed” COX-2 Specific Inhibitor
Penning et al J Med Chem 1997
N N
H 3C
C F 3
S
N H 2
O
O
Polar sulfonamide
group to bind
to hydrophilic
“side pocket”
Methylphenyl
group sits in
hydrophobic
channel
No terminal
acid group to
bind to Arg120
in COX-1
AINS anti COX2

28
“To our knowledge this is the first example of a
membrane protein being successfully studied
as a target in structure-based drug design”
Kurumbail et al Nature 1996
.
AINS anti COX2
Conséquences thérapeutiques ?

29
A.I.N.S. ratio inhibition COX 2 / COX 1 valdecoxib 0,003 rofecoxib 0,005 celecoxib 0,030 nimesulide 0,038 meloxicam 0,040 piroxicam 0,1 diclofenac 0,3 ibuprofène 2,6 naproxène 3,8 ketoprofène 5,1 indométhacine 10
Bejarano Curr Rev Pain 1999
Classification / sélectivité AINS anti COX2

30
Sélectivité d’inhibition
d’après Fitzgerald et Patrono N Engl J Med 2001
Sélectivité
COX-1
Sélectivité
COX-2
Indométacine Célécoxib
Rofécoxib
Nimésulide
Meloxicam
Ibuprofène
Naproxène
Paracétamol
6-MNA
Diclofénac
0,01 0,10 1,00 10,00 100,00
0,01
0,10
1,00
10,00
100,00
Cyclooxygénase-1 IC50 (µM)
Cyc
loo
xyg
én
as
e-2
IC
50 (
µM
)
valdecoxib

31
Effets adverses AINS conventionnels
Effets prévisibles / inhibition cyclo-oxygénase tissulaire . Tératogénicité, inhibition fermeture canal artériel . Retard déclenchement et prolongation travail obstétrical . Dyspepsie, ulcères, hémorragies digestives, perforation ulcère . Rétention hydro-sodée, aggravation insuffisance cardiaque . Aggravation insuffisance rénale hémorragie digestive ( lésion préexistante ) . Effets anti-agrégant plaquettaire hémorragie péri-partum . Aggravation possible infection : fasciite nécrosante
AINS anti COX2

32
La sélectivité prévient-elle le risque hémostatique ? * celecoxib à doses > doses thérapeutiques (+50%) pas d'effets agrégabilité plaquettaire et thromboxanes Mengle-Gaw et al Arthritis Rheum 1997
* rofecoxib à doses > doses thérapeutiques (X 10 et 20) temps de saignement non modifié Lanza et al Aliment Pharmacol Ther 1999
AINS anti COX2

33
*
*
*
*
** **
**
**
** p < 0,001 vs kétorolac
** p < 0,001 vs placebo
VARIATION DE L’AGRÉGATION PLAQUETTAIRE INDUITE PAR L’ACIDE ARACHIDONIQUE
Sujets jeunes (20 à 55 ans)
Noveck RJ, et al. Parecoxib sodium does not impair platelet function in healthy elderly
and non-elderly individuals. Two randomised, controlled trials.Clin Drug Invest 2001 Non commercialisé en France.
Avant traitement
J 8, 30 min avant injection
J 8, 2 h après injection
J 8, 4 h après injection
J 8, 6 h après injection
(n = 15)
Placebo
(n = 15)
Kétorolac 30 mg IV
4 fois/j
(n = 15)
Parécoxib 40 mg IV
2 fois/j
100
80
60
40
20
0 Ag
rég
ati
on
pla
qu
ett
air
e (
%)
(méd
ian
e ±
in
terq
uart
ile)

34
AGRÉGATION PLAQUETTAIRE INDUITE PAR L’ACIDE ARACHIDONIQUE
Sujets âgés (65 à 83 ans)
100
80
60
40
20
0
Sujets âgés
Parécoxib sodium
40 mg 2 fois/j IV
(n = 14)
Kétorolac
15 mg 4 fois/j IV
(n = 20)
Placebo
(n = 20)
* p < 0,001 vs kétorolac
** p < 0,001 vs placebo
Avant traitement
J 8, 30 min avant injection
J 8, 2 h après injection
J 8, 4 h après injection
J 8, 6 h après injection
Agré
gation p
laquettaire (
%)
(média
ne ±
inte
rquart
ile)
Noveck et al. Parecoxib sodium does not impair platelet function in healthy elderly and non-elderly individuals.
Two randomised, controlled trials. Clin Drug Invest 2001
AINS anti COX2

35
AINS – Amygdalectomie
Risque relatif pour un saignement postopératoire sévère
Marret et al Anesthesiology 2003

36
AINS – Amygdalectomie
Risque relatif de réintervention
Marret et al Anesthesiology 2003

37
A 2013 updated systematic review & meta-analysis of 36 randomized
controlled trials:
no apparent effects of non steroidal anti-inflammatory agents on the
risk of bleeding after tonsillectomy Riggin L et al. Clin. Otolaryngol. 2013, 38, 115–129
Any hemorrhage that could be managed conservatively, all
NSAIDs.
38
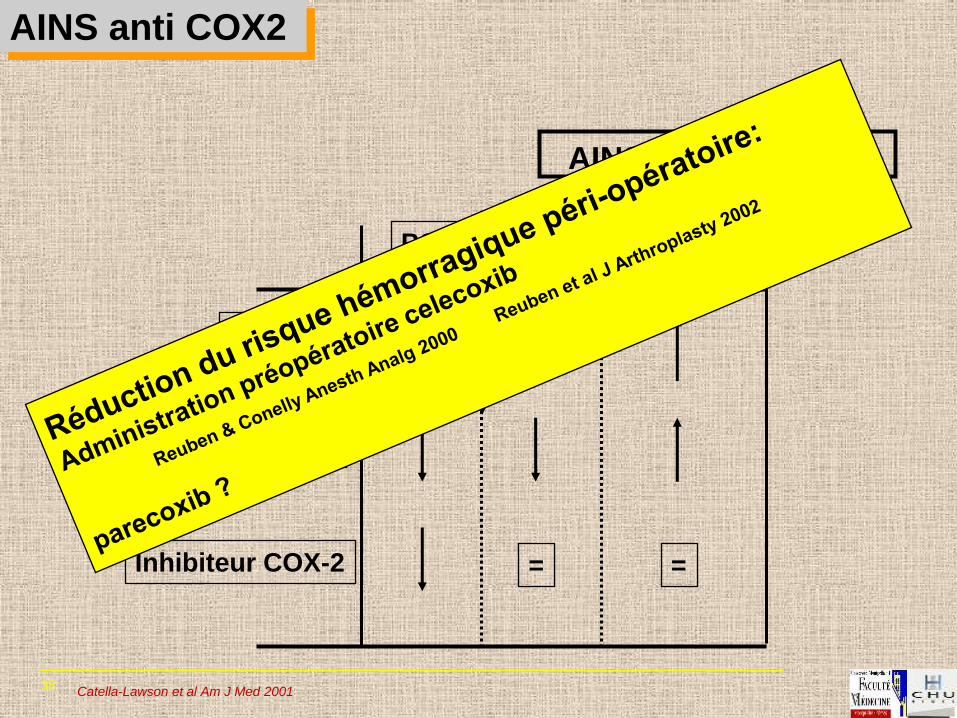
AINS et saignement
PGI2 TXA2 Hémorragie
Aspirine
AINS classique
Inhibiteur COX-2
=
= =
Catella-Lawson et al Am J Med 2001
AINS anti COX2

39
Risque cardiovasculaire
Risque lié à l’effet pro-agrégant; étude VIGOR:
8076 patients: rofecoxib ou naproxène, pas d’aspirine
risque relatif d’accident CV: 2,4 (IC: 1,4-4,0)
Etude CLASS (8059 patients, celecoxib vs ibuprofène ou diclofenac, aspirine autorisée):
pas d’excès d’évènements CV
Mais risque annualisé d’infarctus supérieur à celui observé avec l’aspirine (Steg, 2002)
AINS anti COX2

40
Cyclooxygénases et hémostase
Catella-Lawson & Crofford Cyclooxygenase inhibition and thrombogenicity. Am J Med 2001
Plaquettes
COX-1
Vasoconstricteur
Promoteur de l’agrégation plaquettaire
Hémostase Thrombose
Cellules endothéliales
COX-1
COX-2
Thromboxane (TxA2) Prostacycline (PGI2)
AINS classiques
Inhibiteurs COX-2
Vasodilatateur
Inhibiteur de l’agrégation plaquettaire
Faible dose aspirine
Définitif
Bref
Autres facteurs : NO, diphosphatase
Effet pro-agrégant ? AINS anti COX2

41
ISCOX-2: Evènements CV après chirurgie cardiaque
Nussmeier et al. NEJM, 2005

42
A.I.N.S. antiCOX2 périopératoires
• Risque accru, dose-dépendant, d’accident coronarien ou vasculaire cérébral : 2035 patients traités
par celecoxib (essai prévention adénome colorectal) Solomon et al N Engl J Med 2005
• Pas d’accroissement du risque coronarien par les AINS non-sélectifs (4975 patients)
Garcia-Rodriguez et al Circulation 2004
Pas de conclusion possible sur l’utilisation périopératoire du celecoxib, du parecoxib et du
valdecoxib.
• Données contradictoires sur celecoxib : pas d’augmentation du risque ?
d’après Wu CL. Refresher Course Lecture ASRA 2005 et Ferrante FM. Refresher Course Lecture ASRA 2005

43
JAMA. 2006 Sep 12
Cardiovascular Risk and Inhibition of Cyclooxygenase: A Systematic Review of the Observational
Studies of Selective and Nonselective Inhibitors of Cyclooxygenase 2.
McGettigan P, Henry D
Clinical Pharmacology, School of Medicine and Public Health, Newcastle, New South Wales, Australia.
Evidence that rofecoxib increases the risk of myocardial infarction has led to scrutiny of other
nonsteroidal anti-inflammatory drugs (NSAIDs). Regulatory agencies have provided variable advice
regarding the cardiovascular risks with older nonselective NSAIDs.
OBJECTIVE: To undertake a systematic review and meta-analysis of controlled observational studies
to compare the risks of serious cardiovascular events with individual NSAIDs and cyclooxygenase 2
inhibitors.
DATA SOURCES: electronic databases (1985-2006), scientific meeting proceedings, epidemiological
research Web sites, and bibliographies of eligible studies. STUDY SELECTION: Eligible studies were
of case-control or cohort design, reported on cardiovascular events (predominantly myocardial
infarction) with cyclooxygenase 2 inhibitor, NSAID use, or both with nonuse/remote use of the drugs
as the reference exposure. Of 7086 potentially eligible titles, 17 case-control and 6 cohort studies
were included. Thirteen studies reported on cyclooxygenase 2 inhibitors, 23 on NSAIDs, and 13 on
both groups of drugs.
CONCLUSIONS: This review confirms the findings from randomized trials regarding the risk of
cardiovascular events with rofecoxib and suggests that celecoxib in commonly used doses may not
increase the risk, contradicts claims of a protective effect of naproxen, and raises serious questions
about the safety of diclofenac, an older drug

44
Safety of a cyclo-oxygenase-2 inhibitor in patients with aspirin-sensitive asthma
Martin-Garcia et al, Chest 2002;121:1812-7
40 patients avec asthme et intolérance à l’aspirine et aux AINS
Peak-Flow/jour pendant 1 semaine avant le test de provocation et VEMS avant et après le test
J1: rofecoxib 6,25 mg
J3: rofecoxib 12,5 mg
J10: rofecoxib 25 mg
Tous les patients ont toléré la dose de 25 mg de rofécoxib
VEMS inchangé
AINS anti COX2

45
La sélectivité modifie t-elle l'efficacité analgésique ? * rofecoxib et celecoxib / administration chronique ostéoarthrites efficacité identique aux AINS conventionnels Hubbard et al Rheumatol Eur 1998
* rofecoxib et celecoxib / administration aiguë douleurs dentaires efficacité identique aux AINS conventionnels Mehlisch et al Clin Pharmacol Ther 1997 Erich et al Clin Pharmacol Ther 1999
MAIS : augmenter la sélectivité n'augmente pas l'efficacité analgésique celecoxib (x 375) vs rofecoxib (x 800)
AINS anti COX2

46
Hydrolyse
Glucuronide
Métabolite actif
hydroxylé Glucuronide
(Sulphonamide)
Hydroxylation Glucuronidation
d’après Karim et al J Clin Pharmacol 2001
Parecoxib prodrogue injectable du valdecoxib
parecoxib (prodrogue)
O N
S O 2 N
CH3
COCH2CH3
-
Na+
valdecoxib (principe actif)
O N
SO2NH2
CH3

47
BC
C
AB A
ABC
Délai d’installation de l’analgésie
Rapport d’expert clinique. Étude 018. N93-00-06-018.
0
20
40
Tem
ps
mé
dia
n (
min
)
(n = 37)
Placebo
31 min
(n = 43)
Parécoxib 20 mg IV
27 min
(n = 36)
Parécoxib 40 mg IV
11 min
(n = 41)
Kétorolac 30 mg IV
12 min
(n = 39)
Morphine 4 mg IV
15 min
CHIRURGIE ORTHOPÉDIQUE
(a) Prothèse totale de genou.
Lettres identiques (A,B,C) : pas de différence significative entre les traitements.
Significativité définie par p 0,05.
Coxibs postopératoires

48
B
A
A
A
B
Rapport d’expert clinique. Étude 018. N93-00-06-018.
6
5
4
3
2
1
0
Tem
ps m
éd
ian
(h
eu
res)
(n = 37)
Placebo
1 h 48 min
(n = 43)
Parécoxib 20 mg IV
3 h 09 min
(n = 36)
Parécoxib 40 mg IV
5 h 10 min
(n = 41)
Kétorolac 30 mg IV
4 h 35 min
(n = 39)
Morphine 4 mg IV
2 h 07 min
(a) Prothèse totale de genou.
Lettres identiques (A,B) : pas de différence significative entre les traitements.
Significativité définie par p 0,05.
Délai de demande analgésique
CHIRURGIE ORTHOPÉDIQUE
Coxibs postopératoires

49
Both oral valdecoxib and injected parecoxib are effective treatments for acute postop. pain
valdecoxib more efficacious and longer duration of action vs other NSAIDs and coxib
parecoxib, as injectable, advantageous in postoperative period, patients unable to swallow
and patients with nausea and vomiting
efficacité analgésique comme agent unique ?
Coxibs postopératoires
50
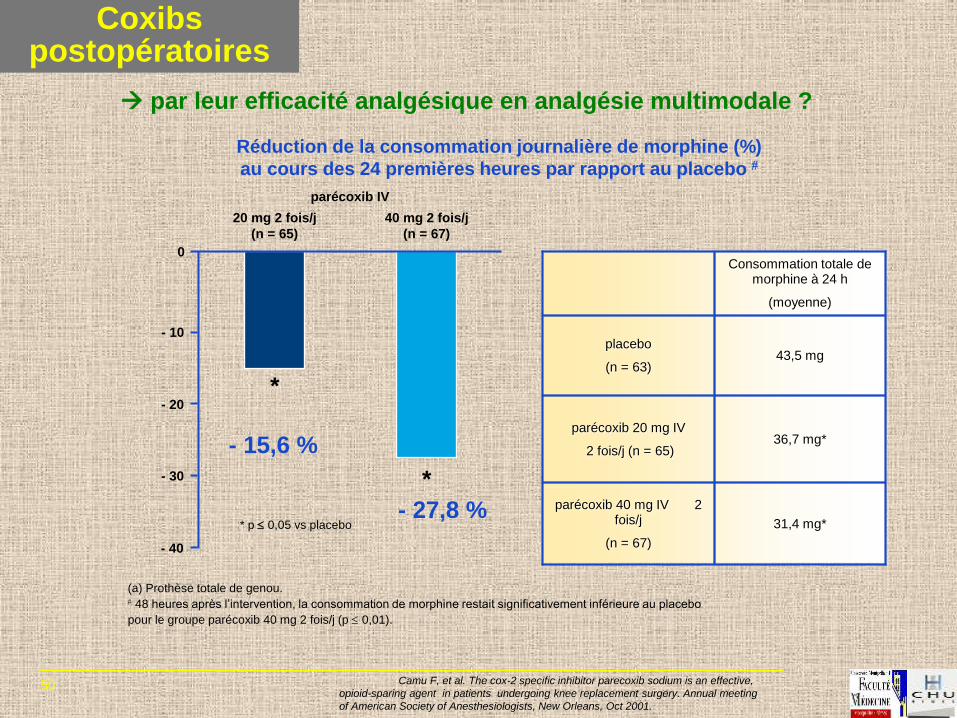
*
*
* p 0,05 vs placebo 31,4 mg*
parécoxib 40 mg IV 2 fois/j
(n = 67)
36,7 mg* parécoxib 20 mg IV
2 fois/j (n = 65)
43,5 mg placebo
(n = 63)
Consommation totale de morphine à 24 h
(moyenne)
Réduction de la consommation journalière de morphine (%)
au cours des 24 premières heures par rapport au placebo
- 40
- 30
- 20
- 10
0
parécoxib IV
20 mg 2 fois/j
(n = 65)
40 mg 2 fois/j
(n = 67)
Camu F, et al. The cox-2 specific inhibitor parecoxib sodium is an effective,
opioid-sparing agent in patients undergoing knee replacement surgery. Annual meeting
of American Society of Anesthesiologists, New Orleans, Oct 2001.
(a) Prothèse totale de genou. 48 heures après l’intervention, la consommation de morphine restait significativement inférieure au placebo
pour le groupe parécoxib 40 mg 2 fois/j (p 0,01).
- 15,6 %
- 27,8 %
par leur efficacité analgésique en analgésie multimodale ?
Coxibs postopératoires

51
d’après Viscusi et al Anesth Analg 2004 feb.
In-hospital resource use to manage pain after single dose of IV parecoxib sodium, a novel parenteral
COX-2 inhibitor, for pain associated with laparoscopic cholecystectomy
Diminution consommation analgésique, sortie + rapide
Durée de séjour en S.S.P.I. : 78 vs 90 min, p < 0,05
Durée de séjour en centre ambulatoire : 6,9 vs 9,8 h , p = 0,04
Patient postdischarge symptom experience after single presurgery dose of IV parecoxib sodium, a novel
COX-2 inhibitor, followed by oral valdecoxib for pain associated with laparoscopic cholecystectomy
réduction scores de douleur et consommation analgésique
d’après Joshi et al Anesth Analg 2004 feb.
Coxibs postopératoires
par leur efficacité analgésique préventive ?
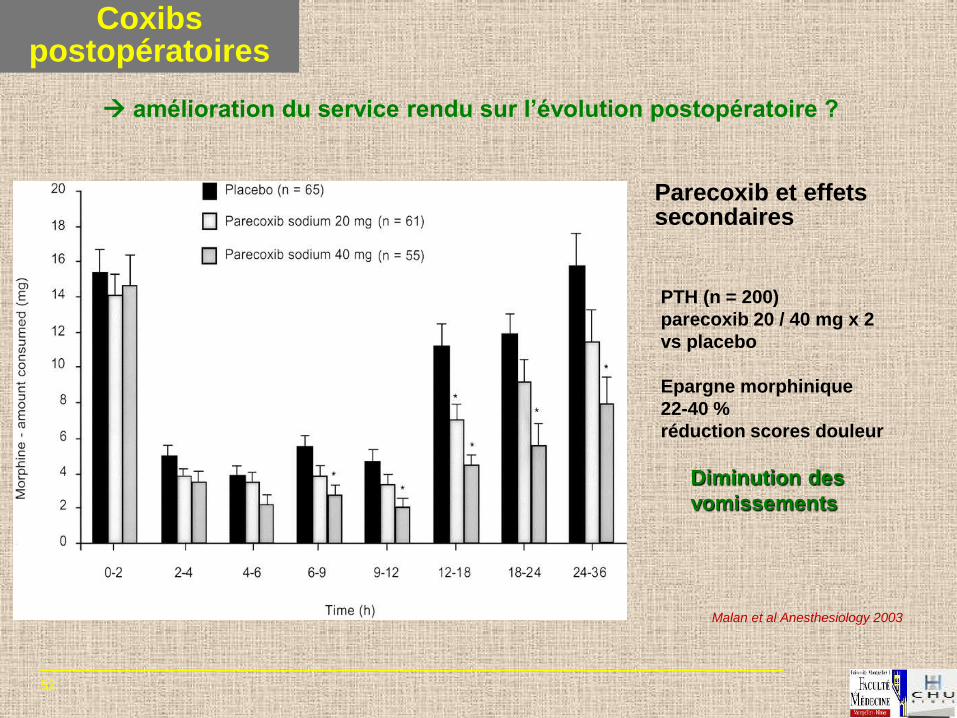
52
Parecoxib et effets secondaires
Malan et al Anesthesiology 2003
PTH (n = 200)
parecoxib 20 / 40 mg x 2
vs placebo
Epargne morphinique
22-40 %
réduction scores douleur
Diminution des
vomissements
amélioration du service rendu sur l’évolution postopératoire ?
Coxibs postopératoires

53
Effect of administration of nonsteroidal antiinflammatory drugs (NSAIDs) in addition to patient-controlled analgesia intravenous morphine after surgery on the relative risk of postoperative nausea and vomiting
Marret E et al Anesthesiology 2005 102: 1249-1260

54
(n=7)
Nausea (n=18)
Pruritus (n=9)
Urinary
Retention
Apnea (n=3)
Rel . Risk 0.4 1.0 1.6
NSAIDs better Control better
AINS et effets secondaires morphine
RR=0.80 (0.73-0.89) P<0.001
RR=0.88 (0.66-1.16)
RR=0.69 (0.43-1.11)
RR=0.86 (0.45-1.67)
Marret et al Anesthesiology 2003 19 studies 1939 patients (1069 NSAID’s)
A.I.N.S. périopératoires

55
Adding COX-2 inhibitors to opioids: Reducing opioid adverse events by
reducing opioid use
„Once threshold reached, every further 3–4 mg increase will be associated with 1 clinically meaningful opioid-related symptom’
Morphine equivalent dose on day 0–1 (mg)
0 10 20 30 40 50 60
No event
1 event
2 events
3 events All patients
Regression for all patients
Clinically meaningful events on day 1 following lap cholecystectomy
Zhao et al J Pain Symptom Manage 2004
A.I.N.S. périopératoires

56
McDaid et al. Health Techno Ass 2010; Maund et al. BJA 2011
Comparaison Conso de morphine de
base (mg)
Différence moyenne:
(mg)
placebo 37,43 (2) 0
paracetamol vs placebo -6,34 (-9,02 à -3,65)
AINS vs placebo -10,18 (-11,65 à -8,72)
COX-2 vs placebo -10,92 (-12,77 à -9,08)
AINS vs paracetamol -3,85 (-6,80 à -0,89)
COX-2 vs paracetamol -4,58 (-7,83 à -1,35)
COX-2 vs AINS -0,74 (-3,03 à 1,56)
60 études
Méta analyse: association paracétamol, AINS, COX-2 et morphine

57
PARECOXIB, PROPACETAMOL AND THEIR COMBINATION FOR ANALGESIA AFTER TOTAL HIP ARTHROPLASTY: A
RANDOMIZED NON-INFERIORITY TRIAL Accepted for publication Acta Anaesthesiol Scand 2017
Camu F, Borgeat A, Heylen RJ, Viel EJ , Boye ME, Cheung RY
This study assessed non-inferiority of parecoxib versus combination parecoxib+propacetamol and compared the
opioid-sparing effects of parecoxib, propacetamol and parecoxib+propacetamol versus placebo after total hip
arthroplasty.
METHODS: Randomized, placebo-controlled, parallel-group, non-inferiority study, patients received one of four IV
treatments after surgery: parecoxib 40 mg bid (n = 72); propacetamol 2 g qid (n = 71); parecoxib 40 mg bid plus
propacetamol 2 g qid (n = 72); or placebo (n = 38) with supplemental IV patient-controlled analgesia (morphine).
Patients and investigators were blinded to treatment. Pain intensity at rest and with movement was assessed
regularly, together with functional recovery (modified Brief Pain Inventory-short form) and opioid-related side
effects (Opioid-Related Symptom Distress Scale) questionnaires up to 48h.
RESULTS: After 24 h, cumulative morphine consumption was reduced by 59.8% (P < 0.001), 38.9% (P < 0.001), and
26.8% (P = 0.005) in the parecoxib+propacetamol, parecoxib, and propacetamol groups, respectively, compared
with placebo. Parecoxib did not meet criteria for non-inferiority to parecoxib+propacetamol.
Parecoxib+propacetamol and parecoxib significantly reduced least squares mean pain intensity scores at rest
and with movement compared with propacetamol (P < 0.05). One day after surgery, parecoxib+propacetamol
significantly reduced opioid-related symptom distress and decreased pain interference with function compared
with propacetamol or placebo.
CONCLUSION: Parecoxib and parecoxib+propacetamol provided significant opioid-sparing efficacy compared
with placebo; non-inferiority of parecoxib to parecoxib+propacetamol was not demonstrated. Opioid-sparing
efficacy was accompanied by significant reductions in pain intensity on movement, improved functional
outcome, and less opioid-related symptom distress. Study medications were well tolerated.

58
Figure 3. (A) Least squares mean (LSM) pain
intensity score (visual analog scale [VAS])
during first 48h after surgery (modified
intent-to-treat cohort, last observation
carried forward) and (B) LSM Opioid-Related
Symptom Distress Scale (OR-SDS) scores
for each dimension and composite of all
three dimensions on Day 1 (modified intent-
to-treat cohort).

59
• AINS utiles pour l’analgésie multimodale postopératoire
• Nombreuses interactions additives et synergiques avec les autres analgésiques
• Sécurité d’utilisation des AINS traditionnels et des inhibiteurs de COX-2 quand sont respectées les CI, les doses et les durées de traitement.
• Les AINS et les inhibiteurs de COX-2 n’exposent pas à un risque majoré de complications cardiovasculaires dans la chirurgie non cardiaque à condition que les patients n’aient pas d’antécédents cardiovasculaires.
• AINS et inhibiteurs de COX-2: interrogation sur le risque de fistule digestive dans la chirurgie colorectale.
CONCLUSION

60
Merci de m’avoir écouté…


















