
Rapid determination of aminoglycosides in pharmaceutical ...
Upload
juan-celis-salinasCategory
view
98download
4
Aminoglycosides:
Dosing and Duration of
Therapy
William A. Craig, MD
University of Wisconsin and
Wm S. Middleton Memorial VA Hospital
Madison, WI USA

Time Course of Antibacterial Activity of Tobramycin and Ticarcillin Against
Pseudomonas aeruginosa
Time (hours)
0 2 4 6
Log
CF
U p
er T
high
4.5
5.0
5.5
6.0
6.5
7.0
7.5
8.0
4 mg/kg
12 mg/kg
20 mg/kg
0 2 4
300 mg/kg
800 mg/kg
2400 mg/kg
Tobramycin Ticarcillin
Craig and Gudmundsson 1996
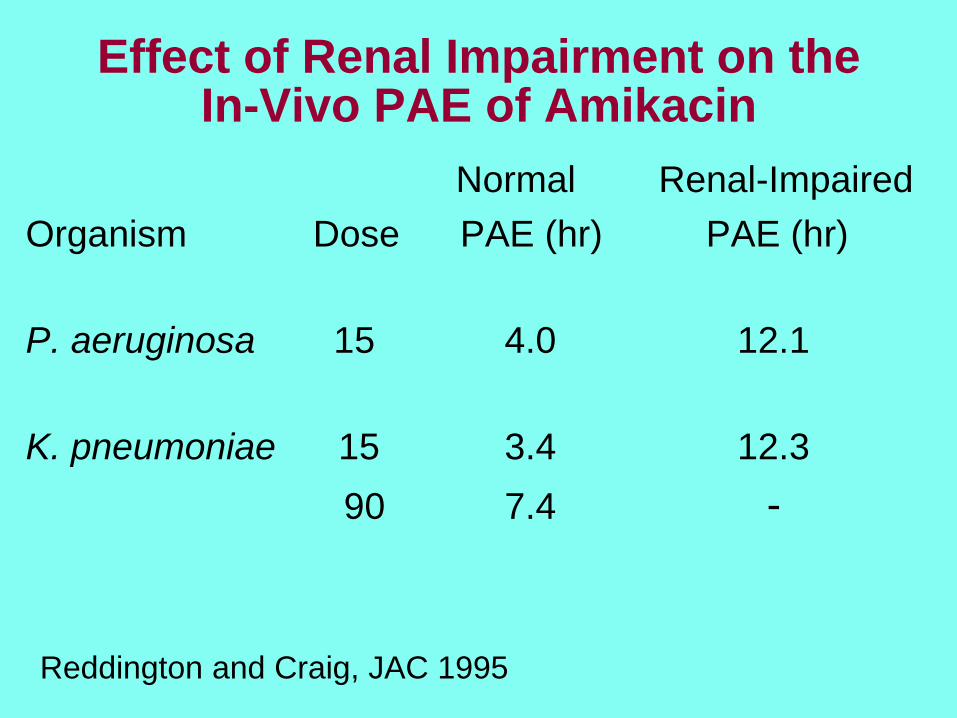
Effect of Renal Impairment on the In-Vivo PAE of Amikacin
Normal Renal-Impaired
Organism Dose PAE (hr) PAE (hr)
P. aeruginosa 15 4.0 12.1
K. pneumoniae 15 3.4 12.3
90 7.4 -
Reddington and Craig, JAC 1995
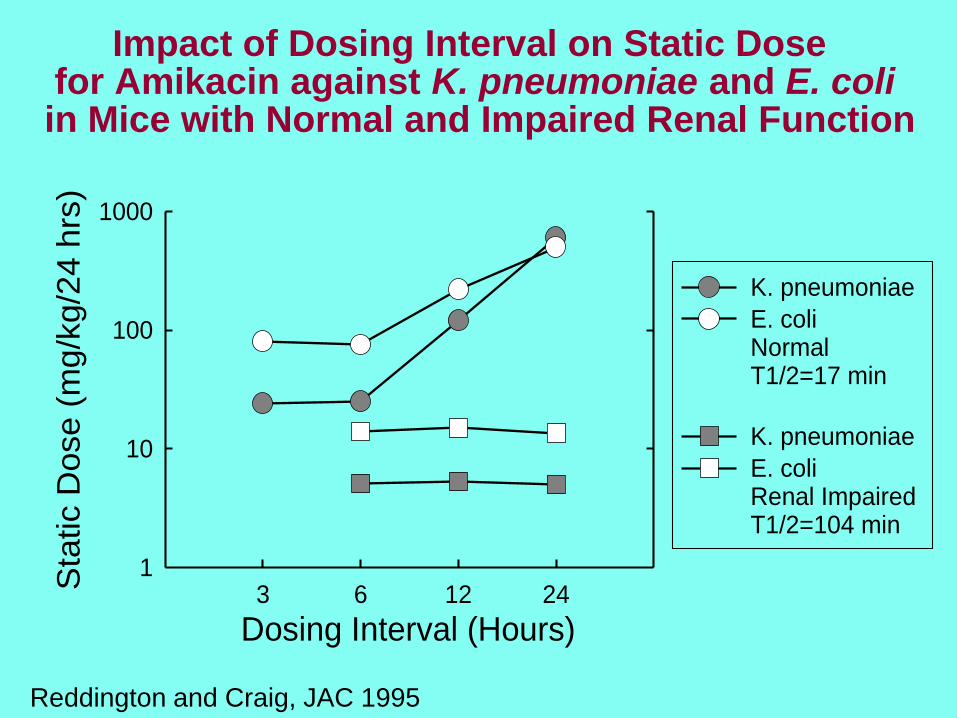
Impact of Dosing Interval on Static Dose for Amikacin against K. pneumoniae and E. coliin Mice with Normal and Impaired Renal Function
Dosing Interval (Hours)3 6 12 24
Sta
tic D
ose (
mg/k
g/2
4 h
rs)
1
10
100
1000
K. pneumoniae
E. coliNormal T1/2=17 min
K. pneumoniae
E. coliRenal Impaired T1/2=104 min
Reddington and Craig, JAC 1995
Major Goal of Pharmacodynamics
Establish the PK/PD TARGET required
for effective antimicrobial therapy
- identify which PK/PD indice (T>MIC,
AUC/MIC, peak/MIC) best predicts in
vivo antimicrobial activity
- determine the magnitude of the
PK/PD parameter required for in vivo
efficacy (static effect, 1 or 2 log kill)
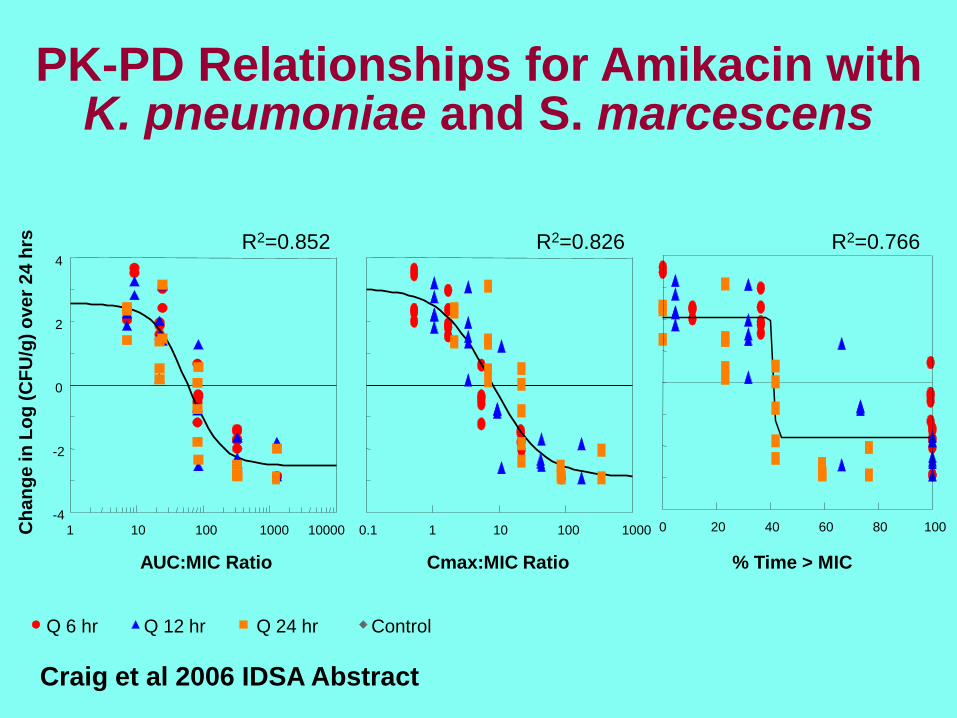
PK-PD Relationships for Amikacin with K. pneumoniae and S. marcescens
Q 6 hr Q 12 hr Q 24 hr Control
1 10 100 1000 10000-4
-2
0
2
4
AUC:MIC Ratio
Ch
an
ge
in
Lo
g (
CF
U/g
) o
ve
r 2
4 h
rs R2=0.852
0.1 1 10 100 1000
Cmax:MIC Ratio
R2=0.826
% Time > MIC
R2=0.766
0 20 40 60 80 100
Craig et al 2006 IDSA Abstract
PK/PD Indices: Aminoglycosides
AUC/MIC and Peak/MIC are important indices
determining efficacy of aminoglycosides in animal
infection models. A 24-hr AUC/MIC value of
100 along with a peak/MIC ratio 8-10 is
required for maximal efficacy.
A Peak/MIC ratio of 8-10 is required for 90%
efficacy in serious Gram-negative bacillary
infections in humans.
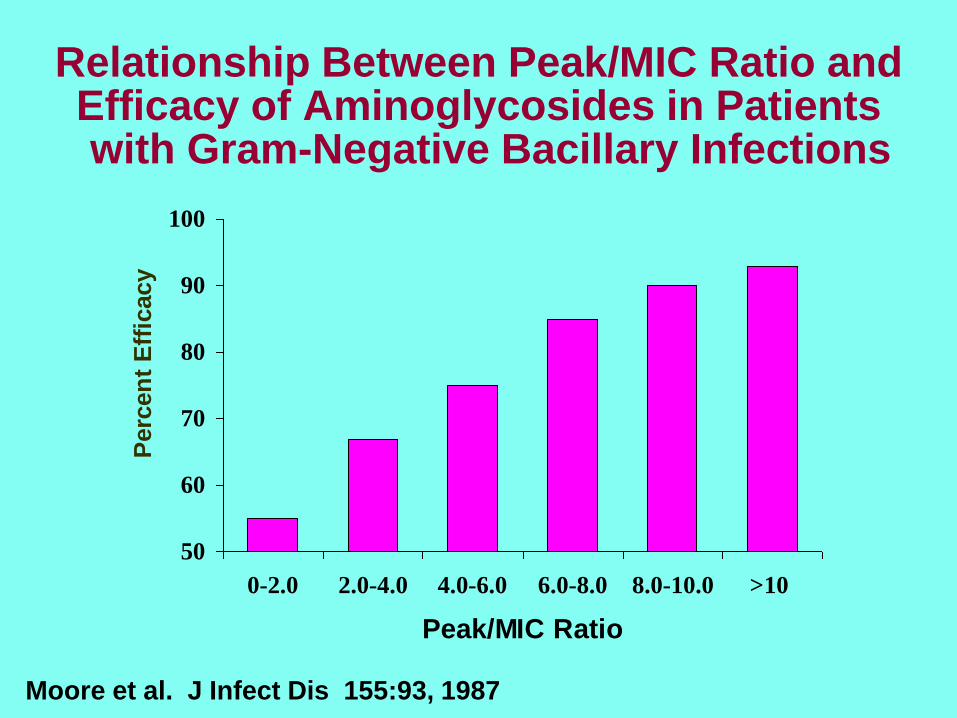
Relationship Between Peak/MIC Ratio and Efficacy of Aminoglycosides in Patientswith Gram-Negative Bacillary Infections
50
60
70
80
90
100
0-2.0 2.0-4.0 4.0-6.0 6.0-8.0 8.0-10.0 >10
Peak/MIC Ratio
P
erc
en
t E
ffic
acy
Moore et al. J Infect Dis 155:93, 1987
Efficacy of Tobramycin Monotherapy in Patients with Gram-Negative Bacillary
Infections
23 patients with nosocomial pneumonia or intra-abdominal infections
Clinical Cure
24 hr AUC/MIC > 110 80%
P<0.01 24 hr AUC/MIC < 110 47%
Smith et al. Clin Ther 2001; 23:1231

R²0.6451EXPOSURE & RESPONSE IN MAN
Tobramycin in Cystic Fibrosis Patients
Mouton JW, Jacobs N, Tiddens H, and Horrevorts AM. Pharmaco-
dynamics of tobramycin in patients with cystic fibrosis. Diagn Microbiol
Infect Dis. 2005;52:123-7.
R2=65% R2=60%
Optimizing Aminoglycosides for Nosocomial Pneumonia
Due to Gram-Negative Bacilli
• Study of 78 patients with nosocomial pneumonia
• Demonstrated a >90% probability of response in
fever and leukocytosis by 7 days if Cmax/MIC ratio
greater than or equal to 10
• Better correlation with peak/MIC than with AUC/MIC
Kashuba et al Antimicrob Agents Chemother 1999; 43:623
Aminoglycoside Monotherapy
• 27 trials in patients with urinary tract infections
aminoglycosides equally effective with competitors
• 9 trials in patients with non-urinary tract infections
higher rate of bacteriological failure with aminoglycosides
more nephrotoxic effects with aminoglycosides
Vidal et al. JAC 60:247, 2007
Combination vs Monotherapyfor Pseudomonas Bacteremia
• Prospective observational study of 200 cases
• 91% received appropriate antipseudomonal antibiotics: 70% combination
21% monotherapy
• Mortality: 27% combination therapy47% monotherapy
Hilfe et al, Am J Med 87:540, 1989
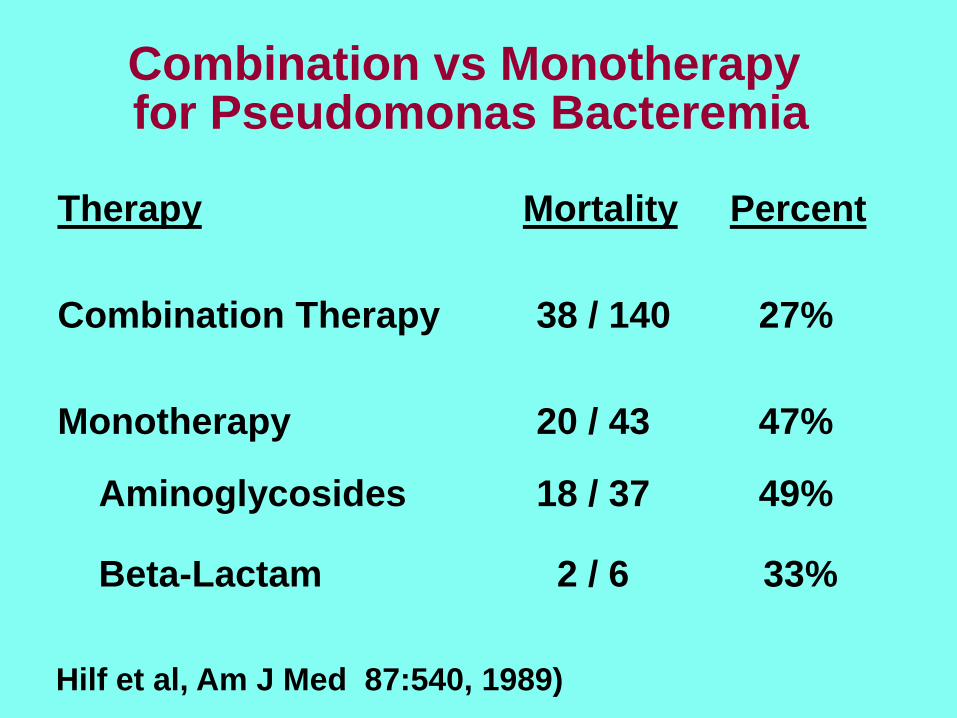
Combination vs Monotherapy for Pseudomonas Bacteremia
Therapy Mortality Percent
Combination Therapy 38 / 140 27%
Monotherapy 20 / 43 47%
Aminoglycosides 18 / 37 49%
Beta-Lactam 2 / 6 33%
Hilf et al, Am J Med 87:540, 1989)
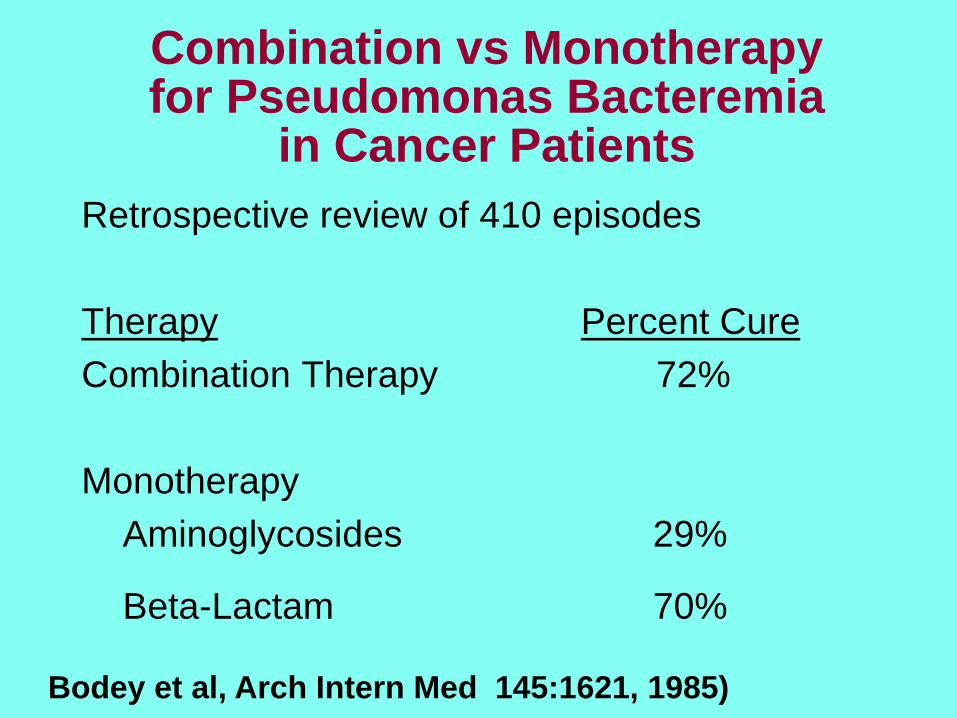
Combination vs Monotherapyfor Pseudomonas Bacteremia
in Cancer Patients
Retrospective review of 410 episodes
Therapy Percent Cure
Combination Therapy 72%
Monotherapy
Aminoglycosides 29%
Beta-Lactam 70%
Bodey et al, Arch Intern Med 145:1621, 1985)
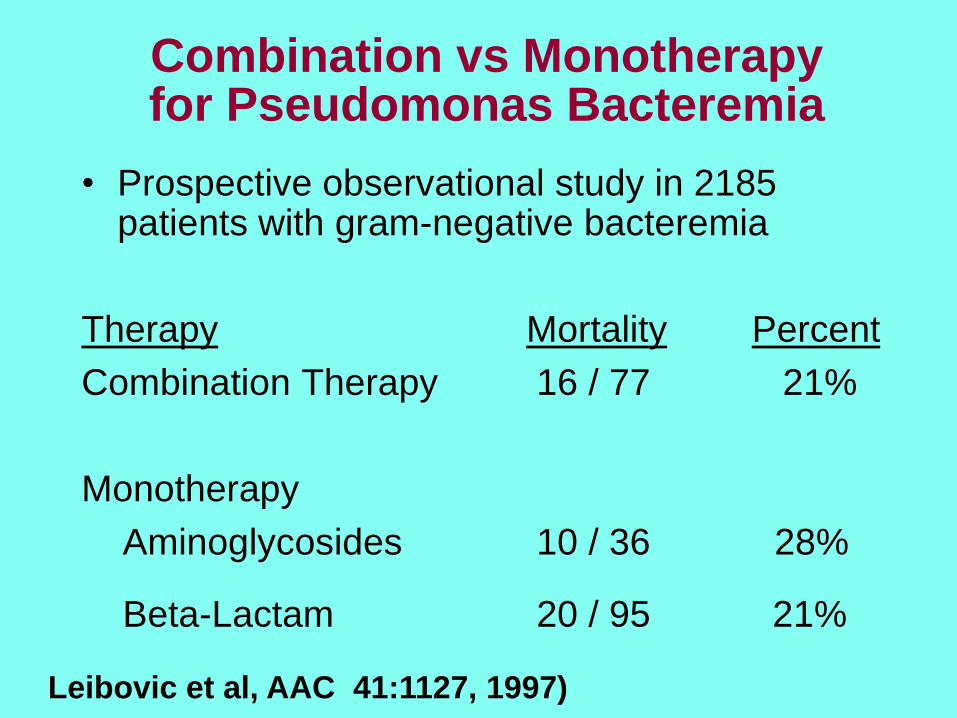
Combination vs Monotherapyfor Pseudomonas Bacteremia
• Prospective observational study in 2185 patients with gram-negative bacteremia
Therapy Mortality Percent
Combination Therapy 16 / 77 21%
Monotherapy
Aminoglycosides 10 / 36 28%
Beta-Lactam 20 / 95 21%
Leibovic et al, AAC 41:1127, 1997)
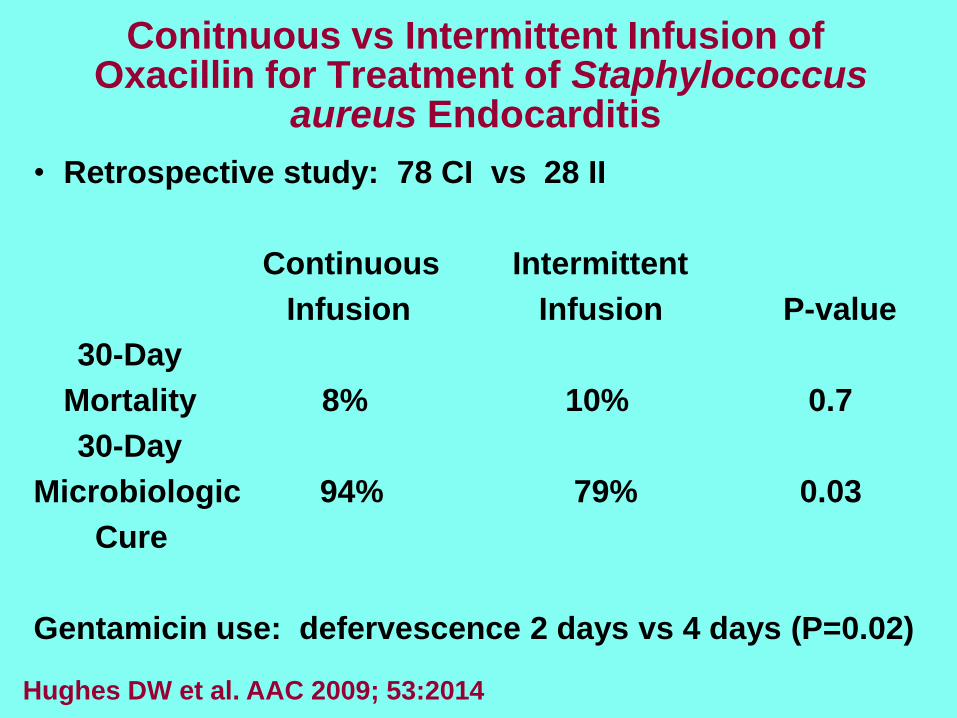
Conitnuous vs Intermittent Infusion of Oxacillin for Treatment of Staphylococcus
aureus Endocarditis
• Retrospective study: 78 CI vs 28 II
Continuous Intermittent
Infusion Infusion P-value
30-Day
Mortality 8% 10% 0.7
30-Day
Microbiologic 94% 79% 0.03
Cure
Gentamicin use: defervescence 2 days vs 4 days (P=0.02)
Hughes DW et al. AAC 2009; 53:2014

Once-Daily Dosing of Aminoglycosides
• 45 studies, mostly prospective, in over 6500 patients comparing once-daily with multiple daily dosing
• Slight non-significant enhancement in efficacy
• Of 9 meta-analyses (of different combinations of these 45 studies), 5 show a lower incidence of nephrotoxicity with once-daily dosing
Turnidge Inf Dis Clinics of N Amer 2003; 17:503
Aminoglycoside Nephrotoxicity
• Megalin is a lipoprotein on the brush border of renal tubular cells that binds aminoglycosides and is important for uptake of these drugs by pinocytosis
• Binding to megalin by aminoglycosides is saturable
• Animals deficient in megalin do not accumulate aminoglycosides in the kidney
• Once-daily dosing results in less uptake in human kidneys than thrice-daily or continuous infusion; nephrotoxicity occurs later with once-daily dosing –usually after 5-7 days; with longer courses the difference between regimens becomes smaller
Drug Metab Pharmacokin 2004;19:159; Rougier F et al AAC 2003; 47:1010
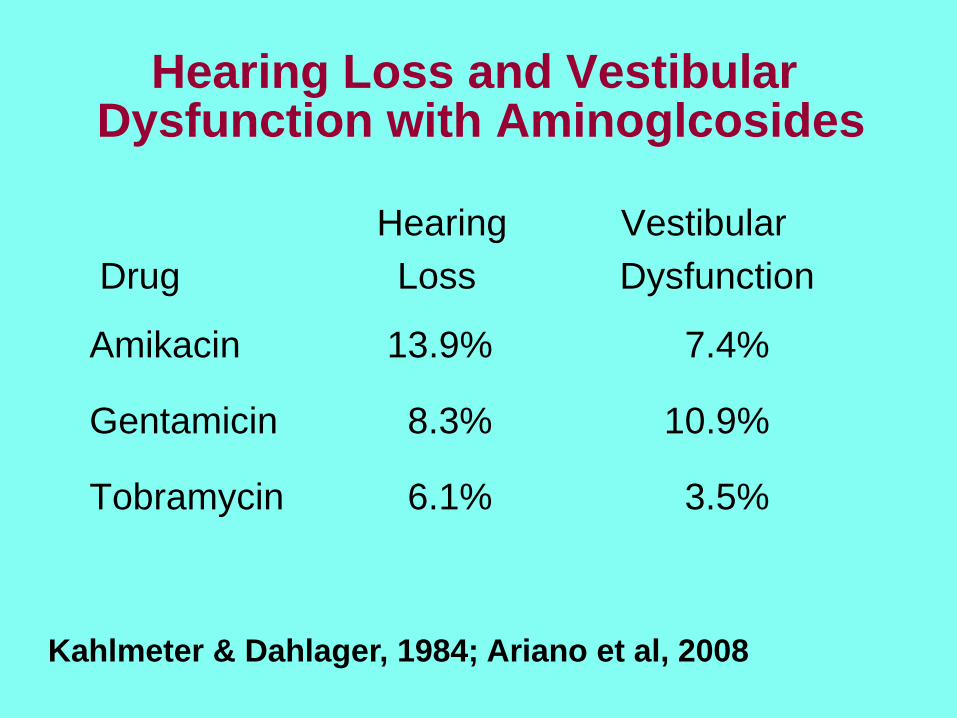
Hearing Loss and Vestibular Dysfunction with Aminoglcosides
Hearing Vestibular
Drug Loss Dysfunction
Amikacin 13.9% 7.4%
Gentamicin 8.3% 10.9%
Tobramycin 6.1% 3.5%
Kahlmeter & Dahlager, 1984; Ariano et al, 2008

Optimizing Use of Aminoglycosides
• Once daily treatment of 5-7 mg/kg (gentamicin, tobramycin) or 15-20 mg/kg (amikacin) for short periods (5-7 days)
• For non-urinary tract infections: Target attainment inadequate for monotherapy against organisms with MICs > 0.5 mg/L (gentamicin, tobramycin) or 2.0 mg/L (amikacin)
• Addition of aminoglycoside to ß-lactam rarely enhances efficacy except possibly for P. aeruginosa infections


















