Aesthetic Surgery Journal Retaining Ligaments of the Face ... · of facial anatomy is critical when...
14
Facial Surgery Aesthetic Surgery Journal 33(6) 769–782 © 2013 The American Society for Aesthetic Plastic Surgery, Inc. Reprints and permission: http://www.sagepub.com/ journalsPermissions.nav DOI: 10.1177/1090820X13495405 www.aestheticsurgeryjournal.com A thorough knowledge of the layers, planes, and structures of facial anatomy is critical when performing aesthetic surgery. The retaining ligaments of the face represent an additional dimension of this anatomy and are important in understanding concepts of facial aging and rejuvenation. Since Mitz and Peyronie’s description of the superficial musculoaponeurotic system (SMAS) in 1976, 1 numerous studies have focused on further clarifying the anatomy of the SMAS and its use as a vehicle in facial rejuvenation. 2-11 Plastic surgeons—including Bosse, Papillon, and Furnas— logically realized the importance of the ligamentous attachments of the SMAS to the facial skeleton and deep fascia. 3,12 These ligaments are consistent anatomic struc- tures and are therefore present in predictable locations. The main significance relates to the surgical release of these ligaments to achieve the desired aesthetic out- come. 11-16 Furthermore, they are useful landmarks because of their intimate relationship with branches of the facial nerve. 11,12,14,15,17-23 Significant research describing the retaining ligaments of the face has advanced our knowl- edge in this field. However, these consistent retaining ligaments have been inconsistently named by different investigators due to subjective interpretation. As a result, ligaments were discovered and named, then rediscovered and renamed, which has led to some confusion (Table 1). 11,12,14-16,18,24,25 Perhaps the tedious dissection required to identify the ligaments has contributed to these varia- tions, as well. The purpose of this article is to review and clarify the anatomy of the retaining liga- ments of the face, including their different descriptions, nomenclature, and clinical significance in facial aesthetic surgery. Retaining Ligaments of the Face: Review of Anatomy and Clinical Applications Mohammed Alghoul, MD; and Mark A. Codner, MD Abstract The retaining ligaments of the face are important in understanding concepts of facial aging and rejuvenation. They are located in constant anatomic locations where they separate facial spaces and compartments. Their superficial extensions form subcutaneous septa that separate facial fat compartments. Their main significance relates to their surgical release in order to achieve the desired aesthetic outcome. Furthermore, they have a sentinel role in their anatomic relationship to facial nerve branches. When performing facial aesthetic surgery, plastic surgeons should select a plane of dissection, release the appropriate ligaments depending on the desired aesthetic goals, and avoid nerve injury by using the ligaments as anatomic landmarks. Descriptions of the retaining ligaments are variable in the literature; due to different interpretations of anatomy, several classifications, locations, and nomenclature systems have been proposed. This article will review and clarify the anatomy of the retaining ligaments of the face, including the cheek, mandible, temporal, and periorbital areas. Keywords retaining ligaments, SMAS, facial compartments, facial nerve, facial surgery, anatomy Accepted for publication February 12, 2013. Dr Alghoul is Assistant Professor in the Division of Plastic Surgery at Northwestern University Feinberg School of Medicine, Chicago, Illinois. Dr Codner is Clinical Assistant Professor of Plastic Surgery at Emory University, Atlanta, Georgia. Corresponding Author: Dr Mark A. Codner, 1800 Howell Mill Road, Suite 140, Atlanta, GA 30318, USA. E-mail: [email protected] Special Topic Downloaded from https://academic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 November 2018
Transcript of Aesthetic Surgery Journal Retaining Ligaments of the Face ... · of facial anatomy is critical when...

Facial Surgery
Aesthetic Surgery Journal33(6) 769 –782© 2013 The American Society for Aesthetic Plastic Surgery, Inc.Reprints and permission: http://www .sagepub.com/journalsPermissions.navDOI: 10.1177/1090820X13495405www.aestheticsurgeryjournal.com
A thorough knowledge of the layers, planes, and structures of facial anatomy is critical when performing aesthetic surgery. The retaining ligaments of the face represent an additional dimension of this anatomy and are important in understanding concepts of facial aging and rejuvenation. Since Mitz and Peyronie’s description of the superficial musculoaponeurotic system (SMAS) in 1976,1 numerous studies have focused on further clarifying the anatomy of the SMAS and its use as a vehicle in facial rejuvenation.2-11 Plastic surgeons—including Bosse, Papillon, and Furnas—logically realized the importance of the ligamentous attachments of the SMAS to the facial skeleton and deep fascia.3,12 These ligaments are consistent anatomic struc-tures and are therefore present in predictable locations. The main significance relates to the surgical release of these ligaments to achieve the desired aesthetic out-come.11-16 Furthermore, they are useful landmarks because of their intimate relationship with branches of the facial nerve.11,12,14,15,17-23 Significant research describing the retaining ligaments of the face has advanced our knowl-edge in this field. However, these consistent retaining ligaments have been inconsistently named by different
investigators due to subjective interpretation. As a result, ligaments were discovered and named, then rediscovered and renamed, which has led to some confusion (Table 1).11,12,14-16,18,24,25 Perhaps the tedious dissection required to identify the ligaments has contributed to these varia-tions, as well. The purpose of this article is to review and clarify the anatomy of the retaining liga-ments of the face, including their different descriptions, nomenclature, and clinical significance in facial aesthetic surgery.
Retaining Ligaments of the Face: Review of Anatomy and Clinical Applications
Mohammed Alghoul, MD; and Mark A. Codner, MD
AbstractThe retaining ligaments of the face are important in understanding concepts of facial aging and rejuvenation. They are located in constant anatomic locations where they separate facial spaces and compartments. Their superficial extensions form subcutaneous septa that separate facial fat compartments. Their main significance relates to their surgical release in order to achieve the desired aesthetic outcome. Furthermore, they have a sentinel role in their anatomic relationship to facial nerve branches. When performing facial aesthetic surgery, plastic surgeons should select a plane of dissection, release the appropriate ligaments depending on the desired aesthetic goals, and avoid nerve injury by using the ligaments as anatomic landmarks. Descriptions of the retaining ligaments are variable in the literature; due to different interpretations of anatomy, several classifications, locations, and nomenclature systems have been proposed. This article will review and clarify the anatomy of the retaining ligaments of the face, including the cheek, mandible, temporal, and periorbital areas.
Keywordsretaining ligaments, SMAS, facial compartments, facial nerve, facial surgery, anatomy
Accepted for publication February 12, 2013.
Dr Alghoul is Assistant Professor in the Division of Plastic Surgery at Northwestern University Feinberg School of Medicine, Chicago, Illinois. Dr Codner is Clinical Assistant Professor of Plastic Surgery at Emory University, Atlanta, Georgia.
Corresponding Author:Dr Mark A. Codner, 1800 Howell Mill Road, Suite 140, Atlanta, GA 30318, USA. E-mail: [email protected]
Special Topic
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018

770 Aesthetic Surgery Journal 33(6)
DefiniTion AnD ClASSifiCATion
The retaining ligaments of the face are strong and deep fibrous attachments that originate from the periosteum or deep facial fascia and travel perpendicularly through facial layers to insert onto the dermis.11,12,14 These ligaments act as anchor points, retaining and stabilizing the skin and superficial fascia (SMAS) to the underlying deep fascia and facial skeleton in defined anatomic locations (Figure 1). Furnas is credited for first using this retaining ligament terminology when he described the retaining ligaments of the cheek.12 Microscopically, each ligament is rooted in a tree-like distribution as a periosteal or deep fascial thick-ening that divides as it approaches the SMAS into numer-ous branches, which insert onto the dermis as described by Mendelson.14 This branching network of fibers is called the retinacular cutis, which is part of a larger complex system of fibrous septa in the subcutaneous layer, described by Gosain et al2 as the “fascial fatty layer” of the face. It is likely that the superficial extensions of the retaining ligaments into the subcutaneous layer (retinacular cutis) contribute to the formation of septa that divide this layer into the fat compartments of the face.26,27 This theory is supported by the fact that some of these subcutaneous septal boundaries overlap with the location of the deeply seated retaining ligaments. Together, both the retaining ligaments and the subcutaneous fibrous septa create zones of adhesion and divide the face into superficial and deep compartments.
Stuzin et al11,28 classified the retaining ligaments as (1) osteocutaneous ligaments originating from the periosteum, such as the zygomatic and mandibular cutaneous liga-ments, and (2) fasciocutaneous ligaments, which coalesce between the superficial and deep fasciae of the face, as with the masseteric and parotid cutaneous ligaments.
Knize24 and Moss et al18 considered a true retaining liga-ment to be a cylindrical arrangement of fibrous tissue that meets the above-mentioned microscopic criteria and inserts directly into the dermis. Examples of true retaining liga-ments, per this definition, are the zygomatic and masse-teric retaining ligaments. Moss et al described other forms of ligamentous attachments, mainly in the temporal and periorbital area, in the form of septa and adhesions. According to Knize and Moss, septa and adhesions are not considered true retaining ligaments since they do not insert directly onto the dermis; instead, the septa exert a direct effect on the SMAS and an indirect effect on the dermis through the retinacular cutis. The authors suggested using a broader term—ligaments of the superficial tissues—to include these other forms of attachments, instead of refer-ring to the entire group as retaining ligaments.18
This classification system (which, again, includes liga-ments, septa, and adhesions), while sound from the mor-phological and structural standpoints, is not without flaws. The orbitomalar ligament, also known as the orbicularis retaining ligament, is morphologically a septal structure, but it should be considered a true ligament according to the Moss et al18 classification since it does attach directly to the dermis.25,29 The zygomatic cutaneous ligaments located posteriorly along the zygomatic arch take a septal form,28,30 while the anterior ones over the junction of the arch and body of the zygoma take a more cylindrical form.14,18 Despite this, these structures are still considered true retaining ligaments in the Moss et al clas-sification. Mendelson et al17 indicated that the retinacular cutis could not be seen in the area of the zygomatic cuta-neous ligaments medial to the zygomaticus major muscle, which means that direct dermal attachment was not histo-logically proven; however, the zygomatic cutaneous liga-ments are considered true retaining ligaments. Finally, the lateral temporal-cheek fat compartment described by Rohrich and Pessa26 has both the superior and inferior temporal septa as its boundaries (Figure 2), which means that both of these septa should have a superficial exten-sion connecting the superficial temporal fascia to the der-mis (ie, they should connect directly to the dermis). Therefore, we prefer using the term retaining ligaments of the face to describe all the above-mentioned ligamentous attachments of the face.
Anatomy
Retaining Ligaments of the Temporal AreaThere is no consensus in the literature on the accurate description and nomenclature of the retaining ligaments of the temporal area.18,24,31-33 There is agreement, however, on the general location of these ligaments. Knize24,32,33 described a zone of adhesion (also called the zone of fixa-tion) as a 6-mm-wide zone located immediately medial to the superior temporal fusion line where the galea and the periosteum are fixed to bone. At the distal end of the zone of adhesion on the supraorbital rim is a strong ligament, which he named the orbital ligament. He also described a
Table 1. Nomenclature of Facial Ligaments in the Literaturea
Orbitomalar ligament (Kikkawa et al25) Orbicularis retaining ligament (Muzaffar et al16)
Superficial lateral canthal tendon (Knize24) Lateral orbital thickening (Muzaffar et al16)
Zone of adhesion (Knize24) Superior temporal septum (Moss et al)
Orbital ligament (Knize24) Temporal ligamentous adhesion (Moss et al)
Orbicularis-temporal ligament (Knize24) Inferior temporal septum (Moss et al18)
Anterior platysma-cutaneous ligament (Furnas12)
Masseteric cutaneous ligament (Stuzin et al11)
Platysma-auricular ligament (Furnas12)Platysma-auricular fascia
(Mendelson14,15)
Parotid cutaneous ligament (Stuzin et al11)
aNote that the nomenclature in each row describes ligamentous structures that occupy the same anatomic location but were given different names by various authors.
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018

Alghoul and Codner 771
narrow band of fusion between the superficial and deep temporal fasciae, which he named the orbicularis-temporal ligament.24 Moss et al18 divided the ligamentous attach-ments of the temporal area into septa, ligamentous adhe-sions, and areas of thickening around the orbital rim, which they referred to as thickenings of the periorbital septum. They also divided the temporal fusion line and zone of adhesion described by Knize into a superior septum (supe-rior temporal septum) and a caudal adhesion (temporal ligamentous adhesion) (Figure 3). Although the temporal ligament described by Moss et al is synonymous with Knize’s orbital ligament, they each had a slightly different location. The temporal ligament, or temporal ligamentous adhesion, was described as a 15 × 20-mm area of adhesion located 10 mm cephalad to the orbital rim, while the orbital ligament was described as a ligament located on the orbital rim.18,24 Moss et al described the temporal ligament as the keystone area for its communication with 3 ligaments: the superior temporal septum superiorly, the inferior temporal septum laterally, and the supraorbital ligamentous adhesion medially (Figure 3). The inferior temporal septum is roughly similar in location to what was described by Knize24,33 as the orbicularis-temporal ligament (Table 1).
Similarly, the presence of ligaments in the forehead area is controversial. Some authors considered the fore-head devoid of named ligaments and instead as being stabilized by the supraorbital and supratrochlear neuro-vascular bundles, which act as retaining ligaments.24 Others described ligamentous attachments such as the supraorbital ligamentous adhesion and superolateral, superomedial, and inferomedial ligaments.18,34 Moss et al18 considered the supraorbital ligamentous adhesion to be the same area that Knize24,32,33 described as zone B of the forehead (the lower 2 cm of the forehead), where the deepest layer of the deep galea is adherent to the periosteum and where periosteal elevation is particularly difficult.
Retaining Ligaments of the Periorbital AreaThe orbicularis retaining ligament, also known in the ocu-loplastic literature as the orbitomalar ligament, is the main periorbital retaining ligament. It is an osteocutaneous liga-ment that originates from the periosteum of the orbital rim, traversing the orbicularis oculi muscle and inserting into the skin of the lid-cheek junction (Figure 1).25,29 In 1963, Hagriss35 described a fascial extension that passed
Figure 1. Anatomic locations of the retaining ligaments of the face.
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018

772 Aesthetic Surgery Journal 33(6)
from the orbital rim to the orbicularis muscle and skin. Kikkawa et al25 was the first to describe this ligament ana-tomically and histologically, and they named it the orbito-malar ligament. Histological analysis showed that the ligament “fanned out” in a lamellar fashion as it traveled through the orbicularis oculi and the SMAS to the skin, similar to the retinacular cutis.25,36
Muzaffar et al16 detailed the anatomic description of this ligament and renamed it the orbicularis retaining liga-ment. His characterization of this retaining ligament was conceptually similar to that by Kikkawa et al25; they said that the ligament is a septal structure originating from the periosteum just outside the inferior orbital rim, in close proximity to the septum orbitale, and inserting on the deep-surface orbicularis oculi muscle. The ligament is ill-defined at the medial origin of the orbicularis, where the muscle fibers are tightly adherent to the orbital rim perios-teum to the level of the medial corneoscleral limbus. Lateral to this point, the muscle separates anteriorly from the rim periosteum and becomes attached to it through the septum-like orbicularis retaining ligament.16 In a recent anatomic study that included 48 hemifaces, Wong et al29
confirmed the presence of a well-defined ligament in this medial adherent area of the orbicularis, which they named the tear trough ligament. This ligament originates from the maxillary periosteum immediately inferior to the orbital rim, sandwiched between and separating the origins of the palpebral and orbital portions of the medial orbicularis oculi muscle. It terminates at the medial corneoscleral limbus, where it becomes continuous with the orbicularis retaining ligament.29 The orbicularis retaining ligament then lengthens in an anterior-posterior dimension to a maximum length of 10 to 20 mm16,29 and then shortens until it reaches the lateral orbital rim, where it terminates in an area of fibrous thickening called the lateral orbital thickening.16,18 The importance of the lateral orbital thick-ening area, also known as the “superficial lateral canthal tendon,”37 is that it indirectly connects the orbicularis retaining ligament to the lateral canthal tendon through the orbicularis deep fascia (septum orbitale) and the tarsal plate, forming a single anatomic unit.16,37 Ghavami et al38 confirmed the circumferential nature of the orbicularis retaining ligament in a cadaver study using an operating microscope. The ligament was noted to be present over
Figure 2. Superficial facial fat compartments and their relationship to the retaining ligaments.
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018

Alghoul and Codner 773
the superior orbital rim as a distinct structure, separate from the septum orbitale.36,38 Wong et al29 named this superior portion of the orbicularis retaining ligament the periorbital septum of the upper orbit.18
Retaining Ligaments of the Cheek and MandibleFurnas12 was the first to describe the anatomy of the retaining ligaments of the cheek. His description included the zygomatic, anterior platysma-cutaneous, mandibular, and platysma-auricular ligaments. Stuzin et al11,28 refined our knowledge of the ligaments and renamed the platysma-cutaneous ligaments as the masseteric ligaments. Most of the work to define the anatomy of the zygomatic and mas-seteric cutaneous ligaments—championed by Stuzin, Mendelson, and others—was done alongside their attempts to describe the surgical anatomy of the extended SMAS facelift for correction of the nasolabial fold.11,13-15,28,39-41 Despite the variation in published descriptions, the zygo-matic ligaments occupied a predictable anatomic location given their relationship to the body and arch of the zygoma. The masseteric ligaments, on the other hand, were less predictable and varied in location given the fact that they are condensations of the deep fascia.11,13,15,30,39
Zygomatic and masseteric ligaments. The zygomatic cuta-neous ligaments are strong fibers that originate at the inferior border of the zygomatic arch and extend anteriorly to the junction of the arch and body of the zygoma.11,12,13,30
These ligaments can take the form of fibrous septa, mainly posteriorly along the arch, and can have a cylindrical shape closer to the origin of the zygomaticus major muscle. The zygomatic ligaments are considered true ligaments due to their direct attachments to dermis. This is mani-fested by skin dimpling that occurs when the surgeon pulls on the cutaneous end of the cut ligament.12
Mendelson et al17,41,42 described zygomatic ligaments medial to the junction of the arch and body, located along the origins of the facial expression muscles (the zygo-maticus major, zygomaticus minor, and levator labii supe-rioris). These ligaments are weaker and often can be disrupted by blunt finger dissection. The masseteric cuta-neous ligaments arise from the masseteric fascia over the masseter muscle.11,28 Their relationship to the muscle is controversial. While some anatomic studies have shown the ligaments arising along the anterior border of the mas-seter,11,28,39 others have shown them to arise 1 to 2 cm posterior to the anterior border14 and even from the mid-dle portion of the muscle.13 Owsley39 described the mas-seteric ligaments as a vertical septum, while other authors, although they did not directly address the morphology or structure, seemed to address them as individual liga-ments.11,13,14,17,28,30 As the zygomatic and masseteric liga-ments were often described together, Mendelson41,42 stated that they take an inverted L shape, with the horizontal limb extending medially across the origin of the muscles of facial expression and the vertical limb formed by the
Figure 3. Retaining ligaments of the temporal area as described by Knize24,32,33 and Moss et al.18 The overlap of color codes suggests similarity in location, despite different nomenclature.
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018

774 Aesthetic Surgery Journal 33(6)
masseteric ligaments. The main zygomatic ligament is located at the angle of the “L,” just lateral to the zygo-maticus major muscle. Stuzin et al28 differed in what they considered a particularly stout zygomatic ligament, which they indicated is located just medial to the zygomaticus minor muscle. Looking at the various illustrations and considering the zygomatic ligaments along the arch, it seems that both zygomatic and masseteric ligaments form, roughly, a T-configuration. The junction of the “T” is near the origin of the zygomaticus major muscle, where both zygomatic ligaments (main zygomatic) and masseteric ligaments (upper masseteric) are stronger (Figure 1).
Several studies have attempted to provide measurements for the dimensions and location of the zygomatic ligaments in relationship to different reference points.12,13,30,43 However, it was not always clear which of the zygomatic ligaments were represented by these measurements. Furnas,12 for example, provided measurements for a typical bundle of zygomatic ligaments 3 mm in width and 0.5 mm in thick-ness located 4.5 cm anterior to the tragus. Özdemir et al13 measured the “zygomatic ligament” dimensions at 1.8 to 3.4 cm × 0.29 to 0.34 cm in men and 1.6 to 3.0 cm × 0.27 to 0.33 cm in women and said that these were located 3.9 to 4.8 cm anterior to the tragus. Alghoul et al30 provided measurements for the main zygomatic ligament, which they defined as the largest ligament in close proximity to the origin of the zygomaticus major muscle, as 1.45 × 0.27 cm in dimension and located at a mean of 4.49 cm from the tragus. They also confirmed that men had larger ligaments than women.
McGregor’s patch. The term McGregor’s patch has been used in the literature to describe the zygomatic ligaments. Kaye44 referred to the McGregor’s patch as an adherent area over the malar eminence. Furnas12 used the term syn-onymously with zygomatic ligaments, and so did other authors.11,13,19,28,40 Stuzin et al28 used the term to describe the fibers comprising the zygomatic ligament extending through the malar fat pad, which they also named a “fibrous McGregor’s patch.” Owsley40 described the McGregor’s patch as dense fascial septi that extends from the zygoma, penetrates the superficial fascia, and inserts into the dermis. Later in his article, he mentioned 3 struc-tures—the transverse facial artery, parotid duct, and zygomatic branch of the facial nerve—traveling deep to the parotid-masseteric fascia and penetrating it in the region of McGregor’s cutaneous ligaments. However, he subsequently mentioned that those structures run superfi-cial to the buccal fat pad. Furnas quoted Dr Mar McGregor verbatim in “The Retaining Ligaments of the Cheek,” saying the following of the patch bearing the original author’s name: “It is the area of fibrous attachment between the anterior edge of the parotid fascia and the dermis of the skin of the cheek.” He also added, “In doing a facelift procedure, if it is not necessary to extend your undermining beyond this patch, you are safer to stop before cutting through,” and “If in order to obtain good skin drapage it is necessary to cut through the fibrous attachment, you must be aware that you will cut a blood vessel which should be cauterized on the skin side and on
the parotid fascia side.”12 The blood vessel to which McGregor referred is most likely a perforator off the trans-verse facial artery, which many surgeons use as a clinical landmark to identify this patch. McGregor then added, “As soon as you cut through this patch, you lose the protection of the parotid fascia on your deep side and you will see loose fat with branches of the facial nerve looking at you, hopefully intact . . . running through the loose fat, a little deeper and a little caudad, is the parotid duct . . . as stated above, I have for years emphasized that this patch is a warning sign asking the surgeon to be aware of the road ahead.”12 The description of “loose fat with branches of facial nerve” seems to resemble the buccal fat pad, which is located anterior and inferior to the zygomatic cutaneous ligaments. The buccal fat pad is more anatomically related to the masseteric cutaneous ligaments, which guard its anterior border. It is therefore unclear from McGregor’s description of the patch that bears his name whether he was describing the zygomatic cutaneous ligaments or more inferiorly located ligaments such as the upper mas-seteric or the masseterics. It should be noted that when McGregor described this “patch,” none of the retaining ligaments of the face had been discovered or named. In addition, a “patch” configuration of the retaining liga-ments of the cheek is not commonly found. On the basis of these facts, we recommend that the term McGregor’s patch, other than having a historical significance, should have no place in the modern anatomic terminology of the retaining ligaments of the face.
Platysma auricular ligament/fascia. Furnas described the platysma-auricular ligament as arising from the parotid fascia and anchoring the posterior border of the platysma to the anterior inferior preauricular skin (Figure 1). According to the classification by Stuzin et al,11,28 this ligament is considered a parotid cutaneous ligament. It is the first ligament encoun-tered during a facelift procedure. The other parotid cutaneous ligaments arise from the parotid fascia over the parotid gland and vary in size, density, and configuration depending on the size and extent of the parotid gland.45 Mendelson46 expanded the description of the platysma-auricular ligament to include an area of adhesion over the parotid gland extending just anterior to the ear cartilage for 25 to 30 mm. He named this area the platysma auricular fascia.
Mandibular ligament. The mandibular ligament is an oste-ocutaneous ligament that arises from the anterior third of the mandible and inserts directly into the dermis.11-13 Its fibers penetrate the inferior portion of the depressor anguli oris muscle.47 Furnas12 described 2 tiers of linear series of parallel fibers 2 to 3 mm from each other, located 1 cm from the inferior border of the mandible. Özdemir et al13 confirmed the presence of 2 distinct fibrous attachments and confirmed histologically the connection between the periosteum and overlying skin. Langevin et al47 reported on the dimensions of the mandibular ligaments measuring 2 cm horizontally × 1.2 cm vertically and located 4.5 cm anterior to the angle of the mandible. Reece et al48 identi-fied another osteocutaneous ligamentous structure that travels as a posterior extension of the mandibular ligament
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018

Alghoul and Codner 775
originating 1 cm superior to the border of the mandible. They named this structure the mandibular septum. This septum extends from the mandibular ligament anteriorly and ends abruptly posteriorly at another vertical septum that forms the anterior border of the lateral temporal–cheek fat compartment (Figure 1).
Facial CompartmentsAs stated earlier, the retaining ligaments of the face are present in certain locations over the facial skeleton to stabilize the soft tissue planes. They extend through all the concentric layers and bind them together in fixed immobile points. The areas in between the ligaments are spaces and compartments where facial movements take place.17,18,49,50 The diversion of the ligaments into the reti-nacular cutis in the subcutaneous layer connects the super-ficial fascia (SMAS or its equivalent) to the dermis and enables these layers to move as a single unit during facial expression.2,14 As the ligaments divide the sub-SMAS plane into deep facial compartments, the retinacular cutis, with their fibrous septa, divide the pre-SMAS plane, which is the subcutaneous layer, into fat compartments.
Knowledge of the deep facial spaces and compartments is important during facial rejuvenation, since they influ-ence the type and level of dissection performed. Dissection through a space in a sub-SMAS plane can be performed in a blunt fashion, while dissection through the boundaries of the space (the retaining ligaments) requires sharp dis-section. Also, the level and difficulty of dissection may differ between compartments; for example, a dissection plane is often transitioned from a sub-SMAS plane in the temporal compartment to a subperiosteal plane in the forehead compartment. These 2 compartments are sepa-rated by the zone of adhesion, per Knize’s description,24,32 or the superior temporal septum and temporal ligamen-tous adhesion, per Moss et al.18 Similarly, the superior temporal septum and the inferior temporal septum divide the temporal space into 2 compartments, the upper and lower temporal compartments. The upper temporal com-partment is bounded superiorly by the superior temporal septum and inferiorly by the inferior temporal septum. No important structures pass through this compartment, and dissection can proceed bluntly through the loose areolar tissue. The inferior temporal compartment, on the other hand, is bounded superiorly by the inferior temporal sep-tum and inferiorly by the zygomatic cutaneous ligaments overlying the zygomatic arch, and it contains important anatomic structures such as the temporal branches of the facial nerve, the sentinel vessels, and branches of the zygomaticotemporal nerve.18 Careful dissection should be performed when entering the inferior temporal compart-ment to protect these “at-risk” structures.
The orbicularis retaining ligaments form the superior and inferior boundaries of the orbital compartments of the upper and lower lid, respectively—also called the preseptal space.16,17,26 The orbicularis retaining ligament of the lower eyelid also forms the superior border of the prezygomatic space, while the inferior border is formed by the medial zygomatic cutaneous ligaments.17,51 The lateral zygomatic cutaneous ligaments over the zygomatic arch, on the other
hand, separate the temporal space from the lateral cheek compartment. The masseteric cutaneous ligaments separate the lateral cheek compartment and premasseter space over the lower masseter from the masticator space containing the buccal fat pad.49,50 Similarly, the location of the retaining ligaments overlaps with some of the boundaries of the super-ficial fat compartments of the face described by Rohrich and Pessa.26,27 The orbicularis retaining ligament forms the supe-rior border of the nasolabial and medial fat compartments. These 2 compartments combine to form the malar fat pad, an important structure in midfacial aging.52 Elevation and repositioning of the malar fat pad has been described for midface aesthetic enhancement.40,53,54 The zygomatic liga-ments overlap with the more superficial superior cheek sep-tum, separating the lateral orbital compartment from the middle fat compartment. The masseteric cutaneous liga-ments overlap with the septum, separating the middle and medial fat compartments. The temporal portion of the lateral temporal–cheek fat compartment is bounded superiorly by the superior temporal septum and inferiorly by the inferior temporal septum, while the lateral orbital compartment is sandwiched between the inferior temporal septum superiorly and the superior cheek septum inferiorly. The platysma-auricular ligament corresponds to the plane between the lateral temporal cheek compartment and the postauricular fat compartment.26,27 Finally, the mandibular ligament forms the anterior border of the inferior jowl fat compartment, while the mandibular septum separates both the superior and infe-rior jowl fat compartments superiorly from the submandibu-lar jowl-fat compartment inferiorly48 (Figure 2).
Relationship of the Retaining Ligaments to Nerve BranchesOne of the most fascinating aspects of the anatomy of the retaining ligaments of the face is their spatial relationship to facial nerve branches (Figure 4).* Since the ligaments can be used as landmarks to navigate facial nerve and sensory branches, knowledge of this relationship is critical for safe release of the ligaments while avoiding nerve injury. The inferior temporal septum is a landmark for the temporal branches of the facial nerve that pass just medial and parallel.18,24 These branches travel in close proximity to the undersurface of the superficial temporal fascia and are elevated with the flap.18-23 Approaching and releasing the inferior temporal septum should be a warning sign for the surgeon to slow down and perform careful dissection, making sure to “stay down” on the deep temporal fascia.
The orbitomalar ligament has an intimate relationship to the zygomaticofacial nerve branches located just inferior to the lateral aspect of the ligament. However, these branches can be compromised without any consequence.55 The zygo-matic retaining ligaments are landmarks for the zygomatic facial nerve branches.11-15,28,30 Furnas12 was the first to show that a zygomatic branch passes in a deep plane just inferior to the zygomatic ligament. Other authors considered the area immediately inferior to the zygomatic ligament to be a danger zone due to the proximity of zygomatic nerve
*References 11, 12, 14, 15, 17-20, 24, 28, 30, 47.
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018

776 Aesthetic Surgery Journal 33(6)
branches.11,14,15,28 A recent study showed that the main zygo-matic and upper masseteric retaining ligaments, located at a mean of 11 mm from each other, create a pathway where an upper zygomatic nerve passes in a deep plane, 4 mm deep to the deep fascia. A lower zygomatic nerve passes just inferior to or penetrates the upper masseteric ligament at a more superficial level, 1 mm deep to the deep fascia, and pierces the deep fascia just distal to the ligament.30 The authors of that study concluded that the area (approximately 1 cm) immediately inferior to the main zygomatic ligament is rela-tively safe, except in 5% to 9% of cases, in which the upper zygomatic nerve gives off a more superficial branch that travels superficial to the zygomaticus major muscle.28,30 Another important observation is that facial nerve branches often penetrate the ligaments. This incidence was reported to be 27% for the zygomatic ligaments and 66% for the mas-seteric ligaments.19,30
The masseteric ligaments are important landmarks for the buccal facial nerve branches. These ligaments guard the nerves, which penetrate the deep fascia and become superfi-cial on top of the buccal fat pad, just distal to the masseteric ligaments.14,15 In other words, releasing the masseteric retain-ing ligaments in a sub-SMAS plane may cause herniation and exposure of the buccal fat pad, with the buccal facial branches lying superficial to it. Langevin et al47 described
the relationship of the marginal mandibular nerve to the mandibular ligaments. In 20 hemifaces, the nerve was found to run just posterior to the mandibular ligament. Finally, the great auricular nerve is anatomically related to the subcuta-neous extension of the platysma-auricular ligament. This septal extension separates the lateral temporal–cheek fat compartment from the postauricular compartment, and the great auricular nerve travels through this septum.26,27
CliniCAl SignifiCAnCeRetaining Ligaments and Facial AgingFacial aging results from a combination of soft tissue descent and volumetric deflation.10,11,15,25,56,57 The loss of tissue elas-ticity combined with repetitive motion from muscle contrac-tion and gravity is believed to cause tissue descent.25 The role of the retaining ligaments in this process is not well defined. Some authors believe that laxity of the retaining ligaments results in laxity and descent of the soft tissue they sup-port.11,13,28,34,40,48 Another school of thought suggests that the ligaments remain relatively strong while the unsupported tissue in between (in the spaces and compartments) descends with time. This phenomenon is responsible for the “stig-mata” of facial aging, manifested in bulges and grooves.49,50,58
Figure 4. Relationship of the retaining ligaments of the face to facial nerve branches.
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018

Alghoul and Codner 777
The location of the retaining ligaments is where these grooves show. Perhaps one of the most notable signs of aging is the nasojugal groove and its lateral extension, the palpe-bromalar groove. These grooves correspond to the location of the tear trough ligament and orbicularis retaining liga-ment, respectively, and mark the location of the lid-cheek junction.17,18,36,38,51
As the orbital septum attenuates with age, the periorbi-tal fat bulges anteriorly against the septum and inferiorly against the orbicularis retaining ligament. The formation of this bulge, combined with volumetric deflation in the upper cheek, leads to accentuation and visibility of the orbicularis retaining ligament at the lid-cheek junction.16,29 Kikkawa et al25 suggested that the orbitomalar ligament, or orbicularis retaining ligament, distends and stretches with aging, which would theoretically lower the lid-cheek junction.59,60 This, however, contradicts Lambros’s find-ings56,57 that the lid-cheek junction is remarkably stable in position over time. The ligament’s V-shape is due to non-uniform length (distance from the orbital rim to muscle insertion), which allows the longest portion at the apex of the “V” to distend more.16,29,36,51 Similarly, the medial limb of the zygomatic cutaneous ligaments, described by
Mendelson et al, contributes to the formation of the mid-cheek grove through the cutaneous extensions.17,49,58 The prezygomatic space is bounded superiorly by the orbicula-ris retaining ligament and inferiorly by the medial limb of the zygomatic ligaments. Bulging and ptosis of this space with age form malar bags and festoons.17
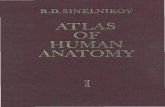
Another classic stigmata of facial aging is formation of jowls, formed by the descent of the premasseteric space, which overlies the lower portion of the masseter.15,49,50 According to Reece et al,48 the superior and inferior jowl fat compartments descend, secondary to attenuation of the man-dibular septum. Either way, as the jowl forms, its anterior extension is limited by the mandibular ligament. The groove that forms just anterior to the jowl corresponds to the man-dibular ligament. Another unique aspect of the mandibular ligament is that its subcutaneous extension (retinacular cutis) can cause skin indentation with aging. Failure to recognize and correct this deformity by subcutaneous release can lead to patient dissatisfaction after facelift surgery (Figure 5).
Concepts of Release and RedrapingAny facial rejuvenation procedure that undermines a superficial fascial flap (SMAS, superficial temporal
Figure 5. Stigmata of facial aging as they relate to retaining ligaments of the face in the form of grooves.
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018

778 Aesthetic Surgery Journal 33(6)
fascia, or platysma) will require release of the retaining ligaments to allow unrestricted mobilization and redrap-ing of the flap. Dividing the ligaments in the sub-SMAS plane will eliminate the restraining effect of the ligament on the flap. By releasing the tethered portion of the
SMAS, the surgeon can effect a change in an area distal to this tethered point. Imagine that point A is the area where the flap was raised and where a pulling force will ultimately be applied to redrape the flap, and point B is the ptotic area in the face that needs to be lifted (Figure 6). If
Figure 6. Concepts for release of the retaining ligaments and redraping of the skin and superficial musculoaponeurotic system (SMAS). Point A is where the dissection starts, and point B is the area of the face that needs to be lifted or tightened. A′ and B′ are locations of points A and B, respectively, after the skin or SMAS flap is pulled. I, subcutaneous facelift; II, SMAS facelift; III, deep plane and composite facelift; and IV, SMAS plication.
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018

Alghoul and Codner 779
the tethering ligament in between is not released, exces-sive force will need to be applied on point A to effect some change in point B. This excessive tension can com-promise the flap and produce unnaturally tight results. If flap elevation is not performed and plication is planned instead, knowledge of the location of the retaining liga-ment will help in carefully choosing the areas of plication to achieve maximum results.
The retaining ligaments can be divided at different levels depending on the plane of dissection. In the subcu-taneous plane, the surgeon will encounter numerous fibrous septa that need to be divided sharply. In the sub-SMAS plane, the main trunk of the ligament is encoun-tered and should also be divided sharply, paying close attention to the location of the facial nerve branches. In the temporal area, remaining on the deep temporal fascia when dividing the ligamentous attachments (the inferior temporal septum or orbicularis-temporal ligament) will protect the frontal branches of the facial nerve. On the contrary, the zygomatic and masseteric ligaments in the cheek should be divided as close as possible to the SMAS, away from the deep fascia, to avoid injuring the zygo-matic and buccal branches. In the subperiosteal plane, the ligament should be lifted with the periosteum using blunt dissection.
When applying this concept to browlifting, point A is the incision site and point B is the brow. The superficial temporal fascia slides over the deep temporal fascia, con-tributing to brow ptosis.24,32 When performing a browlift, a composite flap is raised in the subperiosteal and sub-galeal planes, medial and lateral to the temporal fusion line, respectively. To achieve adequate mobilization of the lateral brow, the intervening ligamentous attachments should be divided.18,24,32-34 In addition to the ligaments, periosteal release should be performed as close as possible to the orbital rim, to avoid inadvertent trauma to the fron-tal facial nerve branches.
Similarly, in the case of the orbicularis retaining ligament, point A is the area of the lower lid subciliary or conjunctival incision, and point B is the area below the lid-cheek junction. Dividing the ligament will facilitate release and redraping of the orbicularis oculi muscle in cosmetic blepharoplasty.61,62 It also allows access through the lower lid for midface lifting63-65 and cheek skin recruitment for lower lid reconstruction. Another important clinical application for the release of the orbitomalar ligament is treating a tear trough deformity and blending the lid-cheek junction with fat transposition across the anatomic area of the ligament66-71 or placement of orbital rim implants.72,73 Other reported clinical uses for the orbicu-laris retaining ligament include its suspension for midface lifting59 and ectropion repair.74
The same concepts apply in facelift procedures regard-less of the technique. In a subcutaneous facelift with or without SMAS plication, the ligaments are divided in the subcutaneous plane, while in a deep plane and composite facelifts, the ligaments are divided in the sub-SMAS plane.75 The parotid cutaneous ligaments or platysma-auricular fascia will be first encountered if the sub-SMAS
dissection is started in the preauricular area. If the preau-ricular area is considered point A, then it seems logical that the release of platysma-auricular fascia would improve the jowl to a greater degree. However, some surgeons do not advocate releasing this adherent area of platysma-auricular fascia, instead starting their dissection superiorly and anteriorly, completely bypassing it.14,15 If a sub-SMAS dissection is not performed, then plicating the mobile SMAS anterior to these ligaments can be as effective.76
To mobilize the SMAS flap in a superior lateral vector, the surgeon should divide the zygomatic retaining liga-ments along the inferior border of the arch. However, lift-ing the midface from a preauricular incision will require the release of the main zygomatic and upper masseteric cutaneous ligaments.† Releasing the lower masseteric liga-ments is usually unnecessary and often leads to the her-niation of the buccal fat pad with the overlying buccal nerve branches. The release of the mandibular retaining ligament in a sub-SMAS plane is unnecessary and could be dangerous since it is located distal, or anterior, to point B (the jowl, in this case) and has an intimate relationship with the marginal mandibular nerve. We hypothesize that in some patients, the cutaneous extension of the mandibu-lar ligament produces a visible indentation at the caudal extension of the marionette line. Dividing the ligament in a subcutaneous plane, at the level of the retinacular cutis, can improve the aesthetic appearance of this area (Figure 7). It should be noted that the shape, density, and distribu-tion of the retaining ligaments of the cheek can be variable among different faces, and each person can have unique ligament topography. Despite this variability, there are some more constant and predictable anatomic locations and relationships such as the zygomaticus major muscle, main zygomatic, and upper masseteric ligaments and their relationship to the zygomatic nerve branches.30 This ana-tomic variability should be recognized when performing a sub-SMAS dissection.
ConCluSionS
The retaining ligaments of the face are important land-marks that occupy predictable anatomic locations. When performing facial aesthetic surgery, plastic surgeons should decide on a plane of dissection, release the appro-priate ligaments depending on the desired aesthetic goals, and avoid nerve injury by using the ligaments as anatomic landmarks. Clarification of the anatomic definitions of the facial retaining ligaments and knowledge of their location, function, and proximity to the SMAS and facial nerves should add to the safety and efficacy of facial aesthetic surgery. Anatomists should be aware of, respect, and acknowledge the anatomic descriptions of the facial retain-ing ligaments to avoid confusion of complex facial ana-tomic structures.
†References 14, 15, 28, 40, 42, 49, 75, 77.
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018

780 Aesthetic Surgery Journal 33(6)
Disclosures
Dr Mohammed Alghoul declared no potential conflicts of interest with respect to the research, authorship, and publica-tion of this article. Dr Mark Codner is a paid consultant for Mentor Corp (Santa Barbara, California) and Syneron Corp (Irvine, California) and receives royalties for books published by Quality Medical Publishing (St Louis, Missouri) and Else-vier (New York, New York).
fundingThe authors received no financial support for the research, authorship, and publication of this article.
RefeRenCeS
1. Mitz V, Peyronie M. The superficial musculoaponeu-rotic system (SMAS) in the parotid and cheek area. Plast Reconstr Surg. 1976;58:80-88.
2. Gosain AK, Yousif NJ, Madiedo G, et al. Surgical anat-omy of the SMAS: a reinvestigation. Plast Reconstr Surg. 1993;92:1254-1265.
3. Bosse J, Papillon J. Surgical anatomy of the SMAS at the malar region. In: Transactions of the IX International Con-gress of Plastic and Reconstructive Surgery. New York, NY: McGraw-Hill; 1987:348-349.
4. Jost G, Levet Y. Parotid fascia and face lifting: a criti-cal evaluation of the SMAS concept. Plast Reconstr Surg. 1984;74:42-51.
5. Wassef M. Superficial fascila and muscular layers in the face and neck: a histological study. Aesthetic Plast Surg. 1987;11:171-176.
6. Thaller SR, Kim S, Patterson H, et al. The submuscular aponeurotic system (SMAS): A histologic and compara-tive anatomy evaluation. Plast Reconstr Surg. 1990;86:690-696.
7. Pensler JM, Ward JW, Parry SW. The superficial muscu-loaponeurotic system in the upper lip: an anatomic study in cadavers. Plast Reconstr Surg. 1985;75:488-494.
8. de Castro CC. The role of the superficial musculoaponeu-rotic system in face lift. Ann Plast Surg. 1986;16:279-286.
9. de Castro C. Superficial musculoaponeurotic system- platysma: a continuous study. Ann Plast Surg. 1991;26:203.
10. Yousif NJ, Gosain A, Matloub HS, Sanger JR, Madiedo G, Larson DL. The nasolabial fold: an anatomic and histo-logic reappraisal. Plast Reconstr Surg. 1994;93(1):60-69.
11. Stuzin JM, Baker TJ, Gordon HL. The relationship of the superficial and deep facial fascias: relevance to rhytidec-tomy and aging. Plast Reconstr Surg. 1992;89:441-451.
12. Furnas DW. The retaining ligaments of the cheek. Plast Reconstr Surg. 1989;83:11-16.
13. Özdemir R, Kilinc H, Unlu RE, et al. Anatomicohistologic study of the retaining ligaments of the face and use in face lift: retaining ligament correction and SMAS plica-tion. Plast Reconstr Surg. 2002;110:1134-1149.
14. Mendelson BC. Extended sub-SMAS dissection and cheek elevation. Clin Plast Surg. 1995;22:325-339.
Figure 7. (A) This 54-year-old woman presented with a prominent mandibular cutaneous ligament and underwent facelift surgery (superficial musculoaponeurotic system plication) and upper and lower blepharoplasty. There was no skin resurfacing performed. Note the circular indentation resulting from subcutaneous extension of the mandibular ligament. (B) The same patient had a facelift and was unhappy with the area caudal to the marionette line. She underwent revision surgery, and the subcutaneous undermining was extended to release the mandibular ligament. The skin was then redraped, achieving the final result shown 6 months postoperatively in this photograph.
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018

Alghoul and Codner 781
15. Mendelson BC. Correction of the nasolabial fold: extended SMAS dissection with periosteal fixation. Plast Reconstr Surg. 1992;89:822-835.
16. Muzaffar AR, Mendelson BC, Adams WP. Surgical anat-omy of the ligamentous attachments of the lower lid and lateral canthus. Plast Reconstr Surg. 2002;110(3):873-884.
17. Mendelson BC, Muzaffar AR, Adams WP Jr. Surgi-cal anatomy of the midcheek and malar mounds. Plast Reconstr Surg. 2002;110:885-911.
18. Moss CJ, Mendelson BC, Taylor GI. Surgical anatomy of the ligamentous attachments in the temple and perior-bital regions. Plast Reconstr Surg . 2000;105:1475-1498.
19. Gosain AK. Surgical anatomy of the facial nerve. Clin Plast Surg. 1995;22:241-251.
20. Owsley JQ, Agarwal CA. Safely navigating around the facial nerve in three dimensions. Clin Plast Surg. 2008;35:469-477.
21. Stuzin JM, Wagstrom L, Kawamoto HK, et al. Anatomy of the frontal branch of the facial nerve: the significance of the temporal fat pad. Plast Reconstr Surg. 1989;83:265-271.
22. Trussler AP, Stephan P, Hatef D, et al. The frontal branch of the facial nerve across the zygomatic arch: anatomi-cal relevance of the high-SMAS technique. Plast Reconstr Surg. 2010;125:1221-1229.
23. Tzafetta K, Terzis JK. Essays on the facial nerve, part I: microanatomy. Plast Reconstr Surg. 2010;125:879-902.
24. Knize DM. Anatomic concepts for brow lift procedures. Plast Reconstr Surg. 2009;124(6):2118-2126.
25. Kikkawa DO, Lemke BN, Dortzbach RK. Relations of the superficial musculoaponeurotic system to the orbit and characterization of the orbitomalar ligament. Ophthal Plast Reconstr Surg. 1996;12:77-88.
26. Rohrich RJ, Pessa JE. The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007;119(7):2219-2227.
27. Rohrich RJ, Pessa JE. The retaining system of the face: histologic evaluation of the septal boundaries of the subcutaneous fat compartments. Plast Reconstr Surg. 2008;121(5):1804-1809.
28. Stuzin JM, Baker TJ, Gordon HL, et al. Extended SMAS dissection as an approach to midface rejuvenation. Clin Plast Surg. 1995;22:295-311.
29. Wong CH, Hsieh MKH, Mendelson B. The tear trough ligament: anatomical basis for the tear trough deformity. Plast Reconstr Surg. 2012;129(6):1392-1402.
30. Alghoul M, Bitik O, McBride J, Zins JE. Relationship of the zygomatic facial nerve to the retaining ligaments of the face: the subSMAS danger zone. Plast Reconstr Surg. 2013;131(2):245e-252e.
31. Knize DM. Galea aponeurotica and temporal fascias. In: Knize DM, ed. Forehead and Temporal Fossa: Anatomy and Technique. Philadelphia, PA: Lippincott Williams & Wilkins; 2001:45.
32. Knize DM. An anatomically based study of the mechanism of eyebrow ptosis. Plast Reconstr Surg. 1996;97(7):1321-1333.
33. Knize DM. The importance of the retaining ligamen-tous attachments of the forehead for selective eyebrow
reshaping and forehead rejuvenation. Plast Reconstr Surg. 2007;119(3):1119-1120.
34. Sullivan PK, Salomon JA, Woo AS, Freeman MB. The importance of the retaining ligamentous attachments of the forehead for selective eyebrow reshaping and fore-head rejuvenation. Plast Reconstr Surg. 1996;117(1):95-104.
35. Hargiss J. Surgical anatomy of the eyelids. Trans Pac Coast Otolaryngol Ophthalmol Soc. 1963;44:193.
36. Hwang K, Nam YS, Kim DJ, Han SH. Surgical anatomy of retaining ligaments in the periorbital area. J Craniofac Surg. 2008;19(3):800-804.
37. Knize DM. The superficial lateral canthal tendon: ana-tomic study and clinical application to lateral cantho-pexy. Plast Reconstr Surg. 2002;109(3):1149-1163.
38. Ghavami A, Pessa JE, Janis J, Khosla R, Reece EM, Rohrich RJ. The orbicularis retaining ligament of the medial orbit: closing the circle. Plast Reconstr Surg. 2008;121(3):994-1001.
39. Owsley J. Superficial musculoaponeurotic system pla-tysma face lift. In: Dudley H, Carter D, Russell R, eds. Operative Surgery. London, UK: Butterworth; 1986.
40. Owsley JQ. Elevation of the malar fat pad superficial to the orbicularis oculi muscle for correction of prominent nasolabial folds. Clin Plast Surg. 1995;22:279-293.
41. Mendelson BC. SMAS fixation to the facial skeleton: ratio-nale and results. Plast Reconstr Surg. 1997;100:1834-1845.
42. Mendelson BC. Surgery of the superficial musculoapo-neurotic system: principles of release, vectors and fixa-tion. Plast Reconstr Surg. 2001;107(6):1545-1552.
43. Hwang K, Kim DH, Kim DJ, Kim YS. Anatomy and ten-sile strength of the zygomatic ligament. J Craniofac Surg. 2011;22(5):1831-1833.
44. Kaye BL. Extended face lift with ancillary procedures. Ann Plast Surg. 1981;6:335-346.
45. Alghoul M, Codner MA. Retaining ligaments of the face. Paper presented at: Southeastern Society of Plastic and Reconstructive Surgery Annual Meeting; June 2-6 2012; Amelia Island, FL.
46. Mendelon B. Facelift anatomy, SMAS retaining ligaments and facial spaces. In: Aston SJ, Steinbrech DS, Walden JL, eds. Aesthetic Plastic Surgery. London, UK: Saunders Elsevier; 2009.
47. Langevin CJ, Engel S, Zins JE. Mandibular ligament revis-ited. Paper presented at: Ohio Valley Society of Plastic Surgery Annual Meeting; May 17, 2008; Cleveland, OH.
48. Reece EM, Pessa JE, Rohrich RJ. The mandibular sep-tum: anatomical observations of the jowls in aging-implications for facial rejuvenation. Plast Reconstr Surg. 2008;121(4):1414-1420.
49. Warren RJ, Aston SJ, Mendelson BC. Face lift. Plast Reconstr Surg. 2011;128(6):747e-764e.
50. Mendelson BC, Freeman ME, Wu W, Huggins RJ. Surgi-cal anatomy of the lower face: the premasseter space, the jowl, and the labiomandibular fold. Aesthetic Plast Surg. 2008;32(2):185-195.
51. Gamboa GM, de La Torre JI, Vasconez LO. Surgical anat-omy of the midface as applied to facial rejuvenation. Ann Plast Surg. 2004;52:240-245.
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018

782 Aesthetic Surgery Journal 33(6)
52. Paul MD, Calvert JW, Evans GRD. The evolution of the midface lift in aesthetic plastic surgery. Plast Reconstr Surg. 2006;117(6):1809-1827.
53. Hamra ST. A study of the long-term effect of malar fat pad repositioning in face lift surgery: short term success but long-term failure. Plast Reconstr Surg. 2002;110:940-951.
54. Owsley JQ. Lifting the malar fat pad for correction of prominent nasolabial folds. Plast Reconstr Surg. 1993;91:463-474.
55. McCord CD, Codner MA. Classical surgical eyelid anat-omy. In: McCord CD, Codner MA, eds. Eyelid and Perior-bital Surgery. St Louis, MO: Quality Medical Publishing; 2008:3-46.
56. Lamros V. Observations on periorbital and midface aging. Plast Reconstr Surg. 2007;120(5):1367-1376.
57. Lambros V. Models of facial aging and implications for treatment. Clin Plast Surg. 2008;35:319-327; discussion 317.
58. Mendelson BC, Jacobson SR. Surgical anatomy of the midcheek: facial layers, spaces and the midcheek seg-ments. Clin Plast Surg. 2008;35:395-404; discussion 393.
59. Korn BS, Kikkawa DO, Cohen SR. Transcutaneous lower eyelid blepharoplasty with orbitomalar suspension: retro-spective review of 212 consecutive cases. Plast Reconstr Surg. 2010;125(1):315-323.
60. Lucarelli MJ, Khwarg SI, Lemke BN, Kozel JS, Dortz-bach RK. The anatomy of midfacial ptosis. Ophthal Plast Reconstr Surg. 2000;16:7-22.
61. Codner MA, Wolfli JN, Anzarut A. Primary transcuta-neous lower blepharoplasty with routine lateral canthal support: a comprehensive 10-year review. Plast Reconstr Surg. 2008;121(1):241-250.
62. McCord CD, Codner MA, Hester TR. Redraping the orbi-cularis arc. Plast Reconstr Surg. 1998;102(7):2471-2479.
63. McCord CD, Codner MA. Lower lid blepharoplasty and midface lift. In: McCord CD, Codner MA, eds. Eyelid and Periorbital Surgery. St Louis, MO: Quality Medical Pub-lishing; 2008:223-268.
64. Hester TR, Codner MA, McCord CD. The “centrofacial” approach for correction of facial aging using the trans-blepharoplasty subperiosteal cheek lift. Aesthetic Surg J. 1996;16:51-58.
65. Hester TR, Codner MA, McCord CD, Nahai F, Giannopou-los A. Evolution of technique of the direct transpalpe-broplasty approach for the correction of lower lid and midfacial aging: maximizing results and minimizing complications in a 5-year experience. Plast Reconstr Surg. 2000;105:393-406.
66. Goldberg RA. Transconjunctival orbital fat repositioning: transposition of orbital fat pedicles into a subperiosteal pocket. Plast Reconstr Surg. 2000;105(2):743-748.
67. Momosawa A, Kurita M, Ozaki M, et al. Transconjuncti-val orbital fat repositioning for tear trough deformity in young Asians. Aesthetic Surg J. 2008;28(3):265-271.
68. Hidalgo DA. An integrated approach to lower blepharo-plasty. Plast Reconstr Surg. 2011;127(1):386-395.
69. Freeman S. Transconjunctival sub-orbicularis oculi fat (SOOF) pad lift blepharoplasty: a new technique for the effacement of nasojugal deformity. Arch Facial Plast Surg. 2000;2:16-21.
70. Hamra ST. Arcus marginalis release and orbital fat pres-ervation in midface rejuvenation. Plast Reconstr Surg. 1995;96(2):354-362.
71. Stutman RL, Codner MA. Tear trough deformity: review of anatomy and treatment options. Aesthetic Surg J. 2012;32(4):426-440.
72. Yaremchuk MJ, Kahn DM. Periorbital skeletal augmen-tation to improve blepharoplasty and midfacial results. Plast Reconstr Surg. 2009;124(6):2151-2160.
73. Yaremchuk MJ. Infraorbital rim augmentation. Plast Reconstr Surg. 2001;107(6):1585-1592.
74. Kahana A, Lucarelli MJ. Adjunctive transcanthotomy lateral suborbicularis fat lift and orbitomalar ligament resuspension in lower eyelid ectropion repair. Ophthal Plast Reconstr Surg. 2009;25(1):1-6.
75. Hamra ST. The deep-plane rhytidectomy. Plast Reconstr Surg. 1990;86:53-63.
76. Robins LB, Brothers DB, Marshall DM. Anterior SMAS plication for the treatment of prominent nasomandibu-lar folds and restoration of normal cheek contour. Plast Reconstr Surg. 1995;96:1279-1288.
77. Warren RJ. The oblique SMAS with malar fat pad ele-vation. Paper presented at: 29th Annual Meeting of the Canadian Society for Aesthetic Plastic Surgery; October 3-4, 2002; Toronto, Ontario, Canada.
Dow
nloaded from https://academ
ic.oup.com/asj/article-abstract/33/6/769/198068 by guest on 24 N
ovember 2018