AJOG+April June+2011+Issue
50
Volume : 2 April-June 2011
-
Upload
josefa-lucop-bentayen -
Category
Documents
-
view
61 -
download
3
description
obstetrics
Transcript of AJOG+April June+2011+Issue

Volume : 2 April-June 2011


Volume 2, April-June 2011
Online Submission
Contents
Asian Journal of
frOm the ISSue edItOr
Alka Kriplani 5
frOm the deSk Of GrOup edItOr-In-chIef
Emergency Contraception 6KK Aggarwal
clInIcAl Study
Outpatient Vaginal Administration of Isosorbide Mononitrate for Preinduction Cervical Ripening 7T Shubhamangala, Ramalingappa C Antaratani
Re-laparotomy after Cesarean Section - Our Experience in a Teaching Hospital of West Bengal 12Amitava Pal, Raghunath Bhattacharya Sudhir Adhikari, Anita Roy
A Study on Pregnancy-induced Acute Renal Failure 18AR Patel, PR Shah, Daniel P Sam, Anand IS, Gireesh MS
cASe repOrt
Management of Complex Vesicovaginal Fistulas: A Brief Report with Focus on Preventive Aspects 20 RB Singh, Satish Dalal, S Nanda
Hydatid Cyst Mimicking as Ovarian Tumor 24 Sumitra Yadav, HK Kansal, Anita Singh, Sanjay Patidar
Acute Pancreatitis Complicating Pregnancy with Severe Thrombocytopenia 29 Kurmapu Sandhya Rani
A Case of Abruption of the Succenturiate Lobe of Placenta 32 Amol Tilve, Roque Ribeiro
An IJcp Group publication
AJOG Speciality panelDr (Mrs) Prabha Arora (Delhi)Dr Hema Divakar (Bangalore)Dr Kamini A Rao (Bangalore)Dr Deepti Goswami (Delhi)Dr Neerja Bhatla (Delhi)Dr Bhawna Malhotra (Delhi)Dr Biswas Nicholas (Australia)Dr Sudhaa Sharma (Jammu)Dr Jaibhagwan Sharma (Delhi)Dr Veena Mathur (Agra)Dr Pradeep Garg (Delhi)
corporate panel
Dr Alka Kriplani editorconsultant editorDr Urmil SharmaAssistant editorsDr Nutan Agarwal (Delhi)Dr Neera Aggarwal (Delhi)Dr A Biswas (Singapore)Dr CS Dawn (Kolkata)Dr Gauri (Delhi)Dr Suneeta Mittal (Delhi)Dr S Mehra (Delhi)Dr Prashant Mangeshikar (Mumbai)Dr Prakash Trivedi (Mumbai)Dr Gita Ganguly Mukherjee (Kolkata)
Dr Sanjiv Chopra Prof. of Medicine & Faculty Dean
Harvard Medical SchoolGroup consultant editor
Dr Deepak Choprachief editorial Advisor
Dr KK Aggarwalcmd, publisher and Group editor-in-chief
Dr Veena AggarwalJoint md & Group executive editor
Anand Gopal Bhatnagar editorial Anchor
editorial Board
Advisory Body Heart Care Foundation of India
Non-Resident Indians Chamber of Commerce & IndustryWorld Fellowship of Religions
Dr Alka Kriplani Asian Journal of Obs & Gynae practice
Dr VP Sood Asian Journal of ear, nose and throat
Dr Praveen Chandra Asian Journal of clinical cardiology
Dr Swati Y Bhave Asian Journal of paediatric practice
Dr Vijay Viswanathan the Asian Journal of diabetology
Dr KMK Masthan Indian Journal of multidisciplinary dentistry
Dr M Paul Anand, Dr SK Parashar cardiologyDr CR Anand Moses Dr Sidhartha Das Dr A Ramachandran Dr Samith A Shetty diabetologyDr Ajay Kumar GastroenterologyDr Koushik Lahiri dermatologyDr Georgi Abraham nephrologyDr Sidharth Kumar Das rheumatology
Dr V Nagarajan neurology
Dr Thankam Verma, Dr Kamala Selvaraj Obs and Gyne

editorial policies
The purpose of IJCP Academy of CME is to serve the medical profession and provide print continuing medical education as a part of their social commitment. The information and opinions presented in IJCP group publications reflect the views of the authors, not those of the journal, unless so stated. Advertising is accepted only if judged to be in harmony with the purpose of the journal; however, IJCP group reserves the right to reject any advertising at its sole discretion. Neither acceptance nor rejection constitutes an endorsement by IJCP group of a particular policy, product or procedure. We believe that readers need to be aware of any affiliation or financial relationship (employment, consultancies, stock ownership, honoraria, etc.) between an author and any organization or entity that has a direct financial interest in the subject matter or materials the author is writing about. We inform the reader of any pertinent relationships disclosed. A disclosure statement, where appropriate, is published at the end of the relevant article.
note: Asian Journal of Obs & Gynae practice does not guarantee, directly or indirectly, the quality or efficacy of any product or service described in the advertisements or other material which is commercial in nature in this issue.
published, printed and edited byDr KK Aggarwal, on behalf of
IJCP Publications Pvt. Ltd. and Published at
E - 219, Greater Kailash, Part - 1, New Delhi - 110 048E-mail: [email protected]
printed at IG Printers Pvt. Ltd., New DelhiE-mail: [email protected]
© copyright 2011 IJcp publications pvt. ltd. All rights reserved.
The copyright for all the editorial material contained in journal, in the form of layout, content including images and
design, is held by IJCP Publications Pvt. Ltd. No part of this publication may be published in any form whatsoever without
the prior written permission of the publisher.
Volume 2, April-June 2011
Contents
edItOrIAl & BuSIneSS OffIceSdelhi mumbai kolkata Bangalore chennai hyderabad
Dr Veena Aggarwal9811036687
E - 219, Greater Kailash, Part - I,
New Delhi - 110 048 Cont.: 011-40587513
[email protected]@gmail.com
SubscriptionDinesh: [email protected]: 09831363901
Dr Veena Aggarwal9811036687
Building No - D 10 Flat No - 43, 4th Floor Asmita Co-operative
Housing Society Near Charkop Naka
Marvey Road Malad (W)
Mumbai 400 [email protected]
Sr. BmRitu Saigal
9831363901Flat 5E,
Merlin Estate Geetanjali
25/8 Diamond Harbour Road
Kolkata - 700 008 Cont.: 24452066
Sr. BmH Chandrashekar
9845232974Arora Business Centre, 111/1 &
111/2, Dickenson Road (Near Manipal
Centre)Bangalore - 560 042
Cont.: 25586337 [email protected]
Sr. BmChitra Mohan9841213823
40A, Ganapathy-puram
Main Road Radhanagar Chromepet
Chennai - 600 044Cont.: 22650144 [email protected]
Sr. Bm Venugopal
9849083558H. No.
16-2-751/A/70 First Floor
Karan Bagh Gaddiannaram Dil Sukh Nagar
Hyderabad - 500 059
Cont.: [email protected]
Sr.: Senior; BM: Business Manager
Asian Journal of
cASe repOrt
Umbilical Endometriosis: A Rare Cutaneous Endometriosis 37 Debasmita Mandal, Nibedita Chattopadhaya, Raj Shekhar Sarkar, Hena Kausar, Sougata Banerjee, Ratna Deep Ganguli
Rarity but Reality: A Rare Presentation of Granulosa Cell 40 M Sivasundari, Ravi Kumar Barua, Arunita Nandy
emedInewS SectIOn
From eMedinewS 43
phOtO quIz
Nutan Agarwal 45
flOw chArt
Polycystic Ovarian Syndrome with Infertility: Evidence-based Management 47 Garima Kachhawa, Alka Kriplani

�Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
Dear Reader,
This issue is a testimony of our commitment to disseminate recent and important information in the fast progressing field of Obstetrics and Gynecology. Liberalization of cesarean section operation has led to increased incidence of cesarean section. Sometimes unacceptably high cesarean rates are reported in different patient populations. It is a major surgery and is associated with certain risks and complications. Complication rate depends on indication of operation also. One of the important complications is need to perform re-laparotomy after cesarean section. The article by Dr Pal presents in detail their experience on cases of ‘Re-laparotomy after cesarean section’ from a teaching hospital in West Bengal.
Pregnancy-related acute renal failure is not an uncommon problem especially in the developing countries. An article titled ‘A study on pregnancy-induced acute renal failure’ highlights the etiological factors and clinical outcome in their patients of acute renal failure of obstetrical origin.
Vesicovaginal fistula because of neglected and obstructed labor is a very rare entity in the developed world, although with improving obstetrical services its incidence is becoming less in our country also, but we still get such cases from time to time. An article on ‘Management of complex vesicovaginal fistula’ beautifully presents the etiological factors as well as different surgical techniques used for their repairs.
The need to ripen the cervix prior to induction of labor cannot be overemphasized in order to achieve high success for induction of labor. Various drugs are available and have been tried for the same. The article by Dr Shubhamangala and Ramalingappa presents their experience with isosorbide mononitrate for this indication.
The present issue also contains our regular columns like Interesting Case Reports, Flow Chart, eMedinewS Section and Photo Quiz.
I am sure this issue will make for an interesting and informative reading.
n n n
Dr Alka KriplaniProfessor and Head of Unit IIDept. of Obstetrics and GynecologyAIIMS, New DelhiE-mail: [email protected]
from the issue editor

� Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
There are no medical contraindications to the use of emergency contraception. Neither a physical examination nor laboratory testing is needed before prescribing oral emergency contraception. Administer emergency contraception as soon as possible, but upto 120 hours, after an episode of unprotected intercourse in
women who wish to prevent pregnancy. When a copper intrauterine device is used, the window can be extended to five days after presumptive ovulation. Given the uncertainty in timing of ovulation, emergency contraception is offered, when indicated, without regard to day of the menstrual cycle. One should use levonorgestrel rather than an estrogen-progestin regimen because it is more effective and has fewer side effects.
One should use levonorgestrel 1.5 mg. Use ulipristal for women who request emergency contraception at any time within 120 hours, but in particular after 72 hours after unprotected intercourse. A routine follow-up office visit is not required after taking emergency contraception. Menstrual bleeding after oral hormonal emergency contraception typically occurs within one-week of the expected time. A pregnancy test should be performed if bleeding has not occurred within 3-4 weeks or if there is persistent vaginal bleeding or abdominal pain.
Women using emergency contraception pills should be advised that a risk of pregnancy still exists if they have unprotected sexual intercourse after emergency contraception pills have been taken. A repeat course of emergency contraception can be given, but it is preferable that they begin regular use of nonemergency contraception, which can be initiated the day after emergency contraception administration.
Give women a home supply of emergency contraceptives or encourage them to buy them in advance.
Women 16 and under can be given a prescription for emergency contraception in advance.
In August 2010, the US Food and Drug Administration approved the progesterone receptor modulator ulipristal for emergency contraception. As with oral levonorgestrel or oral ethinyl estradiol-levonorgestrel, it can be used for upto 120 hours after unprotected intercourse. In contrast to these regimens, it requires a prescription and may be more effective in women who seek emergency contraception 72-120 hours after unprotected intercourse.
Suggested Reading 1. Glasier AF, Cameron ST, Fine PM, Logan SJ, Casale W, Van Horn J, et al. Ulipristal acetate versus levonorgestrel for
emergency contraception: a randomised non-inferiority trial and meta-analysis. Lancet 2010;375:555-62.
n n n
Dr KK AggarwalPadma Shri and Dr BC Roy National AwardeeSr Physician and Cardiologist, Moolchand MedcityPresident, Heart Care Foundation of IndiaGroup Editor-in-Chief, IJCP GroupEditor-in-Chief, eMedinewSChairman Ethical Committee, Delhi Medical CouncilDirector, IMA AKN Sinha Institute (08-09)Hony. Finance Secretary, IMA (07-08)Chairman, IMA AMS (06-07)President, Delhi Medical Association (05-06)[email protected] http//twitter.com/DrKKAggarwalKrishan Kumar Aggarwal (Facebook)
from the desk of group editor-in-chief
Emergency Contraception

�Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
AbstrAct
Objective: The aim of the study was to determine whether isosorbide mononitrate (ISMN) 60 mg administered vaginally is effective for preinduction cervical ripening on an outpatient basis. Methods: The study was carried out at Karnataka Institute of Medical Sciences, Hubli from November 2007 to October 2008. Hundred women with singleton pregnancies with Bishop score ≤6 were randomized to receive either ISMN slow-release (ISMN-SR) 60 mg or vitamin C vaginally on an outpatient basis. Bishop score, proportions establishing spontaneous labor were assessed after 48 hours. Requirement of additional cervical ripening agent, need for oxytocin, admission-delivery interval, neonatal outcome (Apgar score 5 minutes, neonatal intensive care unit [NICU] admission and meconium stained liquor) and side effects were compared. Results: In ISMN-SR group, there was a marked increase in the proportion of women establishing spontaneous labor (36% vs 12%) and being favorable for induction of labor (40% vs 9.09%). There was a significantly higher Bishop score (6.76 ± 2.65 vs 4.6 ± 2.17) and decrease in proportion of subjects requiring further ripening (38% vs 80%). Admission-delivery interval was shorter in ISMN group (p < 0.001). There were no significant differences in mode of delivery and fetal distress. Headache was seen in 22% of women in the ISMN group (p < 0.01). Conclusion: ISMN administered vaginally is effective for preinduction cervical ripening.
Key words: Outpatient cervical ripening, isosorbide mononitrate, nitric oxide
Outpatient Vaginal Administration of Isosorbide Mononitrate for Preinduction Cervical Ripeningt Shubhamangala*, ramalingappa c Antaratani**
*Assistant ProfessorDept. of Obstetrics and GynecologyVydehi Institute of Medical Science and Research Centre, Bangalore**ProfessorDept. of Obstetrics and GynecologyKarnataka Institute of Medical Science, HubliAddress for correspondenceDr T ShubhamangalaAssistant ProfessorDept. of Obstetrics and GynecologyVydehi Institute of Medical Science and Research Centre, BangaloreE-mail: [email protected]
Before the onset of labor, the cervix usually undergoes a process called ‘ripening’, in which it softens, dilates and effaces. These changes
result in substantially decreased cervical resistance to labor pains. Sometimes, it is necessary to bring on labor artificially because of safety concerns for the mother or baby. Labor induction, when performed in a woman with unripe cervix often results in prolonged and difficult labor. Failed induction, secondary to ineffective labor or excessive uterine activity causing fetal distress are the main problems resulting in increased risk of cesarean delivery.
Nitric oxide (NO) is produced through NO synthetase (NOS) which is expressed in three isoforms: Neuronal, inducible and endothelial NOS1, all of which are
present in the various cells of the uterine cervix.2-4 The expression of NOS isoforms and the release of NO in the cervix have been shown to increase with advancing gestational age and during cervical ripening. Since, it does not cause uterine contractions, it may be suitable for outpatient use as against prostaglandins.
An ideal cervical ripening agent would induce ripening without causing contractions, since the lack of uterine contractions obviates fetal monitoring; such an agent could be used on an outpatient basis. There is increasing interest in carrying out cervical ripening on an outpatient basis, advantages of which are - patient convenience and reduced hospitalization costs. There is increasing interest in outpatient cervical ripening which is driven at least in part by financial costs associated with an inpatient stay in the labor ward. Additionally, there is a wish to ‘deinstitutionalize’ the process of labor, and, where appropriate, to offer women the opportunity to remain as an outpatient for a longer period of time.
The present study was conducted to determine the efficacy of NO donor: Isosorbide mononitrate (ISMN), as a preinduction cervical ripening agent on an outpatient basis.
clinicAl study

� Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
clinicAl study
Material and Methods
This study was carried out in Karnataka Institute of Medical Sciences, Hubli during the period from November 2007 to October 2008. It included 100 patients with various indications for induction of labor with unripe cervix.
Study design: Randomized stratified (nulliparous/multiparous), placebo-controlled study. Active placebo treatment was allocated in a 1:1 ratio.
Each of the women selected had been subjected to detailed history, general and abdominal examination. Vaginal examination was done to examine the bony pelvis and to detect cervical score. Inducibility was predicted using the Bishop pelvic scoring system. Ultrasound examination was done to assess fetal viability, lie, presentation, position, fetal weight, fetal number, amniotic fluid volume, placental location and fetal well-being.
Indications for induction of labor were according to hospital protocols. Common indications for induction were to be postdated pregnancies, pregnancy-induced hypertension, intra-uterine growth restriction, Rh-isoimmunization, fetus with major congenital anomaly, intrauterine death of fetus, etc.
Pregnant women were eligible for enrollment if they were: Between 37 and 43 week’s gestation, singleton pregnancy with the fetus in cephalic presentation, unfavorable cervix, (defined as a Bishop score ≤6), had intact membranes and willing to participate in the study. Exclusion criteria were: Cephalopelvic disproportion (CPD), previous uterine scar, nonvertex presentation, multifetal pregnancy, significant vaginal bleeding, chorioamnionitis, severe pre-eclampsia, uncontrolled diabetes mellitus, contraindication to receive prostaglandins or NO (history of hypersensitivity, heart disease, glaucoma or asthma), prelabor rupture of membranes, established fetal distress, fetal compromise of sufficient degree that daily fetal monitoring is scheduled.
Eligible patients were taken for study. Procedure having been explained and having obtained their written consent for participation, subjects were randomly divided into two groups. The first group (A) consisted of 50 cases that used 60 mg ISMN tablet introduced into posterior vaginal fornix. The second group (B)
consisted of 50 cases used as a placebo vitamin C tablet applied into posterior vaginal fornix. Subjects were examined after 48 hours or earlier if they came with any complaints. Cervix was defined as ripe if Bishop score was >6. After assessment of Bishop score, subjects received inpatient cervical ripening if Bishop score was ≤6 and oxytocin drip if Bishop score was >6. Cervical ripening was done with misoprostol 25 µg placed in posterior vaginal fornix every six hours till Bishop score was >6. After that cervical score and depending on the uterine contraction frequency and duration, augmentation with oxytocin was done. If the cervical score was >6, augmentation of labor was done by oxytocin drip. When regular uterine contractions with a favorable cervix and a well-fitted vertex, amniotomy was performed. Intrapartum monitoring was continued. Failed labor induction was defined as the inability to achieve a cervical dilation of 4 cm and 90% effacement, or at least 5 cm (regardless of effacement) after a minimum of 12-18 hours of membrane rupture and oxytocin administration (with a goal of 250 MU or 5 contractions/10 minutes). Favorable cervix was defined as Bishop score of >6. Cesarean section was done for obstetric indications and documented. Mode of delivery and neonatal outcome were recorded with respect to meconium staining, Apgar score at one minute and five minutes and admission to neonatal intensive care unit (NICU). Indications for operative deliveries were documented. The analytic statistics was performed using the unpaired student test. To compare two rates or percentages, chi-square test was used. Fisher’s test was if numbers in the contingency table were very small (<5).
Results
The clinical characteristics for women in both groups were comparable as regards to clinical criteria namely: Maternal age, parity, gestational age and initial Bishop score with no significant difference between both groups (p > 0.05) as shown in Table 1. Indications for induction of labor were presented in Table 2. There were 34% unscheduled admissions in cases and 16% in controls (p < 0.001). Significant number of women in ISMN-treated group went into spontaneous labor <48 hours in cases (13 [26%] vs 5 [10%]) (Table 3). Cases had improved Bishop score (6.76 ± 2.65 vs 4.6 ± 2.18, p < 0.001), change in Bishop score (4.36 ± 2.83 vs

�Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
clinicAl study
2 ± 2.24, p < 0.001) as well as favorable Bishop score at 48-hour/next visit (31 vs 10, p < 0.001).
The number of doses of additional cervical ripening was higher with controls (38% vs 80%, p < 0.05). Inpatient induction/admission in labor to delivery was shorter in cases than controls (9.21 ± 4.55 hours vs 12.9 ± 4.65 hours, p < 0.001). There were no differences in duration of first, second and third stages of labor. Also, no differences were observed between both groups regarding the mode of delivery, for indications for operative delivery as well as fetal outcomes in both groups as found through Apgar score, meconium stained liquor or admissions to NICU. Table 4 demonstrates maternal and fetal side effects and their incidence among both groups. Headache was more common in ISMN group (22% vs 4%, p < 0.05).
Discussion
The need to ripe the cervix prior to induction of labor has become a reality in our lives as induction especially with unfavorable cervix in a full term pregnancy is still a problem to the obstetricians. NO donors were tried for the first time before
surgical evacuation of the first trimester pregnancy’ in the form of vaginal tablet by Thomson et al5 and intracervically by Arteaga-Troncoso et al.6
The results from the current study show that ISMN is an efficient cervical ripening agent compared to placebo; especially on an outpatient basis. In ISMN group, there was increase in the proportion of women establishing spontaneous labor and having Bishop score favorable for induction of labor. In present study, in ISMN group there was a significantly higher Bishop score at 48-hour (6.76 ± 2.65 vs 4.6 ± 2.17, p < 0.001), a higher change in score (4.36 ± 2.83 vs 2 ± 2.24, p < 0.001) and decrease in proportion of subjects requiring further ripening (38% vs 80%, p < 0.001) (Table 3). In those who needed inpatient cervical ripening, doses in ISMN-treated group were less than in placebo-treated. Similar response was seen by Rameez et al7 where proportion establishing spontaneous labor was (28% vs 7.5%), score being favorable for induction of labor was (40% vs 9%), an increase in Bishop score (3.8 vs 1.3) and need for additional cervical ripening was seen in 32% versus 79% in placebo group. Admission to delivery interval was shorter in ISMN group in the present study (9.21 ± 4.65 hours vs 12.91 ± 4.55 hour, p < 0.001).
No significant differences in cesarean delivery rates including any differences in fetal outcomes and admissions to intensive care unit were noted in the present study. Headache was the main side effect seen in 22% of women in the ISMN group but was not so severe to need analgesia. However, in the present study, women who had headache did not feel it to be significant.
table 1. Clinical Characteristics of Women in Study Groupclinical characteristics ISmn group (n = 50) placebo group (n = 50) p value Significancematernal age (years)Range 18-29 18-29 >0.05 Not significantMean ± SD 23.12 ± 2.82 23.08 ± 2.78 >0.05 Not significantGestational age (days)Range 273-299 270-303 >0.05 Not significantMean ± SD 286.56 ± 5.89 286.28 ± 8.59 >0.05 Not significantBishop scoreRange 1-4 1-5 >0.05 Not significantMean ± SD 2.369 ± 0.72 2.62 ± 0.9 >0.05 Not significantISMN = Isosorbide mononitrate, n = Number of subjects
table 2. Indications for Induction of LaborIndications for labor induction
case (n = 50)
control (n = 50)
total
Postdated pregnancy 33 (66%) 25 (50%) 68 (68%)
Pre-eclampsia 12 (24%) 22 (44%) 34 (34%)
Oligohydramnios 5 (10%) 3 (6%) 8 (8%)
Others - - -

10 Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
clinicAl study
table 3. Comparison Between Study Groups
case (n = 50) control (n = 50) p value Significance
Unscheduled admissions 17 (34%) 8 (16%) <0.001 Significant
Unscheduled admissions for cause other than labor 4 (8%) 3 (6%) >0.05 Not significant
Established labor (<48 hour) 13 (26%) 5 (10%) <0.05 Significant
Established labor (≥48%) 5 (10%) 1 (2%) >0.05 Not significant
Bishop score at 48-hour/next visit
Range 3-12 2-12 <0.001 Significant
Mean ± SD 6.76 ± 2.65 4.6 ± 2.18
Change in Bishop score at 48-hour/next visit
Range 0-10 0-10 <0.001 Significant
Mean ± SD 4.36 ± 2.83 2 ± 2.24
Favorable score (>6) 31 (62%) 10 (20%) <0.001 Significant
Unfavorable score (≤6) 19 (38%) 40 (80%) <0.001 Significant
Bishop score favorable for induction with oxytocin 13 (40.6%) 4 (9.09%) <0.001 Significant
Women who needed inpatient cervical ripening 19 (38%) 40 (80%) <0.001 Significant
Requirement of oxytocin 47 (94%) 47 (94%) >0.05 Not significant
Duration from inpatient induction/admission in labor to delivery
Range 1.66-20.91 hours 1-23 hours <0.001 Significant
Mean ± SD 9.21 ± 4.55 hours 12.9 ± 4.65 hours
Duration of first stage
Mean ± SD 6.193 ± 2.6 hours 5.7 ± 2.3 hours >0.05 Not significant
Duration of second stage
Mean ± SD 41.3 ± 19.9 minutes 40.42 ± 20.3 minutes >0.05 Not significant
Duration of third stage
Mean ± SD 6.58 ± 3.98 minutes 5.88 ± 3 minutes >0.05 Not significant
Normal vaginal delivery 40 (80%) 42 (84%) >0.05 Not significant
Operative vaginal delivery 3 (6%) 2 (4%) >0.05 Not significant
Cesarean section 7 (14%) 6 (12%) >0.05 Not significant
Apgar score 1-minute
Range 4-9 4-9
Mean ± SD 7.88 ± 0.93 7.38 ± 1.08 >0.05 Not significant
Apgar score 5 minute
Range 7-10 6-10
Mean ± SD 9.62 ± 0.69 9.34 ± 0.96 >0.05 Not significant
Thick meconium 2 (4%) 4 (8%) >0.05 Not significant
Thin meconium 11 (22%) 12 (24%) >0.05 Not significant
Admissions to NICU 1 (2%) 4 (8%) >0.05 Not significant

11Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
clinicAl study
Conclusion
To summarize, it was found from the study that ISMN was more effective than placebo with respect to number of women going into spontaneous labor, improvement in cervical score, favorability for induction of labor, admission to delivery interval and reduced the number of doses of inpatient cervical ripening agent without increasing cesarean delivery rate and affecting neonatal outcomes.
However, following are the drawbacks of the study: 1) ISMN tablets intended for oral administration were administered vaginally. NO donors in vaginal paste or gel form may allow better drug absorption. 2) Study population is less. The definitive clinical efficacy needs to be evaluated in larger series of patients.
Use of NO donor, ISMN may have the major advantage that uterine contractions are not stimulated and may allow cervical ripening before induction of labor to be performed as an outpatient procedure. The use of NO donors for the induction of cervical ripening at term may prove to be a major therapeutic advance.
AcknowledgementWe thank Dr US Hangaraga, MD, OBG Professor and Head of the department, Karnataka Institute of Medical Sciences, Hubli for constant support and allowing for the study the department. All staff members and postgraduates of Dept. of OBG, Karnataka Institute of Medical Sciences, Hubli for their co-operation.
References1. Alderton WK, Cooper CE, Knowles RG. Nitric
oxide synthases: structure, function and inhibition. Biochem J 2001;357:593-615.
2. Tschugguel W, Schneeberger C, Lass H, Stonek F, Zaghula MB, Czerwenka K, et al. Human cervical ripening is associated with an increase in cervical inducible nitric oxide synthase expression. Biol Reprod 1999;60(6):1367-72.
3. Ledingham MA, Thomson AJ, Young A, Macara LM, Greer IA, Norman JE. Changes in the expression of nitric oxide synthase in the human uterine cervix during pregnancy and parturition. Mol Hum Reprod 2000; 6(11):1041-8.
4. Bao S, Rai J, Schreiber J. Brain nitric oxide synthase expression is enhanced in the human cervix in labor. J Soc Gynaecol Investig 2001;8(3):158-64.
5. Thomson AJ, Lunan CB, Cameron AD, Cameron IT, Greer IA, Norman JE. Nitric oxide donors induce ripening of the human uterine cervix: a randomized controlled trial. Br J Obstet Gynaecol 1997;104(9):1054-7.
6. Arteaga-Troncoso G, Villegas-Alvarado A, Belmont-Gomez A, Martinez-Herrera FJ, Villagrana-Zesati R, Guerra-Infante F. Intracervical application of the nitric oxide donor isosorbide dinitrate for induction of cervical ripening: a randomized controlled trial to determine clinical efficacy and safety prior to first trimester surgical evacuation of retained products of conception. BJOG 2005;112(12):1615-9.
7. Rameez MF, Goonewardene IM. Nitric oxide donor isosorbide mononitrate for pre-induction cervical ripening at 41 weeks’ gestation: a randomized controlled trial. J Obstet Gynaecol Res 2007;33(4)452-6.
n n n
table 4. Complications Seen in Both Groupscase control p value Interpretation
Nausea and vomiting 2 (4%) 3 (6%) >0.05 Not significantHeadache 11 (22%) 2 (4%) <0.05 SignificantPalpitation — — — —Hyperstimulation — — — —Tachysystole — — — —Fetal tachycardia 0 2 (4%) >0.05 —Postpartum hemorrhage 4 (8%) 5 (10%) >0.05 —

12 Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
AbstrAct
Objectives: The aim of our study was to analyze the indications, risk factors, operative procedures and outcome of cases requiring laparotomy following cesarean section (CS) done in the institution and referred from outside hospitals within six weeks of puerperium. Study design: A retrospective descriptive study was done in the Dept. of Obstetrics and Gynecology, Burdwan Medical College, Burdwan over five years from 1st January, 2005 to 31st December, 2009. One hundred forty-four cases required re-laparotomy following CS. Categorical data was analyzed by Chi-square test and p < 0.5 is statistically significant. Results: In the study period 13,642 (16%) cases of CS was performed out of 85,260 deliveries and re-laparotomy was done in 144 cases and the rate was 1.06% of cesarean deliveries. Out of these 144 cases, 78 cases were operated in the institution while 66 cases were referred from peripheral hospitals following CS. The commonest indication of re-laparotomy was secondary postpartum hemorrhage (PPH) (32.64%). Other indications were primary PPH (26.38%) followed by uterine sepsis (10.42%), rectus sheath hematoma (6.94%) and burst abdomen (8.34%). The risks associated with repeat CS was (relative risk [RR] 1.67; 95% confidence interval [CI] 1.192-2.36; p = 0.0040), obstructed labor (RR 3.25, 95% CI 2.34-4.44; p < 0.0001) and APH with placenta previa (RR 2.08; 95% CI 1.10-3.95; p = 0.0230). Main surgeries performed at re-laparotomy were brace suture (20.83%), subtotal hysterectomy (17.36%) and drainage of rectus sheath hematoma (6.94%). More than one procedure was adopted in some cases. There were 28 maternal deaths out of 144 cases of re-laparotomy and hemorrhagic shock contributed 46.43% (13/28) of maternal death within 6-24 hours. Other causes of death were sepsis (10 cases), renal failure (4 cases) and coagulation failure (1 case). Conclusions: Identification of risk factors of CS, good surgical technique in primary operation, prompt intervention and proper postoperative management following re-laparotomy can improve the maternal outcome.
Key words: Cesarean section, re-laparotomy, postpartum hemorrhage, indications
Re-laparotomy after Cesarean Section - Our Experience in a Teaching Hospital of West BengalAmitava pal*, raghunath Bhattacharya**, Sudhir Adhikari†, Anita roy‡
*Associate Professor**Senior Resident†Professor‡Professor and HeadDept. of Obstetrics and GynecologyBurdwan Medical College, BurdwanAddress for correspondenceDr Amitava Pal12/3J, Northern AvenueSundaram Apartment, Kolkata - 37E-mail: [email protected]
Cesarean section (CS) is an operation that mainly evolved to save a maternal life during difficult childbirth. In present era, there
is liberalization of CS with a view to gaining safe motherhood, small family norm and also to decrease the perinatal mortality and morbidity.1 It is a major operation and is associated with certain risks and complications though there is enormous improvement of surgical techniques, anesthesia coverage, monitoring system and blood transfusion facility with effective antimicrobials. Practically the complications depend
upon the indication of operation and also the quality of surgery. In some cases the complications need further laparotomy (re-laparotomy) to save the mother’s life.
In this study, we critically evaluated the cases of re-laparotomy following cesarean delivery done either in institution or referred from outside to find out its trends, indications, risk factors for operative procedure at laparotomy, outcome of cases and due precautionary measures to prevent such complications.
Material and Methods
The retrospective descriptive study was done in the Dept. of Obstetrics and Gynecology, Burdwan Medical College, Burdwan from 1st January, 2005 to 31st December, 2009 over a period of five years. It is a rural-based teaching hospital with a good catchment area for referrals, even outside of West Bengal. During the study period 13,642 CSs were performed out of 85,260 deliveries. Re-laparotomy was done in 144 cases and the rate was 1.06% of cesarean deliveries.
clinicAl study

13Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
clinicAl study
Out of these 144 cases, 78 cases were operated in the institution while 66 cases had cesarean delivery at peripheral hospitals and private nursing homes. As it is a training and teaching hospital the residential medical officers (RMOs), senior residents (SRs) and postgraduate students (PGs), all perform CS under direct supervision of senior surgeons. In the hospital, re-laparotomy following CS was done by RMOs in 50 (34.72%) cases and 94 (65.28%) cases were done by visiting consultants. All cases of re-laparotomy within six weeks of postpartum period were analyzed. The data of the patients were collected from patient’s case records, operation log book and referral notes of the primary CS. The parameters noted were age, parity, indications of primary CS, risk factors, indications of re-laparotomy, time interval from primary CS to re-laparotomy, procedure undertaken during reopening, amount of blood transfused, duration of hospital stay and the outcome following re-laparotomy. Risk association (relative risks with 95% confidence interval [CI]) was calculated and categorical data was analyzed by χ2 test and p value <0.05 is statistically significant.
ResultsA total of 144 cases were re-opened following CS. Of these, 78 cases were operated in the institution and 66 cases were referred from peripheral hospitals and private clinics. In the study period, a total of 13,642 (16%) CSs were performed out of 85,260 deliveries and the incidence of re-laparotomy following institutional CS was 0.57 (78/13,642) percent. During the same period a total of 39 cases (0.054%) required laparotomy following 71,618 vaginal deliveries in the institution (OR 10.5543; 95% CI 7.1829-15.508; χ2 = 223.774; DF = 1; p ≤ 0.0001). The characteristics of 144 cases of re-laparotomy ranged from 15 to 35 years (mean ± SD, 25 ± 4.88 years, 95% CI, 24.2002-25.7998) and parity ranged from 0 to 5 with a median of 2.5 (mean ± SD, 2.5 ± 1.8, 95% CI, 0.4304-4.5696). Sixty-five percent of the patients having re-laparotomy were from poor socioeconomic status. Out of 78 re-laparotomy cases following institutional CS, 53 cases (67.95%) were booked.
Table 1 shows the commonest indication of repeat laparotomy was postpartum hemorrhage (PPH) in 85 cases (59.02%) of which secondary PPH cases were 47 (32.64%) and primary PPH due to atonicity were 38
cases (26.38%). Rectus sheath hematoma occurred in 10 cases (6.94%) and we included these in our series as peritoneal cavity was explored in addition to the drainage of hematoma.
Table 2 describes the indications of primary operation and risk association of re-laparotomy. The common indications of CS was post-CS pregnancy (3,125, 22.91%), followed by fetal distress (2,046, 14.99%) and repeat CS (1534, 11.24%). Of the 144 re-laparotomy cases, 133 cases (92.4%) had undergone emergency CS and 11 cases (7.6%) had elective CS. The commonest indication of emergency CS was obstructed labor (22.2%, 32/144). Only in 4.99 (7/144%) of cases, emergency CS was done for prolonged labor. Of the emergency CS, 31.58% (42/133) of cases were done during intrapartum period. Sixty-five percent (51/78) of the institutional cesarean delivery cases were performed within 0-8 hours of admission, and the remaining 27 cases were admitted in the antenatal ward. Out of these 27 cases, intrapartum CS was done in 16 cases and the residual 11 cases was operated as an elective case. Spinal anesthesia was used both for emergency and elective CS.
Table 3 summarizes the different procedures undertaken at laparotomy. In case of PPH, we first used oxytocic drugs, blood transfusion and antibiotics in secondary PPH. When the medical treatment failed, a surgical procedure was adopted. The main surgeries included were application of brace suture in 30 cases (20.83%), subtotal hysterectomy in 25 cases (17.36%) and total hysterectomy in nine cases (6.25%).
table 1. Indications of Re-laparotomyIndications no of cases
(n = 144)percent
(%)Postpartum hemorrhage 85 59.02 Primary PPH 38 26.38 Secondary PPH 47 32.64Uterine sepsis 15 10.42Rectus sheath hematoma 10 6.94Intraperitoneal hemorrhage 7 4.86Burst abdomen 12 8.34Abdominal wound dehiscence 6 4.17Others* 9 6.25*Others; bladder injury (1 case), broad-ligament hematoma (4 cases), abdominal distension (4 cases).

14 Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
clinicAl study
Table 4 describes the case-fatality rate following re-laparotomy. A total of 28 cases died following re-laparotomy with case fatality rate of 19.44% (28/144). Thirteen patients died due to PPH and
table 2. Indication of Cesarean Section for Primary Operation and Re-laparotomy in the Study Groups and its Risk AssociationIndications of cS no. of primary
cS (n = 13,642)no. of hospital cases
needing re-laparotomy (n = 78)
no. of referred cases needing re-laparotomy*
(n = 66)
rr (95% cI) p value#
Post CS pregnancy (one CS before)
3,125 (22.91) 14 (17.95) 9 (13.64) 0.69 (0.48-1.01) 0.0470$
Repeat CS 1,534 (11.25) 12 (15.38) 15 (22.73) 1.67 (1.19-2.36) 0.0040$
Fetal distress 2,046 (14.99) 17 (21.79) 0 0.78 (0.50-1.23) 0.2810
Obstructed labor 955 (7.00) 10 (12.83) 22 (33.33) 3.25 (2.34-4.44) <0.0001$
Prolonged labor 682 (4.99) 3 (3.86) 4 (6.06) 0.97 (0.47-2.00) 0.9380
Hypertensive disorder 1,637 (11.99) 6 (7.69) 6 (9.09) 0.69 (0.40-1.19) 0.1730
APH with placenta previa 413 (3.04) 5 (6.41) 4 (6.06) 2.08 (1.10-3.95) 0.0230$
Malpresentation 1,091 (7.99) 8 (10.23) 4 (6.06) 1.04 (0.60-1.80) 0.8820
Multiple pregnancy 409 (2.99) 3 (3.86) 2 (3.03) 1.16 (0.49-2.76) 0.7380
Failed induction 989 (7.26) 0 0 — —
CPD 550 (4.03) 0 0 — —
Others 211 (1.56) 0 0 — —CS: Cesarean section; APH: Antepartum hemorrhage; CPD: Cephalopelvic disproportion; n (%); RR: Relative risks (95% CI: Confidence interval).*For referred cases primary CS was done in other hospitals that required re-laparotomy.#P value was calculated from χ2 analysis.$Significant as p value is <0.05.
table 3. Procedure Adopted During Re-laparotomyprocedure no. of cases
(n = 144)*Brace suture 30 (20.83)Subtotal hysterectomy 25 (17.36)Total hysterectomy 9 (6.25)Bilateral uterine and ovarian artery ligation 20 (13.89)Resuturing of uterine incision 18 (12.5)Repair of bladder injury 1 (0.69)Drainage of blood clot from under surface of the rectus sheath and peritoneal cavity toileting
10 (6.94)
Internal iliac artery ligation 4 (2.79)Repair of anterior abdominal wall 19 (13.19)Repair of intestinal injury 3 (2.08)Negative laparotomy 5 (3.48)*More than one procedure adopted in some cases; n (%)
shock within 6-24 hours. Ten patients died due to sepsis and multi-organ failure within 8-9 days and one patient died due to coagulation failure within five hours in a case of pregnancy-induced hypertension.
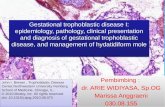
Figure 1 shows the trend analysis of re-laparotomy in hospital and referred cesarean delivery cases in a 5-year period. Fitting of a trend line to the observed data shows that a higher value of R2 (R2 = 0.7697) indicates a better fit to the re-laparotomy cases following institutional CS where as low value (R2 = 0.0027) in referred cases shows lack of fit.
Figure 2 shows 50 cases (34.73%) of re-laparotomy within 24 hours. These were the cases of primary PPH (38), intraperitoneal hemorrhage (7), broad-ligament hematoma (4), and bladder injury (1). Twelve cases of burst abdomen, six cases of abdominal wound dehiscence and three cases of rectus sheath hematoma was repaired on the seventh postoperative day after stitch removal.

1�Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
clinicAl study
Discussion
Cesarean section is now safer than it has been, in terms of advances in techniques, anesthesiology, blood transfusion, surgery and the availability of powerful antibiotics. But it is not entirely safe and therefore, is not an alternative to vaginal delivery.
In our study period, the incidence of CS was 16% (13,642/85,260) which was lower than the studies
table 4. Case-fatality Following Re-laparotomycauses of death no. of death
(n = 28)Indications of re-laparotomy
Indications of cS delivery
time interval between re-laparotomy to death
Hemorrhagic shock 13 PPH with shock (13) Obstructed labor (5) 11 hoursPlacenta previa (5) 6 hours
Repeat CS (3) 24 hours
Sepsis with vital organs failure 10 Rectus sheath hematoma (2)
Obstructed labor (10) 8 days
Secondary PPH (8) 9 days
Renal failure 4 PPH (3) (Atonic uterus)
Obstructed labor (3) Prolonged labor (1)
4 hours 7 hours
Rectus sheath hematoma (1)
Coagulation failure 1 Internal hemorrhage (1)
Hypertensive disorder (1)
5 hours
conducted by other authors.1,2 Due to high rise of CS rate at the tertiary centers, obstetricians now deal with a lot of complications and published data on reopening of abdomen following primary CS is not sufficient. One such series from a teaching hospital in Bangladesh, with a CS rate of 48.43% showed a re-laparotomy rate of 0.63%, out of total 7,909 deliveries.3 Another study from a teaching hospital Ghana with a CS rate of 17% showed a re-laparotomy rate of 0.7%, out of a total
2004.5 2005 2005.5 2006 2006.5 2007 2007.5 2008 2008.5 2009 2009.5Year
No. o
f cas
es
25
20
15
10
5
0
y = - 2.5x + 5033.1R2 = 0.7697
y = 0.1x - 187.5R2 = 0.0027
InstitutionReferredLinear (Institution)Linear (Referred)
figure 1. A line diagram showing the trend analysis of re-laparotomy in hospital and referred cesarean delivery cases in a 5-year period (2005-2009).

1� Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
clinicAl study
of 36,012 deliveries.4 In our hospital the incidence of CS was 16% and repeat re-laparotomy was needed in 1.06% (144/13,642) of cesarean deliveries and 0.05% cases following vaginal delivery. The limitation of our study was that in 66 out of 144 cases, CS was done at peripheral hospital, so the overall incidence was difficult to calculate as the denominator of the incidence was not definitely known.
The main and most frequent indication of CS in our study was post-CS pregnancy followed by fetal distress. The indications of emergency CS in obstructed and prolonged labors were 7.00% and 4.99%, respectively. CS in second sage of labor with impacted head is more prone to trauma, hemorrhage and infection of the lower segment of uterus.5 The deeply engaged head can be delivered by modified Patwardhan’s method6 or by pushing the fetal head up transvaginally7 to prevent trauma of lower uterine segment. The commonest indication of re-laparotomy was PPH, which was similar to the findings of other studies.3,4,8 When all the conservative medical management failed, laparotomy followed by conservative surgery like brace (Hayman) suture,9 uterine artery ligation, hypogastric artery ligation were done stepwise.10 Secondary PPH demanded more frequent re-laparotomy (32.64%) than primary PPH (26.38%) cases in our series. Our finding was inconsistent with the other studies where
0 5 10 15 20 25 30 35 40Re-laparotomy cases in percent
Within 16th to 42nd POD
Within 8th to 15th POD
Within 7th POD
Within 24 hours
25.69
25
14.58
34.73
Series 1
figure 2. Distribution of time interval from cesarean delivery to re-laparotomy.
secondary PPH accounts for re-laparotomy in 33% and 30.30% of cases respectively.3,8 Out of 47 cases of secondary hemorrhage, 38 cases were referred and in 25 cases, exact cause of PPH was not definitely known as USG could not detect any bits of placenta inside the uterus or exploration under anesthesia fails to detect any bits of placental tissue inside. Of these 25 cases, conservative medical management including dilatation and curettage improved eight cases, conservative surgical approach responded only in 12 cases and five cases needed subtotal hysterectomy and the rest 13 grossly infected cases needed hysterectomy. Conservative surgical methods adopted in our study for management of secondary PPH were wound debridement, resuturing, uterine and ovarian artery ligation, and internal iliac artery ligation. Four cases required third time laparotomy and hysterectomy was mandatory in all these cases. Nine cases of secondary hemorrhage where primary section was done in our institution responded by medical management (6 cases), conservative surgical approach (3 cases).
In case of placenta previa proper hemostasis of placental bed in lower uterine segment should be done before closure of incision in CS. Hwu et al11 introduced vertical compression sutures in lower segment of the uterus to control bleeding from placenta previa and where hemostasis was doubtful per vaginal bleeding was assessed before closure of the abdomen and

1�Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
clinicAl study
total hysterectomy was adopted where bleeding was uncontrollable. Rectus sheath hematoma was commonly found in our study in 6.94% of cases especially in lower abdominal transverse incision during CS. Routine observation and securing of blood vessels on the under surface of the rectus abdominis muscles before closure of rectus sheath is very much important to reduce the incidence of rectus sheath hematoma. Routine removal of blood clots and peritoneal toileting was done as parietal peritoneum was kept opened routinely in our series. Modified Joel-Cohen technique might reduce the incidence of rectus sheath hematoma.12
Maternal mortality was greater in patients who required re-laparotomy following CS. It was 19.44% (28 out of 144) in our study where as the mortality was 12% in other Indian study,8 19% in African4 and 25% in Bangladesh3 studies. Special supervision should be needed in certain indications of CS, requiring re-laparotomy like post-CS, repeat CS pregnancy, obstructed labor, placenta previa and all these cases should be done by experienced surgeons rather than by trainee. Maternal mortality was higher in emergency CS and in referred cases. Maternal mortality can be minimized by optimum time taken during operation, good surgical technique, meticulous case management and availability of blood and facilities of high-dependency units (HDUs) or obstetric intensive care units (ICUs).
Conclusion
Cesarean section is a life saving measure, but is not risk free. It should be done only when it is judiciously indicated with prior counseling regarding complications.CS and re-laparotomy following CS should be done by experts with good technique to reduce hemorrhage, damage of gut or bladder and maternal death when associated with certain risk factors. The lower the CS rate, the lower will be the complications including re-laparotomy. Prompt intervention, proper postoperative management and well-equipped ICU facilities can reduce maternal mortality. Periodic audit of labor ward is also very much essential to improve the maternal outcome.
Acknowledgement
We are thankful to the Medical Superintendent Cum Vice-Principal of Burdwan Medical College and Hospital for allowing us to use the hospital records for our study.
References1. Chhari V, Bhattacharjee S. Outcomes of high-risk
caesarean section - an ongoing challenge. Asian J Obstet Gynecol 2010;2:18-22.
2. Olivares Morales AS, Santiago Ramirez JA, Cortes Ramirez P. Incidence and indication for caesarean section at the Central Military Hospital of Mexico. Ginecol Obstet Mex 1996;64:79-84.
3. Rouf S, Sharmin S, Dewan F, Akhter S. Relaparotomy after caesarean section: experience from tertiary referral and teaching hospital of Bangladesh. Bangladesh J Obstet Gynecol 2009;24(1):3-9.
4. Seffah JD. Re-laparotomy after caesarean section. Int J Gynaecol Obstet 2005;88(3):253-7.
5. Fasubaa OB, Ezechi OC, Orji EO, Ogunniyi SO, Akindele ST, Loto OM, et al. Delivery of the impacted head of the fetus at caesarean section after prolonged obstructed labour: a randomized comparative study of two methods. J Obstet Gynaecol 2002;22(4):375-8.
6. Parulekar SV. Practical Gynecology and Obstetrics, 1st edition, Vora Medical Publication, Bombay 1987:365.
7. Bergholt T, Stenderup JK, Vedsted-Jakobsen A, Helm P, Lenstrup C. Intraoperative surgical complication during caesarean section: an observational study of the incidence and risk factors. Acta Obstet Gynecol Scand 2003;82(3):251-6.
8. Seal SL, Kamilya G, Bhattacharyya SK, Mukherji J, Bhattacharyya AR. Relaparotomy after caesarean delivery: experience from an Indian teaching hospital. J Obstet Gynaecol Res 2007;33(6):804-9.
9. Hayman RG, Arulkumaran S, Steer PJ. Uterine compression sutures: surgical management of post-partum haemorrhage. Obstet Gynecol 2002;99(3): 502-6.
10. Francois KE. Postpartum haemorrhage. In: Obstetric Intensive Care Manual. 2nd edition, Foley MR, Strong TH, Garite TJ, (Eds.), Tata McGraw-Hill Publishing Company Ltd: New Delhi 2005:24-37.
11. Hwu YM, Chen CP, Chen HS, Su TH. Parallel vertical compression sutures: a technique to control bleeding from placenta previa or accreta during caesarean section. BJOG 2005;112(10):1420-3.
12. Wallin G, Fall O. Modified Joel-Cohen technique for caesarean delivery. Br J Obstet Gynecol 1999:51-6.
n n n

1� Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
clinicAl study
AbstrAct
Introduction: The incidence of acute renal failure (ARF)-related to pregnancy in the developed countries is 1-2.8%, in the developing countries it is 9-25%. The reason of the lower incidence in the developed countries is the prevention of the pregnancy complications and early treatment, and more effective treatment of the pre-eclampsia. Aim: To evaluate the contributing factors responsible for renal failure of obstetric origin and also to study the statistical outcome with adequate dialysis and supportive care in renal failure of obstetric origin. Material and methods: Based on the inclusion and exclusion criteria, 52 patients with pregnancy-induced ARF who were admitted at Institute of Kidney Diseases and Research Centre and Institute of Transplantation Sciences from January 2008 to October 2008 were included in the study. Conclusion: The incidence of ARF of obstetric origin was 9.06% out of total ARF admissions in hospital in our study. Mortality was higher (28.57%) amongst the patients with home delivery compared to hospital delivery (15.55%). All the patients who expired had mortality before they could recover their renal function and had associated morbidity of infection, SIC, pre-eclampsia, hepatic encephalopathy. India is a country of high birth rate, and the incidences of pregnancy-related ARF can be brought down by healthcare providers who can contribute to this cause by increasing the awareness of the potential dangers related to pregnancy and better healthcare options.
Key words: Acute renal failure, pregnancy
A Study on Pregnancy-induced Acute Renal Failure
Ar patel*, pr Shah**, daniel p Sam*, Anand IS*, Gireesh mS**
*Shri Sarvajanik Pharmacy College, Mehsana**Institute of Kidney Diseases and Research Centre Ahmedabad
The incidence of acute renal failure (ARF)- related to pregnancy in the developed countries is 1-2.8%; in the developing countries, the
incidence is 9-25%. The reason of the lower incidence in the developed countries is the prevention of the pregnancy complications and early treatment, and more effective treatment of the pre-eclampsia.
In developing nations like ours, pregnancy-related ARF may comprise upto 25% of referrals to dialysis centers and is associated with substantial maternal and fetal mortality.
Aim and Objectives
To evaluate the contributing factors responsible for renal failure of obstetric origin and also to study the statistical outcome with adequate dialysis and supportive care in renal failure of obstetric origin.
Material and Methods
In this prospective study, 70 patients with ARF of obstetric origin were studied at Institute of Kidney Diseases and Research Centre, Ahmedabad during period of June 2008 to January 2009.
Inclusion criteria
Pregnant women who were previously healthy and had developed ARF due to obstetrical complication.
exclusion criteria
Evidence of renal disease prior to pregnancy
History of hypertension or diabetes mellitus before gestation
History of nonsteroidal anti-inflammatory drug (NSAID) or analgesic nephropathy
History of renal stone disease
History of reflux nephropathy

1�Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
clinicAl study
table 2. Various Factors According to Place of Deliveryplace of delivery
no. of patients
mortality complete recovery
partial recovery
no recovery
Hospital 45 (86.53%)
7 (15.55%)
25 (55.55%)
8 (17.77%)
6 (13.33%)
Home 7 (13.46%)
2 (28.57%)
3 (42.85%)
0 1 (14.28%)
table 3. Maternal Outcomematernal outcome no. of patients percentageComplete recovery 28 53.86%Partial recovery 8 15.38%No recovery 7 13.46%Expired 9 17.30%
Results
Table 1 represents the various factors of obstetric origin for ARF. Mortality was higher in patients with home delivery (Table 2). The outcomes among patients are described in Table 3.
Conclusion
Mortality was higher (28.57%) amongst patients with home delivery compared to hospital delivery (15.55%).
table 1. Various Factors of Obstetric Origin for ARFVarious factor no. of patients
(n = 52) percentage
Postabortion sepsis 14 26.92%
Hemorrhage (APH) 05 9.61%Hemorrhage (PPH) 04 7.69%Pre-eclampsia/eclampsia
10 19.23%
Puerperal sepsis 19 36.53%
India is a country with a high birth rate. The incidences of pregnancy-related ARF could be brought down by healthcare providers who can contribute to this cause by increasing the awareness of the potential dangers related to pregnancy and better healthcare options. This pregnancy-related complication, though has decreased now, but not to a satisfactory level. By increasing the awareness of these complications among rural and urban areas, it may be possible to avoid such type of complications in cases of home delivery also.
Suggested Reading1. Pertuiset N, Grunfeld JP. Acute renal failure in pregnancy.
Baillieres Clin Obstet Gynaecol 1994;8(2):333-51.
2. Davison J. Renal complications that may occur in pregnancy. In: The Oxford Text Book of Clinical Nephrology. 3rd edition, Oxford University Press 2005; 15(2):2233-42.
3. Chugh KS, Singhal PC, Kher VK, Gupta VK, Malik GH, Narayan G, et al. Spectrum of acute cortical necrosis in Indian patients. Am J Med Sci 1983;286:(1)10-20.
4. Turney JH, Ellis CM, Parsons FM. Obstetric acute renal failure 1956-1987. Br J Obstet Gynecol 1989;96(6): 679-87.
5. Prakash J, Tripathi K, Malhotra V, Kumar O, Srivastava PK. Acute renal failure in eastern India. Nephrol Dial Transplant 1995;10(11):2009-12.
6. Selcuk NY, Tonbul HZ, San AR. Changes in frequency and etiology of acute renal failure in pregnancy (1980-1997). Ren Fail 1998;20(3):513-7.
7. Utaş C, Yalçindag C, Taşkapan H, Güven M, Oymak O, Yücesoy M. Acute renal failure in Central Anatolia. Nephrol Dial Transplant 2000;15(2):152-5.
8. Gerrard JM, Catts GRD, Jones MC. Acute renal failure: Iceberg revisited (abs). Nephrol Dial Transplant 1992;7:458.
n n n

20 Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
AbstrAct
During last five years, we operated upon 21 cases of vesicovaginal fistulas. We report herein six complex fistulas that had different morbid anatomy and required different surgical routes and procedures for their repair. All these fistulas would have been prevented if due precautions had been taken during obstetric/gynecological procedures. The results of the repaired fistulas following general plastic surgical principles and team approach were acceptable with formation of no residual/recurrent fistula.
Key words: Risky zone, safe zone, vesicovaginal fistula, ureteric reimplantation
Management of Complex Vesicovaginal Fistulas: A Brief Report with Focus on Preventive AspectsrB Singh*, Satish dalal**, S nanda†
cAse report
*Senior ProfessorDept. of Burns and Plastic Surgery, Hypospadias and VVFs Clinic**Associate ProfessorDept. of General Surgery†Senior Professor, Dept. of Obstetrics and GynecologyPt. BD Sharma Postgraduate Institute of Medical Sciences (PGIMS) Rohtak, HaryanaAddress for correspondenceDr Satish Dalal9J/54, Medical CampusPGIMS, Rohtak-124 001, HaryanaE-mail: [email protected]
Vesicovaginal fistula (VVF), commonly caused by obstructed labor, is one of the worst complications of childbirth and
poor obstetric care in the developing world. This unpleasant complication leaves the affected women with continuously leaking urine, excoriation of vulva and vagina, often rendering them social outcasts.1 This report will highlight six different varieties of such fistulas focussing on their etiological factors and different surgical techniques used for their repairs. This will also help in framing necessary guidelines for prevention of such genitourinary fistulas.
Case Reports
case 1
Following prolonged obstructed labor due to cephalopelvic disproportion (CPD) and stillbirth, a 35-year-old G2P1A0S1 developed mega VVF with circumferential loss of the bladder neck. Both the ureteric orifices were located in the risky zone. Total hysterectomy, repair of upper defect of the
bladder and the vaginal cuff, bilateral ureteric reimplantation along with omental flap interposition were done. Through transvaginal route, the lower part of the bladder defect was repaired and reinforced with Martius onlay flap (Fig. 1 a and b). She was fully continent because of the presence of residual healthy sphincter in the lower part of the uninvolved urethra. The extreme pressure of the presenting head against the pubic symphysis resulted in necrosis of whole of the circumference of neck of bladder. Timely obstetrical help (reporting to a hospital in time and the availability of an expert obstetrician) would not have allowed this complication to occur. She was continent from the day of removal of Foley’s catheter.
case 2
Following total hysterectomy for menorrhagia due to multiple large fibroids, a 50-year-old G3P3A0S0 developed
figure 1. Preoperative morbid anatomy (a) and postoperative illustration (b).
(a) (b)

cAse report
21Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
high VVF and chronic pain in the hypogastrium. She was partly continent. Ultrasonography (USG) revealed pelvic collection and left-sided hydronephrosis. Leakage of urine in the vagina was from the pelvic urinoma formed due to a rent in the left ureter. Repair of the bladder, vaginal cuff, left ureteric reimplantation and omental flap interposition were done (Fig. 2 a and b). Distorted anatomy of the pelvic organs due to giant uterine fibroids could be the cause for such iatrogenic complication. The operating surgeon should have been extremely alert and careful under the circumstances having distorted pelvic anatomy. A preoperative intravenous pyelogram (IVP) will outline the course of the ureters and will help in prevention of ureteric injury to occur during the surgical procedures carried out in presence of distorted pelvic anatomy. After the completion of the surgical procedures under such circumstances, the surgeon should ensure (outline the ureters by their peristaltic movements, no watery fluid leaking or any evidence of fluid collection or dissect the ureters along their course to ascertain their integrity) that ureters are intact without any breach in their walls. She had normal act of micturition on follow-up.
case 3
Following prolonged obstructed labor, a 35-year-old G3P2A0S1 developed high VVF involving complete base of the bladder. Both the ureteric orifices were not visible despite careful search and rapid infusion of 2,000 ml of normal saline in a short span of 30 minutes along with intravenous administration of 40 mg of furosemide. The spurt of the urine could not be seen, but the urine was collecting in the vagina. Eversion of fistulous margins revealed ureteric openings
figure 2. Preoperative morbid anatomy (a) and postoperative illustration (b).
figure 4. Preoperative morbid anatomy (a) and postoperative illustration (b).
figure 3. Preoperative morbid anatomy (a) and postoperative illustration (b).
on the vaginal side of the margins of the fistula. Total hysterectomy, repair of the bladder and vaginal cuff, bilateral ureteric reimplantation along with omental flap interposition were done (Fig. 3 a and b). Education of the pregnant women, availability of obstetric care at peripheral health centers and hospitals would prevent such disasters to happen. She had normal stream of urine with full control.
case 4
Following obstructed labor due to CPD, a 35-year-old G2P2A0S0 developed high VVF. Transperitoneal- transvesical exploration revealed loss of anterior lip of the cervix and both ureteric orifices in safe zone. Total hysterectomy, repair of bladder and vaginal cuff along with omental flap interposition were done (Fig. 4 a and b). Widespread availability of the obstetric facilities will avoid such complications to happen. She had no abnormality of micturition after repair of VVF.
(a) (b)
(b)(a)
(a) (b)

cAse report
22 Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
case 5
Following total hysterectomy for menorrhagia due to dysfunctional uterine bleeding (DUB), a 35-years-old G2P2A0S0 developed high VVF along with prolapsed fallopian tube into the vagina. Exploration revealed a cavity containing serous fluid, rents in bladder and vaginal cuff and the right fallopian tube was herniating into the vagina and the bladder. Both the ureteric orifices were in safe zone. Repair of bladder, vagina, right salpingectomy with omental flap interposition were done (Fig. 5 a and b). Adequate drainage of pelvic cavity, proper hemostasis and multilayered eccentric closure of bladder and vaginal cuff would have prevented this collection, VVF and the herniation of the fallopian tube. She did not make any complaint regarding control of urination later.
case 6
Following total hysterectomy for menorrhagia due to DUB, a 40-year-old G3P3A0S0 developed high VVF
near the dome of the bladder. The bladder and the vagina were widely separated. Both ureteric openings were within safe zone. Local transposition flap from the bladder wall was designed to close the VVF eccentrically (Fig. 6 a and b). No other reinforcement flap was used. While repairing the vaginal cuff, deep sutures taken through the full thickness of the wall of the bladder had resulted in formation of this VVF in the dome of the bladder. Little care to clearly define bladder and vaginal cuff before putting sutures would have prevented this morbidity. She admitted to having normal control on micturition on discharge.
DiscussionThe key to successful repair of VVF lies in the classic principles defined by Couvelaire in 1953, “good visualization, good dissection, good approximation of the margins and good urine drainage.2 These principles still hold true and can be achieved both through vaginal and abdominal approaches. Although the choice of technique partly depends on the characteristics of the fistula, it also depends on the experience of the surgical team. Most of the simple VVFs can be easily managed through transvaginal route but when the fistula is complex vaginal exposure is suboptimal which may compromise the repair or endanger the ureters.3 In these circumstances, a transabdominal approach should be preferred.3,4 The six cases of complex VVFs, reported herein were successfully managed with this approach.
The fundamental principles of repair i.e., adequate exposure, tension free approximation of fistula edges, nonoverlapping suture lines, multilayered closure of bladder and vagina at right angle to each other, good hemostasis and adequate postoperative bladder drainage are essential factors for successful outcome.2,3 All these factors were successfully followed in all our cases. Nowadays, it is mandatory for all repairs to be strengthened with routine use of reinforcement flaps, for which several such flaps have been described in literature with their multifactorial mechanism of action.5,6 Omental flap in transperitoneal and Martius flap in transvaginal approach are two such reinforcement flaps, which are most versatile and can be harvested with ease without producing any functional or cosmetic donor site deformities.7
In view of the observations made while dealing with different kinds of VVFs, it is necessary to lay down certain guidelines. The results are better with
figure 5. Preoperative morbid anatomy (a) and postoperative illustration (b).
figure 6. Preoperative morbid anatomy (a) postoperative illustration (b).
(a) (b)
(a) (b)

cAse report
23Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
team approach and such team should consist of a senior gynecologist, a general surgeon and a plastic surgeon/urologist. All the members of operating team should be:
Well conversant with normal and morbid anatomy of pelvis
Familiar with different surgical procedures and techniques
Expert in harvesting of need-based reinforcement flaps
Have an updated knowledge of preventing bladder injuries under adverse circumstances like repeat lower segment cesarean section (LSCS), subtotal hysterectomy for control of bleeding and frozen pelvis, etc.
Conclusion
It is important to remember that vast majority of fistulas are preventable. Prevention of such fistulas include antenatal education, awareness of women in their reproductive periods, easily available transport facilities and widespread availability of obstetrical facilities even in the remote and rural areas.
We aim to highlight following facts through presentation of this report:
Surgical correction of VVFs is still a great challenge, but best results can be achieved through a team approachSince vast majority of fistulas are preventable, proper emphasis should be given on preventive aspects.
References1. Latzko W. Postoperative vesicovaginal fistulas: genesis
and therapy. Am J Surg 1942;58:211-8.
2. Couvelaire R. Reflections on a personal statistics of 136 vesicovaginal fistulas. J Urol Medicale Chir 1953;59: 150-60.
3. Hadley HR. Vesicovaginal fistula. Curr Urol Rep 2002; 3(5):401-7.
4. O’Conor VJ Jr, Sokol JK, Bulkley GJ, Nanninga JB. Suprapubic closure of vesicovaginal fistulas. J Urol 1973; 109(1):51-4.
5. Fitzpatrick C, Elkins TE. Plastic surgical techniques in the repair of vesicovaginal fistulas: a review. Int Urogynecol J 1993;4(5):287-95.
6. Singh RB, Parvthran NM, Nanda S. Plastic reconstruction of a mega vesicovaginal fistula using broad ligament flaps: a new technique. Int Urogynecol J Pelvic Floor Dysfunct 2003;14(1):62-3.
7. Singh RB, Pavithran NM, Khatri HL, Nanda S. Technical aspects in the management of complex vesicovaginal fistulas. Trop Doct 2005;35(1):40-1.
n n n

24 Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
AbstrAct
Hydatid disease remains endemic in various parts of the world due to the close association that exists between sheep, dogs and humans. Humans are the accidental intermediary hosts in the biologic cycle of the Echinococcus granulosus, which is the most frequent hydatidosis in the environment. USG and CT are both excellent imaging modalities for the detection of hydatid cysts. CT provides 3-D view and delineates the cyst, which is useful when diagnosis is uncertain, or when rupture or infection has occurred.
Key words: Hydatid disease, abdominal lump, adnexal mass
Hydatid Cyst Mimicking as Ovarian Tumor
Sumitra yadav*, hk kansal**, Anita Singh†, Sanjay patidar†
*Associate Professor and Unit Head**Senior Resident†ResidentsDept. of Obstetrics and Gynecology MGM Medical College and MYH Hospital, Indore (MP)Address for correspondenceDr Sumitra Yadav30, Nayapura, Aerodrome RoadIndore - 452 005, MPE-mail:[email protected], [email protected]
Hydatid disease is a cyclozoonosis in which humans are accidental intermediary hosts in the biologic cycle of Echinococcus granulosus,
the most frequent etiologic agent for hydatidosis. It usually involves the liver (75%), lungs (5-15%) and other organs in the body such as the spleen, brain, heart, kidneys and ovary (10-20%). Hydatid disease evokes much interest not only for the diversity of the anatomical and clinical forms it produces but also for the problems of diagnosis and therapy it creates, particularly when located at unusual sites.
Case Report
A 70-year-old lady presented with a history of abdominal lump since 1-2 years, which was gradually increasing in size. Patient had persistent dull-aching pain abdomen. Initially the size of the lump was 3-4 × 4 cm in right iliac fossa; now it was 10 × 8 cm. It was associated with history of loss of appetite and weight loss. Patient also had history of constipation on and off for which she used to take medication (i.e. laxative) sometimes. There was no history of cough, vomiting,
jaundice, malena, hemoptysis and hematemesis. She was P2L2; married for 50 years and menopausal since 20 years. Physical examination revealed severe general cachexia (weight 30 kg) and a large mass (10 × 8 × 6 cm size) arising from pelvis on right side of abdomen. The mass was dull on percussion without any fluid thrill or shifting dullness, it appeared solid to cystic in consistency with ill-defined margins. There was no hepatosplenomegaly and lymphadenopathy. Further investigations were done to find out the exact extent and nature of disease.
Laboratory investigations: Hemoglobin (Hb) 7 g/dl; total and differential leukocyte counts were normal; renal and liver function tests were also normal; sputum for acid-fast bacilli (AFB) was negative; CA-125 - 50 IU/ml.
USG of abdomen and pelvis: Normal liver, echogenic mass in the spleen of size 2.5 cm. An adnexal mass was seen on the right side, which was cystic in consistency, size 12.3 × 10.3 cm with septations, solid component seen posterior to urinary bladder in pelvis; uterus/ovary not visualized.
Magnetic resonance imaging (MRI) of whole abdomen and pelvis showed an 8.4 × 5 cm sized right adnexal mass which appeared heterogeneously hyperintense on T2 and hypo on T1 images. It appeared well-marginated and revealed dense calcification. A predominantly cystic lesion in the left adnexae measuring 9 × 9 cm displacing the uterus to the right was also seen. It revealed multiple nodular mural components as well as multiple septae and locules within. No evidence of T1 hyperintensity
cAse report

cAse report
2�Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
was seen to suggest fat/hemorrhagic products. Rim calcification was seen. The fat planes appeared well preserved and the bowel loops were displaced; the urinary bladder appeared displaced anteriorly and Foley’s catheter was seen in situ. Intervening fat planes were preserved. No significant pelvic lymphadenopathy or free fluid was seen. Ureters were not dilated. The liver was normal in size and density - no focal lesion was seen. The gallbladder, biliary tree and pancreas were normal. The portal vein, splenic vein and spleen were normal. There was focal hyperintense lesion with hypointense smooth uniform rim seen in the splenic parenchyma measuring approximately 4.4 × 3.2 cm. Calcifications were seen in the both adrenals; kidneys were normal except for a simple cyst in upper pole of left kidney. No retroperitoneal lymphadenopathy was seen. The bowel loops were normal.
Outcome
The patient was taken for exploratory laparotomy after transfusing 2 units of blood, with 1 unit blood in hand. Intraoperatively, the bowel loops were found to be adherent to the underlying mass. Blunt dissection done and uterus could not be easily identifiable. That mass appeared as caseous material. Dissection was completed taking due precautions. There were dense adhesions and on left side of ovary there were daughter hydatid cysts, 6-7 in number and sized 4-5 cms size. Pericyst and daughter cysts (Figs. 1 and 2) were removed with some difficulty. Betadine washing was done. Samples were collected from both sides for histopathology. A drain was kept in the pelvic area.
histopathology report
Material for examination: Left ovarian cyst, right ovarian caseous material (Fig. 3).
Microscopic: Hematoxylin and eosin (H&E) stained sections studied from ovarian tissue show cyst wall comprising of acellular eosinophilic laminated material. Brood capsule and scolices were also appreciated. Features were suggestive of hydatid cyst ovary.
Discussion
Hydatid disease remains endemic in various parts of the world due to the close association that exists between sheep, dogs and humans. Humans become infected
by accidental ingestion of food or water contaminated by tapeworm eggs. Humans are the accidental intermediary hosts in the biologic cycle of the E. granulosus, which is the most frequent hydatidosis in the environment. After ingestion, the eggs pass into the small bowel,
figure 1. Pericyst (Hydatid cyst material) in right-sided ovary.
figure 2. Left ovarian cysts.
figure 3. Caseous material in right-sided ovarian tissue.

cAse report
2� Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
where they hatch and are absorbed. The parasites then travel through the bloodstream and eventually establish cystic lesions in various organs. The liver is the most likely organ to be involved through portal drainage, but any organ may be infected. Each cystic lesion contains fluid and multiple secondary daughter cysts. The development of the parasitic larval stage in the organs of the host manifests in the form of cysts (hydatids). A typical hydatid cyst consists of three layers:1 Pericyst, ectocyst and endocyst. Complications are seen in one-third of cases.
The most common complication is rupture of cyst, which may result in anaphylactic shock and formation of localized or generalized secondary-echinococcosis.2 Fever with chills and rigors can occur if the cyst is secondarily infected. Jaundice, biliary colic and urticaria will develop if there is an intrabiliary rupture of the cyst.3 Intrathoracic rupture may lead to shoulder pain and phlegmatic cough containing blood and bile.4 USG and CT are both excellent imaging modalities for the detection of hydatid cysts. However, USG is less accurate in localizing and delineating the extent of the cyst though it’s cost-effective. The sensitivity of CT scan is 90-100%.5 It provides 3-D view and delineates the cyst, which is useful when diagnosis is uncertain or when rupture or infection has occurred.6
The WHO has outlined the treatment guidelines for hydatid cysts. Surgery is the treatment of choice for all patients with symptomatic disease and who are fit for surgery.7
References1. Milicevic M. Hydatid disease. In: Surgery of the Liver
and Biliary Tract. 2nd edition, Blumgart LH, (Ed.), Churchill Livingstone: New York 1994:1121-50.
2. Dew H. Some complications of hydatid disease. Br J Surg 1930;18(70):275-93.
3. Humayun MS, Rady AM, Soliman GM. Obstructive jaundice secondary to intrabiliary rupture of hepatic hydatid cyst. Int Surg 1989;74(1):4-6.
4. Saidl F. Surgery of hydatid disease. 1st edition, WB Saunders: Philadelphia 1976:112-21.
5. Safioleas M, Misiakos E, Manti C, Katsikas D, Skalkeas G. Diagnostic evaluation and surgical management of hydatid disease of liver. World J Surg 1994;18(6):859-65.
6. El-Tahir MI, Omojola MF, Malatani T, al-Saigh AH, Ogunbiyi OA. Hydatid disease of liver: evaluation of ultrasound and computed tomography. Br J Radiol 1992;65:390-2.
7. WHO Informal Working Group on Echinococcosis. Guidelines for treatment of cystic and alveolar echinococcosis in humans. Bull World Health Organ 1996;74(3):231-42.
n n n

clinicAl study


2�Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
AbstrAct
A 30-week pregnant woman presented with severe upper abdominal pain, fever and vomiting. Acute pancreatitis was diagnosed on the basis of high lipase (690 units), amylase (664 units) and hyperglycemia. She was also hypertensive and found to have high leukocytosis (30,000/mm3) and severe thrombocytopenia (11,000/mm3). The patient was managed conservatively with enteral nutrition, antibiotics, insulin, antihypertensives and repeated platelet transfusions. When the leukocyte count came down to 15,000/mm3, steroid was administered. Upon induction with vaginal misoprostol, she delivered vaginally a live baby of 1.4 kg, who was appropriately managed and discharged in good health. The obstetric scenario here was challenging and demanded continuous input from the various members of the multidisciplinary team. Despite the complexicity of the case, multidisciplinary approach, judicial planning and close monitoring helped in reaching a successful outcome.
Key words: Upper abdominal pain, lipase, amylase, leukocytosis
Acute Pancreatitis Complicating Pregnancy with Severe Thrombocytopeniakurmapu Sandhya rani
Former Consultant Dept. of Obstetrics and GynecologyCARE Hospital, Banjara Hills, Hyderabad Address for correspondenceDr Kurmapu Sandhya RaniFlat: 104, Raghava Residency Apts, Road No-11Banjara Hills, Hyderabad - 34E-mail: [email protected]
Acute pancreatitis in pregnancy is rare, with an incidence between 1 in 1,000 to 1 in 10,000 births.1 The majority of cases occur in the third
trimester, and gallstones are the most common cause.2 Weight gain and hormonal changes in pregnancy can lead to biliary sludge and gallstone formation.3 Alcohol and hyperlipidemia are other etiological factors; the latter accompanied by a poor outcome.4,5 However, in a significant proportion of patients no cause can be identified, and these are labeled as idiopathic.5
When pancreatitis occurs, complications can be multiple with life-threatening consequences to both the mother (maternal mortality 0-37%) and the fetus (perinatal mortality about 11%).6 However, these can be successfully managed by a specialized multidisciplinary approach through careful planning and judicial decision-making.
Case Report
A 26-year-old G2P1 was treated for four days by a GP at 30 weeks gestation for fever, vomiting and upper
abdominal pain. She had been started on methyldopa for hypertension. Suspecting acute pancreatitis with a serum amylase of 645 units, she was referred to our tertiary care hospital for further management. She had pre-eclamptic toxemia in her first pregnancy but had a successful normal vaginal delivery two and a half years ago. There was no other significant past medical history including gallstones, diabetes; she was nonalcoholic.
Upon admission, she appeared bloated with generalized edema and a purpuric rash over the chest, anterior abdominal wall and lower limbs. She had a large hematoma over her left buttock where an intramuscular injection was given at an earlier hospital. She was apyrexial with a blood pressure (BP) of 160/100 mmHg, pulse 88/min and respiratory rate of 34/min. She had tenderness in the epigastrium and right hypochondrium. Her uterus was found to be of 30 weeks size, soft, relaxed, nontender, without clinical appreciation of liquor and a fetal heart rate of 120/min. A speculum examination revealed thick curdy vaginal discharge, which was sent for culture and sensitivity.
Her hemoglobin (Hb) was 13 gm% and she had leukocytosis (WBC 30,000/mm3, predominant neutrophilia 73%) with severe thrombocytopenia of 11,000/mm3. Serum amylase and lipase were elevated at 664 and 690 units, respectively, with an LDH of 582 U/l and elevated blood sugars (362 mg/dl). Liver function tests were essentially normal with a total and direct bilirubin of 0.8 and 0.3 mg/dl, respectively,
cAse report

cAse report
30 Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
and SGOT 46 and SGPT 28 IU/l. Coagulation profile including fibrinogen levels (230 mg/dl), electrolytes, triglycerides and renal function tests were normal. A peripheral smear confirmed neutrophilic leukocytosis with a left shift, toxic granules and a marked thrombocytopenia; the film was negative for malaria parasites. Urine examination revealed albumin 4+.
Ultrasonography revealed a 30-week fetus in cephalic presentation with absent fetal movements, fetal heart rate of 120 minutes and scanty liquor. Extrauterine findings include mild splenomegaly, minimal fluid in the peritoneal cavity and small bilateral pleural effusions. The pancreatic head was small and grossly normal; body and tail were not visualized. The gallbladder, biliary tree, liver and kidneys were normal.
At this stage, a diagnosis of acute pancreatitis complicating pregnancy associated with severe thrombocytopenia was made. Sepsis was also suspected due to the high neutrophil leuckocytosis, although this could have been due to inflammation secondary to the acute pancreatitis. There was little evidence for disseminated intravascular coagulation (DIC) as the coagulation profile and fibrinogen were normal. The patient was managed in the medical intensive care unit with specialist input from Gastroenterology, Critical Care Physicians, Hematology and Endocrinology and with the Obstetrician as the primary consultant.
After careful discussion, it was decided to delay any obstetric intervention until the suspected sepsis was controlled and the platelet count improved to a reasonable level. Body temperature was normal at admission; but, subsequent monitoring showed low grade pyrexia. She was treated empirically with a broad-spectrum antibiotic (piperacillin + tazobactam) to cover for sepsis. Hyperglycemia was controlled with Insulin Sliding Scale, and a persistently elevated BP of around 180/120 mmHg was treated with a combination of methyldopa, nifedipine and labetalol. Despite this, the BP remained resistant causing fear of further maternal and fetal complications.
She received platelet transfusion as well as fresh frozen plasma, with only minimal improvement in platelet count. Nutrition and hydration were maintained through nasogastric tube feeding as well as intravenous fluids. She was treated with clotrimazole vaginal pessaries following clinical diagnosis of candidiasis
which was confirmed later with a positive high vaginal swab culture. Blood cultures and rest of the sepsis screen were negative. Nevertheless, she finished the course of antibiotics. She was also negative for HIV, hepatitis B, leptospirosis, dengue, Widal and antinuclear antibodies (ANA). A negative ANA virtually excludes systemic lupus erythematosus (SLE).
When the leukocytosis reduced to 15,000/mm3 by Day 6, dexamethasone was administered for two days to facilitate fetal lung maturity and boost platelet count. This combined with further platelet transfusion helped in improving the count to 52,000/mm3 by Day 7. Labor was induced with two doses of misoprostol on Days 7 and 8. Patient developed uterine contractions and delivered vaginally a 1.4 kg child with Apgar 4, resuscitated by a pediatrician. There was no excess blood loss at delivery.
The patient was closely monitored after delivery for any possible complications. She developed significant cough and breathlessness three hours after delivery and auscultation revealed bilateral lung crepitations. A chest X-ray confirmed pulmonary edema which was managed with furosemide and continuous positive airway pressure (CPAP) assistance. The patient did not develop any complications over the subsequent postpartum period. Platelets improved to 4,00,000/mm3 and the leukocytosis resolved by Day 15. The newborn was also found to be thrombocytopenic and was transfused platelets. Breastfeeding was allowed. Mother was discharged with her baby on Day 20 when she was advised to continue her antihypertensive medication, and to breastfeed her baby.
Discussion
The clinical presentation was almost similar to HELLP (Hemolysis, Elevated Liver enzymes and Low Platelets) syndrome but there was no evidence of hemolysis on peripheral smear, and moreover bilirubin and liver function tests were essentially normal. Acute pancreatitis was diagnosed through the clinical presentation as well as high serum lipase, amylase, leukocytosis and hyperglycemia. Due to the potential radiation exposure to the fetus, a CT scan could not be performed to aid the diagnosis of acute pancreatitis. The underlying cause for the acute pancreatitis was therefore not clear in this case. There was no history of alcohol intake and ultrasound did not show any gallstones. A viral

cAse report
31Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
etiology is possible, and this may also explain the severe thrombocytopenia.
This case of acute pancreatitis at 30 weeks gestation with a high leukocytosis and very low platelets, with secondary hyperglycemia and resistant hypertension posed a challenging situation to the entire team. The high neutrophilia suggested sepsis of bacterial origin, and although no focus was found, it was decided to treat the patient empirically. The timing of steroid was well-planned, which was administered when the reduced leukocytosis was evident. The decision to delay any obstetric intervention until the presumed sepsis was controlled and platelets improved was also crucial in this case.
High risk to the fetus, which was preterm with absent fetal movements and multiple maternal complications was expected. Labor induction was rightly timed. Also, a conservative approach by itself was a good choice while managing such critical cases, which averted possible serious complications. Most importantly, continuous supervision for possible complications even after delivery is of utmost necessary and such anticipation and close monitoring helped in the prompt diagnosis and treatment of pulmonary edema.
Conclusion
This case is a good example of a concerted effort by a multidisciplinary team in managing a complicated
obstetric case. The obstetric scenario was very challenging to the entire team. Prompt discussions and appropriate decisions of the team are crucial while managing critically ill pregnant woman at preterm with many medical complications like hypertension, acute pancreatitis, severe thrombocytopenia and hyperglycemia. The obvious risk to the fetus in such a scenario needs to be well-explained to the patient’s family as was done in this case. It was greatly satisfying to have a successful obstetric outcome, which was honestly not expected.
References 1. McKay AJ, O’Neill J, Imrie CW. Pancreatitis, pregnancy
and gallstones. Br J Obstet Gynaecol 1980;87(1):47-50.2. Ramin KD, Ramin SM, Richey SD, Cunningham FG.
Acute pancreatitis in pregnancy. Am J Obstet Gynecol 1995;173(1):187-91.
3. Stampfer MJ, Maclure KM, Colditz GA, Manson JE, Willett WC. Risk of symptomatic gallstones in women with severe obesity. Am J Clin Nutr 1992;55(3):652-8.
4. Eddy JJ, Gideonsen MD, Song JY, Grobman WA, O’Halloran P. Pancreatitis in pregnancy. Obstet Gynecol 2008;112(5):1075-81.
5. Takaishi K, Miyoshi J, Matsumura T, Honda R, Ohba T, Katabuchi H. Hypertriglyceridemic acute pancreatitis during pregnancy: prevention with diet therapy and omega-3 fatty acids in the following pregnancy. Nutrition 2009;25:1094-7.
6. Corlett RC Jr, Mishell DR Jr. Pancreatitis in pregnancy. Am J Obstet Gynecol 1972;113(3):281-90.
n n n

32 Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
AbstrAct
Succenturiate lobe of placenta is a morphological abnormality, in which there are one or multiple accessory lobes connected to the main part of the placenta by blood vessels. It has been known to be located on the lower segment and then present either as placenta previa or as a case of vasa previa, if vessels connecting the main placenta with the succenturiate placenta lie below the presenting part. Here, we present a rare case of antepartum hemorrhage resulting from the abruption of the succenturiate lobe of placenta.
Key words: Abruptio placenta, succenturiate lobe, accidental hemorrhage
A Case of Abruption of the Succenturiate Lobe of PlacentaAmol tilve*, roque ribeiro*
*Obstetrician and GynecologistJMJ Hospital, Porvorim, GoaAddress for correspondenceDr Amol TilvePeace Heaven ‘A’, H. No - 755/9/3Opposite Corporation Bank - Socorro BranchAlto-Porvorim, Bardez; Goa 403 521E-mail: [email protected]
Antepartum hemorrhage, i.e., bleeding after the 20th week of pregnancy, occurs in 25% of all pregnancies and placental abruption accounts
for approximately one-quarter of such cases.1 Placental abruption and placenta previa are the two common causes of antepartum hemorrhage. The diagnosis of placental abruption is always clinical,2,3 and the condition should be suspected in women who present with vaginal bleeding or abdominal pain or both. The succenturiate placenta is a morphological abnormality, in which there are one or multiple accessory lobes connected to the main part of the placenta by blood vessels.4 The incidence is 16-28 cases per 10,000 pregnancies. Here, we report a case in which placental abruption occurred in the succenturiate lobe of the placenta.
Case Report
Mrs. SDC, 33-year-old, G2P1 with previous preterm delivery was on regular antenatal follow-up. She was admitted at 32 weeks of gestation with complaints of spotting for three days followed by fresh bleeding on the day of admission with a diagnosis of ?accidental hemorrhage. Ultrasound examination done at
admission showed a single live intrauterine gestation at 31-32 weeks in cephalic presentation with adequate liquor. Placenta was anterior with no previa and with evidence of a small retroplacental clot. Her condition was stable and bleeding was minimal.
On general physical examination: Patient was conscious and of good built; weight 66 kgs; no pallor/icterus/pedal edema; pulse - 98/min; BP - 124/80 mmHg.
Examination of respiratory and cardiovascular systems revealed no abnormality.
Per abdominal examination: Uterus 30 week size, relaxed, fetus in cephalic presentation; FHS - present and regular (150 beats/min).
Routine tests: Hb - 11 g/dl; HIV/VDRL/HbsAg - NR; urine and stool: NAD.
USG: Single live intrauterine gestation at 31-32 weeks, liquor adequate, anterior placenta, evidence of a small retroplacental clot, cervix long with internal os closed.
Diagnosis: G2P1 at 32 weeks of gestation with ?abruptio placenta.
As the patient’s condition was stable, bleeding was minimal and in view of the preterm gestation, she was put on conservative management, with close watch on both fetal and maternal conditions. She received steroid prophylaxis for fetal lung maturity. There were small intermittent bouts of bleeding but the maternal and fetal condition remained stable.
cAse report

cAse report
33Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
Repeat ultrasound two weeks after admission showed a live fetus in cephalic presentation 34-35 weeks, with anterior placenta and a small retroplacental clot. The estimated fetal weight was 2.5 kgs. A decision for induction of labor was taken since the estimated fetal weight was 2.5 kgs and because of the facts that the patient was covered with steroids for fetal lung maturity and had had intermittent bleeding. Labor was induced with prostaglandin tablets and followed by artificial rupture of membranes (ARM), which revealed blood-stained liquor. Further augmentation with slow oxytocin drip resulted in a vaginal delivery of a live baby girl of 2.6 kgs. Placenta was delivered and revealed a succenturiate lobe (Figs. 1 and 2). There was a huge retroplacental clot occupying the whole of succenturiate lobe, while the rest of the placenta was normal.
Discussion
Placental abruption is defined as the complete or partial separation of the placenta before delivery and is one of the leading causes of vaginal bleeding in the second-half of pregnancy.1,2 Approximately 0.51% of the pregnancies are complicated by placental abruption.2,5
It is one of the most important causes of maternal morbidity and perinatal mortality. Approximately 10% of all preterm births and upto one-third of all perinatal deaths are caused by placental abruption.2,6 Placental abruption is suspected in all patients presenting with bleeding, uterine contractions and fetal distress.
Hemorrhage into the decidua basalis occurs as the placenta separates from the uterus, which usually
manifests as vaginal bleeding. However, at times the hemorrhage may be concealed with no signs of vaginal bleeding. Bleeding, if it continues, may result in fetal and maternal distress and if not attended to appropriately can result in maternal and fetal death. Management depends on severity of abruption, period of gestation, fetal and maternal condition. In case of deteriorating maternal condition and fetal demise, pregnancy is terminated by attempting a vaginal delivery if no contraindications exist. Labor, induced with amniotomy, usually progresses rapidly and may be further augmented with oxytocin drip.
Cesarean section is needed when labor does not progress well or the maternal condition becomes unstable. In case of a live fetus and a stable maternal condition, management is decided by the period of gestation. In term gestation, induction of labor is the best option. In preterm gestation, a policy of wait and watch, along with steroid injections for fetal lung maturity usually pays good returns. Close monitoring of both maternal and fetal condition is carried out to watch for fetal and maternal distress. Labor is induced at term or at the first signs of fetal or maternal distress.
Succenturiate placenta is usually a postnatal diagnosis but can also be suspected on an antenatal ultrasound.4,7,8 Its antenatal recognition is important as vessels connecting the main placenta with the succenturiate placenta, if lying below the presenting part: Vasa previa may rupture during labor causing massive hemorrhage and fetal death. In addition, there is an increased risk of postpartum hemorrhage from retention of placental material.4,7,8 A bilobate placenta is a similar anomaly
figure 2. Postnatal picture showing maternal surface of the placenta and abruption of the succenturiate lobe.
figure 1. Postnatal picture showing fetal surface of the placenta and succenturiate lobe.
placentaSuccenturiate lobe with abruption Succenturiate
lobe
main placenta

cAse report
34 Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
and it is not clear from literature as to what is the exact difference, if any exists.9 It appears that some authors use the term ‘bilobate’ when both segments of the placentas are almost equal in size and ‘succenturiate’ when there is a greater difference between the two segments. When an outlying portion of the placenta has not maintained its vascular connections with decidua vera, the placenta is called placenta spuria. Succenturiate placentas are known to be located on the lower segment and the management then would be that as of placenta previa.
Conclusion
Our case was treated as a case of placental abruption and was managed conservatively till fetal maturity and then delivered by induction of labor at term. Succenturiate lobe with complete abruption of the lobe was noted on delivery of the placenta. This case is presented for the rare occurrence of placental abruption in the succenturiate lobe.
References1. Konje JC, Taylor DJ. Bleeding in late pregnancy. In:
High Risk Pregnancy. 2nd edition, James DK, Steer PJ, Weiner CP, et al (Eds.), WB Saunders Co: Edinburgh, UK 2001:111-28.
2. Oyelese Y, Ananth CV. Placental abruption. Obstet Gynecol 2006;108(4):1005-16.
3. FayePetersen OM, Heller DS, Joshi VV, (Eds). Gross abnormalities of the placenta: lesions due to disturbances of maternal and of fetal blood flow. In: Handbook of Placental Pathology. 2nd edition, Taylor & Francis: Oxon, UK 2006:2751.
4. Jeanty P, Kirkpatrick C, Verhoogen C, Struyven J. The succenturiate placenta. J Ultrasound Med 1983;2:9-12.
5. Kyrklund-Blomberg NB, Gennser G, Cnattingius S. Placental abruption and perinatal death. Paediatr Perinat Epidemiol 2001;15(3):290-7.
6. Ananth CV, Getahun D, Peltier MR, Smulian JC. Placental abruption in term and preterm gestations: evidence for heterogeneity in clinical pathways. Obstet Gynecol 2006;107(4):785-92.
7. Hata K, Hata T, Aoki S, Takamori H, Takamiya O, Kitao M. Succenturiate placenta diagnosed by ultrasound. Gynecol Obstet Invest 1988;25(4):273-6.
8. Nelson LH, Fishburne JI, Stearns BR. Ultrasonographic description of succenturiate placenta. Obstet Gynecol 1977;49(1 suppl):79-80.
9. Angtuaco TL, Boyd CM, Marks SR, Quirk JG, Galwas B. Sonographic diagnosis of the bilobate placenta. J Ultrasound Med 1986;5(11):672-4.
n n n



3�Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
AbstrAct
Endometriosis is a common and important clinical entity among the women of reproductive age group. Presence of extrapelvic deposits of endometrial implants may occur in upto 12% of affected women. Cutaneous endometriosis is rare and usually appears in surgical scars following procedures like hysterectomy, lower uterine segment cesarean section, episiotomy and laparoscopy. It can also happen spontaneously. Umbilical endometriosis is the rarest variant of cutaneous endometriosis constituting 0.5-1% of all endometrial ectopia. It should be included in the differential diagnosis of any umbilical nodule. In this article, we report a case of umbilical endometriosis in a young woman, which presented with a different peculiar clinical picture of pain and swelling of umbilical lesion during physiological amenorrheic phase of lactation without bleeding. But the same lesion started bleeding when she resumed her normal menstrual cycle.
Key words: Cutaneous endometriosis, menstrual cycle, lactational amenorrhea
Umbilical Endometriosis: A Rare Cutaneous Endometriosisdebasmita mandal*, nibedita chattopadhaya**, raj Shekhar Sarkar†, hena kausar‡, Sougata Banerjee#, ratna deep Ganguli#
*RMO cum Clinical Tutor**Assistant Professor†Specialist Medical OfficerDept. of Obstetrics and Gynecology‡Junior Resident#Consultant, Dept. of PathologySSKM Hospital, KolkataAddress for correspondenceDr Debasmita Mandal C/o: Dr Saroj Mandal Qr/No: Block C-IIISSKM Hospital Campus, 242, AJC Bose Road Kolkata - 700 020, West Bengal E-mail: [email protected]: debasmita [email protected]
Endometriosis is classically defined as the presence of functional endometrial glands and stroma outside the uterine cavity. The frequent sites
of endometriotic implantations are peritoneal surfaces of reproductive organs, but it can also be found in extrapelvic sites in upto 12% of affected women.1 Amongst all endometriosis, the incidence of cutaneous endometriosis is 1.1% and that which arises from the umbilical region is about 30%.2 Till date, umbilical endometriosis has been reported in >100 cases and was first described by Villar in 1886.3 The prevalence of pelvic endometriosis is high (44%) in asymptomatic women undergoing laparoscopy for nongynecological symptoms, while incidence of umbilical endometriosis is only 0.5-1.0% of all women with extragonadal endometriosis.2
We herein report a rare case of cutaneous endometriosis i.e., umbilical endometriosis in a young woman presenting as cyclical tender umbilical nodule. The aim of reporting this case is to highlight the importance of history in diagnosis and the diagnosis dilemmas involved.
Case Report
A 23-year-old primipara presented to the Gynecology Outpatient clinic of SSKM Hospital, Kolkata with history of a tender umbilical nodule of 10 months duration after a lower segment cesarean section done one year back. During lactational amenorrhea, she noticed a nodule in the umbilical region swelling up and becoming tender cyclically.
After six months, when she resumed her normal menstruation, the umbilical nodule became swollen up, tender premenstrually and started releasing blood-stained discharge during menstrual cycles. Her cycles were regular without history of dysmenorrhea and she had conceived spontaneously. General physical examination was normal. Local examination during postmenstrual period revealed a 3 × 3 cm, nontender, nonreducible, firm, lobulated umbilical nodule and without a cough impulse (Fig. 1). There was no discharge. Mild ulceration was seen on the inner surface of umbilicus. Other systemic examinations were unremarkable.
cAse report

cAse report
3� Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
Discussion
The term endometriosis was coined in the late 19th century by Sampson to characterize ectopic tissue possessing histological structure and function of the uterine mucosa.2 It also includes those abnormal conditions which may result not only from invasion of organs and other structure by this tissue, but also from its reaction to menstruation.2 Cutaneous endometriosis is rare and many theories have been put forth to explain to its development. It can be divided into spontaneous and iatrogenic forms, occurring in surgical scars of abdominopelvic surgeries including hysterectomy, cesarean section, episiotomy and laparoscopy.4 The spontaneous form may arise from embolization of endometrial tissue via lymphatic vessels. Iatrogenic endometrioma probably develops by implantation of viable endometrial cells.4 Kerr et al reported one such case of umbilical endometriosis with no medical or surgical history. It can occur spontaneously without any hormonal influence or any other physiological influence.
Some other observers believe that development of endometriosis occurs from pluripotent cells of coelom. This theory explains the presence of endometriosis wherever coelomic epithelium or vestige is present (i.e., umbilicus, in the pelvis and hernial sacs).4
Amongst all cutaneous endometriosis, the umbilicus represents the location of 0.5-1% of all endometrial ectopia.2,4 Dessy et al studied four cases of umbilical endometriosis and clinically described those as small, firm, bluish-pink masses on the umbilicus with
figure 1. Clinical presentation of tender umbilical nodule. figure 3. Histology: Microphotograph showing glandular structures lined by endometrial epithelial cells (H&E stain: 100x).
figure 2. Removal of umbilical endometriotic nodule by giving hemi- circumferential incision around umbilicus.
Her routine hematological investigations were normal. Fine needle aspiration cytology (FNAC)-guided biopsy gave the diagnosis of umbilical endometriosis. The nodule was excised by a lateral hemicircumferential incision around the umbilicus (Fig. 2). The nodular lesion had no connection to deep structures. Histopathology examination of the excised specimen revealed glandular structures lined by endometrial epithelial cells and surrounded by cellular stroma (Fig. 3). These features confirmed the diagnosis of umbilical endometriosis. The woman was discharged on 4th postoperative day with advice of injection depot medroxyprogesterone acetate (150 mg) to be taken intramuscularly monthly. She was absolutely asymptomatic at 3rd and 6th month follow-up.

cAse report
3�Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
diameter varying few millimeters to 6 cm during menstruation.4 The endometrioma might cause pain, increased swelling in the premenstrual phase and may start bleeding during menstruation.4 On examination, the tender umbilical nodule could exude old blood on pressure. The atypical presentation of our case was the presence of cyclical painful umbilical nodule in the lactational amenorrhea for six months. The nodule started releasing blood-stained discharge only after she resumed her normal menstrual cycle. Probably this is the first case of umbilical endometriosis to be reported during lactational amenorrhea phase.
From various literatures we observe that the diagnostic ladder for this rare disease includes accurate history, proper physical examination to identify the pathognomonic signs and FNAC-guided biopsy of the nodule. Ultrasonography shows presence of hyperechogenic structure with small hypoechogenic spots inside with predominant venous pattern and absence of connection to deep fascial plane.4 On magnetic resonance imaging (MRI), umbilical endometrioma appeared as homogenously hypointense on T1 weighted images and shading (i.e. loss of signal within the lesion) on T2 weighted images.5 Treatment is surgical excision by giving hemicircumferential incision
on the inner aspect of umbilicus and repositioning the umbilicus to its original position.4
Conclusion
The combination of typical clinical features and FNAC-guided biopsy or the distinctive ultrasonography findings usually allow a definitive diagnosis of umbilical endometriosis. Though cutaneous endometriosis is very rare, it should still be included in the differential diagnosis of any abdominal lesion that exhibits cyclical variation.
References1. Kerr OA, Mowbray M, Tidman MJ. An umbilical
nodule due to endometriosis. Acta Derm Venereol 2006;86(3):277-8.
2. Rai R, Sathyamoorthy A, D’Souza C. Umbilical endometriosis. J Clin Diagnos Res 2008;2(6):1203-6.
3. Hill AD, Banwell PE, Sangwan Y, Darzi A, Manzies-Gow N. Endometriosis and umbilical swelling. Clin Exp Obstet Gynecol 1994;21(1):28-9.
4. Dessy LA, Buccheri EM, Chiummariello S, Gagliardi DN, Onesti MG. Umbilical endometriosis, our experience. In Vivo 2008;22(6):811-5.
5. Hartigan CM, Holloway BJ. Case report: MR imaging features of endometriosis at the umbilicus. Br J Radiol 2005;78(932):755-7.
n n n

40 Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
AbstrAct
Granulosa cell tumors represent 3-5% of all ovarian neoplasms. The long-term survival rate ranges from 75% to 90%. However, stage III disease, although rare, carries a poor prognosis with a 5-year survival rate of 0-22%. Only 15% of patients are first examined for acute abdomen associated with hemoperitoneum. Our patient, a 42-year-old woman presented with hemoperitoneum Grade III shock. Emergency laparotomy with right-sided ovariotomy was done. Histopathology revealed a granulosa cell tumor. Staging laparotomy was done which revealed Stage III C. Postoperative chemotherapy was given. This case is being presented because of its rarity and rare presentation.
Key words: Granulosa cell tumor, reticulin, Call-Exner bodies, ovary
Rarity but Reality: A Rare Presentation of Granulosa Cellm Sivasundari*, ravi kumar Barua**, Arunita nandy†
*Assistant Professor**Unit Chief†PostgraduateDept. of Obstetrics and GynecologySri Ramachandra Medical College and Research Institute, ChennaiAddress for correspondenceDr M Sivasundari,Assistant ProfessorDept. of Obstetrics and GynecologySri Ramachandra Medical College and Research InstituteChennai, Tamil NaduE-mail: [email protected]
Sex cord stromal tumor accounts for 5-8% of all ovarian malignancies.1 Their extreme rarity represents a limitation in understanding their
natural history, management and prognosis.2 Granulosa cell tumors account for approximately 70% of ovarian sex cord stromal tumors and represents 3-5% of all ovarian neoplasms.3-9 Surgery remains the cornerstone of treatment for patients with sex cord ovarian tumors.2 The prognosis of this tumor is excellent.2
Case Report
A 42-year-old P3L3 sterilized lady reported to the emergency room with complaints of pain abdomen, vomiting and abdominal distention for one day. She had no history of constipation, fever, trauma, bleeding per rectum or bleeding per vaginum. Her last menstrual period was 10 days prior to admission.
On examination, she was found to be pale. Pulse – feeble, 120/min. BP - 60/40 mmHg. She was in Grade III
shock. Systemic examination revealed abdominal distention with guarding and rigidity. There was bilateral forniceal tenderness on per vaginal examination.
Investigations showed severe anemia with hemoglobin 3 g/dl. Ultrasonography (USG) of the abdomen and pelvis showed 8.7 × 8.3 mass in the adnexa with hyperechoic areas. Uterus and left ovary were normal. Free fluid was seen in the abdomen and pelvis needle aspiration was done under USG guidance. Frank blood was aspirated. Emergency laparotomy was done. On laparotomy, hemoperitoneum (2 liters) and ruptured right ovarian mass 10 × 8 cm was present. Left tube and ovary were normal. Right ovariotomy was done. Four units of compatible blood was transfused. Histopathology revealed sex cord stromal tumor with focal granulosa cell component (Fig. 1). Reticulin
figure 1. Magnification is 10x.
cAse report

cAse report
41Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
staining was done, which was positive for granulosa cell (Fig. 2). Immunohistochemistry (Fig. 3) with CD99, which was confirmatory for granulosa cell tumors, was done. Inhibin was done postoperatively, which was within normal limit.
A Surgical and Medical oncology opinion was taken. Staging laparotomy was done after two weeks. Histopathology showed omental deposits from sex cord stromal tumor of the ovary (Fig. 4). It was planned to have six cycles of chemotherapy with BEP regimen. The patient was lost to follow-up after the fourth cycle of chemotherapy.
Discussion
Sex cord stromal tumors of the ovary account for 5-8% of all ovarian malignancies.1 Granulosa cell tumors constitute approximately 70% of ovarian sex cord stromal tumors and represent 3-5% of all ovarian neoplasms.3-9 Granulosa cell tumor, which secretes estrogen, is seen in women of all ages.1 They are found in prepubertal girls in 5% of cases, the remainder are found in women throughout their reproductive and postmenopausal life.1 Grossly, these tumors have a smooth lobulated surface. The solid portions are granular, trabeculated, yellow and grey in color. The granulosa theca cell tumor is probably the most inaccurately diagnosed lesion of the female gonad.1 On microscopy, the classic granulosa cell is round or ovoid with scant cytoplasm. The nucleus contains compact, finely granular cytoplasm suggesting hyperchromatism. Coffee-bean grooved nuclei are common. In the most common variety, the granulosa cells show a tendency to arrange themselves in small cluster or rosettes around a central cavity (i.e. Call-Exner bodies).1
The most common clinical symptoms at presentation are abdominal distention and abdominal pain as a result of the gross size of the tumor and presence of ascites.2 About 15% of patients who have cystic granulosa cell tumor are first examined for acute abdomen, associated with hemoperitoneum.2 Most patients with juvenile granulosa cell tumors present with clinical evidence of isosexual precocious pseudopuberty.10-14 Most women of reproductive age present with menstrual irregularities.1 In postmenopausal women, abnormal uterine bleeding is frequently the initial symptom.1
Surgery remains the cornerstone of treatment for patients with sex cord ovarian tumors.2 Because granulosa cell tumors are bilateral in only about 2% of patients, a unilateral salpingo-oophorectomy is appropriate therapy for Stage Ia tumors in children or in women of reproductive age.1 For perimenopausal and postmenopausal women for whom ovarian
figure 2. Magnification is 25x. It is CD99 immunohistochemistry.
figure 3. Magnification is 10x. It is reticulin stain.
figure 4. Magnification is 10x.

cAse report
42 Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
preservation is not important, a hysterectomy and bilateral-salpingo-oophorectomy should be performed.1 There is no evidence to support the use of adjuvant radiation therapy.1 Although data are inconclusive, 4-6 cycles of BEP regimen in selected patients with Stage III/IV disease is an acceptable regimen.1
The prognosis of this tumor is excellent.2 Average time to recurrence is between five and 10 years.15 The long-term survival rate ranges from 75% to 90% for all stages.2 However, Stage III disease, although rare, carries a poor prognosis with a 5-year survival rate of 0-22%.2
References1. Berek JS. Ovarian and fallopian tube cancer. In: Berek
and Novak’s Gynecology. 14th edition, Berek JS, Natarajan S, (Eds.), Lippincott Williams and Wilkins: Philadelphia 2007:1520-3.
2. Nicoletta Colombo and Gabriella Parma. Ovarian sex cord-stromal tumors. In: Gynecologic Cancer Controversies in Management. 1st edition, Gershenson DM, McGuire WP, Gore M, et al. (Eds.), Elsevier Churchill Livingstone: Philadelphia 2004:503-8.
3. Evans AT 3rd, Gaffey TA, Malkasian GD Jr, Annegers JF. Clinicopathologic review of 118 granulosa and 82 theca cell tumors. Obstet Gynecol 1980;55(2):231-8.
4. Fox H, Agrawal K. Langley FA. A clinicopathologic study of 92 cases of granulosa cell tumor of the ovary with special reference to the factors influencing prognosis. Cancer 1975;35(1):231-41.
5. Björkholm E. Granulosa cell tumors: A comparison of survival in patients and matched controls. Am J Obstet Gynecol 1980;138(3):329-31.
6. Björkholm E, Silfverswärd C. Prognostic factors in granulosa-cell tumors. Gynecol Oncol 1981;11(3): 261-74.
7. Ohel G, Kaneti H, Schenker JG. Granulosa cell tumors in Israel: a study of 172 cases. Gynecol Oncol 1983; 15(2):278-86.
8. Pankratz E, Boyes DA, White GW, Galliford BW, Fairey RN, Benedet JL. Granulosa cell tumors. A clinical review of 61 cases. Obstet Gynecol 1978;52(6):718-23.
9. Schweppe KW, Beller FK. Clinical data of granulosa cell tumors. J Cancer Res Clin Oncol 1982;104(1-2):161-9.
10. Young RH, Dickersin GR, Scully RE. Juvenile granulosa cell tumor of the ovary. A clinicopathological analysis of 125 cases. Am J Surg Pathol 1984;8(8):575-96.
11. Zaloudek C, Norris HJ. Granulosa tumors of the ovary in children: a clinical and pathologic study of 32 cases. Am J Surg Pathol 1982;6(6):503-12.
12. Plantaz D, Flamant F, Vassal G, Chappuis JP, Baranzelli MC, Bouffet E, et al. Granulosa cell tumors of the ovary in children and adolescents. Multicenter retrospective study in 40 patients aged 7 months to 22 years. Arch Fr Pediatr 1992;49(9):793-8.
13. Lack EE, Perez-Atayde AR, Murthy AS, Goldstein DP, Crigler JF Jr, Vawter GF. Granulosa theca cell tumors in premenarchal girls: a clinical and pathologic study of 10 cases. Cancer 1981;48(8):1846-54.
14. Vassal G, Flamant F, Caillaud JM, Demeocq F, Nihoul-Fekete C, Lemerle J. Juvenile granulosa cell tumor of the ovary in children: a clinical study of 15 cases. J Clin Oncol 1988;6(6):990-5.
15. Stenwig JT, Hazekamp JT, Beecham JB. Granulosa cell tumors of the ovary. A clinicopathological study of 118 cases with long-term follow-up. Gynecol Oncol 1979;7(2):136-52.
n n n

43Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
From eMedinewSemedinews section
IVF Pregnancies are Causing Rise in Maternal Mortality Rates
Maternal mortality rates are increasing in according to an editorial in the British Medical Journal. The in vitro fertilization (IVF)-related pregnancies are an additional risk factor for maternal death. A study conducted in The Netherlands, found there were 42 deaths per 1,00,000 IVF pregnancies, compared with six deaths seen among 1,00,000 pregnancies in the general population.
The major causes of maternal death are rare catastrophes, such as hemorrhage and blood clots but the incidence of these problems is increasing, possibly because more pregnant women today have health problems, such as diabetes, obesity or some other chronic condition or also generally older.
One should track IVF-associated risks including ovarian hyperstimulation syndrome to better understand risks associated with IVF.
Just How Bad is Cocaine use during Pregnancy?
Dr Kellie Murphy, co-author of a study in the American Journal of Obstetrics and Gynecology: Women who used cocaine while pregnant had about a one in three chance of having an underweight baby, while women who did not had about a one in 10 chance. An underweight baby is defined as weighing <2,500 grams, or about five and a half pounds.
Women with PCOS may have Four Times the Prevalence of Type 2 DiabetesAccording to a review and meta-analysis published online in the journal Human Reproduction Update, women with polycystic ovary syndrome (PCOS) have a four-fold increased prevalence of type 2 diabetes, independent of body mass index (BMI).
After including 35 studies in the systematic review and 30 in the meta-analysis, the study found that women with PCOS had a 4.48-, 2.48- and 2.88-fold increased prevalence of type 2 diabetes, impaired glucose tolerance (IGT) and the metabolic syndrome, respectively, compared with controls. And, in BMI-matched studies, the corresponding prevalences were increased a respective 4.00-, 2.54- and 2.20-fold.
what is Sec. 314 of the Ipc?
Death Caused by Act Done with Intent to Cause Miscarriage
Sec. 314 IPC provides that whoever, with intent to cause the miscarriage of the woman with child, does any act that causes the death of such woman, shall be punished with imprisonment of either description of a term which may extend to 10 years or shall also be liable to fine. If the act is done without the consent of the woman, shall be punished with imprisonment for life or with punishment above mentioned.
The explanation to this section says that it is not essential to this offence that the offender should know that the act is likely to cause death.A person who attempted to cause miscarriage of a pregnant woman but was unsuccessful in the process and when pregnant girl died several weeks later having developed septicemia without it having been established that the person was responsible for septicemia, the person cannot be held guilty under Sec. 314 of IPC. (Ref: Vatchalabai Maruti Kgar v. State of Maharashtra, 1993 Cri LJ 702 (Bom).
—Dr Sudhir Gupta, Associate Professor, Forensic Medicine & Toxicology, AIIMS
Lab Update
categories of Anemia
Macrocytic/normochromic anemia (increased MCV, normal MCHC)
Folate deficiency (common)B12 deficiency (common)Myelodysplastic syndromes (not uncommon, especially in older individuals)Hypothyroidism (rare)
—Dr Arpan Gandhi and Dr Navin Dang
Medicolegal Update
Lab Update

44 Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
Antiretroviral Triple Therapy may Stem Mother-to-baby Infections
Breastfeeding mothers who have HIV are much less likely to infect their babies if the women receive antiretroviral triple therapy, even before they are sick enough to qualify for it, according to a study in The Lancet.
Methotrexate and Embolization Helpful in Cervical Ectopic Pregnancy
According to a study reported online paper in January 12 Fertility and Sterility, uterine artery embolization in conjunction with methotrexate is an effective conservative treatment of cervical ectopic pregnancy.
Escitalopram, a Nonhormonal Effective Therapeutic Option for Menopausal Hot Flashes
As per a new study reported in the Journal of the American Medical Association (January 19 issue), antidepressant treatment with escitalopram, a selective serotonin reuptake inhibitor (SSRI) significantly reduced frequency and severity of menopausal hot flashes compared with placebo.
emedinews section
What Causes Infertility in Women?
The most common female infertility factor is an ovulation disorder. Other causes of female infertility include blocked fallopian tubes, which can occur when a woman has had pelvic inflammatory disease or endometriosis. Congenital anomalies (birth defects) involving the structure of the uterus and uterine fibroids are associated with repeated miscarriages. Aging is also an important factor in female infertility. The ability for ovaries to produce eggs declines with age, especially after age 35.
—Dr Kaberi Banerjee, Infertility and IVF Specialist Max Hospital; Director Precious Baby Foundation
Infertility Update
n n n
Say no to hCG Diet for Weight LossThe human chorionic gonadotropin (hCG) weight loss diet combines daily injections of hCG with severe calorie restriction, only 500 calories/day. It was first promoted as a weight-loss aid in the 1950s by British physician Dr Albert T. Simeons, who claimed that the hCG regimen caused the body to preferentially burn stored fat, especially fat from the stomach, hips, and thighs. A meta-analysis of 24 studies published in 1995 has concluded that there is no scientific evidence that hCG causes weight loss, redistributes fat, reduces hunger or creates a feeling of well-being.
The FDA has stated that hCG is of no benefit in the treatment of obesity. Nevertheless, the hCG diet has been getting attention because hCG is now available in a sublingual form. No one recommends hCG diet. The calorie intake is too low to provide adequate nutrition. hCG can cause blood clots, headaches, restlessness, depression and dizziness.
The director advertises that he needs a secretary. Necessary skills: Document forming, IT-knowledge and a foreign language. After a couple of days a dog walks in. “I’m an open minded person,” the pale-turned boss stutters, “but I need someone who can form documents…” The dog sits down behind the computer and compiles a totally decent business letter. “Yes, but the IT-knowledge…” The dog quickly writes a little program. “Well, but foreign language?” the totally amazed director asks. “Meow!” says the dog.
Laugh a While
International Medical Science Academy Update
reproductive effects of treatment of cIn
The risk of preterm delivery may increase in women with cervical intraepithelial neoplasia (CIN) who undergo more than one cervical conization. A retrospective study reported that, compared to women with one prior conization, the risk of preterm delivery increased three-fold in women with two prior conizations.

4�Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011
dr nutan AgarwalAssociate ProfessorDept. of Obstetrics and GynecologyAIIMS, New Delhi
PhotoQuiz
Questions1. this patient p1+0+1+1, previous abortion four months back
presented with irregular bleeding. pregnancy test is positive. what is the probable diagnosis?
2. how will you evaluate this case?
3. what should be the treatment?
4. why hysterectomy would have been done in this patient?
Answers1 This patient can be a case of gestational trophoblastic disease.
2. Serum β-hCG should be done after ultrasound β-hCG was >1 lac mIU/ml. A complete work-up is required, which includes X-ray chest, USG abdomen. If X-ray chest is normal, CT chest and scoring has to be done. There is no need for endometrial aspiration for histopathology or therapeutic.
3. Depending on scoring, single or multiagent chemotherapy has to be given.
4. Hysterectomy is done for failed chemotherapy or heavy bleeding. This patient had heavy bleeding for which embolization was done before, but when failed to respond even to multiagent chemotherapy, hysterectomy was performed.
PhotoQuiz
photo Quiz

xxxxxxxxx
4� Asian Journal of Obs and Gynae Practice, Vol. 2, April-June 2011Mail this coupon to : IJCP Publications Pvt. Ltd.Head Office: E - 219, Greater Kailash, Part - 1, New Delhi - 110 048Telefax: 40587513 Mob.: 9891272006Subscription Office: 5E, Merlin Estates, 25/8 Diamond Harbour Road, Kolkata - 700 008Tele No.: 033-24452066 Mob.: 9831363901, E-mail: [email protected], Website: www.ijcpgroup.com
Yes, I am interested in subscribing to the *Institutional Combo Package for one year (Institutional)Yes, I am interested in subscribing to the following journal(s) for one year (Institutional) (Individual)
ISSUES/YEAR INSTITUTIONAL ( Amount)` INDIVIDUAL ( Amount)`JOURNALS
12
4
4
12
4
Asian Journal of
Ear, NoseThroatEar, NoseThroat
4
12 3,500/- 1,650/-
550/-1,200/-
3,500/- 1,650/-
1,200/- 550/-
1,200/- 550/-
1,200/- 550/-
1,200/- 550/-
6 1,500/- 750/-
Payment Information: Total 14,500/- for 1 Year`
Name: ............................................................................................
Speciality: ......................................................................................
Address: ........................................................................................
........................................................................................
Country: ..................................... State: .......................................
Pincode: ....................................
Telephone: ............................... Mobile: ......................................
E-mail: ...........................................................................................
Pay Amount: ......................................................................................
Dated (dd/mm/yyyy): ..........................................................................
Cheque or DD No.: .............................................................................
Drawn on Bank: ................................................................................
Special Discounton Institutional
Packages` 1000/-
Save
Subscription Form (Jan-Dec 2011)
Cheques/DD should be drawn in favor of “M/s IJCP Publications Pvt. Ltd.”
We accept paymentsby Cheque/DD only,Payable at New Delhi.Do not pay Cash.
Subscribe to all JournalsYou Pay 13,500/-`

Flow Chart Dr Garima Kachhawa, Senior Research Associate Prof. Alka Kriplani, Professor and Head of Unit IIDept. of Obstetrics and Gynecology, AIIMS, New Delhi
IntroductionPolycystic ovarian syndrome (PCOS) is a common endocrine disorder associated with psychological, reproductive and metabolic features across the lifespan of a woman.It affects 4-12% of women of reproductive age and represents a major health and economic burden.Recently a community-based prevalence study based on current Rotterdam diagnostic criteria has shown the prevalence to be 11.9-17.8%.
•
••
Polycystic ovarian Syndrome with Infertility: Evidence-based Management
Diagnosis of PCOSCurrently, the ESHRE/ASRM or Rotterdam criteria are the agreed international diagnostic criteria for PCOS.It should be noted that PCOS is a diagnosis of exclusion and conditions including thyroid dysfunction and hyperprolactinemia should be excluded biochemically, whilst rarer conditions should be excluded clinically (Cushing’s syndrome, virilizing tumors, and so on).
•
•
ESHRE/ASRM or Rotterdam criteria (2003) Androgen Excess PCOS Society (2006)Two out of three of the following confirms the diagnosis:
To include both:
— Oligo-ovulation and/or anovulation — Hyperandrogenism (hirsutism and/or hyperandrogenemia)
— Clinical and/or biochemical signs of hyperandrogenism
— Ovarian dysfunction (oligoanovulation and/or polycystic ovaries)
— Polycystic ovaries With exclusion of other etiologies
With exclusion of other androgen excess disorders
Clinical features of PCOSPCOS is a chronic condition with manifestations usually beginning in adolescence then transitioning to include infertility and metabolic complications over time.
Seventy to 80% of women with PCOS presenting with ovarian dysfunction usually manifest as oligomenorrhea/amenorrhea resulting from chronic anovulation/oligo-ovulation.PCOS is the most common cause of anovulatory infertility; affecting 90-95% of women attending infertility clinics.Hirsutism and hyperandrogenism affects 60% of women with PCOS and result from increased synthesis and release of ovarian androgens.Insulin resistance occurs in 50-80% of PCOS women, primarily in those who are overweight.Lean women appear to have less severe insulin resistance.
•
•
•
••Reproductive features Metabolic features Psychosocial features Menstrual dysfunction Insulin resistance AnxietyHirsutism Metabolic syndrome DepressionHyperandrogenism Dyslipidemia Poor self-esteemInfertility Impaired glucose tolerance Reduced quality-of-lifeMiscarriage Type 2 diabetes Negative body imageGestational diabetes Cardiovascular disordersHypertensive disordersEndometrial hyperplasia
Treatment: Targeted approach to therapyTreatment options need to be tailored to the clinical presentation and patient desire. Education on short-term symptoms and long-term risk factors of PCOS is important in allaying anxiety and minimizing the impact of illness in chronic disease. As a prelude to treatment, psychological features need to be acknowledged, discussed and counseling considered, to enable lifestyle change which is unlikely to be successful without first addressing education and psychosocial issues.
••
•
Lifestyle modificationLifestyle change is the first-line treatment in an evidence-based approach in the management of the majority of PCOS women.Furthermore, prevention of excess weight gain should be emphasized in all women with PCOS; both normal and increased body weight. Weight loss of 5-10% has significant clinical benefits such as resumption of regular menses and restoration of ovulation. Incorporating simple moderate physical activity including structured exercise (at least 30 min/day) and low carbohydrate restricted diet increases weight loss and improves clinical outcomes in PCOS.
•
•
•
•
Infertility and overweightLifestyle change (5-10% weight loss and structured exercise).Obesity independently exacerbates infertility and reduces effectiveness of interventions.Maternal and fetal pregnancy risks are greater and long-term metabolic outcomes in the child are related to maternal weight at conception. Overweight women prior to conception should be advised for folate, smoking cessation, weight loss and optimal exercise, prior to additional interventions.Advise women to optimize family planning, given age-related infertility. Individualized stepwise approach for ovulation induction and other assisted reproductive treatments should be offered to these patients.
•
•
•
•
•
•
Medications used to treat infertility in polycystic ovary syndromeMedication Description Indication FDA
CategorySide effects Dose
Clomiphene citrate
Ovulation induction agent
Infertility X Multiple pregnancy/ovarian hyperstimulation, thromboembolism visual disturbances
50-100 mg/day 6
Letrozole Nonsteroidal competitive inhibitor of aromatase
Infertility C Osteoporosis, thromboembolism, MI, hot flashes, arthralgias
2.5 mg/day
Metformin Insulin-sensitizing agent
Insulin resistance; menstrual irregularities
B GI upset, lactic acidosis, increase in homocysteine levels
1,500-2,250 mg/day 10
Pioglitazone Insulin-sensitizing agent
Insulin resistance C CHF, may cause weight gain
30 mg/day
Gonadotropins Ovarian stimulation
Resistant ovaries Multiple pregnancy/ovarian hyperstimulation
37.5-75 IU
GnRh agonist Controlled ovarian stimulation
Resistant ovaries Deficient luteal phase support, premature ovulation
Individualized
GnRh antagonist
Controlled ovarian stimulation
OHSS Mild skin irritation 0.25 µg SC
Drospirenone/ ethinyl estradiol
Oral contraceptive
Menstrual regulator, pre- induction
X Varies Varies
Assisted reproduction techniques: COH/IUI/IVFIVF is a reasonable option, as the number of multiple pregnancies can be kept to a minimum by transferring small numbers of embryos.The optimal stimulation protocol is still under debate and there is need for more RCTs.The increase in the cycle cancellation rate in women with PCOS appears to be due to absent or limited ovarian response or due to increased OHSS, as implantation is not affected in PCOS.Induction of ovulation in combination with IUI is indicated in women with PCOS and an associated male factor and may be proposed in women with PCOS who failed to conceive despite successful induction of ovulation.Currently, double insemination does not appear to enhance the probability of pregnancy as compared with single IUI.
•
••
•
•
Laparoscopic ovarian drillingLaparoscopic ovarian surgery (LOS) can achieve unifollicular ovulation with no risk of OHSS or high-order multiples.Intensive monitoring of follicular development is not required after LOS.LOS is an alternative to gonadotropin therapy for CC-resistant anovulatory PCOS.The treatment is best suited to those for whom frequent ultrasound monitoring is impractical.LOS is a single treatment using existing equipment.The risks of surgery are minimal and include the risk of laparoscopy, adhesion formation and destruction of normal ovarian tissue. Minimal damage should be caused to the ovaries. Surgery should be performed by appropriately trained personnel.
•
•••••
•
Clomiphene citrate, letrozoleCC remains the treatment of first choice for induction of ovulation in most anovulatory women.Selection of patients for CC treatment should take account of body weight/BMI, female age and the presence of other infertility factors.The starting dose of CC should be 50 mg/day (for 5 days) and the recommended maximum dose is 150 mg/day.Results of large trials suggest monitoring by ultrasound or progesterone is not mandatory to ensure good outcome.Life-table analysis of the largest and most reliable studies indicates a conception rate of upto 22% per cycle. Aromatase inhibitors have similar efficacy in inducing ovulation as CC women. Further studies should demonstrate efficacy and safety of aromatase inhibitors.
••
•
•
•
••
Gonadotropins The recommended starting dose of gonadotropin is 37.5-50 IU/day.Adherence to a 14-day starting period at least for the first cycle and small FSH dose increment is less likely to result in excessive stimulation.The duration of gonadotropin therapy generally should not exceed six ovulatory cycles.Low-dose FSH protocols are effective in achieving ovulation in women with PCOS.Intense ovarian response monitoring is required in order to reduce complications and secure efficiency.Strict cycle cancellation criteria should be agreed upon with the patient before therapy is started.Preventing all multiple pregnancies and OHSS is not possible at this time.The routine use of GnRH agonists during ovulation induction with gonadotropins is not recommended.
••
•••
•••
MetforminAt present, use of metformin in PCOS should be restricted to those patients with glucose intolerance.Decisions about continuing insulin sensitizers during pregnancy in women with glucose intolerance should be left to obstetricians providing care and based on a careful evaluation of risks and benefits.Metformin alone is less effective than CC in inducing ovulation in women with PCOS.There seems to be no advantage to adding metformin to CC in women with PCOS.
•
•
••
Stepwise Approach for Ovulation Induction in PCOS
Obese PCOS Lean PCOS
Lifestyle changel Low-fat diet l Active exercise
Clomiphene citrate (CC):50-100 mg o.d. × 5 daysfor 3-6 cycles
No ovulation
Gonadotropins:l Gonadotropin l Gonadotropin + CCl Gonadotropin + Letrozolel CC + Dexamethasone
No ovulation
l In vitro fertilizationl In vitro maturation
l Metformin + CC (Metformin 850 mg b.i.d. for 6-8 weeks; CC 50-100 mg o.d. for 5 days)l Letrozole 2.5 mg o.d. for 5 daysl Laparoscopic ovarian drilling
No ovulation
Ovulation No ovulation
PCOS
Ovulation
Ovulation
Ovulation

in the following sections: In the introduction, state concisely the purpose and rationale for the study and cite only the most pertinent references as background. In the material and methods section describe briefly the plan, the subjects, methods and procedures utilized, and the statistical methods employed. In the results section present the detailed findings. Include mention of all tables, and/or figures. Figures and tables should supplement not duplicate the text. Discussion should consider the results in relation to the hypothesis tested and should be put into context with those reported by other workers. Conclusions drawn should be completely supported by the data in the text.Review and update articles should preferably have highlights emphasizing crucial points in the text, typed on separate pages at the end of the text. Few MCQs (multiple choice questions) based on the text will also help increase readers interest in the article.
References
References must be numbered in the order in which they first appear in the text. Identify references in text, tables and legends by arable numerals in parentheses. The style of reference and abbreviated title of journals must follow that of Index Medicus. For journal references, list all authors when 6 or less, when 7 or more list only first three and add et al. The title of the manuscript will be printed after the author’s names, before the abbreviated title of the journal e.g.,: De Cherney AH, Diamond MP, Lavy G and Polan ML. Endometrial ablation for intractable uterine bleeding. Obstet. Gynecol. 198770:668-670.For book reference list all authors of the book, title, edition, city of publication, publisher, year of publication, chapter and page in that order.Goldrath MH, Garry R. Nd: YAG laser ablation of the endometrium In: Endoscopic Surgery for Gynaecologists 2nd Edition, Sutton C and Diamond N (Eds.), WB Saunders, London 1993:16-21.References should be limited to 20 except for the possible exception of special review articles,The editorial board of the journal has decided to adopt the Vancouver style of uniform requirements for manuscripts submitted to biomedical journals (N Engl J Med 1991;324:421-428) These notes for contributors confirm with the Vancouver style.
Figures
The term figure includes all types of illustrations such as graphs, diagrams, photographs, flow charts and line drawings. Photographs should be supplied in high quality glossy paper usually 127 mm × 173 mm (5" x 7").In case of microphotograph stains used and magnification should be mentioned. Each illustration should bear on its back the figure number, name of the forwarding author and an arrow indicating the top. All illustrations should be submitted in duplicate.
Legends of Figures
Legends for all figures must be typed together in numerical order double spaced on a separate sheet. All illustrations and figures must be referred to in the text and abbreviated as “Fig.”
Tables
Tables should be typed on separate sheets of paper, one table to a page and included at the end of the text. They should be numbered in Arabic numerals. Titles should be brief yet indicate clearly the purpose or content of each table.
Acknowledgement
Acknowledgement should be made to funding institutions and organizations and if to persons, only to those who have made substantial contribution to the study.
Electronic Manuscripts
Electronic manuscripts have the advantage that there is no need for the re-keying of text, thereby avoiding the possibility of introducing errors and fast processing of the article. Format your disk correctly and ensure that only the relevant file (one complete article only) is on the floppy/compact disk. Also specify the type of computer and wordprocessing package used and label the disk with your name and the name of the file on the disk.
The Asian Journal of Obstetrics and Gynaecology is a quarterly journal with wide circulation. The journal provides a medium for the publication of review and update articles on any aspect of Obstetrics and Gynecology practice. It welcomes original articles, case reports, dilemmas of clinical practice, new investigations and surgical techniques in the field of Obstetrics and Gynecology.All communications should be submitted to Editor, Asian Journal of Obstetrics and Gynaecology Practice, E-219, Greater Kailash, Part 1, New Delhi - 110 048.
Editorial Policies
All articles must be submitted to the journal exclusively. A covering letter duly signed should accompany the manuscript and identify the author responsible for correspondence concerning the manuscript. The letter should state that the material contained in the manuscript has not been published and has not been submitted for publication elsewhere. Authors are advised to keep a copy of their manuscript. The preferred medium of submission is on disk with accompanying manuscript. Once the manuscript is published it becomes the property of the journal. The editor shall have the right to edit, condense, alter, rearrange or rewrite approved articles, before publication, without reference to the authors concerned.
Authorship
For manuscripts with multiple authors, each author must qualify by having significantly participated in the study that is reported. Each author must make substantial contributions to first, concept and design or analysis and interpretation of data and second, writing the manuscript or revising it critically for content. Others contributing to the work should be recognized separately in the acknowledgement. Authors should mention their designations, Dept., etc. on the manuscript/covering letter.
General Requirements for Preparation of Manuscripts
The original and one good-quality photocopy of the manuscript and two sets of color/black and white glossy prints of illustrations are required. Manuscripts must be typed double spaced on one side only on white bond paper with 2.5 cm margin at top, bottom and sides. Page numbers should be given consecutively at the top of each page starting with the title page. The authors are not bound to any particular form, however, subject matter should be organized under suitable headings and subheadings such as abstract, introduction, materials and methods, results, discussion, acknowledgements and references. Footnotes should be avoided and their contents incorporated into the text. Articles sent on disks will be given preference.
Title Page
The title page (page 1) should contain the title, names of authors (first name will be shortened to initials), degrees, affiliation of authors i.e., department, section or unit of an institution, hospital or organization and the city, state and or country where it is located, a list of 3-5 key words, and name and address of the author responsible for correspondence.
Abstract
A separate page must accommodate the abstract which should not exceed 200 words. A structured abstract is required for original research articles. A standard abstract is required for review and case report articles.
Structured Abstract
A structured abstract limited to 200 words, should contain the following major headings, objectives(s) study design, results and conclusion(s). The objective(s) reflects the purpose of the study, that is the hypothesis that is being tested. The study design should include the setting for the study, the subjects (number and type), the treatment or intervention, and the type of statistical analysis. The results include the outcome of the study and statistical significance if appropriate. The conclusion(s) state(s) the significance of the results.
Standard Abstract
There are no subheadings in the standard abstract.
TextOnly standard abbreviations are to be used. The full term for which an abbreviation stands should precede its first use in the text unless it is a standard unit of measurement. Regular articles are customarily organized
Guidelines for Authors


F/DX
O/A
JOG
/II/1
/201
1-12