
AN EVALUATION OF GROW, A MUTUAL-HELP COMMUNITY MENTAL HEALTH ORGANISATION
5
COMMUNITY HEALTH STUDIES VOLUME XI. NUMBER 1. 1987 AN EVALUATION OF GROW, A MUTUAL-HELP COMMUNITY MENTAL HEALTH ORGANISATION Jim Young and Christopher L Williams Department of Psjbchology, University q/ Tasmania Introduction For the past decade self-help or mutual help* groups have been of increasing importance as a part of the mental health system both in Australia and overseas.’-4 While mutual help groups and professional services are not necessarily competing modalities,‘ in part the significance of the mutual help strategy lies in its responsiveness to dissatisfaction with bureaucratic and institution- alised services. It provides a means for the movement away from reliance on professionally provided help and institutions toward consumer provided help within the less restrictive environment of the community.6 Mutual-help groups in the mental health field in Australia are now numerous: the Melbourne Collective of Self-Help Groups report 25 organisations sponsoring such groups in that city alone. If the potential of such gropps to contribute to the health of the community is to be realised, not only does their efficacy need to be carefully evaluated but their relationship to other community health services needs also to be understood. The purpose of this report on the first of three stages of a research evaluation is to provide a descriptive step in this direction. Apart from Alcoholics Anonymous, the oldest mutual-help organisation in Australia is GROW which was established (as Recovery) in Sydney in 1957. Recovery was started by a group of former patients of mental hospitals who found friendship and acceptance at meetings of AA but for whom the AA programme was inappropriate. One of the members of the group was a Roman Catholic priest and theologian, Dr Cornelius Keogh, who had himself been hospitalised with serious mental illness and he became central to the organisation as a scribe and author of the Program ofGrowth to Maturity, a compilation of the maxims which the Recoverers found important in their rehabilitation.’ * The terms self-help and mutual-help are often used synonymously in the literature: we have adopted the use of mutual-help as more accurately describing the essentially social nature of the strategy. YOUNG 38 The Program has as its underlying assumption that if the members’ behaviour is ‘ordinary’, no matter what their inclinations or feelings, their acceptance will be assured and their ability to cope and their rehabilitation enhanced. In this context, although members may join with highly specific symptoms or problems, the specifics become irrelevant: no matter what, all members aim, through the application of the Program, to become ‘ordinary’. As a result of this inclusiveness, as the organisation has expanded, many members joining have been people who have never been hospitalised or diagnosed as mentally ill but have been seeking ways to deal with problems with which they have felt unable to cope. The change of name of the organisation to GROW in the mid-70s recognised this fact. GROW groups of no more than 15 members meet for about two hours each week. A highly- structured order of meeting is followed. This provides for the discussion of problems faced by members and the recommendation of practical tasks, anchored in the Program, to meet those problems; a mutual monitoring of progress; and a segment for reading, learning and discussion of some of the Program material. As wellas the weekly meeting, members are encouraged to maintain contact with and support for each other in a ‘caring and sharing community’, and social functions are arranged. GROW has now expanded to more than 300 groups throughout Australia with more than 40 persons employed as staff and a budget of more than $1.5 million. Theoretically, GROW’S operation could be conceptualised in diverse ways. Reissman’s “helper” theory.* social network theory,’.“’ and cognitive- behavioural theory”.” among others would all be appropriate. We decided to include questions which would be congruent with all these theoretical approaches in the belief that an appropriate focus would emerge to guide further study. Such has proved to be the case. COMMUNITY HEALTH STUDIES
Transcript of AN EVALUATION OF GROW, A MUTUAL-HELP COMMUNITY MENTAL HEALTH ORGANISATION

C O M M U N I T Y H E A L T H STUDIES V O L U M E XI . N U M B E R 1. 1987
AN EVALUATION OF GROW, A MUTUAL-HELP COMMUNITY MENTAL HEALTH ORGANISATION
Jim Young and Christopher L Williams
Department of Psjbchology, University q/ Tasmania
Introduction For the past decade self-help or mutual help*
groups have been of increasing importance as a part of the mental health system both in Australia and overseas.’-4 While mutual help groups and professional services are not necessarily competing modalities,‘ in part the significance of the mutual help strategy lies in its responsiveness to dissatisfaction with bureaucratic and institution- alised services. I t provides a means for the movement away from reliance on professionally provided help and institutions toward consumer provided help within the less restrictive environment of the community.6
Mutual-help groups in the mental health field in Australia are now numerous: the Melbourne Collective of Self-Help Groups report 25 organisations sponsoring such groups in that city alone. If the potential of such gropps to contribute to the health of the community is to be realised, not only does their efficacy need to be carefully evaluated but their relationship to other community health services needs also to be understood. The purpose of this report on the first of three stages of a research evaluation is to provide a descriptive step in this direction.
Apart from Alcoholics Anonymous, the oldest mutual-help organisation in Australia is GROW which was established (as Recovery) in Sydney in 1957. Recovery was started by a group of former patients of mental hospitals who found friendship and acceptance at meetings of AA but for whom the AA programme was inappropriate. One of the members of the group was a Roman Catholic priest and theologian, Dr Cornelius Keogh, who had himself been hospitalised with serious mental illness and he became central to the organisation as a scribe and author of the Program ofGrowth to Maturity, a compilation of the maxims which the Recoverers found important in their rehabilitation.’ * The terms self-help and mutual-help are often used synonymously in the literature: we have adopted the use of mutual-help as more accurately describing the essentially social nature of the strategy.
YOUNG 38
The Program has as its underlying assumption that if the members’ behaviour is ‘ordinary’, no matter what their inclinations or feelings, their acceptance will be assured and their ability to cope and their rehabilitation enhanced. In this context, although members may join with highly specific symptoms or problems, the specifics become irrelevant: no matter what, all members aim, through the application of the Program, to become ‘ordinary’. As a result of this inclusiveness, as the organisation has expanded, many members joining have been people who have never been hospitalised or diagnosed as mentally ill but have been seeking ways to deal with problems with which they have felt unable to cope. The change of name of the organisation to GROW in the mid-70s recognised this fact.
GROW groups of no more than 15 members meet for about two hours each week. A highly- structured order of meeting is followed. This provides for the discussion of problems faced by members and the recommendation of practical tasks, anchored in the Program, to meet those problems; a mutual monitoring of progress; and a segment for reading, learning and discussion of some of the Program material. As wellas the weekly meeting, members are encouraged to maintain contact with and support for each other in a ‘caring and sharing community’, and social functions are arranged.
GROW has now expanded to more than 300 groups throughout Australia with more than 40 persons employed as staff and a budget of more than $1.5 million.
Theoretically, GROW’S operation could be conceptualised in diverse ways. Reissman’s “helper” theory.* social network theory,’.“’ and cognitive- behavioural theory”.” among others would all be appropriate. We decided to include questions which would be congruent with all these theoretical approaches in the belief that an appropriate focus would emerge to guide further study. Such has proved to be the case.
C O M M U N I T Y H E A L T H S T U D I E S
Method After extensive negotiations with GROW'S
national and state organisations it was arranged that a questionnaire be administered to all GROW members throughout Australia through the weekly group meetings. Individual members were issued with 'Research Participant Cards' inscribed with a number so that they could be identifiec. yet remain anonymous.
A thirty-item questionnaire was dzveloped by the researchers in consultation with GROW leaders and members and with pilot trials in Tasmania. The questionnaire was then taken to each State by a researcher and introduced to member:, at regional and state meetings and by visiting more isolated groups and group organisers. The group organisers were encouraged to have the members complete the questionnaire at the group meeting but the actual administration to individual members was left in the hands of the organisers who then r8:turned the completed questionnaires by mail.
The questionnaire sought informs.tion in six areas:
demographic details, ( so that the GROW population could be set in context);
social network, (which is widely held to be directly related to mental health and may be a critical factor in GROW'S effectiveness or otherwise);
religious affiliation and practices, I since it had been suggested that GROW was essentially a belief system and that specific: religious orientation was a hallmark of members);
GROW involvement and satisfaction (to get some indication of how central membership o f GROW is in the lives of its members and how it met perceived needs);
reason for becoming a member, (to see whether the needs which members perceived fell into definable or recognisable categories); and.
help sought and /o r received from other sources for the same problems that brought people to GROW and the relation ofsuch help to that which might be received from GROW, (to see whether GROW membership is related to demands on other resources).
Questions were included, not only to provide a basic profile of the organisation and it:; members, but to provide also some guidance in the design of proposed further stages of research and evaluation.
Copies of the questionnaire used are available upon request from the principal author.
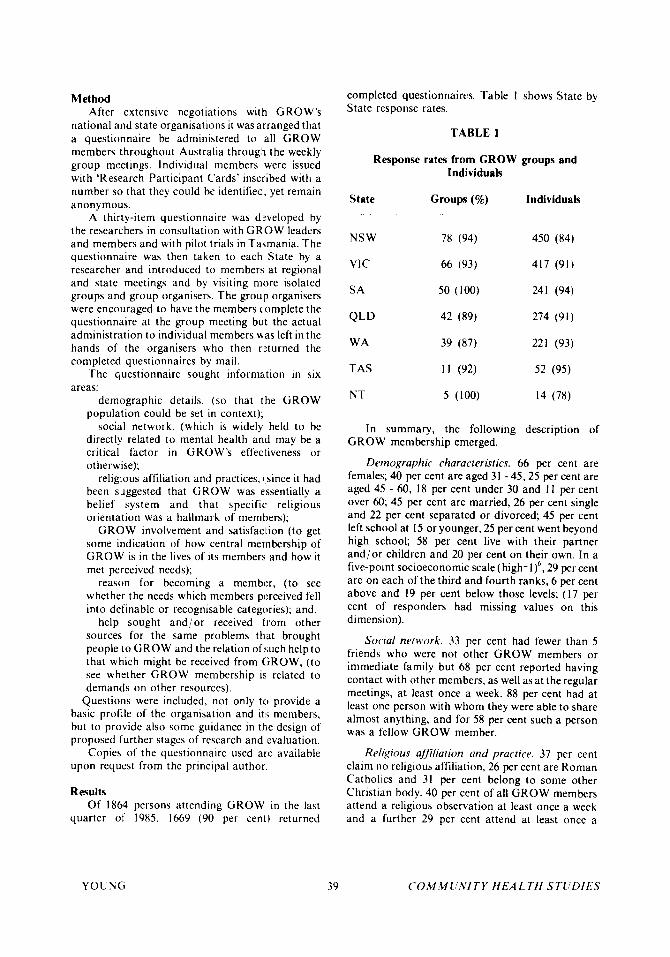
Results Of 1864 persons attending GROW in the last
quarter of' 1985, 1669 (90 per cent) returned
completed questionnaires. Table 1 shows State by State response rates.
TABLE 1
Response rates from GROW groups and Individuals
State Groups (%) Individuals __
NS W 78 (94) 450 (84)
VIC 66 (93) 417 (91)
SA 50 (100) 241 (94)
QLD 42 (89) 274 (91)
WA 39 (87) 221 (93)
TAS 11 (92) 52 (95)
NT 5 (100) 14 (78)
In summary, the following description of GROW membership emerged.
Demographic characteristics. 66 per cent are females; 40 per cent are aged 31 -45,25 per cent are aged 45 - 60, 18 per cent under 30 and 1 I per cent over 60; 45 per cent are married, 26 per cent single and 22 per cent separated or divorced; 45 per cent left school at 15 or younger, 25 per cent went beyond high school; 58 per cent live with their partner and/or children and 20 per cent on their own. In a five-point socioeconomic scale (highzlf , 29 per cent are on each of the third and fourth ranks, 6 per cent above and 19 per cent below those levels; (17 per cent of responders had missing values on this dimension).
Social neinork. 33 per cent had fewer than 5 friends who were not other GROW members or immediate family but 68 per cent reported having contact with other members, as well as at the regular meetings, at least once a week. 88 per cent had at least one person with whom they were able to share almost anything, and for 58 per cent such a person was a fellow GROW member.
Religious afjiliation and practice. 37 per cent claim no religious affiliation, 26 per cent are Roman Catholics and 31 per cent belong to some other Christian body. 40 per cent of all GROW members attend a religious observation at least once a week and a further 29 per cent attend at least once a
Y O U N G 39 C O j M M U N I T Y H E A L T H STlIDIE.7
month. Asked how religious-minded they considered themselves to be, 49 per cent thought they were about average, with 33 per cent rating themselves as more religious-minded than average, and 16 per cent less than average.
GROW involvement andsatisfaction. One third of all GROW members had been a member for two years or more, 47 per cent for less than a year and 9 per cent for less than a month. Most had heard of GROW from a friend (34 per cent) and 25 per cent had been referred by a helping professional. On a five-point scale, 93 per cent rated GROW as either “very helpful” or “extremely helpful” with the problem which brought them to GROW, and 78 per cent said that GROW had exceeded their expectations.
The following percentages checked specific forms of help received from GROW:
Saw others’ view 74 per cent Controlled feelings 72 per cent Gave sense of belonging 72 per cent Taught help for others 67 per cent Changed behaviour 66 per cent Felt less lonely 65 per cent
Felt less fearful Provided activity Other help Gave no help
54 per cent 44 per cent 16 per cent
1 per cent
Help from other sources. 80 per cent of members reported having sought professional help for the problems which brought them to GROW and40 per cent had sought help from sources other than professionals. 79 per cent had at some time taken medication to help with their problems. 46 per cent rated the help they received as helpful while 27 per cent said it made no difference and 8 per cent said it made matters worse.
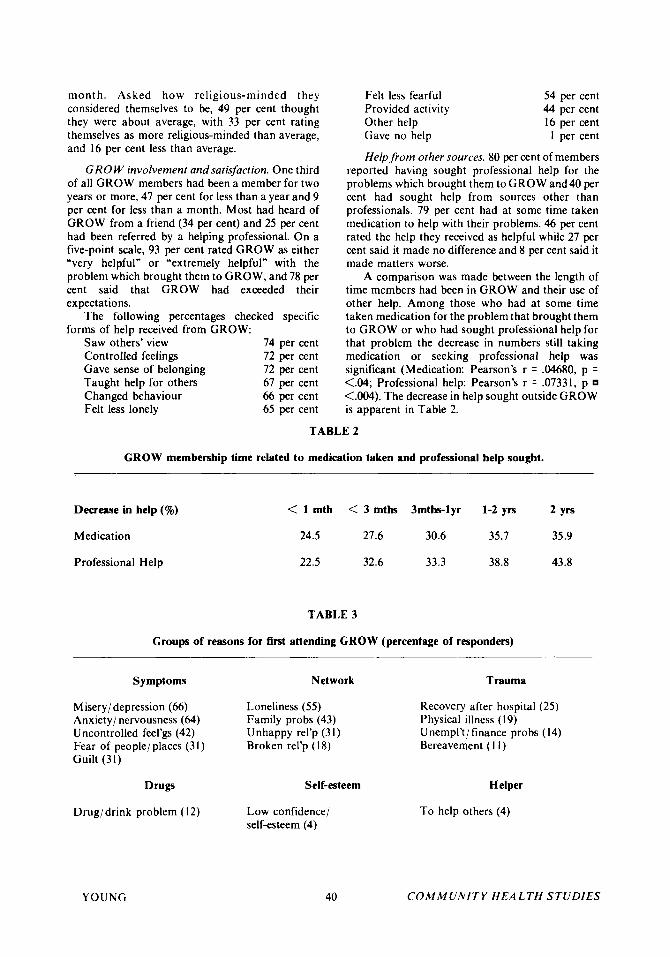
A comparison was made between the length of time members had been in GROW and their use of other help. Among those who had at some time taken medication for the problem that brought them to GROW or who had sought professional help for that problem the decrease in numbers still taking medication or seeking professional help was significant (Medication: Pearson’s r = .04680, p = <.04; Professional help: Pearson’s r = .07331, p <.004). The decrease in help sought outside GROW is apparent in Table 2.
TABLE 2
GROW membership time related to medication taken and professional help sought.
Decrease in help (9%) < 1 mth < 3 mths 3mths-lyr 1-2 yrs 2 yrs
Medication 24.5 27.6 30.6 35.7 35.9
Professional Help 22.5 32.6 33.3 38.8 43.8
TABLE 3
Groups of reasons for first attending GROW (percentage of responders)
Symptoms
Misery/ depression (66) Anxiety/ nervousness (64) Uncontrolled feel’gs (42) Fear of people/places (31) Guilt (31)
Drugs
Drugidrink problem (12)
YOUNG
Network Trauma
Loneliness ( 5 5 ) Family probs (43) Unhappy rel’p (31) Broken rel’p (18)
Recovery after hospital (25) Physical illness (19) Unempl’t/finance probs (14) Bereavement (1 1)
Self-esteem Helper
Low confidence/ self-esteem (4)
40
To help others (4)
COMMUNITY H E A L T H STUDIES
Rea.wns.for joining GROW. The reasons which members checked for joining GROW were grouped into categories relating to (a) psychological symptoms, (b) social network and relational problems, (c) adverse life events or trauma, (d) drug addiction or dependence, (e) probleins relating to low self esteem, and ( f ) attendance for the benefit of someone else. The percentage of responders checking items within these categories are shown in Table 3. An additional 9 per cent of responders gave a specified reason in an “other” category which did not readily fit into the above six.
Although respondents were invited to check any number of reasons for first joining GROW, almost half (816 of 1669) confined their response to one or other of these categories. Numbers of members who could be unequivocally assigned to a (,ategory were: symptom group, 433; network group, 21 I ; trauma group, 29; drug group, 23; self-esteem group, 59; helper group, 61.
Clearly, with only a proportion of the sample accounted for, a typological classification is not possible but factorial and cluster analyes are being undertaken to allow consideration of the total sample and further to define the characteristic sub- groups.
Discussion Having regard to the limitations of the
classification provided by our preliminary analysis noted above, the two major groups idcntified differ from each other in a number of ways. Of the ‘network’ group, fewer have seen professionals in dealing with their problems and those who have done so have rated the professional help they received as being less helpful than the ‘symptom’ group. More live on their own and report a smaller group of friends. However they sec GROW as providing a sense of belonging and GROW as providing an intimate ‘sharer’. The), have more contact with fellow members between formal meetings. O n the average they are younger than the ‘symptom’ group and, proportionate>y, more are men. Since becoming members of GROW they make less use of professional help anti medication than before, but this change is not as marked as that of other groups. They see themselves as less religious-minded than other groups. Within this group, those who came to GROW with a problem of loneliness or isolation tend to be youngx and with a larger proportion of men of lower socioeconomic status. A higher proportion of this subgroup still seek professional help concurrently with GROW membership and still use medication.
O n the other hand, the ‘symptom’ group are predominantly women of lower education standard
Y O U N ( i 41
and socioeconomic status. Most have had professional help and have taken medication for the problems that brought them to GROW, and, although they may still do so, the change toward fewer professional services and less taking of medication is significantly larger for this group. More than expected numbers of this group are referred to C R O W by professional workers. They tend to see professional help as more effective for them, particularly a sub-group who had been hospitalised before coming to GROW. Of the ‘symptoms’ reported as reasons for coming to GROW, rniseryidepression (66 per cent) and anxiety (64 per cent) were the most common complaints. However, people with these complaints reported significantly more help from GROW membership than others.
The most effective way in which the ‘symptom’ group is helped seems to be in the control of feelings and the reduction of irrational fear. This would imply more use by this group of the instructional program of GROW than use of the supportive network provided.
More than half of members who joined GROW with ‘symptom’ problems had been members for more than a year (54 per cent) compared with 38 per cent of the ‘network’ group. This is open to various interpretations, but on the face of it, it is surprising: one might have expected GROW to have provided the extended network for those with ‘network’ problems on an ongoing basis more than for those with ‘symptom’ problems. It may be, however, that ‘symptom’ problems require longer to be alleviated than ‘network’ problems.
From the reported data, GROW appears to be used by members in at least three distinct ways:
1. It provides a rational/ cognitive framework which may be useful particularly to those presenting with what we have called ‘symptoms’. This would appear to be by medium of what the GROW organisation refers to as the ‘GROW Program’.”.’’
2. It provides a supportive network and community which provides support itself but may also provide an educative function for those whose reason for seeking help we have called ‘network’.’.“’
3. It provides a sense of purpose and personal value in a measure to all groups: one of the most commonly listed types of help claimed to have been received in GROW was‘Taught me I could help others’ ~ 67 per cent of all respondents.x
N o clear conclusions as to the effectiveness of GROW can be drawn at this stage of the research. However there are two measures which provide
C O M M (INIT Y HEA L TH STC:UIES
some evidence of value. They are measures of change in the help sought from professional sources and the use of medication: for all members there is a significant negative relationship between the time in GROW and the use of these two outside types of help.
In this respect GROW appears to be similar to Recovery Inc., a mutual-help mental health organisation in the United States. Raiff'4 reported 39.1 per cent improvement in reduction of professional help sought and 49.1 per cent reduction in medication taken.
The advancement of community health standards demands an effective community-based system through which patients released from
institutional care may be reintegrated into their own community.5 A related need is for a service through which people suffering minor or transient mental or emotional disorders may be given support and encouragement to regain their health without resort to institutional care.15 Our initial research would suggest that GROW may provide for some people a means to meet either or both of these needs.
The descriptive study has given direction to the planned research into the process of GROW in which an attempt will be made to delineate more clearly the elements which provide the reported help. Further investigation is also planned to measure the efficacy of GROW in providing rehabilitation of the mentally i l l and the support of those suffering a wide range of emotional distress.
References
1 . Caplan G, Killilea M. (eds.). Support Systems and Mutual Help: Interdisciplinary Explorations. New York Grune & Stratton, 1976.
2. Liberman MA, Borman LD, (eds.) Self-Help Groups for Coping with Crisis. S a n Francisco: Jossey Bass, 1979.
3. Schulberg HC, Killilea M. (eds.). Modern Practice Community Mental Health. San Francisco: Jossey Bass, 1982.
4. Gartner A;Reissman F. (eds.). The Self Help Revolution. Vol X . Community Psychology Series. New York: Human Sciences Press Inc., 1984.
5 . Silverman PR. People Helping People: Beyond the Professional Model. In: Schulberg HC, Killilea M. (eds.). Modern Practice in Community Mental Health. San Francisco: Jossey Bass, 1982.
6. Dumont MP, Self-help treatment programs. A m J Psvchiatry 1974; 131(6):631-635.
7 . GROW. The Program of Growth to Maturity. Revised ed. Sydney: GROW Publications, 1982.
8 . Reissman F. The 'helper' therapy principle.
YOUNG 42
Social Work 1965; 10:27-32. 9. Gottleib BH (ed.). Social Networks and
Social Support. Beverly Hills: Sage, 198 I . 10. Weiss RS. Relationship of Social Support
and Psychological Well-being. In: Schulberg H C and Killilea M. (eds.). Modern Practice of Community Mental Health. S a n Francisco: J ossey Bass, 1982.
1 1 . Beck A. Cognitive Therapy and Emotional Disorders. New Y ork: Internat ional University Press, 1976.
12. M eichenbaum D . Cognitive-Behaviour Modification. New York: Plenum Press, 1977.
13. Power Daniel A. Privilege and Prestige: Occupations in Australia. Melbourne: Longman Cheshire, 1983.
14. Raiff NR. Some Health RelatedOutcomes of Self-Help Participation. In: Gartner A, Reissman F (eds.). The Self Help Revolution. Vol X , Community Psychology Series. New York: Human Sciences Press Inc, 1984.
15. Lieberman MA. Help Seeking and Self Help Groups. In: Lieberman MA, Borman LD. (eds.). Serf Help Groups for Coping nith Crisis. San Francisco: Jossey Bass, 1979.
C O M M U N I T Y H E A L T H STUDIES


















