Advances in Pulmonary Hypertensionpha.files.cms-plus.com/PHAJournal/IssuePDFs/APH v... · Mayo...
56
Vol 13, No 3; 2014 ISSN 1933-088X Pulmonary Hypertension Official Journal of the Pulmonary Hypertension Association Advances in Challenges in Endpoint Development for Pulmonary Hypertension Trials in Children Dunbar Ivy, MD Repurposing FK506 to Increase BMPR2 Signaling and Improve Pulmonary Arterial Hypertension: A Fast Track From Cells to People Edda Spiekerkoetter, MD; Roham T. Zamanian, MD Nitric Oxide erapeutics in Pulmonary Vascular Disease Marc A. Simon, MD, MS PH Grand Rounds: Pulmonary Artery Filling Defects: Are ey All the Same? Nadine Al-Naamani, MD; Richard N. Channick, MD; Ioana R. Preston, MD Roundtable: Reflections on the Scientific Sessions Anna R. Hemnes, MD; Raymond Benza, MD; Karen Fagan, MD; Steven M. Kawut, MD, MS; Jeffrey S. Sager, MD, MSc; Glenna Traiger, RN, MS, CNS-BC Ask the Expert: Should Providers Routinely “Prescribe” Support Group Participation for eir Patients With PAH? Sean M. Studer, MD, MSc PHPN: An Allied Health Professional’s Experience at PHA’s International Conference Chris Archer-Chicko, MSN, CRNP-BC Highlights From PHA’s International Conference: New Treatments and Targets in Pulmonary Hypertension
Transcript of Advances in Pulmonary Hypertensionpha.files.cms-plus.com/PHAJournal/IssuePDFs/APH v... · Mayo...
Vol 13, No 3; 2014
ISSN 1933-088X
Pulmonary HypertensionOff icial Journal of the Pulmonary Hypertension Association
Advances in
Challenges in Endpoint Development for Pulmonary Hypertension Trials in Children Dunbar Ivy, MD
Repurposing FK506 to Increase BMPR2 Signaling and Improve Pulmonary Arterial Hypertension: A Fast Track From Cells to People Edda Spiekerkoetter, MD; Roham T. Zamanian, MD
Nitric Oxide Therapeutics in Pulmonary Vascular Disease Marc A. Simon, MD, MS
PH Grand Rounds: Pulmonary Artery Filling Defects: Are They All the Same? Nadine Al-Naamani, MD; Richard N. Channick, MD; Ioana R. Preston, MD
Roundtable: Reflections on the Scientific Sessions Anna R. Hemnes, MD; Raymond Benza, MD; Karen Fagan, MD; Steven M. Kawut, MD, MS; Jeffrey S. Sager, MD, MSc; Glenna Traiger, RN, MS, CNS-BC
Ask the Expert: Should Providers Routinely “Prescribe” Support Group Participation for Their Patients With PAH? Sean M. Studer, MD, MSc
PHPN: An Allied Health Professional’s Experience at PHA’s International Conference Chris Archer-Chicko, MSN, CRNP-BC
Highlights From PHA’s International Conference: New Treatments and Targets in Pulmonary Hypertension

Editorial Advisory Board
Editor-in-ChiefMyung Park, MDAssociate Professor of MedicineDirector, Pulmonary Vascular Diseases
ProgramDivision of CardiologyUniversity of Maryland School of
MedicineBaltimore, Maryland
Immediate Past Editor-in-ChiefErika Berman Rosenzweig, MDAssociate Professor of Clinical Pediatrics
in MedicineDirector, Pulmonary Hypertension CenterColumbia University College of
Physicians and SurgeonsMorgan Stanley Children’s Hospital of
New YorkNew York, New York
Editor-in-Chief ElectCharles Burger, MDProfessor of MedicineMayo Clinic College of MedicineMedical Director, PH ClinicMayo Clinic FloridaJacksonville, Florida
Associate EditorsHarrison Farber, MDProfessor of MedicineDirector, Pulmonary Hypertension CenterBoston University/Boston Medical CenterBoston, Massachusetts
Deborah Jo Levine, MDAssociate ProfessorPulmonary and Critical Care MedicineLung Transplant PulmonologistDirector of Pulmonary Hypertension CenterDivision of Cardiothoracic SurgeryUniversity of Texas Health Science
Center at San AntonioSan Antonio, TexasSection Editor
Kelly Chin, MDAssistant Professor of MedicineUniversity of Texas Southwestern
Medical CenterDallas, Texas
Fernando Torres, MDDirector, Pulmonary Hypertension ClinicUniversity of Texas Southwestern Medical
CenterDallas, TexasInternational Editor
Editorial BoardLynette M. Brown, MDAssistant Professor of MedicineUniversity of Utah School of MedicineMurray, Utah
Jeffrey D. Edelman, MDAssociate Professor of MedicinePulmonary and Critical Care DivisionUniversity of WashingtonVA Puget Sound Health Care SystemSeattle, Washington
Paul Forfia, MDAssociate Professor of MedicineMedical Director, Pulmonary
Hypertension Program and RightHeart Failure
Temple Heart and Vascular CenterTemple University School of MedicinePhiladelphia, Pennsylvania
Sean Gaine, MD, PhDDirector, National Pulmonary
Hypertension UnitMater Misericordiae University HospitalUniversity College DublinDublin, Ireland
Anna Hemnes, MDAssistant Professor of MedicineAssistant Director, Pulmonary Vascular
CenterVanderbilt UniversityNashville, Tennessee
Dunbar Ivy, MDProfessor of PediatricsUniversity of ColoradoDenver Health Sciences CenterDenver, Colorado
Richard Krasuski, MDDirector of Adult Congenital Heart
Disease ServicesCleveland ClinicCleveland, Ohio
Usha Krishnan, MDAssociate Professor of PediatricsColumbia University Medical CenterAssociate Director, Pulmonary
Hypertension CenterNew York, New York
Ioana Preston, MDCo-Director, Pulmonary Hypertension
CenterTufts Medical CenterBoston, MassachusettsSection Editor
Jonathan Rich, MDAssistant Professor in Medicine-CardiologyNorthwestern University Feinberg School
of MedicineAdvanced Heart Failure and Transplant
CardiologistNorthwestern Memorial HospitalChicago, Illinois
Oksana Shlobin, MDCo-Director, Pulmonary Hypertension
ProgramAssistant Director, Advanced Lung
Disease and Transplant ProgramInova Health SystemFalls Church, Virginia
Sean M. Studer, MD, MScChief of MedicineWoodhull Medical CenterNew York UniversityNew York, New YorkSection Editor
Mary Bartlett, MS, RN, CS, FNPCoordinator, Winthrop University
HospitalPulmonary Hypertension CenterMineola, New YorkPHPN Section Editor
Program DescriptionThe mission of Advances in Pulmonary Hy-pertension is to serve as the premiere forumfor state of the art information regardingdiagnosis, pathophysiology, and treatmentof pulmonary hypertension. The 2008 DanaPoint revision of the World Health Orga-nization Classification serves as a guide tocategories of pulmonary hypertension ad-dressed in Advances in Pulmonary Hyperten-sion. While focusing on WHO Group 1PAH, the other categories (Group 2, pul-monary venous hypertension; Group 3, as-sociated with chronic lung disease and/orhypoxemia; Group 4, pulmonary embolichypertension; Group 5, miscellaneous) arealso addressed. This mission is achieved bya combination of invited review articles,roundtable discussions with panels consist-ing of international experts in PH, and orig-inal contributions.
Objectives● Provide up-to-date information regard-
ing diagnosis, pathophysiology, and treat-ment of pulmonary hypertension.
● Serve as a forum for presentation anddiscussion of important issues in the field,including new paradigms of disease un-derstanding and investigational trialdesign.
The Scientific Leadership Council of the Pulmonary Hypertension AssociationThe scientific program of the Pulmonary Hypertension Association is guided by the association’s Scientific Leadership Council. The Council includes the following health care professionals.
Karen A. Fagan, MDChairChief of Pulmonology, Critical CareProfessor of Internal Medicine and PharmacologyUniversity of South AlabamaMobile, AL
Richard N. Channick, MDImmediate Past ChairAssociate Professor of MedicineHarvard Medical SchoolDirector, Pulmonary Hypertension ProgramMassachusetts General HospitalBoston, MA
Erika S. Berman Rosenzweig, MDChair-ElectAssociate Professor of Clinical Pediatrics in MedicineColumbia Presbyterian Medical CenterNew York, NY
Serpil C. Erzurum, MDChair, Research CommitteeChair, Department of PathobiologyLerner Research InstituteThe Cleveland Clinic FoundationCleveland, OH
Michael A, Mathier, MDChair, PHA Online University CommitteeAssistant Professor of MedicineDirector of Pulmonary Hypertension ProgramUniversity of Pittsburg Medical CenterPittsburgh, PA
Ronald J. Oudiz, MDChair, Insurance Advocacy CommitteeProfessor of MedicineDirector, Liu Center for Pulmonary HypertensionLA Biomedical Research Institute at Harbor-UCLA
Medical CenterTorrance, CA
Myung H. Park, MDEditor-In-Chief, Advances in Pulmonary HypertensionDirector, Pulmonary Vascular Diseases ProgramDivision of CardiologyUniversity of Maryland Medical CenterBaltimore, MD
Robert J. Schilz, DO, PhDChair, Education CommitteeMedical Director, Lung Transplantation and
Pulmonary Vascular DiseaseAssociate Professor of MedicineCase Western Reserve University School of MedicineCleveland, OH
Ian Adatia, MBChBProfessor of PediatricsUniversity of AlbertaDirector, Pulmonary Hypertension ClinicStollery Children’s HospitalAlberta, Canada
Todd M. Bull, MDAssociate Professor of MedicineUniversity of ColoradoDenver, CO
Murali M. Chakinala, MDAssociate ProfessorWashington University School of MedicineDivision of Pulmonary and Critical CareSt. Louis, MO
Lorinda Chung, MDAssistant Professor of MedicineStanford UniversityPalo Alto, CA
Charles D. Burger, MDProfessor of MedicineMayo Clinic College of MedicineJacksonville, FL
Hyong (Nick) Kim, MDAssociate Clinical Professor of Medicine
Director, Pulmonary Vascular MedicineUniversity of California San DiegoLa Jolla, CA
James R. Klinger, MDDirector, Pulmonary Hypertension CenterAssociate Professor of MedicineBrown UniversityProvidence, RI
Irene M. Lang, MDProfessor of Vascular BiologyDeputy Chair, Division of CardiologyMedical University of ViennaVienna, Austria
Roberto F. Machado, MDAssociate Professor of MedicineUniversity of Illinois at ChicagoChicago, IL
Stephen C. Mathai, MD, MHSAssistant Professor of MedicineJohns Hopkins UniversityBaltimore, MD
John H. Newman, MDVanderbilt University School of MedicineNashville, TN
Ioana R. Preston, MDCo-Director, Pulmonary Hypertension CenterAssociate Professor of MedicineTufts University School of MedicineBoston, MA
Virginia Steen, MDProfessor, Division of RheumatologyGeorgetown University Medical CenterWashington, DC
Duncan J. Stewart, MDVice President, ResearchThe Ottawa HospitalOttawa, ON, Canada
Sean Studer, MD, MScChief of MedicineNYU-Woodhull Medical CenterBrooklyn, NY
Fernando Torres, MDHead of Lung Transplant and Pulmonary HTN
ProgramAssociate Professor of Internal MedicineUniversity of Texas Southwestern Medical CenterDallas, TX
Terence Trow, MDAssociate Professor of MedicineDirector, Pulmonary Vascular Disease ProgramSection of Pulmonary and Critical Care MedicineYale School of MedicineNew Haven, CT
Joel A. Wirth, MDDivision of Pulmonary & Critical Care Medicine,
Maine Medical CenterPortland, MATufts University School of MedicineBoston, MA
Roham T. Zamanian, MDAssociate Professor of MedicineStanford School of MedicineStanford, CA
LiaisonsMelisa Wilson, ARNP, ACNP-BC (voting)Chair, PH Professional NetworkOrlando Health Heart InstituteOrlando, FL
Crystal Weber, RN (non-voting)Chair-Elect, PH Professional NetworkChair, PH Professional Network Publications CommitteeDuke UniversityDurham, NC
Rita Orth, RNPHA Board MemberLos Angeles, CA
SLC Distinguished Advisory CommitteeDavid B. Badesch, MDProfessor of MedicineClinical Director, Pulmonary Hypertension CenterUniversity of Colorado Health Sciences CenterAurora, CO
Bruce Brundage, MDProfessor of Medicine EmeritusDavid Geffen School of Medicine at UCLABend, OR
C. Gregory Elliott, MDProfessor of MedicineUniversity of Utah School of MedicineMurray, UT
Michael D. McGoon, MDProfessor of MedicineMayo ClinicRochester, MN
Vallerie V. McLaughlin, MDDirector, Pulmonary Hypertension ProgramProfessor of MedicineUniversity of Michigan CVC Cardiovascular MedicineAnn Arbor, MI
The mission of the Scientific Leadership Council is toprovide medical and scientific guidance and support tothe PHA for:� Developing and disseminating knowledge fordiagnosing and treating pulmonary hypertension.
� Advocating for patients with pulmonary hypertension.� Increasing involvement of basic and clinicalresearchers and practitioners.
More information on PHA’s Scientific LeadershipCouncil and associated committees can be found at www.PHAssociation.org/SLC/

110 Editor’s MemoMyung Park, MD
110 Guest Editor’s MemoAnna R. Hemnes, MD
122 PH Grand Rounds: Pulmonary Artery Filling Defects: Are They All the Same?Nadine Al-Naamani, MD; Richard N. Channick, MD; Ioana R. Preston, MD
125 Challenges in Endpoint Development for Pulmonary Hypertension Trials inChildrenDunbar Ivy, MD
129 Repurposing FK506 to Increase BMPR2 Signaling and Improve PulmonaryArterial Hypertension: A Fast Track From Cells to PeopleEdda Spiekerkoetter, MD; Roham T. Zamanian, MD
134 Nitric Oxide Therapeutics in Pulmonary Vascular DiseaseMarc A. Simon, MD, MS
138 Conference Abstracts
141 Roundtable: Reflections on the Scientific SessionsAnna R. Hemnes, MD; Raymond Benza, MD; Karen Fagan, MD; Steven M.Kawut, MD, MS; Jeffrey S. Sager, MD, MSc; Glenna Traiger, RN, MS, CNS-BC
146 Ask the Expert: Should Providers Routinely “Prescribe” Support GroupParticipation for Their Patients With PAH?Sean M. Studer, MD, MSc
148 PHPN: An Allied Health Professional’s Experience at PHA’s InternationalConferenceChris Archer-Chicko, MSN, CRNP-BC
158 Erratum for “Ask the Expert” Vol 13, No 2, page 92
Advances inPulmonary HypertensionOfficial Journal of the Pulmonary Hypertension Association
CONTENTSPUBLISHERPulmonary Hypertension AssociationKaren A. Fagan, MDRino Aldrighetti, President and CEO
PHA OFFICEPulmonary Hypertension Association801 Roeder Road, Ste 1000Silver Spring, MD 20910301-565-3004; 301-565-3994 (fax)
PUBLISHING OPERATIONSDeborah L. McBride,Managing EditorMcBride Strategic [email protected]
Copyright ©2014 by Pulmonary HypertensionAssociation. All rights reserved. None of thecontents may be reproduced in any formwhatsoever without the written permission ofPHA.
Advances in Pulmonary Hypertension is availableonline at www.PHAOnlineUniv.org/journal
Advances in Pulmonary Hypertension iscirculated to cardiologists, pulmonologists,rheumatologists, and other selected healthcareprofessionals by the Pulmonary HypertensionAssociation. The contents of the articles areindependently determined by the Editor-in-Chief and the Editorial Advisory Board.
Advances in Pulmonary Hypertension: Author Guidelines
General InformationAdvances in Pulmonary Hypertension: Official Journal of thePulmonary Hypertension Association is a quarterly publi-cation directed by an editorial board of renowned expertswith the oversight of the Association’s Scientific Lead-ership Council. Its mission is to help physicians in theirclinical decision making by informing them of importanttrends affecting their practice and providing an analysis ofthe impact of new findings and current information in thepeer-reviewed literature. Each article is reviewed andapproved by members of the Editorial Advisory Board.
While most articles are invited by the editorial board, thefollowing submissions will be considered for publication:
• Reviews that summarize and synthesize peer-reviewedliterature to date on relevant topics
• Letters to the Editor• Clinical case studies
Submitted manuscripts are reviewed by the editorial boardand other experts in the field. Acceptance of manuscriptsis determined by factors such as quality, relevance, andperceived value to clinical decision making.
Manuscript Preparation and Submission ProcessSubmissions should be sent via e-mail as an attachedWord document to the Editor-in-Chief, Myung Park,
MD, at [email protected] Manuscriptsshould be double-spaced and follow AMA style. Full-length manuscripts should not exceed 4,000 wordsincluding references. References should be limited to 50entries. No more than 5 figures should accompany themanuscript. Acceptable file formats are .gif, .tif, and .jpg.Each figure should be a separate file and figure legendsshould appear at the end of the manuscript. Each figureshould be cited by number in the manuscript. Tablesshould be self-explanatory and details of the table shouldnot be repeated in the manuscript. Tables should be pre-pared as part of the Word document. No more than 3tables should be included with the manuscript. Referencesshould conform to AMA style and be numbered consecu-tively in the text. Reference numbers should be placed inparentheses at the end of the relevant sentence.
Accepted manuscripts will be edited for clarity, spelling,punctuation, grammar, and consistency with AMA style.
CopyrightAuthors must confirm they have rights to all material sub-mitted by including a copyright release form with themanuscript. The form can be downloaded from the PHAWeb site, www.PHAssociation.org. Authors acknowledgethe material has not been previously published nor is beingconsidered for publication elsewhere simultaneously withconsideration by Advances in Pulmonary Hypertension.
Any previously published figures, tables, etc. must containa full credit-line from the copyright owner. Authors areresponsible for obtaining permission to reproduce suchmaterial and must provide that material in reproducibleform.
Manuscripts are accepted for exclusive publication inAdvances in Pulmonary Hypertension and will be copy-righted by the Pulmonary Hypertension Association.
Conflict of Interest DisclosuresA statement of any and all grant, contract, and industrialsupport or proprietary interests of the author(s) related tothe subject matter must be submitted with the manuscript.
ChecklistAuthors should be certain to include the following withthe manuscript:
1. Title page listing all authors with their academicdegree(s) and affiliations.
2. Corresponding author contact information includinge-mail and phone number.
3. Copyright release form signed by all authors4. Conflict of Interest forms for all authors5. List of approximately 5 key words for indexing
purposes6. Summary of the paper not exceeding 250 words in the
format of Background; Objectives; Summary/Conclusions
109Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

EDITOR’S MEMO
A Reflection on the Journey toRacing Toward A Cure:The PHA’s 2014 InternationalPH Conference and ScientificSessions
The Pulmonary Hypertension Associa-tion’s conference is like no other. It istruly a one-of-a-kind meeting thatbrings the scientific community togetherwith the patients and their families inthe common goal of sharing informationto help those afflicted with PH. Thismeeting is a living embodiment of themission of the 4 founding women—Dorothy Olson, Teresa Knazik, PatPatson, and Judy Simpson—whotogether set out to eradicate the lone-liness of PH by establishing aPH-focused organization that wouldcreate a network of support for patientsand families, encourage research, andbuild contacts with PH-treating physi-cians. Hence, in 1990 the first issue ofPathlight was published under the orga-nization of United Patient’s Associationfor Pulmonary Hypertension (UPAPH).This was followed by the 1st Interna-tional PH Conference in 1994, held in
Stone Mountain, Georgia where the firstresearch room was created by Dr. GregElliott. His unique idea was the sourceof the blood collections which later con-tributed to the discovery of the geneticmutations associated with PAH. In1997, the organization officially changedits name to Pulmonary HypertensionAssociation and, 1 year later, thePatient’s Survival Guide was published.
The dedicated forces of the like-minded patients and volunteers workingtoward the common goal of increasingawareness and a cure put in motion atrajectory of rapid expansion. Thisdriving mission resulted in the largestconference to date in 2014 with morethan 1500 global attendees. The livinglegacy of the founding women can befelt within the active interchange ofdialogues and questions of theMedically-led Sessions, at the breakfasttables where patients can address ques-tions to physicians and other patients,and in hallways where you see groups ofpeople engaged in sharing experiences,asking questions, and empowering thecommunity with information to bestfight this disease.
The bi-annual conference also hosts aday of state-of-the-art scientific presen-tations from around the world to sharecurrent research. It is my sincere pleasureto present this issue which focuses onthe chosen topics to highlight the latestprogresses in translational research inpulmonary hypertension. I am sincerelygrateful to our guest editor, AnnaHemnes, MD, for inviting key pre-senters to share the findings on novelpathways and signaling systems, as wellas controversies and advances in treatingthe pediatric population with PH. I amalso pleased to present the issue’s featureof PH Grand Rounds of a unique case,roundtable discussions reflecting theachievements of the meeting, and Askthe Expert column contemplating therole of PH support groups. The ongoingwork and accomplishments of the PHcommunity are a tribute to the foundingwomen.
Myung H. Park, MDEditor-in-ChiefUniversity of Maryland School of MedicineBaltimore, MD
GUEST EDITOR’S MEMO
In this issue of Advances in PulmonaryHypertension we focus on the ScientificSessions that occurred in June 2014 atPHA’s 2014 International PH Con-ference. The focus of the ScientificSessions was “New Treatments andTargets in Pulmonary Hypertension.”While this issue highlights several of theinformative and exciting talks that weregiven at the Scientific Sessions, some ofthe many tremendous advances were thegrowing attendance at the Conferenceoverall: more than 1500 people regis-tered;, inspirational interaction withpatients, families and caregivers con-tinued; and cutting edge science waspresented at the poster session the nightprior to the Scientific Sessions. Theunique research room was busy againthis year enrolling patients in what serves
as a tremendous resource to scientistsnow and in the years to come. The dayof the sessions also included thought-provoking debate on the future ofclinical trials in PAH with importantinput from representatives of theNational Institutes of Health.
Our goal was to highlight potentiallytransformative science in all forms ofpulmonary hypertension and in allpatient populations. To that end, talksfocused on pediatric pulmonary hyper-tension as well as new treatment targetsin Group 2 pulmonary hypertension andnew potential therapies in pulmonaryarterial hypertension. The best abstractssubmitted by young investigators werealso presented and are included in thisissue.
This issue is a wonderful synopsis of
the highlights of the Scientific Sessions,but the energy and enthusiasm to find acure for pulmonary hypertension areinadequately sensed on these pages. Asalways, PHA’s International Conferenceand Scientific Sessions fed our appetitefor more research and better care forpatients with pulmonary hypertension. Ithink it is safe to say we all left feelingeager to get back to work!
Anna R. Hemnes, MDAssistant Professor of MedicineAssistant Director, Pulmonary VascularCenterVanderbilt UniversityNashville, TN
110 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

Stimulating*
*Soluble Guanylate Cyclase
What could Adempas mean to your patients?
First and only treatment approved for both PAH and inoperable or persistent/recurrent CTEPH after surgery†
Adempas -US.com
IMPORTANT SAFETY INFORMATION
Please see additional Important Safety Information, including Boxed Warning, throughout and Brief Summary of Prescribing Information at end of advertisement.
WARNING: EMBRYO-FETAL TOXICITY
Do not administer Adempas (riociguat) tablets to a pregnant female because it may cause fetal harm.
Females of reproductive potential: Exclude pregnancy before the start of treatment, monthly during treatment, and 1 month after stopping treatment. Prevent pregnancy during treatment and for one month after stopping treatment by using acceptable methods of contraception.
For all female patients, Adempas is available only through a restricted program called the Adempas Risk Evaluation and Mitigation Strategy (REMS) Program.
†INDICATIONS • Adempas (riociguat) tablets are indicated for
the treatment of adults with persistent/recurrent chronic thromboembolic pulmonary hypertension (CTEPH), (WHO Group 4) after surgical treatment, or inoperable CTEPH, to improve exercise capacity and WHO functional class.
• Adempas is indicated for the treatment of adults with pulmonary arterial hypertension (PAH), (WHO Group 1), to improve exercise capacity, WHO functional class and to delay clinical worsening.‡
Effi cacy was shown in patients on Adempas monotherapy or in combination with endothelin receptor antagonists or prostanoids. Studies establishing effectiveness included predominantly patients with WHO functional class II–III and etiologies of idiopathic or heritable PAH (61%) or PAH associated with connective tissue diseases (25%).
‡ Time to clinical worsening was a combined endpoint defi ned as death (all-cause mortality), heart/lung transplantation, atrial septostomy, hospitalization due to persistent worsening of pulmonary hypertension, start of new PAH-specifi c treatment, persistent decrease in 6MWD and persistent worsening of WHO functional class.
CONTRAINDICATIONSAdempas is contraindicated in:
• Pregnancy. Adempas may cause fetal harm when administered to a pregnant woman. Adempas was consistently shown to have teratogenic effects when administered to animals. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus
• Co-administration with nitrates or nitric oxide donors (such as amyl nitrite) in any form.
• Concomitant administration with specifi c phosphodiesterase-5 (PDE-5) inhibitors (such as sildenafi l, tadalafi l, or vardenafi l) or nonspecifi c PDE inhibitors (such as dipyridamole or theophylline).
WARNINGS AND PRECAUTIONSEmbryo-Fetal Toxicity. Adempas may cause fetal harm when administered during pregnancy and is contraindicated for use in women who are pregnant. In females of reproductive potential, exclude pregnancy prior to initiation of therapy, advise use of acceptable contraception and obtain monthly pregnancy tests. For females, Adempas is only available through a restricted program under the Adempas REMS Program.
Please see additional Important Safety Information, including Boxed Warning, throughout and Brief Summary of Prescribing Information at end of advertisement.
Patients walked farther with Adempas at Week 12: results from Week 2 onward
50%
Adempas could mean moving from the couch to the kitchen
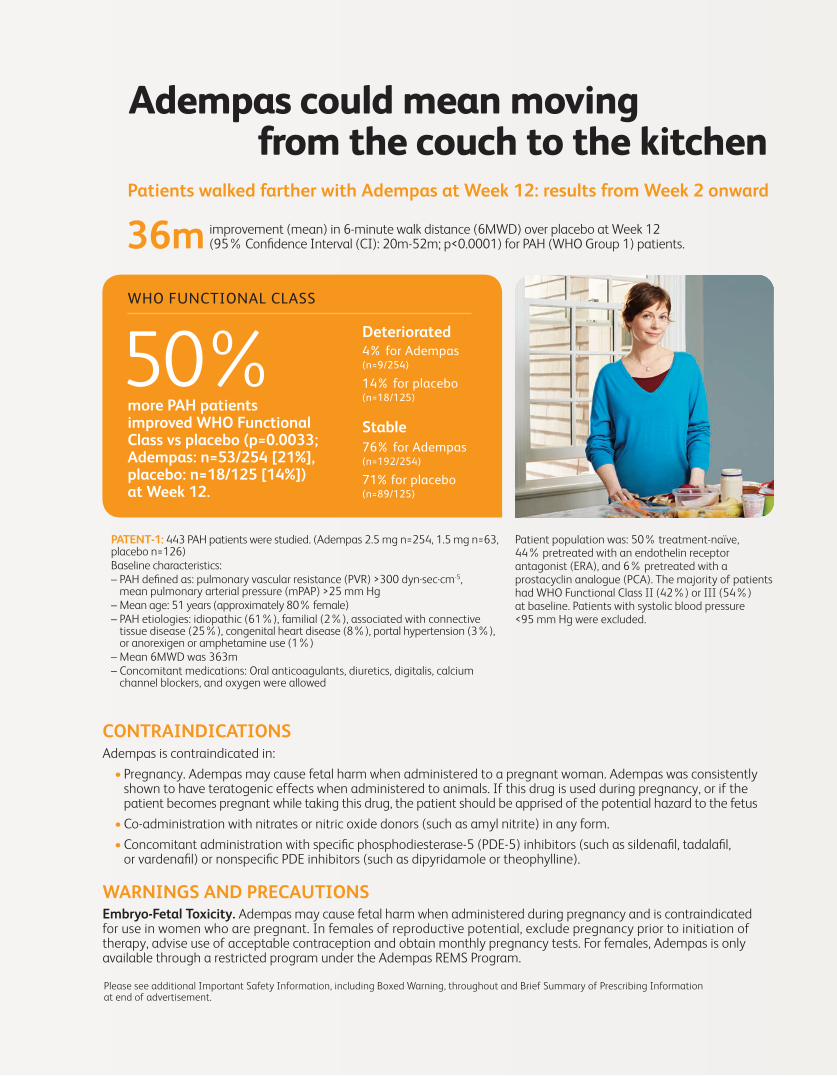
more PAH patients improved WHO Functional Class vs placebo (p=0.0033; Adempas: n=53/254 [21%], placebo: n=18/125 [14%]) at Week 12.
improvement (mean) in 6-minute walk distance (6MWD) over placebo at Week 12 (95% Confi dence Interval (CI): 20m-52m; p<0.0001) for PAH (WHO Group 1) patients. 36m
PATENT-1: 443 PAH patients were studied. (Adempas 2.5 mg n=254, 1.5 mg n=63, placebo n=126)Baseline characteristics: – PAH defi ned as: pulmonary vascular resistance (PVR) >300 dyn·sec·cm-5,
mean pulmonary arterial pressure (mPAP) >25 mm Hg– Mean age: 51 years (approximately 80% female)– PAH etiologies: idiopathic (61%), familial (2%), associated with connective
tissue disease (25%), congenital heart disease (8%), portal hypertension (3%), or anorexigen or amphetamine use (1%)
– Mean 6MWD was 363m – Concomitant medications: Oral anticoagulants, diuretics, digitalis, calcium
channel blockers, and oxygen were allowed
Patient population was: 50% treatment-naïve, 44% pretreated with an endothelin receptor antagonist (ERA), and 6% pretreated with a prostacyclin analogue (PCA). The majority of patients had WHO Functional Class II (42%) or III (54%) at baseline. Patients with systolic blood pressure <95 mm Hg were excluded.
Deteriorated4% for Adempas (n=9/254)
14% for placebo (n=18/125)
Stable
76% for Adempas (n=192/254)
71% for placebo (n=89/125)
WHO FUNCTIONAL CLASS

Adempas -US.com
Stimulating
Soluble Guanylate Cyclase
WARNINGS AND PRECAUTIONSAdempas REMS Program. Females can only receive Adempas through the Adempas REMS Program, a restricted distribution program.
Important requirements of the Adempas REMS program include the following:
• Prescribers must be certifi ed with the program by enrolling and completing training.
• All females, regardless of reproductive potential, must enroll in the Adempas REMS Program prior to initiating Adempas. Male patients are not enrolled in the Adempas REMS Program.
• Female patients of reproductive potential must comply with the pregnancy testing and contraception requirements.
• Pharmacies must be certifi ed with the program and must only dispense to patients who are authorized to receive Adempas.
Further information, including a list of certifi ed pharmacies, is available at www.AdempasREMS.com or 1-855-4ADEMPAS.
Patients walked farther with Adempas at Week 16: results from Week 2 onward
improvement (mean) in 6MWD over placebo at Week 16 (95% CI: 25m-67m; p<0.0001) for CTEPH* (WHO Group 4) patients. 46m
CHEST-1: 261 CTEPH patients were studied. (Adempas n=173, placebo n=88) Baseline characteristics: *Inoperable and recurrent/persistent CTEPH after surgery.
– Mean age: 59 years (range: 18–80)
– Mean 6MWD was 347m
– Concomitant medications: Stable dosages of oral anticoagulants, diuretics, digitalis, calcium channel blockers, and oxygen were allowed, but not nitric oxide donors, endothelin receptor antagonists, prostacyclin analogues, specifi c phosphodiesterase (PDE)-5 inhibitors (such as sildenafi l, tadalafi l, or vardenafi l), and nonspecifi c PDE inhibitors (for example, dipyridamole or theophylline)
Patient population was: 72% inoperable by pulmonary endarterectomy (PEA) (pulmonary vascular resistance [PVR] >300 dyn·sec·cm-5 and mean pulmonary arterial pressure >25 mm Hg measured at least 90 days after the start of full anticoagulation); 28% recurrent or persisting pulmonary hypertension (PH) following PEA (PVR >300 dyn·sec·cm-5 measured at least 180 days following PEA). The majority of patients were WHO Functional Class II (31%) or III (64%) at baseline. Patients with systolic blood pressure <95 mm Hg were excluded.
2xas many CTEPH patients improved WHO Functional Class vs placebo (p=0.0026; Adempas: n=57/173 [33%], placebo: n=13/87 [15%]) at Week 16.
WHO FUNCTIONAL CLASS
Deteriorated5% for Adempas (n=9/173)
7% for placebo(n=6/87)
Stable
62% for Adempas (n=107/173)
78% for placebo (n=68/87)

FOR PAH. FOR CTEPH.
Stimulating
Soluble Guanylate Cyclase
Bayer HealthCare LLC100 Bayer Boulevard, Whippany, NJ 07981 USA©2014 Bayer HealthCare Inc.400-10-0003-14a September 2014
BAYER, the Bayer Cross, and Adempas are registered trademarks of Bayer.
WARNINGS AND PRECAUTIONSHypotension. Adempas reduces blood pressure. Consider the potential for symptomatic hypotension or ischemia in patients with hypovolemia, severe left ventricular outfl ow obstruction, resting hypotension, autonomic dysfunction, or concomitant treatment with antihypertensives or strong CYP and P-gp/BCRP inhibitors. Consider a dose reduction if patient develops signs or symptoms of hypotension.Bleeding. In the placebo-controlled clinical trials, serious bleeding occurred in 2.4% of patients taking Adempas compared to 0% of placebo patients. Serious hemoptysis occurred in 5 (1%) patients taking Adempas compared to 0 placebo patients, including one event with fatal outcome. Serious hemorrhagic events also included 2 patients with vaginal hemorrhage, 2 with catheter site hemorrhage, and 1 each with subdural hematoma, hematemesis, and intra-abdominal hemorrhage.Pulmonary Veno-Occlusive Disease. Pulmonary vasodilators may signifi cantly worsen the cardiovascular status of patients with pulmonary veno-occlusive disease (PVOD). Therefore, administration of Adempas to such patients is not recommended. Should signs of pulmonary edema occur, the possibility of associated PVOD should be considered and if confi rmed, discontinue treatment with Adempas.
93%PAH
More than 90% of Adempas patients survived at 2 years** Data from CHEST-2 and PATENT-2 open-label extension studies. Without a control group, these data must be interpreted cautiously.
At 1 year, probability of survival was 97% in both open-label extension studies.
MOST COMMON ADVERSE REACTIONS • The most common adverse reactions occurring
more frequently (≥3%) on Adempas than placebo were headache (27% vs 18%), dyspepsia/gastritis (21% vs. 8%), dizziness (20% vs 13%), nausea (14% vs 11%), diarrhea (12% vs 8%), hypotension (10% vs 4%), vomiting (10% vs 7%), anemia (7% vs 2%), gastroesophageal refl ux disease (5% vs 2%), and constipation (5% vs 1%).
• Other events that were seen more frequently in Adempas compared to placebo and potentially related to treatment were: palpitations, nasal congestion, epistaxis, dysphagia, abdominal distension and peripheral edema.
For important risk and use information, please see the Brief Summary of the full Prescribing Information, including Boxed Warning, on the next page.
94%CTEPH
PROBABILITY OF SURVIVAL AT 2 YEARS
PROBABILITY OF SURVIVAL AT 2 YEARS

ADEMPAS (riociguat) tablets, for oral useInitial U.S. Approval: 2013
BRIEF SUMMARY of PRESCRIBING INFORMATIONFor additional information, please see the full Prescribing Information at
www.adempas-us.com.
WARNING: EMBRYO-FETAL TOXICITYSee full prescribing information for complete boxed warning
• Do not administer Adempas to a pregnant female because it may cause fetal harm. (4.1, 5.1, 8.1)
• Females of reproductive potential: Exclude pregnancy before start of treatment, monthly during treatment, and 1 month after treatment discontinuation. Prevent pregnancy during treatment and for one month after treatment discontinuation by use of acceptable methods of contraception. (2.3, 5.1, 5.2, 8.6)
• For females, Adempas is available only through a restricted program called the Adempas REMS Program. (5.1, 5.2).
1 INDICATIONS AND USAGE1.1 Chronic-Thromboembolic Pulmonary Hypertension Adempas is indicated for the treatment of adults with persistent/recurrent chronic thromboembolic pulmonary hypertension (CTEPH), (WHO Group 4) after surgical treatment, or inoperable CTEPH, to improve exercise capacity and WHO functional class [see Clinical Studies (14.1)].1.2 Pulmonary Arterial Hypertension Adempas is indicated for the treatment of adults with pulmonary arterial hypertension (PAH), (WHO Group 1), to improve exercise capacity, WHO functional class and to delay clinical worsening. Efficacy was shown in patients on Adempas monotherapy or in combination with endothelin receptor antagonists or prostanoids. Studies establishing effectiveness included predominately patients with WHO functional class II–III and etiologies of idiopathic or heritable PAH (61%) or PAH associated with connective tissue diseases (25%) [see Clinical Studies (14.2)]. 4 CONTRAINDICATIONS4.1 PregnancyAdempas may cause fetal harm when administered to a pregnant woman. Adempas is contraindicated in females who are pregnant. Adempas was consistently shown to have teratogenic effects when administered to animals. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus [see Use in Specific Populations (8.1)].4.2 Nitrates and Nitric Oxide DonorsCo-administration of Adempas with nitrates or nitric oxide donors (such as amyl nitrite) in any form is contraindicated [see Drug Interactions (7.1) and Clinical Pharmacology (12.2)].4.3 Phosphodiesterase InhibitorsConcomitant administration of Adempas with specific PDE-5 inhibitors (such as sildenafil, tadalafil, or vardenafil) or nonspecific PDE inhibitors (such as dipyridamole or theophylline) is contraindicated [see Drug Interactions (7.1) and Clinical Pharmacology (12.2)].5 WARNINGS AND PRECAUTIONS5.1 Embryo-Fetal ToxicityAdempas may cause fetal harm when administered during pregnancy and is contraindicated for use in women who are pregnant. In females of reproductive potential, exclude pregnancy prior to initiation of therapy, advise use of acceptable contraception and obtain monthly pregnancy tests. For females, Adempas is only available through a restricted program under the Adempas REMS Program [see Dosage and Administration (2.3), Warnings and Precautions (5.2) and Use in Specific Populations (8.1, 8.6)].5.2 Adempas REMS ProgramFemales can only receive Adempas through the Adempas Risk Evaluation and Mitigation Strategy (REMS) Program, a restricted distribution program [see Warnings and Precautions (5.1)].Important requirements of the Adempas REMS Program include the following: • Prescribers must be certified with the program by enrolling and completing
training.• All females, regardless of reproductive potential, must enroll in the
Adempas REMS Program prior to initiating Adempas. Male patients are not enrolled in the Adempas REMS Program.
• Female patients of reproductive potential must comply with the pregnancy testing and contraception requirements [see Use in Specific Populations (8.6)].
• Pharmacies must be certified with the program and must only dispense to patients who are authorized to receive Adempas.
Further information, including a list of certified pharmacies, is available at www.AdempasREMS.com or 1-855-4 ADEMPAS.
5.3 HypotensionAdempas reduces blood pressure. Consider the potential for symptomatic hypotension or ischemia in patients with hypovolemia, severe left ventricular
outflow obstruction, resting hypotension, autonomic dysfunction, or concomitant treatment with antihypertensives or strong CYP and P-gp/BCRP inhibitors [see Drug Interactions (7.2) and Clinical Pharmacology (12.3)]. Consider a dose reduction if patient develops signs or symptoms of hypotension.
5.4 BleedingIn the placebo-controlled clinical trials, serious bleeding occurred in 2.4% of patients taking Adempas compared to 0% of placebo patients. Serious hemoptysis occurred in 5 (1%) patients taking Adempas compared to 0 placebo patients, including one event with fatal outcome. Serious hemorrhagic events also included 2 patients with vaginal hemorrhage, 2 with catheter site hemorrhage, and 1 each with subdural hematoma, hematemesis, and intra-abdominal hemorrhage.
5.5 Pulmonary Veno-Occlusive DiseasePulmonary vasodilators may significantly worsen the cardiovascular status of patients with pulmonary veno-occlusive disease (PVOD). Therefore, administration of Adempas to such patients is not recommended. Should signs of pulmonary edema occur, the possibility of associated PVOD should be considered and, if confirmed, discontinue treatment with Adempas.
6 ADVERSE REACTIONSThe following serious adverse reactions are discussed elsewhere in the labeling:• Embryo-Fetal Toxicity [see Warnings and Precautions (5.1)]• Hypotension [see Warnings and Precautions (5.3)]• Bleeding [see Warnings and Precautions (5.4)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.The safety data described below reflect exposure to Adempas in two, randomized, double blind, placebo-controlled trials in patients with inoperable or recurrent/persistent CTEPH (CHEST-1) and treatment naive or pre-treated PAH patients (PATENT-1). The population (Adempas: n = 490; Placebo: n = 214) was between the age of 18 and 80 years [See Clinical Studies (14.1, 14.2)].The safety profile of Adempas in patients with inoperable or recurrent/persistent CTEPH (CHEST-1) and treatment naive or pre-treated PAH (PATENT-1) were similar. Therefore, adverse drug reactions (ADRs) identified from the 12 and 16 week placebo-controlled trials for PAH and CTEPH respectively were pooled, and those occurring more frequently on Adempas than placebo (≥3%) are displayed in Table 1 below. Most adverse reactions in Table 1 can be ascribed to the vasodilatory mechanism of action of Adempas.The overall rates of discontinuation due to an adverse event in the pivotal placebo-controlled trials were 2.9% for Adempas and 5.1% for placebo (pooled data).
Table 1: Adverse Reactions Occurring More Frequently (≥3%) on Adempas than Placebo (Pooled from CHEST-1 and PATENT-1)
Adverse Reactions Adempas % Placebo % (n=490) (n=214)Headache 27 18Dyspepsia and Gastritis 21 8Dizziness 20 13Nausea 14 11Diarrhea 12 8Hypotension 10 4Vomiting 10 7Anemia (including laboratory parameters) 7 2Gastroesophageal reflux disease 5 2Constipation 5 1
Other events that were seen more frequently in Adempas compared to placebo and potentially related to treatment were: palpitations, nasal congestion, epistaxis, dysphagia, abdominal distension and peripheral edema. With longer observation in uncontrolled long-term extension studies the safety profile was similar to that observed in the placebo controlled phase 3 trials.
7 DRUG INTERACTIONS 7.1 Pharmacodynamic Interactions with AdempasNitrates: Co-administration of Adempas with nitrates or nitric oxide donors (such as amyl nitrite) in any form is contraindicated because of hypotension [see Contraindications (4.2) and Clinical Pharmacology (12.2)].PDE Inhibitors: Co-administration of Adempas with specific PDE-5 inhibitors (such as sildenafil, tadalafil, or vardenafil) and nonspecific PDE inhibitors (such as dipyridamole or theophylline), is contraindicated because of hypotension [see Contraindications (4.3) and Clinical Pharmacology (12.2)]. Clinical experience with co-administration of Adempas and

other phosphodiesterase inhibitors (for example, milrinone, cilostazole, roflumilast) is limited.
7.2 Pharmacokinetic Interactions with AdempasSmoking: Plasma concentrations in smokers are reduced by 50-60% compared to nonsmokers. Based on pharmacokinetic modeling, for patients who are smokers, doses higher than 2.5 mg three times a day may be considered in order to match exposure seen in nonsmoking patients. Safety and effectiveness of Adempas doses higher than 2.5 mg three times a day have not been established. A dose reduction should be considered in patients who stop smoking [see Dosage and Administration (2.4) and Clinical Pharmacology (12.3)].Strong CYP and P-gp/BCRP inhibitors: Concomitant use of riociguat with strong cytochrome CYP inhibitors and P-gp/BCRP inhibitors such as azole antimycotics (for example, ketoconazole, itraconazole) or HIV protease inhibitors (such as ritonavir) increase riociguat exposure and may result in hypotension. Consider a starting dose of 0.5 mg 3 times a day when initiating Adempas in patients receiving strong CYP and P-gp/BCRP inhibitors. Monitor for signs and symptoms of hypotension on initiation and on treatment with strong CYP and P-gp/BCRP inhibitors. A dose reduction should be considered in patients who may not tolerate the hypotensive effect of riociguat [see Dosage and Administration (2.5), Warnings and Precautions (5.3) and Clinical Pharmacology (12.3)].Strong CYP3A inducers: Strong inducers of CYP3A (for example, rifampin, phenytoin, carbamazepine, phenobarbital or St. John’s Wort) may significantly reduce riociguat exposure. Data are not available to guide dosing of riociguat when strong CYP3A inducers are co-administered [see Clinical Pharmacology (12.3)].Antacids: Antacids such as aluminum hydroxide/magnesium hydroxide decrease riociguat absorption and should not be taken within 1 hour of taking Adempas [see Clinical Pharmacology (12.3)].
8 USE IN SPECIFIC POPULATIONS8.1 PregnancyPregnancy Category XRisk SummaryAdempas may cause fetal harm when administered to a pregnant woman and is contraindicated during pregnancy. Adempas was teratogenic and embryotoxic in rats at doses with exposures to unbound drug that were approximately 8 times and 2 times, respectively, the human exposure. In rabbits, riociguat led to abortions at 4 times the human exposure and fetal toxicity with exposures approximately 13 times the human exposure. If Adempas is used in pregnancy, or if the patient becomes pregnant while taking this drug, apprise the patient of the potential hazard to the fetus [see Boxed Warning and Contraindications (4.1)]. Animal DataIn rats administered riociguat orally (1, 5, and 25 mg/kg/day) throughout organogenesis, an increased rate of cardiac ventricular-septal defect was observed at the highest dose tested. The highest dose produced evidence of maternal toxicity (reduced body weight). Post-implantation loss was statistically significantly increased from the mid-dose of 5 mg/kg/day. Plasma exposure at the lowest dose in which no adverse effects were observed is approximately 0.4 times that in humans at the maximally recommended human dose (MRHD) of 2.5 mg three times a day based on area under the time-concentration curve (AUC) for unbound drug in rat and humans. Plasma exposure at the highest dose (25 mg/kg/day) is approximately 8 times that in humans at the MRHD while exposure at the mid-dose (5 mg/kg/day) is approximately 2 times that in humans at the MRHD. In rabbits given doses of 0.5, 1.5 and 5 mg/kg/day, an increase in spontaneous abortions was observed starting at the middle dose of 1.5 mg/kg, and an increase in resorptions was observed at 5 mg/kg/day. Plasma exposures at these doses were 4 times and 13 times, respectively, the human exposure at the MRHD.
8.3 Nursing MothersIt is not known if Adempas is present in human milk. Riociguat or its metabolites were present in the milk of rats. Because many drugs are present in human milk and because of the potential for serious adverse reactions in nursing infants from riociguat, discontinue nursing or Adempas.
8.4 Pediatric UseSafety and effectiveness of Adempas in pediatric patients have not been established [see Nonclinical Toxicology (13.2)].
8.5 Geriatric UseOf the total number of subjects in clinical studies of Adempas, 23% were 65 and over, and 6% were 75 and over [see Clinical Studies (14)]. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.Elderly patients showed a higher exposure to Adempas [see Clinical Pharmacology (12.3)].
8.6 Females and Males of Reproductive PotentialPregnancy Testing: Female patients of reproductive potential must have a negative pregnancy test prior to starting treatment with Adempas, monthly during treatment, and one month after discontinuation of treatment with
Adempas. Advise patients to contact their healthcare provider if they become pregnant or suspect they may be pregnant. Counsel patients on the risk to the fetus [see Boxed Warning, Dosage and Administration (2.3) and Use in Specific Populations (8.1].Contraception: Female patients of reproductive potential must use acceptable methods of contraception during treatment with Adempas and for 1 month after treatment with Adempas. Patients may choose one highly effective form of contraception (intrauterine devices [IUD], contraceptive implants or tubal sterilization) or a combination of methods (hormone method with a barrier method or two barrier methods). If a partner’s vasectomy is the chosen method of contraception, a hormone or barrier method must be used along with this method. Counsel patients on pregnancy planning and prevention, including emergency contraception, or designate counseling by another healthcare provider trained in contraceptive counseling [See Boxed Warning].
8.7 Renal ImpairmentSafety and efficacy have not been demonstrated in patients with creatinine clearance <15 mL/min or on dialysis [see Clinical Pharmacology (12.3)].
8.8 Hepatic ImpairmentSafety and efficacy have not been demonstrated in patients with severe hepatic impairment (Child Pugh C) [see Clinical Pharmacology (12.3)].
10 OVERDOSAGEIn cases of overdose, blood pressure should be closely monitored and supported as appropriate. Based on extensive plasma protein binding, riociguat is not expected to be dialyzable.
17 PATIENT COUNSELING INFORMATIONSee FDA-approved patient labeling (Medication Guide).Embryo-Fetal ToxicityInstruct patients on the risk of fetal harm when Adempas is used during pregnancy [see Warnings and Precautions (5.1) and Use in Specific Populations (8.1)]. Instruct females of reproductive potential to use effective contraception and to contact her physician immediately if they suspect they may be pregnant. Female patients must enroll in the Adempas REMS Program. Adempas REMS ProgramFor female patients, Adempas is available only through a restricted program called the Adempas REMS Program [see Warnings and Precautions (5.2)]. Male patients are not enrolled in the Adempas REMS Program. Inform female patients (and their guardians, if applicable) of the following important requirements:• All female patients must sign an enrollment form.• Advise female patients of reproductive potential that she must comply
with the pregnancy testing and contraception requirements [see Use in Specific Populations (8.6)].
• Educate and counsel females of reproductive potential on the use of emergency contraception in the event of unprotected sex or contraceptive failure.
• Advise pre-pubertal females to report any changes in their reproductive status immediately to her prescriber.
Review the Medication Guide and REMS educational materials with female patients.Other Risks Associated with Adempas • Inform patients of the contraindication of Adempas with nitrates or nitric
oxide donors or PDE-5 inhibitors. • Advise patients about the potential risks/signs of hemoptysis and to report
any potential signs of hemoptysis to their physicians.• Instruct patients on the dosing, titration, and maintenance of Adempas.• Advise patients regarding activities that may impact the pharmacology of
Adempas (strong multi pathway CYP inhibitors and P-gp/BCRP inhibitors and smoking). Patients should report all current medications and new medications to their physician.
• Advise patients that antacids should not be taken within 1 hour of taking Adempas.
• Inform patients that Adempas can cause dizziness, which can affect the ability to drive and use machines [see Adverse Reactions (6.1)]. They should be aware of how they react to Adempas, before driving or operating machinery and if needed, consult their physician.
Manufactured for:
Bayer HealthCare Pharmaceuticals Inc. Whippany, NJ 07981
Manufactured in Germany
Issued May 2014
©2013 Bayer HealthCare Pharmaceuticals Inc.
6710501BS

Debuting in Volume 13, No 3 in the Fall of 2014 a
new section will appear in Advances in Pulmonary Hypertension dedicated to inspiring new thoughts
and providing instruction through case reports and
reviews. This section will focus on submissions
from trainees and junior faculty interested in
pulmonary hypertension (PH). It will emulate
Grand Rounds and will highlight clinical cases
that describe an interesting or thought-provoking
entity, mechanism, presentation, or outcome in
patients with PH. The cases will include reviews of
topics that provide insights and education for
clinicians. Interesting cases with associated teach-
ing points and discussion that the case highlights
are encouraged. Mentoring comments from a
member of the editorial board will be included
with each of the cases.
The Advances editorial board encourages program
directors and attendings to promote this opportu-
nity to trainees and junior faculty as an opportu-
nity to share their observations and to obtain
valuable comments from leaders in the field. It’s a
great way to become involved with other clinicians
and researchers.
Potential authors should submit a brief summary
for consideration by the editorial board. Selected
authors will be notified to prepare the complete
case.
Author InstructionsEach case study should be submitted double-spaced in Word. Digital files of illustrations are acceptable as long as they reproduce well.
Abstract: 150 words in narrative format
Text: Maximum 1000 words
Tables and illustrations: Total of 3; color allowed
References: Maximum of 8. Do not include any reference management software.
Format:Introduction and case presentationHistoryClinical featuresClinical evaluationLaboratory and study results (to include imaging if possible, waveforms, etc)Management and therapeuticsOutcomesDiscussion: Review of the literatureRecommendations and commentsMentoring comments from an editorial board member
Case reports that have been presented at meetings are acceptable as long as the meeting information is disclosed on the title page.
IRB approval is not required; nevertheless, authors must preserve patient privacy when writing up the case. On acceptance, written patient permission will be requested as a condition of publication.
Cases will be chosen for publication by members of the Advances in Pulmonary Hypertension editorial board.
Submit a brief summary for consideration to: [email protected]
Section editor: Deborah Jo Levine, MDAssociate Professor of Medicine Pulmonary and Critical Care MedicineDirector of Pulmonary Hypertension CenterDirector of Inpatient and Outpatient Lung TransplantationUniversity of Texas Health Science Center San Antonio
San Antonio, Texas
Introducing Pulmonary Hypertension Grand Rounds (PHGR)

Important Safety InformationCONTRAINDICATIONS• Nitrates: ADCIRCA should not be used in patients taking
medicines that contain nitrates, as the combination could cause a sudden, unsafe drop in blood pressure
• Hypersensitivity Reactions: Patients with a known serious hypersensitivity to tadalafil should not take ADCIRCA
WARNINGS AND PRECAUTIONS• Cardiovascular: Patients who experience anginal chest pain
after taking ADCIRCA should seek immediate medical attention
• Cardiovascular: Phosphodiesterase 5 inhibitors (PDE-5is), including tadalafi l, have mild systemic vasodilatory properties that may result in transient decreases in blood pressure. Before prescribing ADCIRCA, physicians should carefully consider whether their patients with underlying cardiovascular disease could be adversely aff ected by such actions. Pulmonary vasodilators may signifi cantly worsen the cardiovascular status of patients with pulmonary veno-occlusive disease (PVOD) and administration of ADCIRCA to these patients is not recommended
• Cardiovascular: The use of ADCIRCA with alpha blockers, blood pressure medications, or alcohol may lower blood pressure signifi cantly and may lead to symptomatic hypotension (light-headedness or fainting)
• Potential Drug Interactions: Tadalafi l is metabolized predominately by CYP3A in the liver. Use of ADCIRCA withpotent CYP3A inhibitors, such as ketoconazole and itraconazole, should be avoided. For patients on ADCIRCA therapy that require treatment with ritonavir, ADCIRCA should be discontinued atleast 24 hours prior to starting ritonavir. For patients on ritonavir therapy that require treatment with ADCIRCA, start ADCIRCAat 20 mg once a day. Use of ADCIRCA with potent inducers of CYP3A, such as rifampin, should be avoided
• Special Populations: The use of ADCIRCA is not recommended for patients with severe renal or hepatic impairment. Please see Full Prescribing Information for dosing recommendations for patients with mild to moderate renal or hepatic impairment
• Potential Drug Interactions: ADCIRCA contains the same ingredient (tadalafi l) as Cialis®, which is used to treat erectile dysfunction (ED) and the signs and symptoms of benign prostatic hyperplasia (BPH). The safety and effi cacy of combinations of ADCIRCA with Cialis or other PDE-5is have not been studied. Therefore, the use of such combinations is not recommended
• Vision/Hearing: Patients who experience a sudden loss of vision in one or both eyes, which could be a sign of non-arteritic anterior ischemic optic neuropathy (NAION), or sudden decrease or loss of hearing after taking ADCIRCA should seek immediate medical attention.

A diagnosis of pulmonary arterial hypertension (PAH)
CAN STOP A PATIENT IN THEIR TRACKSTake the fi rst step forward to a solid foundation with ADCIRCA® (tadalafi l), a fi rst-line therapy for PAH.
• Prolonged Erection: In rare instances, men taking PDE-5is (including tadalafi l) for ED reported an erection lasting more than four hours. Male patients who experience a prolonged erection should seek immediate medical attention
ADVERSE REACTIONS• Adverse Reactions: The most common adverse event with
ADCIRCA is headache (42% ADCIRCA vs 15% placebo). Other common adverse events (reported by ≥9% of patients on ADCIRCA and more frequent than placebo by 2%) include myalgia (14% vs 4%), nasopharyngitis (13% vs 7%), fl ushing (13% vs 2%), respiratory tract infection (13% vs 6%), extremity pain (11% vs 2%), nausea (11% vs 6%), back pain (10% vs 6%), dyspepsia (10% vs 2%), and nasal congestion (9% vs 1%)
References: 1. ADCIRCA [package insert]. Indianapolis, IN: Eli Lilly and Company; 2013. 2. Galiè N, Brundage BH, Ghofrani HA, et al; on behalf of the Pulmonary Arterial Hypertension and Response to Tadalafi l (PHIRST) Study Group. Tadalafi l therapy for pulmonary arterial hypertension. Circulation. 2009;119(22):2894-2903. 3. SPS and IMS XPO data ending October 2013; 2H Deciles.
www.adcirca.com 1-877-UNITHER
Every Step Matters
*Includes patients on monotherapy and background bosentan therapy.1,2
† Clinical worsening is defi ned as death, lung transplantation, atrial septostomy, hospitalization because of worsening PAH, initiation of new PAH therapy (prostacyclin or analog, endothelin receptor antagonist, PDE-5 inhibitor), or worsening WHO functional class.1
‡ Patients must meet certain eligibility criteria to qualify for assistance. Patients receiving reimbursement under Medicare, Medicaid, VA, DoD (TRICARE), Indian Health Services, or similar federal or state programs, may not be eligible for some assistance. Some portion of this patient assistance may be administered by Caring Voice Coalition (CVC), an independent national nonprofi t organization.
ADCIRCA and Cialis are registered trademarks of Eli Lilly and Company, 2014.
© 2014 Lung Biotechnology Inc. All rights reserved. Printed in the USA. US/ADC/JAN14/134
ISI.HCP.KCGLUNGLLC-4-70.v1
ADCIRCA® (tadalafi l) tablets is a phosphodiesterase 5 inhibitor (PDE-5i) indicated for the treatment of pulmonary arterial hypertension (PAH) (WHO Group 1) to improve exercise ability. Studies establishing eff ectiveness included predominately patients with NYHA Functional Class IIIII symptoms and etiologies of idiopathic or heritable PAH (61%) or PAH associated with connective tissue diseases (23%).
For patients taking ADCIRCA in comparison to patients on placebo at 16 weeks, the average increase from baseline in 6-minute walk distance was 33 meters (108 feet) for all patients* and 44 meters (144 feet) for those on ADCIRCA monotherapy1,2
Clinically proven to reduce risk of clinical worsening vs placebo at 16 weeks1,2†
The recommended dose of ADCIRCA is 40 mg (two 20-mg tablets) taken once-daily, with or without food. Dividing the dose is not recommended
The only once-daily PDE-5 inhibitor for PAH1
The most common (reported by ≥ 13% of patients) treatment-emergent side eff ects of ADCIRCA (headache, myalgia, nasopharyngitis, fl ushing, and respiratory infection) were transient and mild to moderate in intensity1
$20 co-pay for eligible patients on commercial/private insurance plans‡
Help your patients move forward with ADCIRCA—one step at a time.
Please see Brief Summary of Full Prescribing Information on following page. Please see Full Prescribing Information and Patient Information available at www.adcirca.com, or call 1-800-545-5979.

ADCIRCA® (tadalafil) tabletsBRIEF SUMMARYThe following is a brief summary of the Full Prescribing Information on ADCIRCA (tadalafil). Please review the Full Prescribing Information prior to prescribing ADCIRCA.INDICATIONS AND USAGEPulmonary Arterial Hypertension: ADCIRCA is indicated for the treatment of pulmonary arterial hypertension (PAH) (WHO Group 1) to improve exercise ability. Studies establishing effectiveness included predominately patients with NYHA Functional Class II–III symptoms and etiologies of idiopathic or heritable PAH (61%) or PAH associated with connective tissue diseases (23%).CONTRAINDICATIONSConcomitant Organic Nitrates: Do not use ADCIRCA in patients who are using any form of organic nitrate, either regularly or intermittently. ADCIRCA potentiates the hypotensive effect of nitrates. This potentiation is thought to result from the combined effects of nitrates and ADCIRCA on the nitric oxide/cGMP pathway. Hypersensitivity Reactions: ADCIRCA is contraindicated in patients with a known serious hypersensitivity to tadalafil (ADCIRCA or CIALIS). Hypersensitivity reactions have been reported, including Stevens-Johnson syndrome and exfoliative dermatitis.WARNINGS AND PRECAUTIONSCardiovascular Effects: Discuss with patients the appropriate action to take in the event that they experience anginal chest pain requiring nitroglycerin following intake of ADCIRCA. At least 48 hours should elapse after the last dose of ADCIRCA before taking nitrates. If a patient has taken ADCIRCA within 48 hours, administer nitrates under close medical supervision with appropriate hemodynamic monitoring. Patients who experience anginal chest pain after taking ADCIRCA should seek immediate medical attention. PDE5 inhibitors, including tadalafil, have mild systemic vasodilatory properties that may result in transient decreases in blood pressure. Prior to prescribing ADCIRCA, carefully consider whether patients with underlying cardiovascular disease could be affected adversely by such vasodilatory effects. Patients with severely impaired autonomic control of blood pressure or with left ventricular outflow obstruction, (e.g., aortic stenosis and idiopathic hypertrophic subaortic stenosis) may be particularly sensitive to the actions of vasodilators, including PDE5 inhibitors. Pulmonary vasodilators may significantly worsen the cardiovascular status of patients with pulmonary veno-occlusive disease (PVOD). Since there are no clinical data on administration of ADCIRCA to patients with veno-occlusive disease, administration of ADCIRCA to such patients is not recommended. Should signs of pulmonary edema occur when ADCIRCA is administered, the possibility of associated PVOD should be considered. There is a lack of data on safety and efficacy in the following groups who were specifically excluded from the PAH clinical trials:
disease
cardiomyopathy
dysfunction
uncontrolled hypertension
Use with Alpha Blockers and Antihypertensives — PDE5 inhibitors, including ADCIRCA, and alpha–adrenergic blocking agents are vasodilators with blood pressure-lowering effects. When vasodilators are used in combination, an additive effect on blood pressure may be anticipated. In some patients, concomitant use of these two drug classes can lower blood pressure significantly, which may lead to symptomatic hypotension (e.g., fainting). Safety of combined use of PDE5 inhibitors and alpha blockers may be affected by other variables, including intravascular volume depletion and use of other antihypertensive drugs. Use with Alcohol — Both alcohol and tadalafil are mild vasodilators. When mild vasodilators are taken in combination, blood pressure-lowering effects are increased. Use with Potent CYP3A Inhibitors or Inducers:Co-administration of ADCIRCA in Patients on Ritonavir — In patients receiving ritonavir for at least one week, start ADCIRCA
individual tolerability. Co-administration of Ritonavir in Patients on ADCIRCA — Avoid use of ADCIRCA during the initiation of ritonavir. Stop ADCIRCA at least 24 hours prior to starting ritonavir. After at least one
week following the initiation of ritonavir, resume ADCIRCA at
individual tolerability. Other Potent Inhibitors of CYP3A — Tadalafil is metabolized predominantly by CYP3A in the liver. In patients taking potent inhibitors of CYP3A such as ketoconazole and itraconazole, avoid use of ADCIRCA. Potent Inducers of CYP3A — For patients chronically taking potent inducers of CYP3A, such as rifampin, avoid use of ADCIRCA. Use in Renal Impairment: In patients with mild or moderate renal impairment
In patients with severe renal impairment — Avoid use of ADCIRCA because of increased tadalafil exposure (AUC), limited clinical experience, and the lack of ability to influence clearance by dialysis. Use in Hepatic Impairment: In patients with mild to moderate hepatic cirrhosis (Child-Pugh Class A and B) — Because of limited clinical experience in patients with mild to moderate hepatic
In patients with severe hepatic cirrhosis (Child-Pugh Class C) — Patients with severe hepatic cirrhosis have not been studied. Avoid use of ADCIRCA. Visual Loss: Physicians should advise patients to seek immediate medical attention in the event of a sudden loss of vision in one or both eyes. Such an event may be a sign of non–arteritic anterior ischemic optic neuropathy (NAION), a cause of decreased vision, including permanent loss of vision that has been reported postmarketing in temporal association with the use of all PDE5 inhibitors. An observational study evaluated whether recent episodic use of PDE5 inhibitors, as a class, typical of erectile dysfunction treatment, was associated with acute onset of NAION. The results suggest an approximate 2-fold increase in the risk of NAION within 1 to 4 days of PDE5 inhibitor use. It is not possible to determine whether these events are related directly to the use of PDE5 inhibitors or other factors. Physicians should also discuss with patients the increased risk of NAION in individuals who have already experienced NAION in one eye, including whether such individuals could be adversely affected by use of vasodilators such as PDE5 inhibitors. Patients with known hereditary degenerative retinal disorders, including retinitis pigmentosa, were not included in the clinical trials, and use in these patients is not recommended. Hearing Impairment: Physicians should advise patients to seek immediate medical attention in the event of sudden decrease or loss of hearing. These events, which may be accompanied by tinnitus and dizziness, have been reported in temporal association to the intake of PDE5 inhibitors, including ADCIRCA. It is not possible to determine whether these events are related directly to the use of PDE5 inhibitors or to other factors. Combination with Other PDE5 Inhibitors: Tadalafil is also marketed as CIALIS. The safety and efficacy of taking ADCIRCA together with CIALIS or other PDE5 inhibitors have not been studied. Inform patients taking ADCIRCA not to take CIALIS or other PDE5 inhibitors.Prolonged Erection: There have been rare reports of prolonged erections greater than 4 hours and priapism (painful erections greater than 6 hours in duration) for this class of compounds. Priapism, if not treated promptly, can result in irreversible damage to the erectile tissue. Patients who have an erection lasting greater than 4 hours, whether painful or not, should seek emergency medical attention. ADCIRCA should be used with caution in patients who have conditions that might predispose them to priapism (such as sickle cell anemia, multiple myeloma, or leukemia), or in patients with anatomical deformation of the penis (such as angulation, cavernosal fibrosis, or Peyronie’s disease). Effects on Bleeding: PDE5 is found in platelets. When
not prolong bleeding time, relative to aspirin alone. ADCIRCA has not been administered to patients with bleeding disorders or significant active peptic ulceration. Although ADCIRCA has not been shown to increase bleeding times in healthy subjects, use in patients with bleeding disorders or significant active peptic ulceration should be based upon a careful risk-benefit assessment.ADVERSE REACTIONSThe following serious adverse reactions are discussed elsewhere in the labeling:
Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. Tadalafil was
worldwide. In trials of ADCIRCA, a total of 311 and 251
days, respectively. The overall rates of discontinuation because of an adverse event (AE) in the placebo-controlled trial were
discontinuation because of AEs, other than those related to
was 4% compared to 5% in placebo-treated patients. In the placebo-controlled study, the most common AEs were generally transient and mild to moderate in intensity. Table 1presents treatment-emergent adverse events reported by ≥
frequently than with placebo.TABLE 1: Treatment-Emergent Adverse Events Reported by ≥9% of Patients in ADCIRCA and More Frequent than Placebo by 2%
EVENT Placebo (%) ADCIRCA ADCIRCA (N=82) 20 mg (%) 40 mg (%) (N=82) (N=79)Headache 15 32 42
Nasopharyngitis 7 2 13Flushing 2 6 13Respiratory Tract Infection (Upper and Lower) 6 7 13Pain in Extremity 2 5 11
Nasal Congestion (Including sinus
Postmarketing Experience: The following adverse reactions have been identified during post-approval use of tadalafil. These events have been chosen for inclusion either because of their seriousness, reporting frequency, lack of clear alternative causation, or a combination of these factors. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to estimate reliably their frequency or establish a causal relationship to drug exposure. The list does not include adverse events that are reported from clinical trials and that are listed elsewhere in this section. Cardiovascular and cerebrovascular — Serious cardiovascular events, including myocardial infarction, sudden cardiac death, stroke, chest pain, palpitations, and tachycardia, have been reported postmarketing in temporal association with the use of tadalafil. Most, but not all, of these patients had preexisting cardiovascular risk factors. Many of these events were reported to occur during or shortly after sexual activity, and a few were reported to occur shortly after the use of tadalafil without sexual activity. Others were reported to have occurred hours to days after the use of tadalafil and sexual activity. It is not possible to determine whether these events are related directly to tadalafil, to sexual activity, to the patient’s underlying cardiovascular disease, to a combination of these factors, or to other factors.Body as a whole — Hypersensitivity reactions including urticaria, Stevens–Johnson syndrome, and exfoliative dermatitis. Nervous — Migraine, seizure and seizure recurrence, and transient global amnesia. Ophthalmologic — Visual field defect, retinal vein occlusion, and retinal artery occlusion. Non–arteritic anterior ischemic optic neuropathy (NAION), a cause of decreased vision including permanent loss of vision, has been reported rarely postmarketing in temporal association with the use of PDE5 inhibitors, including tadalafil. Most, but not all, of these patients had underlying anatomic or vascular risk factors for development of NAION, including but not necessarily limited to:
hypertension, coronary artery disease, hyperlipidemia, and smoking. It is not possible to determine whether these events are related directly to the use of PDE5 inhibitors, to the patient’s underlying vascular risk factors or anatomical defects, to a

combination of these factors, or to other factors. Otologic — Cases of sudden decrease or loss of hearing have been reported postmarketing in temporal association with the use of PDE5 inhibitors, including tadalafil. In some of the cases, medical conditions and other factors were reported that may have also played a role in the otologic adverse events. In many cases, medical follow-up information was limited. It is not possible to determine whether these reported events are related directly to the use of tadalafil, to the patient’s underlying risk factors for hearing loss, a combination of these factors, or to other factors. Urogenital — Priapism.DRUG INTERACTIONSPotential for Pharmacodynamic Interactions with are using any form of organic nitrate. In clinical pharmacology studies ADCIRCA potentiated the hypotensive effect of nitrates. In a patient who has taken ADCIRCA, where nitrate administration is deemed medically necessary in a life–threatening situation, at least 48 hours should elapse after the last dose of ADCIRCA before nitrate administration is considered. In such circumstances, nitrates should still only be administered under close medical supervision with appropriate hemodynamic monitoring. Alpha-Blockers — PDE5 inhibitors, including ADCIRCA, and alpha–adrenergic blocking agents are both vasodilators with bloodpressure-lowering effects. When vasodilators are used in combination, an additive effect on blood pressure may be anticipated. Clinical pharmacology studies have been conducted with coadministration of tadalafil with doxazosin, alfuzosin or tamsulosin. Antihypertensives — PDE5 inhibitors, including ADCIRCA, are mild systemic vasodilators. Clinical pharmacology studies were conducted to assess the effect of tadalafil on the potentiation of the blood–pressure–lowering effects of selected antihypertensive medications (amlodipine, angiotensin II receptor blockers, bendroflumethiazide, enalapril, and metoprolol). Small reductions in blood pressure occurred following coadministration of tadalafil with these agents compared with placebo. Alcohol — Both alcohol and tadalafil, a PDE5 inhibitor, act as mild vasodilators. When mild vasodilators are taken in combination, blood pressure–lowering effects of each individual compound may be increased. Substantial consumption of alcohol (e.g., 5 units or greater) in combination with ADCIRCA can increase the potential for orthostatic signs and symptoms, including increase in heart rate, decrease in standing blood
did not affect alcohol plasma concentrations and alcohol did not affect tadalafil plasma concentrations. Potential for Other Drugs to Affect ADCIRCA: Ritonavir — Ritonavir initially inhibits and later induces CYP3A, the enzyme involved in the metabolism of tadalafil. At steady state of ritonavir (about 1 week), the exposure to tadalafil is similar as in the absence of ritonavir.Other Potent Inhibitors of CYP3A — Tadalafil is metabolized predominantly by CYP3A in the liver. In patients taking potent inhibitors of CYP3A such as ketoconazole, and itraconazole, avoid use of ADCIRCA. Potent Inducers of CYP3A — For patients chronically taking potent inducers of CYP3A, such as rifampin, avoid use of ADCIRCA. Potential for ADCIRCA to Affect Other Drugs:
— Tadalafil is not expected to cause clinically significant inhibition or induction of the clearance
theophylline, warfarin, midazolam, lovastatin, bosentan).
potentiate the increase in bleeding time caused by aspirin. P-lycoprotein (e.g., digoxin) — Coadministration of tadalafil
pharmacokinetics in healthy subjects.USE IN SPECIFIC POPULATIONSPregnancy: Pregnancy Category B — Animal reproduction studies in rats and mice revealed no evidence of fetal harm. There are, however, no adequate and well-controlled studies of tadalafil in pregnant women. Because animal reproduction studies are not always predictive of human response, tadalafil should be used during pregnancy only if clearly needed.Non–teratogenic effects — Animal reproduction studies showed no evidence of teratogenicity, embryotoxicity, or fetotoxicity when tadalafil was given to pregnant rats or mice at unbound tadalafil exposures up to 7 times the maximum
organogenesis. In one of two perinatal/postnatal developmental studies in rats, postnatal pup survival decreased following maternal exposure to unbound tadalafil concentrations greater than 5 times the MRHD based on AUC. Signs of maternal toxicity occurred at doses greater than 8 times the MRHD based on AUC. Surviving offspring had normal development and reproductive performance. Nursing Mothers: It is not known whether tadalafil is excreted into human milk. While tadalafil or some metabolite of tadalafil
was excreted into rat milk, drug levels in animal breast milk may not accurately predict levels of drug in human breast milk. Because many drugs are excreted in human milk, caution should be exercised when ADCIRCA is administered to a nursing woman. Pediatric Use: Safety and effectiveness of ADCIRCA in pediatric patients have not been established.Geriatric Use: Of the total number of subjects in the clinical study of tadalafil for pulmonary arterial hypertension, 28 percent were 65 and over, while 8 percent were 75 and over. No overall differences in safety were observed between subjects over 65 years of age compared to younger subjects or those over 75 years of age. No dose adjustment is warranted based on age alone; however, a greater sensitivity to medications in some older individuals should be considered. Renal Impairment: For patients with mild or moderate renal
with severe renal impairment, avoid use of ADCIRCA because of increased tadalafil exposure (AUC), limited clinical experience, and the lack of ability to influence clearance by dialysis. Hepatic Impairment: Because of limited clinical experience in patients with mild to moderate hepatic cirrhosis (Child-Pugh Class
Patients with severe hepatic cirrhosis (Child-Pugh Class C) have not been studied, thus avoid use of ADCIRCA in such patients.OVERDOSAGE
given to male patients with erectile dysfunction. Adverse reactions were similar to those seen at lower doses. Doses
pulmonary arterial hypertension. In cases of overdose, standard supportive measures should be adopted as needed. Hemodialysis contributes negligibly to tadalafil elimination.Marketed by: Lung Biotechnology Inc., a wholly-owned subsidiary of United Therapeutics CorporationRx only www.adcirca.com
ADCIRCA (package insert). Indianapolis, IN: Eli Lilly and
BS.HCP.KCGLUNGLLC-4-72.v2
Clearing the Fog: PH-Associated Diseases
If your papatients are juggling multiple conditions associated with pullmonary hypertension, you know that managing their carre can be overwhelming for them and their families.
Now therre’s some clarity: In PHA’s new video series, your pap tients ccana hear stories from fellow PH patients living with aassociatedd d iseases and the healthcare professionals whotreeat them.
Learnn more at:www.PHAssociation.org/PHPlus
Scleleroderma and d PHPH is not my identittyy ... If yourr sickneessss
becomes your idedentn ity, then you don’t have a shot. Yoouu h have to susus rround yourself witth people
who dododo n ot make you feel sick.

PH GRAND ROUNDS
Pulmonary Artery Filling Defects: Are They All the Same?
Section EditorDeborah J. Levine, MD
Nadine Al-Naamani, MDTufts Medical CenterBoston, MARichard N. Channick, MDMassachusetts General HospitalBoston, MAIoana R. Preston, MDTufts Medical CenterBoston, MA
Section editor’s note: The diagnostic evaluation of pulmonary hypertension (PH) is anextensive, yet specific, process. Each individual study is significant, but it is truly theinsightful analysis of the combination of studies that assists us most in making thecorrect diagnosis. In this issue’s PH Grand Rounds, we congratulate Dr Al-Naamaniand her colleagues for reminding us to consider a more in-depth examination of thedata prior to making what seems to be an obvious diagnosis. This case not onlyimparts valuable information on this particular diagnosis, it also demonstrates howthis type of thought process is vital to both the diagnosis and therapy for ourpatients.
Presentation:A 62-year-old man with a known historyof Eisenmenger’s syndrome and pul-monary arterial hypertension (PAH)secondary to congenital heart disease(CHD), status post atrial septal defect(ASD) closure, and paroxysmal atrialfibrillation on warfarin presented to alocal hospital with 2 weeks of worseningdyspnea on exertion to a New YorkHeart Association functional class(NYHA FC) 3 and intermittent palpita-tions. His symptoms had beenprogressive and were occasionally asso-
ciated with lightheadedness, but nosyncope. His past medical history wasremarkable for an ASD closure at theage of 40, and the diagnosis of PAHwith NYHA FC 2 at the age of 57,when it was also determined that theASD closure had opened. During hisevaluation for PAH, he had undergone achest x-ray, a ventilation/perfusion(V/Q) scan (Figure 1A), and a rightheart catheterization (Table 1). He wastreated with sildenafil and latermacitentan was added (via a clinicaltrial), but he had stopped both drugs
approximately 6 months prior due tofinancial reasons and side effects. At thetime of current presentation, the patientwas treated with warfarin and sotalol.He was found to be hypoxic and in atrialfibrillation, with heart rate ranging from110 to 120 beats per minute with astable blood pressure. He underwent aCT angiogram of the chest (CTPA),which was concerning for bilateralchronic pulmonary emboli with signifi-cantly enlarged pulmonary arteries. Hewas transferred to our medical center forfurther workup and evaluation.
Key Words—atrial septal defect, congenital heart disease, dyspnea, pulmonary arterial hypertension, pul-monary artery aneurysmCorrespondence: [email protected]
Figure 1: Lung perfusion scans at initial presentation for evaluation of PAH (A) and at current presentation (B)
122 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

Assessment:His examination was remarkable fortachycardia with an irregular heartrhythm, a parasternal heave, and aholosystolic murmur at the left para-sternal border. He did not have anyevidence of jugular vein distension orlower extremity edema, and his exami-nation was otherwise unremarkable. Hisblood work was significant for an inter-national normalized ratio (INR) of2.66, a brain natriuretic peptide (BNP)of 79 pg/mL, and a troponin I of�0.01 ng/mL. He had a lowerextremity venous Doppler which
showed no evidence of lower extremityvenous thrombosis. His ECG showedatrial fibrillation at a rate of 112 beatsper minute, right axis deviation with aright bundle branch block, and a leftposterior fascicular block. An echocar-diogram showed increased leftventricular (LV) wall thickness withmildly reduced LV systolic function(ejection fraction 40%), flattenedseptum consistent with right ventricular(RV) pressure or volume overload,bi-atrial dilatation with no evidence ofintra-atrial shunt, and a severely dilatedRV with severely reduced RV systolic
function. Right heart catheterizationwas performed (Table 1). CTPAshowed severe dilatation of the pul-monary arteries with nonocclusive,mural thrombi in the large pulmonaryarteries (Figure 2A and B). V/Q lungscan showed diffuse heterogeneous non-segmental perfusion defects in the lungsbilaterally without significant changesfrom baseline scan and consistent withunderlying PAH (Figure 1B).
Diagnosis:The patient was diagnosed with decom-pensated right heart failure due to
Figure 2: A. CTPA representative section demonstrating dilated ectatic pulmonary artery trunk measuring 64.7 mm (blue line) and nonocclusiveintraluminal thrombi in the right pulmonary artery and the main pulmonary trunk (red arrows). B-D. Representative sections of the CTPA showingnonocclusive intraluminal thrombi in the right and left pulmonary artery branches (red arrows)
Table 1. Right heart catheterizations
Initial Current
Right atrial pressure, mm Hg 12/9 (7) 26/22 (18)
Right atrial oxygen saturation, % 66 56
Right ventricular pressure, mm Hg 91/4 (11) 73/15 (34)
Pulmonary artery pressure, mm Hg 92/41 (58) 75/43 (54)
Pulmonary artery oxygen saturation, % 65 59
Pulmonary artery wedge pressure, mm Hg 14/14 (11) 23/22 (18)
Cardiac output, L/min (thermodilution) 6.9 4.5
Cardiac index, L/min/m2 3.5 2.3
Pulmonary vascular resistance, Wood units 6.8 8.0
123Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

untreated PAH. Imaging studies wereevaluated at a chronic thromboembolicpulmonary hypertension (CTEPH) sur-gical center, and there was agreementwith the diagnosis of PAH with sec-ondary “lining” thrombus within theaneurysmal pulmonary arteries. Intra-venous epoprostenol was initiated at adose of 2 ng/kg/min, and it was titratedup by 2 ng/kg/min as tolerated. Thepatient was discharged from the hospitalafter placement of a single lumenHickman on 12 ng/kg/min of epopros-tenol, sotalol and warfarin. In our case,the chronicity of PAH along with reviewof the radiologic studies showing laminarorganized thrombi favored a diagnosis ofPAH with associated pulmonary arteryaneurysm (PAA) and intramuralthrombi. On follow-up in clinic 4 weekspost-hospital discharge, the patientreported significant improvement overall.His breathing had returned to baselineNYHA FC 2 without palpitations orsyncope.
Discussion: Review of the LiteraturePAA, characterized by enlargement ofthe pulmonary artery or its branches, is arare condition that is most commonlyassociated with PAH or CHD.1-4 PAAis not infrequently complicated by intra-mural thrombi and/or pulmonary arterydissection.3 Most often, symptomsattributed to PAA are nonspecific and
diagnosis is made by noninvasiveimaging (chest roentgenogram, comput-erized tomography [CT], or magneticresonance imaging [MRI]). The dis-tinction between in situ thrombosis ofthe ectatic pulmonary arteries in thesetting of PAH and CTEPH is of para-mount importance given the significanttherapeutic implications. We present acase that illustrates the difficulty of dif-ferentiation between these 2 conditions.
Specifically, the combination of a “lowprobability” V/Q scan and centraleccentric mural thrombi supported theconclusion that the patient did not haveCTEPH. In addition, if there is consid-eration that the thrombi are hemo-dynamically relevant, right heartcatheterization and measurement of thepressure gradient across these lesionsmay be informative. In PAH with sec-ondary central thrombi, there should beno pressure gradient from the proximalto distal branches (Channick RN, per-sonal communication, September 2014).
There are several case reports in theliterature about PAA in association withPAH; however, the management of thiscondition remains controversial.1-6 PAAcan be complicated by hemoptysis, pul-monary artery dissection and/or rupture,intramural thrombi, or mechanical com-pression of adjacent structures—namelythe coronary arteries, main bronchi, orthe superior vena cava.3 Although anti-
coagulation would be logical to decreasethe incidence of thrombi in the settingof PAA, the decision is often difficultbecause PAAs are inherently at increasedrisk of bleeding.2
In patients with long-standing PAH,especially when associated with CHD,chest imaging can reveal the presence ofPAA. Given the clinical, prognostic, andtherapeutic implications, it is importantfor physicians who care for such patientsto distinguish between PAA associatedwith intramural thrombi and CTEPH.
References1. Barbour DJ, Roberts WC. Aneurysm of thepulmonary trunk unassociated with intracardiac orgreat vessel left-to-right shunting. Am J Cardiol.1987;59(1):192-194.2. Broberg C, Ujita M, Babu-Narayan S, et al.Massive pulmonary artery thrombosis withhaemoptysis in adults with Eisenmenger’s syn-drome: a clinical dilemma. Heart. 2004;90(11):e63.3. Bartter T, Irwin RS, Nash G. Aneurysms ofthe pulmonary arteries. Chest. 1988;94(5):1065-1075.4. Moser KM, Fedullo PF, Finkbeiner WE,Golden J. Do patients with pulmonary hyper-tension develop extensive central thrombi?Circulation. 1995;91(3):741-745.5. Agarwal PP, Wolfsohn AL, Matzinger FR,Seely JM, Peterson RA, Dennie C. In situ centralpulmonary artery thrombosis in primary pulmonaryhypertension. Acta Radiol. 2005;46(7):696-700.6. Della Coletta JA, Tanni SE, Coelho LS,Cataneo DC, Ribeiro SM, Godoy I. Pulmonaryartery aneurysm complicated by mural thrombus: acase report. Am J Med Sci. 2008;336(1):69.
124 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

Challenges in Endpoint Development for PulmonaryHypertension Trials in Children
Dunbar Ivy, MDProfessor of PediatricsUniversity of Colorado School of MedicineChildren’s Hospital ColoradoAurora, CO
There are currently 12 medications approved for use in the treatment of pulmonaryarterial hypertension (PAH) in adults. These include endothelin receptor antagonists,phosphodiesterase type 5 inhibitors, soluble guanylate cyclase stimulators, and prosta-cyclins. However, in children there are no approved targeted PAH medications, withthe exception of inhaled nitric oxide for treatment of hypoxemic respiratory failure inneonates. This review will address some of the challenges in the development oftreatments for children, including lessons from recent trials, endpoints for clinicaltrials, and challenges with drug approval in children.
Impediments to enrolling children inclinical trials are many. Pulmonaryhypertension (PH) is a rare disorder inadults and even less common inchildren.1 For example, idiopathic pul-monary arterial hypertension (IPAH) is arare disease with an incidence of 1 to 2per million adults. The incidence ofIPAH in children is 0.7 cases permillion children.2 Physicians often pre-scribe drugs approved for use in adultsoff label in children. Furthermore,parents are reluctant to enroll childrenwith a serious disabling and progressivedisease in a controlled clinical trial, espe-cially one in which the child may receivea placebo. Children are considered a vul-nerable population; they aredevelopmentally, physiologically, andpsychologically different than adults,thereby complicating research efforts.3
Investigators and federal agencies arevery reluctant to perform a study inchildren that may be associated withincreased risk. An example is the recentUS Food and Drug Administration(FDA) decision to exclude cardiac cathe-terization from PH clinical trials inchildren. The FDA made this decisionbecause there was a greater risk of deathin children with PH. Although the riskis difficult to quantify, it appears to equalabout 1%.4 There are also consent issues,as parents should provide consent andchildren over 7 years of age must assent.These issues lead to slow enrollment.
The primary endpoint of most adultpulmonary arterial hypertension (PAH)trials has almost exclusively been exercisecapacity as assessed by the 6-minutewalk test,5-12 a combined measureincluding the 6-minute walk,13 and(more recently) event-driven trials.14 Asingle trial used cardiopulmonary exercisetesting15; however, this endpoint wasabandoned since the trial was negative.Secondary endpoints frequently includehemodynamics, functional class, qualityof life, and biomarkers such as brainnatriuretic peptide (BNP).
One of the first studies in childrenwas the BREATHE-3 (Bosentan Ran-domized trial of Endothelin AntagonistTHErapy for pulmonary hypertension)trial of bosentan.16 This was an open-label 12-week study of 19 children;dosing was empiric and based on adultlevels. Study endpoints included pharma-cokinetics, safety, and cardiaccatheterization parameters. The studyrevealed valuable information on dosingand safety. Catheterization parameterswere significant; however, these datawere not sufficient for labeling. Subse-quent studies of bosentan focused onpharmacokinetics of a novel formulationof bosentan in children with PAH. Inthe FUTURE-1 (Pediatric FormUlationof bosenTan in pUlmonary arterialhypeRtEnsion) study, the pharmacoki-netics of bosentan at doses of 2 mg/kgtwice a day was compared with 4 mg/kg
twice a day, and revealed no differencein drug exposure.17 The FUTURE-3study evaluated pharmacokinetics, tolera-bility, safety, and efficacy of the pediatricformulation of bosentan twice vs 3 timesa day.
The STARTS-1 (Sildenafil inTreatment-naıve Children, aged 1-17years, with Pulmonary Arterial Hyper-tension) pediatric trial was a landmarkstudy, as it was the first randomized,double-blind, placebo-controlled, anddose-ranging parallel group study of aPH drug in children.18 It also highlightsmany of the problems inherent in apediatric PH trial. The patient popu-lation was treatment-naıve children aged1 to 17 years with PAH. The trial beganenrollment in August 2003, and com-pleted in February 2008. Thus, it tookmore than 5 years to enroll a sufficientnumber of patients to be tested for theprimary endpoint: to assess the efficacyof 16 weeks of chronic treatment withoral sildenafil in pediatric patients withPAH, as measured by exercise toleranceusing bicycle ergometry testing only inthose subjects able to perform theexercise test. Just about half of thechildren enrolled could perform thebicycle ergometry test. All children hadcardiac catheterization. The primaryefficacy endpoint was the percent changefrom baseline in peak oxygen con-sumption at Week 16, with mainsecondary endpoints of change frombaseline in mean pulmonary arterypressure and pulmonary vascular resis-tance index. Patients were randomized toplacebo, low-dose, medium-dose, orhigh-dose sildenafil and treated for a
Key Words—biomarkers, clinical trials, endpoint, pharmacokinetic parameters, safetyCorrespondence: [email protected]: The University of Colorado receives fees for Dr Ivy to be a consultant for Actelion, Bayer,Gilead, Lilly, Pfizer, and United Therapeutics.
125Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

total of 16 weeks. Cardiac catheter-ization and exercise testing wereperformed after 16 weeks of therapy.The trial did not meet its primary end-point, which was the combined changein placebo-adjusted percent change inpeak oxygen consumption (P�0.056).There were improvements in someparameters of pulmonary pressure andpulmonary vascular resistance. After the16 weeks, patients in the low-, medium-,and high-dose groups remained on thatdose. Patients in the placebo group wererandomized to low, medium, or highdose; patients were then followed for theduration of the study. If the patientrequired additional therapy, he/she wasdiscontinued. The controversy with thestudy arose when mortality was evaluatedon a yearly basis. At 1 year, only 1patient had died in the high-dose group.By 2 years, there was a trend for anincrease in mortality in the high-dosegroup. By 3 years, the hazard ratio formortality was 3.95 (95% confidenceinterval, 1.46-10.65) for high vs lowdose. Most patients who died (28/37)had idiopathic/heritable PAH (76% vs33% overall) and baseline functional classIII/IV disease (38% vs 15% overall);patients who died had worse baselinehemodynamics. Kaplan-Meier estimated3-year survival rates from the start ofsildenafil were 94%, 93%, and 88% forpatients randomized to low-, medium-,and high-dose sildenafil.19 Based on this,the data monitoring committee recom-mended that all patients down-titratefrom the high dose.
Review of the STARTS-1 and -2data by the FDA and the EuropeanMedicines Agency (EMA) resulted indisparate recommendations. Sildenafilwas approved by the EMA in 2011,with a later warning on avoidance of useof the high dose. In August 2012, theFDA released a strong warning againstthe (chronic) use of sildenafil for pedi-atric patients (ages 1 through 17) withPAH (http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm317743.htm). The warning stated that “. . . thisrecommendation against (sildenafil) use isbased on a recent long-term clinical pedi-atric trial showing that: (1) children takinga high dose of Revatio had a higher risk of
death than children taking a low dose, and(2) the low doses of Revatio are noteffective in improving exercise ability.Revatio has never been approved for thetreatment of PAH in children, and in lightof the new clinical trial information, off-label (not approved by FDA) use of thedrug in pediatric patients is not recom-mended . . . .” The results of theSTARTS-2 trial are difficult to inter-pret: 1) there was no placebo groupincluded; 2) doses of sildenafil changedduring the study; 3) patients requiringadditional PAH therapy were with-drawn; 4) children were not censoredonce withdrawn from the study to addtherapy or because of withdrawal ofconsent, but continued to be followed;5) the mortality signal was not consistentacross weight groups or etiologies.Children 8-20 kg did not have anincrease in mortality with high-dosesildenafil, nor did patients with con-genital heart disease. The study ended inDecember 2012; at that time, there were42 deaths: 18% of the total. In thelow-dose groups, mortality was 9.1%; inthe medium-dose group, mortality was17.6%; and in the high-dose group,mortality was 24%. Following a meetingwith the FDA by members of theAmerican Heart Association, AmericanCollege of Cardiology, and AmericanAcademy of Pediatrics, the FDA clar-ified the sildenafil warning, stating thatthere may be situations in which therisk-benefit profile of Revatio may beacceptable in individual children, andthat sildenafil is still not recommendedin children with PH. The statementfurther indicates that the initial recom-mendation was not intended to suggestthat Revatio should never be used inchildren (http://www.fda.gov/Drugs/DrugSafety/ucm390876.htm).
Other biomarkers have been evaluatedin children with PAH and may be usedas secondary endpoints. Several studieshave evaluated the levels of BNP/N-terminal pro-BNP (NT-proBNP) inchildren with PAH, and found thatthose children with a higher value havean increase in mortality.20-22 In the Reg-istry to Evaluate Early and Long-termPAH Disease Management (REVEAL),older age at diagnosis, cardiac index atdiagnosis, and pulmonary vascular resis-
tance index at diagnosis were associatedwith worse survival.23 In the Netherlandsregistry, mortality variables associatedwith increased mortality includedincreased World Health Organization(WHO) functional class (WHO-FC),decreased systolic blood pressure,increased pulmonary to systemic arterialpressure ratio, increased NT-proBNP,and increased uric acid.24 Worse survivalhas consistently been associated withworse WHO-FC in children.23-26 Fur-thermore, hemodynamic parameters areassociated with survival.26,27 Imagingstudies such as cardiac MRI and tissueDoppler evaluation are also predictive ofoutcome.28,29 Other clinically relevantendpoints might include growth param-eters and quality-of-life questionnaires.30
A fault of these studies is thattreatment-induced changes were notshown. Recently a study in the Nether-lands has shown that the variables ofWHO-FC, NT-proBNP, and tricuspidannular plane systolic excursion by echo-cardiography were identified as follow-uppredictors in which treatment-inducedchanges were associated with survival.30
Exercise capacity is of particularinterest, as it satisfies the FDA require-ments that drugs make patients feelbetter and live longer. The challengewith 6-minute walk distance is thatchildren are not reliable in performingthis test and sometimes run for parts ofthe test. Baseline 6-minute walk distanceis not a predictor of survival, neitherwhen expressed as an absolute distancein meters nor when adjusted to referencevalues expressed as z-score or as per-centage of predicted value.22,24,25,31,32
Cardiopulmonary exercise testing stillhas a potential role, but has not beenproven to be a surrogate; the only pedi-atric trial in which it was used, theSTARTS-1 trial, did not meet theprimary endpoint.
Future clinical trials should bedesigned to be informative for practicingphysicians. They should include safety,pharmacokinetics, a measure of efficacy,and cardiac catheterization in a subpopu-lation. An efficacy endpoint is needed,particularly if there is a desire to obtainlabeling, and for industry to obtain apatent extension. The EMA has man-dated a pediatric investigational plan
126 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

(PIP) for all new drugs. A PIP is adevelopment plan intended to ensurethat the necessary data are obtainedthrough studies to support the authori-zation of a medicine for children. In theUS, pediatric PAH is an orphan disease,and therefore there is no mandate forstudy. The requirements for a patentextension are rigorous and require arobust efficacy trial. Time to clinicalworsening or event-driven trials haveshown promise in adult PH. Themacitentan-SERAPHIN (Study with anEndothelin Receptor Antagonist in Pul-monary arterial Hypertension to ImprovecliNical outcome) trial utilized a mor-bidity and mortality primary endpointthat included the time from the initi-ation of treatment to the first occurrenceof a composite endpoint of death, atrialseptostomy, lung transplantation, initi-ation of treatment with intravenous orsubcutaneous prostanoids, or worseningof PAH.14 A similar design is appealingin pediatrics because it allows for aclinical worsening event-driven trial thatwould not require a single primary vali-dated endpoint. Disadvantages of thistrial design would include the need for alarge number of patients to meet anendpoint. These trials would take severalyears and would likely require multipledoses to satisfy the concern of a dose-response increase in mortality withsildenafil.
In conclusion, PAH trials are difficultto perform in children for many reasons.Both consent and assent are required;inclusion of a placebo arm is challengingfor parents to accept; and an efficacy trialis difficult to perform due to the smallnumber of patients involved. A hemody-namic or exercise primary endpoint isproblematic since not all patients areevaluable, and the FDA has limited theuse of catheterization in approvedclinical trials. Safety and pharmacokineticparameters are important evaluations inany pediatric trial. An event-driven trialis more appealing, but will take years toenroll and complete.
References1. Ivy DD, Abman SH, Barst RJ, et al. Pediatricpulmonary hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D117-D126.
2. van Loon RL, Roofthooft MT, Hillege HL,et al. Pediatric pulmonary hypertension in theNetherlands: epidemiology and characterizationduring the period 1991 to 2005. Circulation. 2011;124(16):1755-1764.3. Adatia I, Haworth SG, Wegner M, et al.Clinical trials in neonates and children: Report ofthe pulmonary hypertension academic researchconsortium pediatric advisory committee. PulmCirc. 2013;3(1):252-266.4. Beghetti M, Berger RM, Schulze-Neick I, etal; TOPP Registry Investigators. Diagnostic evalu-ation of paediatric pulmonary hypertension incurrent clinical practice. Eur Respir J. 2013;42(3):689-700.5. Rubin LJ, Badesch DB, Barst RJ, et al.Bosentan therapy for pulmonary arterial hyper-tension. N Engl J Med. 2002;346(12):896-903.6. Galie N, Olschewski H, Oudiz RJ, et al;Ambrisentan in Pulmonary Arterial Hypertension,Randomized, Double-Blind, Placebo-Controlled,Multicenter, Efficacy Studies (ARIES) Group.Ambrisentan for the treatment of pulmonaryarterial hypertension: results of the ambrisentan inpulmonary arterial hypertension, randomized,double-blind, placebo-controlled, multicenter,efficacy (ARIES) study 1 and 2. Circulation. 2008;117(23):3010-3019.7. Galie N, Ghofrani HA, Torbicki A, et al;Sildenafil Use in Pulmonary Arterial Hypertension(SUPER) Study Group. Sildenafil citrate therapyfor pulmonary arterial hypertension. N Engl J Med.2005;353(20):2148-2157.8. Galie N, Brundage BH, Ghofrani HA, et al;Pulmonary Arterial Hypertension and Response toTadalafil (PHIRST) Study Group. Tadalafiltherapy for pulmonary arterial hypertension. Circu-lation. 2009;119(22):2894-2903.9. Barst RJ, Rubin LJ, Long WA, et al; PrimaryPulmonary Hypertension Study Group. A com-parison of continuous intravenous epoprostenol(prostacyclin) with conventional therapy forprimary pulmonary hypertension. N Engl J Med.1996;334(5):296-302.10. Simonneau G, Barst RJ, Galie N, et al;Treprostinil Study Group. Continuous subcuta-neous infusion of treprostinil, a prostacyclinanalogue, in patients with pulmonary arterialhypertension: a double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med. 2002;165(6):800-804.11. Ghofrani HA, Galie N, Grimminger F, et al;PATENT-1 Study Group. Riociguat for thetreatment of pulmonary arterial hypertension.N Engl J Med. 2013;369(4):330-340.12. Jing ZC, Parikh K, Pulido T, et al. Efficacyand safety of oral treprostinil monotherapy for thetreatment of pulmonary arterial hypertension: arandomized, controlled trial. Circulation. 2013;127(5):624-633.13. Olschewski H, Simonneau G, Galie N, et al;Aerosolized Iloprost Randomized Study Group.Inhaled iloprost for severe pulmonary hypertension.N Engl J Med. 2002;347(5):322-329.14. Pulido T, Adzerikho I, Channick RN, et al;SERAPHIN Investigators. Macitentan and mor-bidity and mortality in pulmonary arterialhypertension. N Engl J Med. 2013;369(9):809-818.
15. Barst RJ, Langleben D, Frost A, et al;STRIDE-1 Study Group. Sitaxsentan therapy forpulmonary arterial hypertension. Am J Respir CritCare Med. 2004;169(4):441-447.16. Barst RJ, Ivy D, Dingemanse J, et al. Phar-macokinetics, safety, and efficacy of bosentan inpediatric patients with pulmonary arterial hyper-tension. Clin Pharmacol Ther. 2003;73(4):372-382.17. Beghetti M, Haworth SG, Bonnet D, et al.Pharmacokinetic and clinical profile of a novel for-mulation of bosentan in children with pulmonaryarterial hypertension: the FUTURE-1 study. Br JClin Pharmacol. 2009;68(6):948-955.18. Barst RJ, Ivy DD, Gaitan G, et al. A ran-domized, double-blind, placebo-controlled, dose-ranging study of oral sildenafil citrate in treatment-naive children with pulmonary arterialhypertension. Circulation. 2012;125(2):324-334.19. Barst RJ, Beghetti M, Pulido T, Layton G,Konourina I, Zhang M, Ivy DD; STARTS-2Investigators. STARTS-2: long-term survival withoral sildenafil monotherapy in treatment-naivepediatric pulmonary arterial hypertension. Circu-lation 2014;129(19):1914-1923.20. Lammers AE, Hislop AA, Haworth SG.Prognostic value of B-type natriuretic peptide inchildren with pulmonary hypertension. IntJ Cardiol. 2009;135(1):21-26.21. Bernus A, Wagner BD, Accurso F, Doran A,Kaess H, Ivy DD. Brain natriuretic peptide levelsin managing pediatric patients with pulmonaryarterial hypertension. Chest. 2009;135(3):745-751.22. Van Albada ME, Loot FG, Fokkema R,Roofthooft MT, Berger RM. Biological serummarkers in the management of pediatric pulmonaryarterial hypertension. Pediatr Res. 2008;63(3):321-327.23. Barst RJ, McGoon MD, Elliott CG,Foreman AJ, Miller DP, Ivy DD. Survival inchildhood pulmonary arterial hypertension: insightsfrom the registry to evaluate early and long-termpulmonary arterial hypertension disease man-agement. Circulation. 2012;125(1):113-122.24. van Loon RL, Roofthooft MT, Delhaas T, etal. Outcome of pediatric patients with pulmonaryarterial hypertension in the era of new medicaltherapies. Am J Cardiol. 2010;106(1):117-124.25. Moledina S, Hislop AA, Foster H, Schulze-Neick I, Haworth SG. Childhood idiopathicpulmonary arterial hypertension: a national cohortstudy. Heart. 2010;96(17):1401-1406.26. Ivy DD, Rosenzweig EB, Lemarie JC, BrandM, Rosenberg D, Barst RJ. Long-term outcomesin children with pulmonary arterial hypertensiontreated with bosentan in real-world clinical set-tings. Am J Cardiol. 2010;106(9):1332-1338.27. Douwes JM, van Loon RL, Hoendermis ES,et al. Acute pulmonary vasodilator response in pae-diatric and adult pulmonary arterial hypertension:occurrence and prognostic value when comparingthree response criteria. Eur Heart J. 2011;32(24):3137-3146.28. Takatsuki S, Nakayama T, Jone PN, et al.Tissue Doppler imaging predicts adverse outcomein children with idiopathic pulmonary arterialhypertension. J Pediatr. 2012;161(6):1126-1131.
127Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

29. Moledina S, Pandya B, Bartsota M, et al.Prognostic significance of cardiac magnetic reso-nance imaging in children with pulmonaryhypertension. Circ Cardiovasc Imaging. 2013;6(3):407-414.30. Ploegstra MJ, Douwes JM, Roofthooft MT,
Zijlstra WM, Hillege HL, Berger RM. Identifi-cation of treatment goals in paediatric pulmonaryarterial hypertension. Eur Respir J. 2014. In press.31. Haworth SG, Hislop AA. Treatment andsurvival in children with pulmonary arterial hyper-tension: the UK Pulmonary Hypertension Service
for Children 2001-2006. Heart. 2009;95(4):312-317.32. Lammers AE, Munnery E, Hislop AA,Haworth SG. Heart rate variability predictsoutcome in children with pulmonary arterial hyper-tension. Int J Cardiol. 2010;142(2):159-165.
128 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

Repurposing FK506 to Increase BMPR2 Signaling andImprove Pulmonary Arterial Hypertension: A Fast Track FromCells to People
Edda Spiekerkoetter, MDThe Vera Moulton Wall Center for
Pulmonary Vascular DiseaseDepartment of Medicine, Stanford
University School of MedicineStanford, CA
Roham T. Zamanian, MDThe Vera Moulton Wall Center for
Pulmonary Vascular DiseaseDepartment of Medicine, Stanford
University School of MedicineStanford, CA
To improve long-term survival in pulmonary arterial hypertension (PAH), newtreatment approaches that target occlusive vasculopathy instead of vasoconstriction ofpulmonary arteries are necessary. Identifying genes or pathways that unify differentpathologies and etiologies in PAH is a crucial first step for drug development. Thebone morphogenetic protein receptor 2 (BMPR2) pathway, originally described asthe cause of familial PAH, has gained significant interest over the past few years as apotential master switch in PAH, and therefore presents a promising treatment targetin PAH. FK506 (tacrolimus) was found in a high-throughput screen of US Foodand Drug Administration (FDA)-approved drugs to significantly increase BMPR2signaling. Low-dose FK506 was able to restore normal BMPR2 signaling andfunction in patient pulmonary artery (PA) endothelial cells, inhibit proliferation andinduce apoptosis in PA smooth muscle cells, and prevent and reverse pulmonaryhypertension (PH) in 3 experimental rodent models of PH. As an FDA-approveddrug, it was possible to relatively quickly (in approximately 2 years) translate the basicscience discoveries from the bench to the clinic. A Phase 2 proof-of-concept safetyand tolerability trial is underway (ClinicalTrials.gov Identifier: NCT01647945) toevaluate the use of low-dose FK506 in PAH and to identify patients who mightrespond best to FK506 depending on their impairment in BMPR2 signaling.
Pulmonary arterial hypertension (PAH)is a devastating disease that affectspatients of all ages, and if left untreatedleads to right heart failure and deathwithin 2 to 3 years.1,2 The histopa-thology is characterized by occlusivevasculopathy of pulmonary arteries withdysfunction of endothelial and smoothmuscle cells, as well as adventitialfibroblasts and inflammatory cells.Unfortunately, existing PAH drugs onlydilate pulmonary arteries, while occlusivevasculopathy progresses unchecked untilpatients eventually need lung transplan-tation or die of the disease.3-5 Therefore,there is a fundamental gap betweencurrent treatment for PAH and the needto reverse occlusive vasculopathy inPAH. Numerous molecular abnormal-ities have been described in PAH,6 yettranslation into the clinic has been ham-
pered as respective therapies that target acandidate pathway propose only onetreatment for one abnormality,7 nottaking into account different etiologies,pathologies, as well as multiple contrib-uting factors in PAH such as theinvolvement of the immune system,8
metabolism,7 elastase activation,9 andepigenetic mechanisms.10-14
THE IMPORTANCE OF BMPR2SIGNALING AS A POTENTIAL“MASTER SWITCH” IN PAHIt has emerged that the bone morphoge-netic protein receptor (BMPR2) pathwaymight link many of the “players” inPAH pathology, in that it either regu-lates or is regulated—is either acause or a consequence of the abovemechanisms15-20—which makes modu-lation of BMPR2 signaling a promising
treatment approach.21,22 Germline muta-tions causing BMPR2 loss of functionhave been described in about 80% ofpatients with hereditary PAH,23,24 andmutations in other members of thetransforming growth factor (TGF)-�superfamily have been found, such asaktivin-like kinase-1 (ALK1), endoglin,smad9, and caveolin-1, which also resultin dysfunctional BMPR2 signaling.21
Furthermore, even patients without aBMPR2 mutation have reduced BMPR2expression in their pulmonary arteries atthe time of lung transplantation.25 Thereis evidence that patients with idiopathicor autoimmune-associated PAH withongoing inflammation and increasedlevels of the cytokine IL-6 have lowerBMPR2 expression in their blood, and ithas been shown in cell culture that IL-6reduces BMPR2 expression via aSTAT3-miR17/92 mechanism.16
As further evidence that BMPR2dysfunction might be the result of analtered immune system, it was shownthat the viral proteins HIV-nef andHIV TAT, which are released byinfected lymphocytes and macrophagesduring an HIV infection, decrease
Key Words—drug repurposing, FK506, PAH, BMPR2 signaling, FKBP12Correspondence: [email protected]: Dr Zamanian is a consultant for United Therapeutics, Actelion, and Bayer, and has receivedresearch support from Actelion and United Therapeutics. Drs Zamanian and Spiekerkoetter are advisorsfor Selten Pharma Inc. Drs Spiekerkoetter and Zamanian are supported by the Vera Moulton Wall Centerfor Pulmonary Vascular Disease at Stanford. Dr Spiekerkoetter is supported by grants from the NationalInstitutes of Health (NIH)/NIH Heart, Lung and Blood Institute (NHLBI), the Pulmonary HypertensionAssociation (PHA), SPARK at Stanford, and the Stanford Cardiovascular Institute.
129Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

BMPR2 expression in pulmonary arterysmooth muscle cells (PASMCs): HIVTAT by repressing the BMPR2 pro-moter26 and HIV-nef potentially byinterfering with the intracellular traf-ficking of BMPR2.27 Macaques withinfected chimeric simian/human immu-nodeficiency virus (SHIV) containingHIV-1-derived Nef protein developsevere pulmonary hypertension (PH)characterized by occlusive pulmonaryvasculopathy mimicking the humandisease.28 The effect of an HIVinfection on BMPR2 expression is evenmore pronounced in the presence ofdrugs such as cocaine,29 commonly usedby HIV-positive intravenous drug users.On the contrary, reconstitution ofathymic rats with regulatory T cells pre-vents PH induced by the vascularendothelial growth factor (VEGF)receptor blocker SUGEN5416, and isassociated with an increase in BMPR2expression in pulmonary arteries.17
With regard to the role of BMPR2in metabolism, recent data suggest thatenhanced estrogenic activity decreasesBMP signaling in a susceptible host,whereas altered BMP signaling modifiesestrogenic activity.30 BMPR2 isinvolved in the regulation of hepcidingene expression and iron metabolism,31
and most recently has been shown to be
associated with insulin resistance32,33
and impaired fatty acid oxidation inexperimental PH.34 In addition, meta-bolic reprogramming in PAH occursdownstream of BMPR2,35 which issupported by studies in mice with adisease-causing mutation in BMPR2that are more susceptible to oxidantinjury in mitochondrial membranescompared to wild-type animals.36 Fur-thermore, it was recently shown thatthe human neutrophil inhibitor elafininteracts with caveolin-1 to facilitateBMPR2 signaling and endothelialhomeostasis,37 linking elevated elastaseactivity to a reduced BMPR2 signaling.In addition, Drake et al showed thatmutations in BMPR2 impaired normalmicro RNA processing of miR-21 andmiR-27a, which likely contributes tovascular cell proliferation in PAH.38
These examples illustrate that BMPR2signaling presents a critical pathway inPAH and a potential master switchlinking different PAH pathologies andetiologies. We hypothesize that there isa threshold of BMPR2 signaling belowwhich PAH develops, either due to aBMPR2 mutation, environmentalfactors, or modifier genes. Therefore,targeting the BMPR2 pathway could bea promising treatment approach inPAH (Figure 1).
INCREASING BMPR2SIGNALING WITH FK506We performed a high throughput screenof �3000 US Food and Drug Adminis-tration (FDA)-approved drugs andbioactive compounds using a reporter cellline where the BMP response element(BRE) from the Id1 promoter waslinked to luciferase22 to identify acti-vators of Id1 expression and, respectively,BMPR2 signaling. FK506 (tacrolimus)was identified as the best BMPR2activator. Even at low, sub-immunosuppressive doses (0.2-2ng/mL), FK506 was able to bind toFKBP12, and by doing so removed theBMPR2 inhibitor FKBP12 from thetype 1 receptors ALK1, ALK2, andALK3, allowing for phosphorylation ofthe type 1 receptor and subsequentdownstream smad dependent and inde-pendent signaling. In addition, FK506inhibited the phosphatase calcineurin,which also facilitated phosphorylation ofthe type 1 receptor. Previous studies hadshown that FKBP12 was necessary forSMURF-1 mediated degradation of type1 and type 2 TGF-� receptors.39 Byremoving FKBP12 from the type 1receptor, FK506 is able to preventSMURF-1 and smad7 mediated type 1and type 2 receptor degradation, leadingto an increase in BMPR2 protein
Figure 1: Strategy to identify new treatments in PAH. Figure 1 shows the drug development approach to finding new treatments in PAH—fromthe identification of a new drug target for PH based on a known genetic basis in PAH to the final testing of a repurposed drug in patients.
130 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

expression (unpublished data). FK506was superior to rapamycin and cyclo-sporin in increasing BMPR2 signaling,due to its dual function as a calcineurininhibitor and binder of FKBP12, as wellas its ability to remove FKBP12 from all3 type 1 receptors, ALK1, ALK2, andALK3, which are implicated in BMPsignaling (Figure 2).
FK506 PREVENTS ANDREVERSES EXPERIMENTAL PHIncreasing BMPR2 signaling bylow-dose FK506 (blood level 0.2 ng/mL)prevented the development of hypoxia-induced PH in mice with a conditionalendothelial deletion of BMPR2 byimproving endothelial health and pre-venting loss of small vessels.22 Low-doseFK506 was also able to reverse estab-lished severe PH in rats exposed to theendothelial toxin monocrotaline byreducing medial hypertrophy. Fur-thermore, low-dose FK506 reversedsevere PH and occlusive vasculopathy inrats where PH was induced by theVEGF receptor blocker SUGEN5416,followed by 3 weeks exposure to 10%hypoxia and 5 weeks normoxia. Thisanimal model refined by Abe et al40
mimics the clinical disease very well, as itis characterized by severe PH accom-panied by an occlusive vasculopathy ofsmall pulmonary arteries.
FK506 IN CLINICAL USEFOR PAHFK506 has been used for more than 20years as a potent immunosuppressiveagent in solid organ transplantation.Low-dose FK506 is used in certain auto-immune diseases such as psoriasis andrheumatoid arthritis, again for its anti-inflammatory properties.41 Furthermore,FK506 was found to increase endothelialexpression of ALK1 and endoglin.42 Asloss-of-function mutations in these genesare observed in PAH associated withhemorrhagic hereditary telangiectasia(HHT), FK506 could also be ofpotential benefit in patients with thisdisorder. In fact, FK506 was given fol-lowing liver transplant in a patient withHHT who had multiple arteriovenousmalformations, and it was noted thatinternal and external telangiectases, epi-staxes, and anemia disappeared,suggesting that the mechanism of actionof FK506 involved partial correction ofendoglin and ALK1 haploinsufficiency.42
We have treated 3 end-stage PAHpatients with low-dose FK506 with verypromising results (unpublished data).Subsequently, a Phase 2 proof-of-concept safety and tolerability trial wasinitiated at Stanford University to testwhether low-dose FK506 treatment isfeasible in PAH, and to identify patientswho might benefit most from low-doseFK506 depending on their BMPR2impairment (ClinicalTrials.gov Identifier:NCT01647945). One goal of this trial isto develop a “BMPR2 signature” in theblood of PAH patients at baseline andfollow-up to first prove that the BMPR2pathway is targeted by the study drug,and second to define and develop criteriathat might reflect which patient sub-group potentially responds best totherapy—valuable information for thedesign of a subsequent efficacy trial.
THE ADVANTAGES OF DRUGREPOSITIONING IN PAH—FROM CELLS TO PEOPLERecycling is good for the environmentand for drug development, as well.There are multiple advantages to repur-posing existing drugs for the treatmentof PAH. New drug development is a
Figure 2: FK506 increases BMPR2 signaling through multiple avenues. The left panel shows that in the presence of a subactivating dose of theligand BMP, phosphorylation of the type 1 receptor and subsequent downstream signaling is inhibited by binding of FKBP12 to the phosphory-lation site of the type 1 receptor. Under the same conditions, yet with FK506 present (right panel), FK506 pulls FKBP12 away from the type 1receptor. By doing so, it allows the type 1 receptors (ALK1, ALK2, ALK3) to become phosphorylated. Furthermore, binding of SMURF-1 to thereceptor complex is prevented, as SMURF-1 requires FKBP12 to be present as a docking site. Consequently, SMURF-1 mediated degradationof the type 1 and 2 receptors is impaired, leading to an increased protein expression of BMPR2. As a third mode of action, FK506 inhibits thephosphatase calcineurin, facilitating phosphorylation of the type 1 receptor.
131Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

long, expensive, and complicated processstarting with research to determinetargets for treatment. Once a promisingcompound has been identified, pre-clinical research is done, which ofteninvolves pharmacokinetic and toxicologystudies, testing of the compound inmodel systems of disease such asPASMCs as well as in animal models ofPAH. Once a compound has completedpreclinical testing, it moves into humanclinical trials. The purpose of a clinicaltrial is to test a new drug or other inter-vention for safety and effectiveness intreating the disease in question before itcan be prescribed to patients. Theinstitutional principal investigators andreview boards, the Data SafetyMonitoring Board, and the steeringcommittees are charged with oversight ofthe trial, whereas the FDA is involved inevaluation and approval of new therapiesin PAH. The average drug developmenttime once a lead compound has beenidentified is about 15 years, includingpreclinical research, development, pivotaltrials, clinical research, and post-approvalstudies. The average cost for drug devel-opment is between $500 million and $1billion, and is relatively more expensivefor rare diseases such as PAH. Identi-fying and testing drugs that are alreadyFDA approved shortens the devel-opment duration significantly. Inaddition, drug development can be con-siderably less expensive with repurposeddrugs, which might result in betteraffordability for patients.
As repurposed drugs were originallydeveloped for different indications, themode of action often involves severaldifferent pathways instead of a singleone. This is a potential advantage, asseen in the case of low-dose FK506 andPAH. While FK506 increases BMPR2signaling, it also mildly inhibits thenuclear factor of activated T-cells(NFATc) activation. Although not themajor effect, as least in our studies ofexperimental PH, the potential effect onNFATc signaling might be beneficial inPAH. Cyclosporin was found to inhibitNFATc2, restore the potassium channelKv1.5 expression, decrease proliferation,and increase apoptosis of PASMCs, andwas able to decrease established PH inthe monocrotaline rat model.43
Changing the paradigm of drug devel-opment from novel compounds for PAHto repurposing existing drugs offers theadvantage of a known safety and toxicityprofile, resulting in shorter dose-findingstudies and accelerating the use of apotential disease-modifying drug inpatients.
References1. Barst RJ, Rubin LJ, Long WA, et al; PrimaryPulmonary Hypertension Study Group. A com-parison of continuous intravenous epoprostenol(prostacyclin) with conventional therapy forprimary pulmonary hypertension. N Engl J Med.1996;334(5):296-301.2. Benza RL, Miller DP, Barst RJ, Badesch DB,Frost AE, McGoon MD. An evaluation oflong-term survival from time of diagnosis in pul-monary arterial hypertension from the REVEALRegistry. Chest. 2012;142(2):448-456.3. Chin KM, Kim NH, Rubin LJ. The rightventricle in pulmonary hypertension. Coron ArteryDis. 2005;16(1):13-18.4. Stacher E, Graham BB, Hunt JM, et al.Modern age pathology of pulmonary arterial hyper-tension. Am J Respir Crit Care Med. 2012;186(3):261-272.5. Rich S, Pogoriler J, Husain AN, Toth PT,Gomberg-Maitland M, Archer SL. Long-termeffects of epoprostenol on the pulmonary vascu-lature in idiopathic pulmonary arterialhypertension. Chest. 2010;138(5):1234-1239.6. Pullamsetti SS, Schermuly R, Ghofrani A,Weissmann N, Grimminger F, Seeger W. Noveland emerging therapies for pulmonary hyper-tension. Am J Respir Crit Care Med. 2014;189(4):394-400.7. Paulin R, Michelakis ED. The metabolictheory of pulmonary arterial hypertension. Circ Res.2014;115(1):148-164.8. Tian W, Jiang X, Tamosiuniene R, et al.Blocking macrophage leukotriene b4 preventsendothelial injury and reverses pulmonary hyper-tension. Sci Transl Med. 2013;5(200):200ra117.9. Cowan KN, Heilbut A, Humpl T, Lam C,Ito S, Rabinovitch M. Complete reversal of fatalpulmonary hypertension in rats by a serine elastaseinhibitor. Nat Med. 2000;6(6):698-702.10. Bogaard HJ, Mizuno S, Hussaini AA, et al.Suppression of histone deacetylases worsens rightventricular dysfunction after pulmonary arterybanding in rats. Am J Respir Crit Care Med. 2011;183(10):1402-1410.11. Caruso P, Dempsie Y, Stevens HC, et al. Arole for miR-145 in pulmonary arterial hyperten-sion: evidence from mouse models and patientsamples. Circ Res. 2012;111(3):290-300.12. Courboulin A, Paulin R, Giguere NJ, et al.Role for miR-204 in human pulmonary arterialhypertension. J Exp Med. 2011;208(3):535-548.13. Kim GH, Ryan JJ, Marsboom G, Archer SL.Epigenetic mechanisms of pulmonary hypertension.Pulm Circ. 2011;1(3):347-356.14. Zhao L, Chen CN, Hajji N, et al. Histonedeacetylation inhibition in pulmonary hypertension:
therapeutic potential of valproic acid and suberoy-lanilide hydroxamic acid. Circulation. 2012;126(4):455-467.15. Davis BN, Hilyard AC, Lagna G, Hata A.SMAD proteins control DROSHA-mediatedmicroRNA maturation. Nature. 2008;454(7200):56-61.16. Brock M, Trenkmann M, Gay RE, et al.Interleukin-6 modulates the expression of the bonemorphogenic protein receptor type II through anovel STAT3-microRNA cluster 17/92 pathway.Circ Res. 2009;104(10):1184-1191.17. Tamosiuniene R, Tian W, Dhillon G, et al.Regulatory T cells limit vascular endothelial injuryand prevent pulmonary hypertension. Circ Res.2011;109(8):867-879.18. Casalena G, Daehn I, Bottinger E. Trans-forming growth factor-�, bioenergetics, andmitochondria in renal disease. Semin Nephrol. 2012;32(3):295-303.19. Austin ED, Cogan JD, West JD, et al.Alterations in oestrogen metabolism: implicationsfor higher penetrance of familial pulmonary arterialhypertension in females. Eur Respir J. 2009;34(5):1093-1099.20. Hamid R, Cogan JD, Hedges LK, et al. Pen-etrance of pulmonary arterial hypertension ismodulated by the expression of normal BMPR2allele. Hum Mutat. 2009;30(4):649-654.21. Austin ED, Loyd JE. The genetics of pul-monary arterial hypertension. Circ Res. 2014;115(1):189-202.22. Spiekerkoetter E, Tian X, Cai J, et al. FK506activates BMPR2, rescues endothelial dysfunction,and reverses pulmonary hypertension. J Clin Invest.2013;123(8):3600-3613.23. Deng Z, Morse JH, Slager SL, et al. Familialprimary pulmonary hypertension (gene PPH1) iscaused by mutations in the bone morphogeneticprotein receptor-II gene. Am J Hum Genet. 2000;67(3):737-744.24. Thomson JR, Machado RD, Pauciulo MW,et al. Sporadic primary pulmonary hypertension isassociated with germline mutations of the geneencoding BMPR-II, a receptor member of theTGF-beta family. J Med Genet. 2000;37(10):741-745.25. Atkinson C, Stewart S, Upton PD, et al.Primary pulmonary hypertension is associated withreduced pulmonary vascular expression of type IIbone morphogenetic protein receptor. Circulation.2002;105(14):1672-1678.26. Caldwell RL, Gadipatti R, Lane KB,Shepherd VL. HIV-1 TAT represses transcriptionof the bone morphogenic protein receptor-2 inU937 monocytic cells. J Leukoc Biol. 2006;79(1):192-201.27. Sehgal PB, Mukhopadhyay S. Dysfunctionalintracellular trafficking in the pathobiology of pul-monary arterial hypertension. Am J Respir Cell MolBiol. 2007;37(1):31-37.28. George MP, Brower A, Kling H, et al. Pul-monary vascular lesions are common in SIV- andSHIV-env-infected macaques. AIDS Res Hum Ret-roviruses. 2011;27(2):103-111.29. Dalvi P, O’Brien-Ladner A, Dhillon NK.Downregulation of bone morphogenetic proteinreceptor axis during HIV-1 and cocaine-mediated
132 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

pulmonary smooth muscle hyperplasia: implicationsfor HIV-related pulmonary arterial hypertension.Arterioscler Thrombosis Vasc Biol. 2013;33(11):2585-2595.30. West J, Austin E, Fessel JP, Loyd J, HamidR. Rescuing the BMPR2 signaling axis in pul-monary arterial hypertension. Drug Discov Today.2014;19(8):1241-1245.31. Mayeur C, Leyton PA, Kolodziej SA, Yu B,Bloch KD. BMP type II receptors have redundantroles in the regulation of hepatic hepcidin geneexpression and iron metabolism. Blood. 2014;124(13):2116-2123.32. Brunner NW, Skhiri M, Fortenko O, et al.Impact of insulin resistance on ventricular functionin pulmonary arterial hypertension. J Heart LungTransplant. 2014;33(7):721-726.33. Zamanian RT, Hansmann G, Snook S, et al.Insulin resistance in pulmonary arterial hyper-tension. Eur Respir J. 2009;33(2):318-324.34. Hemnes AR, Brittain EL, Trammell AW,et al. Evidence for right ventricular lipotoxicity inheritable pulmonary arterial hypertension. Am JRespir Crit Care Med. 2014;189(3):325-334.
35. Fessel JP, Hamid R, Wittmann BM, et al.Metabolomic analysis of bone morphogeneticprotein receptor type 2 mutations in human pul-monary endothelium reveals widespread metabolicreprogramming. Pulm Circ. 2012;2(2):201-213.36. Fessel JP, Flynn CR, Robinson LJ, et al.Hyperoxia synergizes with mutant bone morpho-genic protein receptor 2 to cause metabolic stress,oxidant injury, and pulmonary hypertension. Am JRespir Cell Mol Biol. 2013;49(5):778-787.37. Nickel NP, Kaschwich M, Diebold I, Li C,Spiekerkoetter EF, Rabinovitch M. The humanneutrophil inhibitor elafin interacts with caveolin-1to facilitate BMPR-2 signaling and endothelialhomeostatis associated with reversal of experi-mental pulmonary hypertension. Am J Respir CritCare Med. 2014;189:A3638.38. Drake KM, Zygmunt D, Mavrakis L, et al.Altered MicroRNA processing in heritable pul-monary arterial hypertension: an important role forSmad-8. Am J Respir Crit Care Med. 2011;184(12):1400-1408.39. Yamaguchi T, Kurisaki A, Yamakawa N,Minakuchi K, Sugino H. FKBP12 functions as an
adaptor of the Smad7-Smurf1 complex on activintype I receptor. J Mol Endocrinol. 2006;36(3):569-579.40. Abe K, Toba M, Alzoubi A, et al. Formationof plexiform lesions in experimental severe pul-monary arterial hypertension. Circulation. 2010;121(25):2747-2754.41. Motomura H, Matsushita I, Seki E, MineH, Kimura T. Inhibitory effect of tacrolimus onprogression of joint damage in patients with rheu-matoid arthritis. Int J Rheum Dis. 2013 Nov 20. Inpress.42. Albinana V, Sanz-Rodriguez F, Recio-Poveda L, Bernabeu C, Botella LM.Immunosuppressor FK506 increases endoglin andactivin receptor-like kinase 1 expression and modu-lates transforming growth factor-�1 signaling inendothelial cells. Mol Pharmacol. 2011;79(5):833-843.43. Bonnet S, Rochefort G, Sutendra G, et al.The nuclear factor of activated T cells in pul-monary arterial hypertension can be therapeuticallytargeted. Proc Natl Acad Sci U S A. 2007;104(27):11418-11423.
133Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

Nitric Oxide Therapeutics in Pulmonary Vascular Disease
Marc A. Simon, MD, MSAssistant Professor of Medicine,
Bioengineering, and ClinicalTranslational Science
Division of Cardiology, Department ofMedicine
University of PittsburghHeart & Vascular Institute, University of
Pittsburgh Medical CenterPittsburgh, PA
Clinical trials of inhaled nitrite to treat pulmonary arterial hypertension (PAH) areongoing. The pathogenesis of PAH involves smooth muscle hypertrophy as a resultof endothelial dysfunction and/or chronic vasoconstriction. Nitric oxide (NO) is apotent vasodilator and a primary therapeutic pathway for PAH. This review willaddress some of the emerging PAH treatment strategies utilizing the NO pathway.
The pathogenesis of pulmonary arterialhypertension (PAH) involves smoothmuscle hypertrophy as a result of endo-thelial dysfunction and/or chronicvasoconstriction. Progressive vesselremodeling occurs with intimal andadventitial proliferation.1 Nitric oxide(NO) is a potent vasodilator and aprimary therapeutic pathway for PAH.2
Flow through the vessel produces shearstress on the endothelium, activatingnitric oxide synthase (NOS), which con-verts L-arginine to L-citrulline and NO.NO then diffuses into the vascularsmooth muscle cells to activate solubleguanylyl cyclase, which convertsguanosine triphosphate (GTP) to cyclicguanosine monophosphate (cGMP),mediating vasodilation via increasedactivity of calcium-sensitive K� channels(BKCa).
3 This inhibits voltage-gated,L-type Ca2� channels, with subsequentdecreased intracellular Ca2�, resulting invasorelaxation (Figure 1).4
NO PATHWAY THERAPEUTICTARGETS FOR PAHThere is therapeutic opportunity at eachstep along the NO pathway (Figure 2).Working through the pathway, L-arginine can be given to load theconversion to L-citrulline and NO, NOcan be given directly or as nitrite, solubleguanylate cyclase can be directly stimu-lated by riociguat, phosphodiesterasetype 5 can be inhibited by sildenafil or
tadalafil to increase cGMP, and calciumchannels can be directly blocked bycalcium channel inhibitors.
Administration of L-arginine has beenshown in very small studies to reducemean pulmonary artery pressure and pul-monary vascular resistance.5,6 This hasbeen associated with increased levels ofL-citrulline, indicating production ofNO. However, there has not beenenough evidence to include it in themost recent guidelines.7,8
NO can be given directly via inha-lation. It is a mainstay of the acutevasodilator challenge when invasivelymeasuring hemodynamics. Because of itsextremely short duration of action, NOmust be given continuously for thera-peutic benefit. This, as well as cost, haslimited therapeutic administration ofinhaled NO to short courses in theintensive-care setting, where acutereduction of pulmonary pressures maybenefit pulmonary hypertension (PH),acute respiratory distress syndrome, pul-monary embolus, and perioperative rightventricular (RV) failure.9-12 Unfortu-nately, inhaled NO has shown noimprovement in mortality.13,14
The soluble guanylate cyclase stimu-lator riociguat has recently shown benefitin both PAH and chronic thromboem-bolic PH (CTEPH).15,16 Significantimprovements were seen in multipleendpoints including hemodynamics (pul-monary vascular resistance, mean
pulmonary arterial pressure, and cardiacoutput), functional class, quality of life,and clinical events (hospitalizations dueto PH, start of new treatment for PH,decrease in 6-minute walk distance[6MWD] due to PH, worsening offunctional class due to PH, death; seenonly for PAH, not CTEPH, althoughthere were few numbers of events).
The phosphodiesterase type 5 inhib-itors, sildenafil and tadalafil, aremainstays of therapy for PAH, withimprovements seen in hemodynamics(pulmonary vascular resistance, meanpulmonary arterial pressure, and cardiacoutput), functional class, 6MWD, andremarkable survival results.17-20 Beyondthe effects on the pulmonary circulation,sildenafil has been reported to improveRV function,21-24 which is now felt tobe an important goal of PAH treatmentdue to the implications of RV failure onmorbidity and mortality.25-29
Calcium channel blockers were amongthe first medications used to treat PAH.Nifedipine, diltiazem, and amlodipinehave been used. There are several limita-tions to calcium channel blockers.Positive clinical response to therapyrequires high doses that are difficult toachieve, and lack of durable treatmentresponse limits the therapeutic benefit ofcalcium channel blockers.30,31
LIMITATIONS TO NOS-DEPENDENT NO SIGNALINGThere are several limitations to NOS-dependent NO signaling. First, activity islimited by the short half-life of NO inblood (�2 milliseconds because NO is
Key Words—hypoxia, nitric oxide, nitrite, vasodilation, 6-minute walk distanceCorrespondence: [email protected]: Dr Simon has no relevant personal financial relationship to disclose.
134 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014
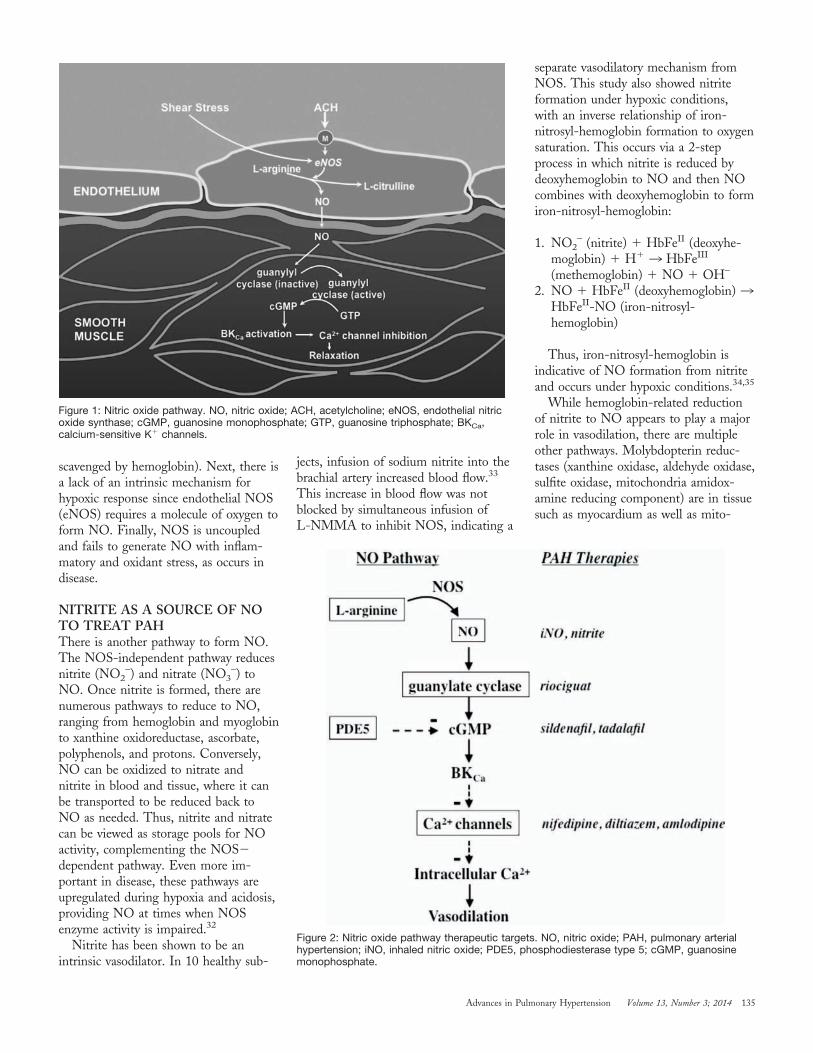
scavenged by hemoglobin). Next, there isa lack of an intrinsic mechanism forhypoxic response since endothelial NOS(eNOS) requires a molecule of oxygen toform NO. Finally, NOS is uncoupledand fails to generate NO with inflam-matory and oxidant stress, as occurs indisease.
NITRITE AS A SOURCE OF NOTO TREAT PAHThere is another pathway to form NO.The NOS-independent pathway reducesnitrite (NO2
–) and nitrate (NO3–) to
NO. Once nitrite is formed, there arenumerous pathways to reduce to NO,ranging from hemoglobin and myoglobinto xanthine oxidoreductase, ascorbate,polyphenols, and protons. Conversely,NO can be oxidized to nitrate andnitrite in blood and tissue, where it canbe transported to be reduced back toNO as needed. Thus, nitrite and nitratecan be viewed as storage pools for NOactivity, complementing the NOS�dependent pathway. Even more im-portant in disease, these pathways areupregulated during hypoxia and acidosis,providing NO at times when NOSenzyme activity is impaired.32
Nitrite has been shown to be anintrinsic vasodilator. In 10 healthy sub-
jects, infusion of sodium nitrite into thebrachial artery increased blood flow.33
This increase in blood flow was notblocked by simultaneous infusion ofL-NMMA to inhibit NOS, indicating a
separate vasodilatory mechanism fromNOS. This study also showed nitriteformation under hypoxic conditions,with an inverse relationship of iron-nitrosyl-hemoglobin formation to oxygensaturation. This occurs via a 2-stepprocess in which nitrite is reduced bydeoxyhemoglobin to NO and then NOcombines with deoxyhemoglobin to formiron-nitrosyl-hemoglobin:
1. NO2– (nitrite) � HbFeII (deoxyhe-
moglobin) � H� 3 HbFeIII
(methemoglobin) � NO � OH–
2. NO � HbFeII (deoxyhemoglobin) 3HbFeII-NO (iron-nitrosyl-hemoglobin)
Thus, iron-nitrosyl-hemoglobin isindicative of NO formation from nitriteand occurs under hypoxic conditions.34,35
While hemoglobin-related reductionof nitrite to NO appears to play a majorrole in vasodilation, there are multipleother pathways. Molybdopterin reduc-tases (xanthine oxidase, aldehyde oxidase,sulfite oxidase, mitochondria amidox-amine reducing component) are in tissuesuch as myocardium as well as mito-
Figure 2: Nitric oxide pathway therapeutic targets. NO, nitric oxide; PAH, pulmonary arterialhypertension; iNO, inhaled nitric oxide; PDE5, phosphodiesterase type 5; cGMP, guanosinemonophosphate.
Figure 1: Nitric oxide pathway. NO, nitric oxide; ACH, acetylcholine; eNOS, endothelial nitricoxide synthase; cGMP, guanosine monophosphate; GTP, guanosine triphosphate; BKCa,calcium-sensitive K� channels.
135Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

chondria. Nitrite anhydrases (ferrichemoglobin, nitrophorin, carbonic anhy-drase) can stabilize reactions effectively,allowing for NO transport.
In terms of treatment of PAH, nitritehas been shown in preclinical models toameliorate hypoxia-induced pulmonaryvasoconstriction and prevent RV hyper-trophy.36,37 Inhaled nitrite is currentlyunder development for the treatment ofPAH, with data to date showing safetyand initial efficacy trials underway. Therehas been no significant methemoglo-binemia by 1- and 12-month rat andcanine toxicology studies, a concernraised by the chemistry shown above,except at very high doses. A repeat-doseescalation Phase 1A study has beencompleted in normal volunteers showingsafety up to 90 mg (dose placed into themedication chamber) on backgroundsildenafil in normal volunteers and 11PAH patients. A Phase 2 proof ofconcept international trial of chronicadministration of inhaled nitrite 4 timesper day was closed earlier this year forfinancial reasons, but prior to this, 29PAH patients were treated for up to 354days (information courtesy of AiresPharmaceuticals). A Phase 2 study of theacute effects of inhaled nitrite on PHpatients (both Group 1 and Group 3) isin progress at our institution in whichthere have been no adverse events, andpreliminary results suggest significantreduction in pulmonary vascular resis-tance to a similar degree as inhaled NO,a modest but significant decrease in sys-temic vascular resistance, a significantdecrease in right atrial pressure, and anincrease in RV contractility index.
In summary, clinical trials of inhalednitrite to treat PAH are ongoing, withexciting early results that, if confirmed infuture larger trials, may broadentreatment strategies utilizing the NOpathway.
References1. Gaine S. Pulmonary hypertension. JAMA.2000;284(24):3160-3168.2. Humbert M, Sitbon O, Simonneau G.Treatment of pulmonary arterial hypertension.N Engl J Med. 2004;351(14):1425-1436.3. Archer SL, Huang JM, Hampl V, Nelson DP,Shultz PJ, Weir EK. Nitric oxide and cGMP causevasorelaxation by activation of a charybdotoxin-sensitive K channel by cGMP-dependent protein
kinase. Proc Natl Acad Sci U S A. 1994;91(16):7583-7587.4. Michelakis ED, Tymchak W, Noga M, et al.Long-term treatment with oral sildenafil is safeand improves functional capacity and hemody-namics in patients with pulmonary arterialhypertension. Circulation. 2003;108(17):2066-2069.5. Mehta S, Stewart DJ, Langleben D, Levy RD.Short-term pulmonary vasodilation with L-argininein pulmonary hypertension. Circulation. 1995;92(6):1539-1545.6. Nagaya N, Uematsu M, Oya H, et al.Short-term oral administration of L-arginineimproves hemodynamics and exercise capacity inpatients with precapillary pulmonary hypertension.Am J Respir Crit Care Med. 2001;163(4):887-891.7. Galie N, Hoeper MM, Humbert M, et al;ESC Committee for Practice Guidelines (CPG).Guidelines for the diagnosis and treatment of pul-monary hypertension: the Task Force for theDiagnosis and Treatment of Pulmonary Hyper-tension of the European Society of Cardiology(ESC) and the European Respiratory Society(ERS), endorsed by the International Society ofHeart and Lung Transplantation (ISHLT). EurHeart J. 2009;30(20):2493-2537.8. McLaughlin VV, Archer SL, Badesch DB, etal; American College of Cardiology FoundationTask Force on Expert Consensus Documents;American Heart Association; American College ofChest Physicians; American Thoracic Society, Inc.;and Pulmonary Hypertension Association.ACCF/AHA 2009 expert consensus document onpulmonary hypertension a report of the AmericanCollege of Cardiology Foundation Task Force onExpert Consensus Documents and the AmericanHeart Association developed in collaboration withthe American College of Chest Physicians;American Thoracic Society, Inc.; and the Pul-monary Hypertension Association. J Am CollCardiol. 2009;53(17):1573-1619.9. Pepke-Zaba J, Higenbottam TW, Dinh-XuanAT, Stone D, Wallwork J. Inhaled nitric oxide asa cause of selective pulmonary vasodilatation inpulmonary hypertension. Lancet. 1991;338(8776):1173-1174.10. Rossaint R, Slama K, Steudel W, et al.Effects of inhaled nitric oxide on right ventricularfunction in severe acute respiratory distress syn-drome. Intensive Care Med. 1995;21(3):197-203.11. Summerfield DT, Desai H, Levitov A,Grooms DA, Marik PE. Inhaled nitric oxide assalvage therapy in massive pulmonary embolism: acase series. Respir Care. 2012;57(3):444-448.12. Solina A, Papp D, Ginsberg S, et al. A com-parison of inhaled nitric oxide and milrinone forthe treatment of pulmonary hypertension in adultcardiac surgery patients. J Cardiothorac Vasc Anesth.2000;14(1):12-17.13. Griffiths MJ, Evans TW. Inhaled nitric oxidetherapy in adults. N Engl J Med. 2005;353(25):2683-2695.14. Creagh-Brown BC, Griffiths MJ, EvansTW. Bench-to-bedside review: Inhaled nitric oxidetherapy in adults. Crit Care. 2009;13(3):221.15. Ghofrani HA, D’Armini AM, GrimmingerF, et al; CHEST-1 Study Group. Riociguat forthe treatment of chronic thromboembolic pul-
monary hypertension. N Engl J Med. 2013;369(4):319-329.16. Ghofrani HA, Galie N, Grimminger F, et al;PATENT-1 Study Group. Riociguat for thetreatment of pulmonary arterial hypertension.N Engl J Med. 2013;369(4):330-340.17. Barst RJ, Beghetti M, Pulido T, et al;STARTS-2 Investigators. STARTS-2: long-termsurvival with oral sildenafil monotherapy intreatment-naive pediatric pulmonary arterial hyper-tension. Circulation. 2014;129(19):1914-1923.18. Galie N, Brundage BH, Ghofrani HA, et al;Pulmonary Arterial Hypertension and Response toTadalafil (PHIRST) Study Group. Tadalafiltherapy for pulmonary arterial hypertension. Circu-lation. 2009;119(22):2894-2903.19. Galie N, Ghofrani HA, Torbicki A, et al;Sildenafil Use in Pulmonary Arterial Hypertension(SUPER) Study Group. Sildenafil citrate therapyfor pulmonary arterial hypertension. N Engl J Med.2005;353(20):2148-2157.20. Oudiz RJ, Brundage BH, Galie N, et al;PHIRST Study Group. Tadalafil for the treatmentof pulmonary arterial hypertension: a double-blind52-week uncontrolled extension study. J Am CollCardiol 2012;60(8):768-774.21. Nagendran J, Archer SL, Soliman D, et al.Phosphodiesterase type 5 is highly expressed in thehypertrophied human right ventricle, and acuteinhibition of phosphodiesterase type 5 improvescontractility. Circulation. 2007;116(3):238-248.22. Andersen A, Nielsen JM, Rasalingam S,Sloth E, Nielsen-Kudsk JE. Acute effects of silde-nafil and dobutamine in the hypertrophic andfailing right heart in vivo. Pulm Circ. 2013;3(3):599-610.23. Xie YP, Chen B, Sanders P, et al. Sildenafilprevents and reverses transverse-tubule remodelingand Ca(2�) handling dysfunction in right ventriclefailure induced by pulmonary artery hypertension.Hypertension. 2012;59(2):355-362.24. Borgdorff MA, Bartelds B, Dickinson MG,et al. Sildenafil enhances systolic adaptation, butdoes not prevent diastolic dysfunction, in thepressure-loaded right ventricle. Eur J Heart Fail.2012;14(9):1067-1074.25. McLaughlin VV, Gaine SP, Howard LS, etal. Treatment goals of pulmonary hypertension.J Am Coll Cardiol. 2013;62(25 Suppl):D73–D81.26. Vonk-Noordegraaf A, Haddad F, Chin KM,et al. Right heart adaptation to pulmonary arterialhypertension: physiology and pathobiology. J AmColl Cardiol. 2013;62(25 Suppl):D22–D33.27. D’Alonzo GE, Barst RJ, Ayres SM, et al.Survival in patients with primary pulmonary hyper-tension. Results from a national prospectiveregistry. Ann Intern Med. 1991;115(5):343-349.28. Benza RL, Miller DP, Gomberg-MaitlandM, et al. Predicting survival in pulmonary arterialhypertension: insights from the Registry toEvaluate Early and Long-Term Pulmonary ArterialHypertension Disease Management (REVEAL).Circulation. 2010;122(2):164-172.29. Ghio S, Klersy C, Magrini G, et al. Prog-nostic relevance of the echocardiographicassessment of right ventricular function in patientswith idiopathic pulmonary arterial hypertension.Int J Cardiol. 2010;140(3):272-278.
136 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

30. Rich S, Kaufmann E, Levy PS. The effect ofhigh doses of calcium-channel blockers on survivalin primary pulmonary hypertension. N Engl J Med.1992;327(2):76-81.31. Sitbon O, Humbert M, Jaıs X, et al.Long-term response to calcium channel blockers inidiopathic pulmonary arterial hypertension. Circu-lation. 2005;111(23):3105-3111.32. Lundberg JO, Weitzberg E, Gladwin MT.The nitrate-nitrite-nitric oxide pathway in physi-ology and therapeutics. Nat Rev Drug Discov.
2008;7(2):156-167.33. Cosby K, Partovi KS, Crawford JH, et al.Nitrite reduction to nitric oxide by deoxyhemo-globin vasodilates the human circulation. Nat Med.2003;9(12):1498-1505.34. Brooks J. The action of nitrite on haemo-globin in the absence of oxygen. Proc R Soc Med.1937;123:368-382.35. Doyle MP, Pickering RA, DeWeert TM,Hoekstra JW, Pater D. Kinetics and mechanism ofthe oxidation of human deoxyhemoglobin by
nitrites. J Biol Chem. 1981;256(23):12393-12398.36. Hunter CJ, Dejam A, Blood AB, et al.Inhaled nebulized nitrite is a hypoxia-sensitiveNO-dependent selective pulmonary vasodilator.Nat Med. 2004;10(10):1122-1127.37. Zuckerbraun BS, Shiva S, Ifedigbo E, et al.Nitrite potently inhibits hypoxic and inflammatorypulmonary arterial hypertension and smoothmuscle proliferation via xanthine oxidoreductase-dependent nitric oxide generation. Circulation.2010;121(1):98-109.
137Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

ORAL ABSTRACT PRESENTATIONS
Conference Abstracts
A record number of abstracts were submitted during PHA’s 2014 International Con-ference and Scientific Sessions in June. The winning abstracts were presented as oralabstracts during the scientific sessions and are included in this issue of Advances.
Non-Biased Proteomics Discovery ofPulmonary Artery Hypertension Bio-markers Periostin and MatrixMetalloproteinase 9Nies MK, Yang J, Fu Z, Everett ADJohns Hopkins University, Baltimore,Maryland, USABackground: Identification of a pul-monary hypertension (PH) biomarkerwould aid in risk stratification, non-invasive monitoring of therapeuticefficacy and even as a potential thera-peutic target. Our aim was to identifyPH biomarkers via proteomic analysis ofPH and control lung, followed by com-plementary techniques to demonstratealteration in PH lung and plasma.
Methods: Homogenized lung extractfrom the Pulmonary HypertensionBreakout Initiative (PHBI) biorepositoryfrom end stage PH patients (idiopathicPAH�5, PAH-associated with con-genital heart disease�5, control� 5) wasanalyzed by non-biased, high resolutionmass spectrometry (Orbitrap Elite).Selection of lead biomarkers was by bio-logical feasibility and spectral countingwith �2 or �0.5 fold change betweenPH and control. Lung western blot,IHC and ELISA were performed onPHBI homogenized lung, paraffinembedded lung and plasma, respectively,from adult PAH patients and controls.Data was analyzed by one way ANOVAand Kruskal Wallis.
Results: 860 non-redundant lung pro-teins were identified (APAH� 620,IPAH� 688, control�688; figure 1); 38proteins were �2 fold up or �0.5 folddown in PH versus control lung.
Periostin (IPAH 7.5 fold, APAH 9.5fold) and matrix metalloproteinase 9(MMP9) (IPAH and APAH ��0.5fold) were identified as promising leadbiomarkers. Western blot revealed ele-vated periostin while MMP9 decreasedin PH versus control lung (figure 2a and2b). Periostin IHC stained alveolarendothelial cells (figure 3). ELISA assayshowed increased periostin in PH versuscontrol plasma (n� 17, PH median9738 ng/mL, control median 1433ng/mL, p� 0.0502) (figure 4).
Conclusions: Periostin and MMP9have reciprocal expression in PH lung.Periostin is predominately endothelialexpressed, with circulating periostin apromising new PH biomarker. MMPsplay a significant role in PH patho-genesis. Future studies will include largersample sets, including pediatric patients,and evaluate additional potential PHbiomarkers generated from proteomiclung analysis.
Figure 1: Lung Proteins Figure 2A: Lung Western Blot Figure 2B: Lung Western Blot Densitomery
Figure 3: Periostin Immunohistochemistry Figure 4: Plasma Periostin: PH vs control
138 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

Resistin-like Molecule ProteinsPromote Pulmonary Vascular Endo-thelial Activation and Apoptosis: CrossTalk Between Vascular Endothelial andSmooth Muscle CellsYamaji-Kegan K,Johns RADepartment of Anesthesiology and CriticalCare Medicine, Johns Hopkins UniversitySchool of Medicine, Baltimore, Maryland,USABackground: Pulmonary hypertension(PH) is a devastating disease of the pul-monary vasculature characterized byenhanced inflammation, vasoconstriction,pulmonary artery smooth muscle cell(PASMC) proliferation, and remodelingof small pulmonary arteries. Injury toendothelium and consequent woundrepair cascades have been suggested totrigger pulmonary vascular remodeling inthis disease. The relationship betweeninjury to endothelium and disease patho-genesis in this disorder remains poorlyunderstood. We and others have shownthat in rodents, resistin-like molecule �(RELM�; also known as HIMF orFIZZ1) plays a critical role in the patho-genesis of lung inflammation and thedevelopment of PH. In this study, wedissected the mechanism by whichRELM�/HIMF and its humanhomolog resistin (hResistin) induce pul-monary endothelial cell (EC) activationand apoptosis. We also examined theeffect of conditioned media fromRELM�/HIMF- or hResistin-treatedECs on PASMC proliferation.
Methods: We stimulated primary pul-monary microvascular EC from mouseor human with RELM�/HIMF orhResistin, respectively, and examinedwhether these RELM proteins induceapoptosis by TUNEL assay and ana-lyzing apoptosis-related signaling. Wealso examined EC activation by quanti-fying the expression EC exocytosiscomponents in response to hResistin.Lastly, we determined the effect of ECconditioned medium on PASMC prolif-eration and bone marrow derived(BMD) cell recruitment in response toRELM proteins.
Results: Both RELM�/HIMF andhResistin caused apoptosis in PMVEC.RELM �/HIMF-induced EC apoptosisis mediated by activation of p53 and
caspase-3. hResistin treatment increasedthe expression of von Willebrand Factorand Angiopoietin-2 from PMVEC.These molecules are known as the ECexocytosis components that are releasedfrom EC in response to the stress/injury. EC conditioned medium treatedwith RELM proteins significantlyenhanced PASMC proliferation andBMD cell recruitment as compared tonon-treated EC conditioned controlmedium.
Conclusions: Our results suggest thatRELM�/HIMF and hResistin induceEC activation and apoptosis, and theseapoptotic EC lead the production ofgrowth factors that stimulate PASMCproliferation. Thus, an EC apoptosis-SMC growth loop could result in theprogression of pulmonary vascularremodeling in PH. The more detailedmechanisms by which PASMC growthfactors and chemokines are regulated inpulmonary EC in response to RELMproteins is under investigation.
Right Ventriculo-Arterial Coupling inPatients with Pulmonary ArterialHypertension Undergoing Rapid DoseEscalation of TreprostinilRischard F1, Champion HC2,Vanderpool R2, Simon M2, Jenkins I3,Hansen L1, Knoper S1, Waxman A4
1Department of Pulmonary and CriticalCare Medicine, University of Arizona,Tucson, Arizona, USA; 2Pulmonary Vas-cular Disease Center, University ofPittsburgh, Pittsburgh, Pennsylvania, USA;3BIO5 Institute, University of Arizona,Tucson, Arizona, USA; 4Pulmonary Vas-cular Disease Program, Brigham andWomen’s Hospital, Boston, Massachusetts,USABackground: The mechanism of vaso-active therapy in pulmonary arterialhypertension (PAH) on ventriculo-arterial interaction is not wellestablished. Therefore, we prospectivelyinvestigated the effect of treprostinil onpulmonary vascular elastance (Ea), rightventricular (RV) systolic (Ees) and cou-pling in PAH patients.
Methods and Results: Single-beat RVpressure-volume analysis was performedin 9 functional class IV PAH patientsbefore and after rapid inpatient doseescalation, and after gradual outpatient
dose increase of treprostinil. Data arepresented as mean�SEM. Treprostinildose was 12.8�0.46 ng/kg/min at dis-charge and 44.2�4.34 ng/kg/min by3 months (mo.). Treprostinil was mostconsistently associated with a decreasein Ea (2.44�0.26 mmHg/ml baseline,1.95�0.49 mmHg/ml discharge, and1.38�0.28 mmHg/ml 3 mo. Ees wasdecreased slightly at discharge(1.62�0.35 mmHg/ml baseline vs.1.49�0.3 mmHg/ml) and then reducedfurther by 3 mo. (0.85�0.18mmHg/ml). The decrease in Ea, com-pared to Ees, was more pronounced atdischarge, but relatively the same at3 mo. leading to a coupling ratio of0.68�0.15 baseline, 0.98�0.23 dis-charge, and 0.68�0.16 at 3 mo. Mostpatients demonstrate similar changes inEa and Ees (both direction and mag-nitude) at discharge and 3 mo. AlthoughEes decreased at 3 mo., there was906�530 mmHg*ml stroke work reservewith exercise and a 139�45 M increasein 6 minute walk distance vs. discharge.Both RV stroke work (RVSW) increasedand work efficiency maintained at dis-charge and 3 mo. RV end-diastolicvolumes (RV EDV) however re-mained elevated 241�28.2 ml baseline,225�30.4 ml discharge, and 218�24.5 ml 3 mo.
Conclusions: Treprostinil primarilyexerts its effects by lowering RVafterload (Ea) both acutely and at 3 mo.This effect governs the improvement inRV systolic pump failure and contractilereserve. Increases in RVSW are likelyrelated to significant lowering ofafterload and persistently high baselinepreload dependent (heterometric) auto-regulation.
Trends in Pediatric Inpatient SildenafilUse in the United States, 2004-2013Yung D1, Tejtel KS2
1University of Washington, Bellevue,Washington, USA; 2Baylor University,Waco, Texas, USABackground: Since sildenafil becamecommercially available in 1998 andapproved for adult pulmonary arterialhypertension (PAH) in 2005, reports ofpediatric sildenafil use have increased.However, a black-box FDA warning was
139Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

given in the summer of 2012 based onresults of a placebo-controlled trial inchildren ages 1-17. We sought to under-stand sildenafil use in hospitalizedchildren over time.
Methods: The Pediatric Health Infor-mation System (PHIS) database wasqueried between January 2004 and June2013 for sildenafil use in hospitalizedpatients with demographic, primary
diagnosis and clinical data (Table 1,Figure 1).
Results: There were 23,164 hospi-talized children who received at least onedose of sildenafil.
Conclusion: After the FDA warningagainst sildenafil use in children in 2012there has been decrease in the use ofsildenafil use in all age groups and anassociated decrease in mortality.
Figure 1: Number of patients with sildenafil use by age and year, plus mortality. The first usewas reported in 2004.
Table 1. Clinical Data
Number(%)
Primary Diagnosis
Congenital Heart Disease 5589 (24)
Pulmonary hypertension 1624 (7)
Pneumonia (bacterial or viral) 1629 (7)
Prematurity or RDS 888 (4)
Gender, Male 12133 (52)
Length of stay 7 days or less 9816 (42)
Mechanical ventilation 13122 (57)
ECMO 1431 (6)
Readmission within one year 9748 (55)
140 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

PULMONARY HYPERTENSION ROUNDTABLE
Reflections on the Scientific Sessions
Following PHA’s International PH Conference and Scientific Sessions in Indianapolis on June 20-22, 2014, a group of cliniciansgathered by phone to discuss the highlights of the meeting they would take to their practice. Guest editor Anna R. Hemnes, MD, AssistantProfessor of Medicine and Assistant Director, Pulmonary Vascular Center at Vanderbilt University and Chair of the Scientific Sessions,facilitated the call. Discussants were Raymond Benza, MD, Cardiovascular Institute, Allegheny General Hospital, Pittsburgh; KarenFagan, MD, University of South Alabama, Mobile; Steven M. Kawut, MD, MS, Penn Cardiovascular Institute, University of Pennsyl-vania School of Medicine, Philadelphia; Jeffrey S. Sager, MD, MSc, Santa Barbara, CA; and Glenna Traiger, RN, MS, CNS-BC,Pulmonary Hypertension Program, UCLA.
Dr Hemnes: My goal today was basi-cally to talk about the scientific sessionsand the conference and what everybody’sthoughts were. I think there were 1,580registrations for the conference, whichwas tremendously successful. My firstquestion for the group, and I thinkeverybody could answer this, was that atthe end of every CME evaluation thatwe fill out, the question that gets askedis, what are you going to change aboutyour practice, and what’s your take homemessage from this meeting? While Ithink very little from the scientific ses-sions is really ready to take home to ourpractice, but let’s say what from the con-ference made the greatest impression forus. What was the most prominent thingyou took home from the conference?
Dr Benza: To me, the conference againwas a wonderful opportunity to share inthe collegiality of the group, which weknow is fairly unique to the pulmonaryhypertension community. You know, theability to see friends and colleagues andinteract with them face-to-face in asupportive and casual atmosphere sur-rounded by the patients we treat is atruly unique experience. And also theability to pass on practical information tolarge numbers of patients is one of themost valuable experiences I’ve had as apracticing clinician. Every time Icome back from that meeting, I feelre-oriented in why I do what I do andfeel very charged at the end of the day.That renewal, energy, and enthusiasmnot only help me take care of mypatients better, but also allow me toconduct my research with more vigor.
Dr Kawut: I agree with Ray. I cameback from the conference with a sense ofthe incredible hope that patients feel inthe current day. The pace of approvedtherapies seems to increase every year. Sowhile a mere 10, 15 years ago, maybethere were 1 or 2 therapies, now there’s,what, 12 or 13? I lose count. That senseof hope from the patients invigorates mewhen I go back to my own practice.
Dr Sager: I echo many of the senti-ments that Steve and Ray expressed. Inaddition, some of the most fascinatingdevelopments that I have noticed overthe past several years attending the PHAconference are the increased knowledgebase that the patients have developed.This is clearly evident by the breadthand depth of the questions posed to theexpert panels, often stumping us. Thismotivates me upon my return from theconference to improve my understandingand knowledge of the details of newclinical trials and research in the fieldwith the ultimate hope of finding a curefor this devastating disease.
Ms Traiger: To tag onto what Dr Sagerjust said, I was really impressed with thepatient-led sessions that were offered.The patients are really stepping up andtaking an active role in the conferencenow. And I think they’re really doing agreat job in educating their peers on pul-monary hypertension.
Dr Benza: There certainly is a level ofsophistication that our patients have thatI think is fairly unique to this group ofpeople. For example, during the con-
ference I passed out some surveys to getpatient opinions about some risk stratifi-cation algorithms I’ve been working on.Not only did I get 100% of the surveysreturned, unusual in itself, but inaddition to having my questionsanswered, I received fantastic suggestionsthat I didn’t even ask for. And so thatreally is a fairly good testament to thequality, enthusiasm and sophistication ofthe patients that we take care of.
Dr Hemnes: Thank you. Those are allreally great points and I couldn’t agreewith you all more. I was also reallyimpressed with the presentations thathappened during the scientific sessions atthe future of pulmonary hypertensionand how fast science is moving forwardin our understanding of this disease andhow that is going to translate in the nextdecades to improved patient care. Notonly just in pulmonary arterial hyper-tension but also in pediatric pulmonaryhypertension and non-Group 1 pul-monary hypertension, which I thoughtwas very exciting. One of the things thatI thought was interesting that we wereunable to put in the scientific sessions,that I think some of the people on thiscall might be able to help us thinkabout, was the topic of new treatmentsand targets not in the pulmonary vascu-lature in pulmonary hypertension. Andessentially, all of the presenters weretalking about pulmonary vascular targetsin pulmonary hypertension, becausethat’s really where our science is rightnow, and especially in terms of thera-peutics. But I was thinking that maybe 5or 10 years from now a future scientific
141Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

session might be devoted to the rightventricle and treatment aimed at it inpulmonary hypertension. And I wonderif Steve or Ray, might you have anythoughts about what that conferencewould look like in the future?
Dr Kawut: Anna, that’s a timely point.Corey Ventetuelo is the first author of apaper from our group, just published inCirculation, which showed that changesin hemodynamics, which we all considerto be the cornerstone of the under-standing of this disease, actually explainvery little of the impact of our effectivetreatments on outcomes, at least in theshort term. So while we think ourcurrent treatments improve outcomebecause they decrease pulmonary vascularresistance or improve cardiac output(both measured at rest), that doesn’tseem to be the case. This really showshow little we know about how thesetreatments actually work. There may beother parameters and physiologicpathways, such as the ability of the RVto mount a response to exercise, theergoreflex, and peripheral vascular andmuscular responses. There is a well-known study of a long-term PAHsurvivor on IV epoprostenol, whichshowed dramatic pulmonary vasculardisease, but good right ventricular adap-tation. So I think while we think weknow how these drugs work (mainly byacting on the pulmonary vasculature),this may not be the case. And so 10years down the line, we may be targetingother parameters and other systems whichwe’re currently not, just as you say.
Dr Benza: Similar to what Steve wasmentioning, I think the most infor-mative conference is going to be onethat doesn’t isolate the pulmonary vascu-lature and/or the right ventriclecontextually, but rather reviews this asone unit. I truly believe that theknowledge gained in the next 5 yearswill be driving us in a direction wheretailored therapy will conjointly treat thepulmonary vasculature and the rightheart. So drugs and/or drug regimensthat not only reduce resistance, but alsoimprove intrinsic right ventricularactivity, and RV PA coupling is wherethe money is going to be. A conference
designed to look at all 3 of these param-eters together would be ideal as this isgoing to be the way we treat this diseasein the not-so-distant future. As Stevementioned, it’s just not what’s in thepulmonary vessels. It’s the connectionbetween the pulmonary vessels and theright heart and even the systemic skeletalmusculature that’s important.
Dr Hemnes: Thanks. I think those areimportant comments. And I do think,too, that there’s a wealth of literaturelooking at mechanistically how the rightheart fails that will translate into newtherapeutics for the right heart in thefuture, and even some of that’s bornefruit in clinical trials already, with trialsof beta-blockers that are now we’rebeginning to see data from, which areexciting and interesting and may showus a way forward in how to study thatbetter. And I agree with you, Ray, that Ithink linking the two—pulmonary vas-cular and right heart together—will bethe future. And clearly, the othermetrics, as well. Was there any sciencethat was presented at the meeting thatyou all felt was particularly promising orexciting to you?
Dr Sager: I was particularly intriguedwith the work that Dr EddaSpiekerkoetter is doing on the immuno-suppressant drug FK-506 (Tacrolimus)as it related to BMPR2 receptor sig-naling. This is a commonly used drug inthe transplant world and now may havean application in the field of pulmonaryarterial hypertension. Edda found in herexperimental lab that low-dose FK-506reverses established pulmonary hyper-tension in rats and mice. Improvedunderstanding of the BMP signalingpathway may lead to future drug devel-opment. It allows me to think differentlyabout this condition in terms of not justsimply finding a vasodilator, but some-thing that may be an immune-modulated condition. Thinking outsidethe box of the conventional 3 knowntargeted pathways is essential for us tomove forward in the field.
Dr Benza: As a transplant physician,knowing that these pathways intersectwith others, particularly with regard to
pulmonary artery remodeling, is reallyquite fascinating. This type of treatmentparadigm could extend to other immu-nosuppressant regimens, including drugslike sirolimus, which also has remodelingeffects on smooth muscle cells in vitro.So this “non-3 pathway thinking,”—akinto the TKI inhibitor story—is reallyinnovative and out of the box thinking.
Dr Hemnes: I agree. I thought that wasa really interesting new direction. And Iliked the idea, too, of trying to figureout which patients that those particularagents would be useful in. And I thinkdata like yours, Ray, from the REVEALregistry, will be helpful to figure outwhich are the highest risk patients thatmay benefit the most from a moreaggressive regimen. But also on amolecular level, trying to identifypatients who are likely to have, forinstance, BMPR2 suppression or moreprofound BMPR2 suppression than youraverage PH patient who may benefitfrom FK506 or some similar agent willbe useful. Have you ever thought, Ray,about applying REVEAL registry datato select patients for individual therapies?
Dr Benza: You know, we had thoughtabout that many times; but we thoughtthat those type of questions would bestbe answered in the form of clinical trialwork because sometimes you can extrap-olate too much from the databases,which might mislead you. So the answeris yes, we have thought about that andwe thought it was best not to actually dothat. And the interesting thing aboutthat, Anna, is that when you look at themedications in the context of how prog-nosis is altered by their use, it’s really inthe movement of the risk factors that wemonitor, not the actual drug type that’sthe most important thing. So, how adrug drives the change in a predictivefactor, like a 6-minute walk distance,WHO functional class, or a BNP level iswhat changes risk, not actually the drugitself, per se.
Dr Hemnes: Interesting, thanks. Well,one of the other topics that came up atthe scientific sessions was pediatric pul-monary hypertension, which is animportant feature of our conference with
142 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

the pediatric patients and families thatare there. It’s also an emerging area ofresearch and controversy. And I thoughtDunbar Ivy’s presentation on pediatricpulmonary hypertension and clinical trialdesigns in that group of patients wasfascinating, particularly highlighting thechallenges of sildenafil research in pedi-atric pulmonary hypertension. Didanyone have any thoughts on this par-ticular field or Dunbar’s presentationthat was enlightening?
Dr Benza: As someone who just treatsadult pulmonary hypertension, I lovelistening to talks about pediatric PHbecause, one, it allows me to recognizehow much more difficult it is to treatchildren with this disease than it isadults. And, secondly, how much morewe need to do in that particular field andhow it really lags behind the things thatwe do in the adult world. So I thinkthat’s what I really got an appreciationfrom listening to him speak.
Dr Hemnes: Yes, I had similarthoughts. He did such a nice job ofhighlighting the challenges of studying adrug and its efficacy in the pediatricpopulation, it really made me appreciateall the wonderful tools that we have withadults. And although there are clear lim-itations to a 6-minute walk, at least wedo have that, and that’s not even reallyat all useable in the pediatric population.He just did such a nice job of high-lighting the tremendous challenges thatphysicians and patients face in that pop-ulation.
Dr Kawut: Both for children and adults,the ultimate goal is a valid surrogateendpoint, whether it’s a blood test orsome other biomarker or imagingparameter, which will help you predictthe effect of the therapy on the ultimateoutcome. The only way to do that, ofcourse, is to include these potential sur-rogates in ongoing clinical trials. Everyclinical trial we execute without theinsertion of some investigational sur-rogate endpoint is really a lostopportunity that can never be regained.
Dr Fagan: I think one thing that hereally highlighted for me was the present
day limitations that they have on deter-mining efficacy. I was really stunned bythe FDA limitation on using hemody-namics in these studies, because, as he sowell pointed out, there’s so little else thatis something that can be applied acrossmultiple different pediatric situationsfrom infancy, toddlerhood, childhood,into early adolescence. The one thingthat I think most of us as adults wouldsay is, well, the hemodynamics are thethings that we can use, if nothing else, atleast to determine an efficacy profile ofsomething. They’re limited even by thatand I found that to be really, really sur-prising that the FDA has mandated thatthat not be used as an endpoint.
Dr Hemnes: Yeah, I couldn’t agreemore. He really brought out the chal-lenges. And it made me wonder about apath forward for pediatric pulmonaryhypertension and how best to do that.And obviously, as Ray mentioned, noneof us is a pediatric pulmonologist—or apediatric pulmonary hypertension spe-cialist. But I think of all the challengesthat we as adult physicians and scientistsstruggle with every day, their challengesare many times greater and veryimportant that we recognize movingforward.
Dr Kawut: Maybe the ideal endpoint isa patient (or parental) reported outcome.I don’t think we have any validatedquestionnaires for pediatric pulmonaryhypertension, but such an instrumentcould be noninvasive and clinicallymeaningful.
Dr Fagan: Yes, absolutely.
Dr Hemnes: I agree. And maybe also away forward for drug approval in thefuture, in the absence of the other sur-rogate markers that you mentioned. Ithink that’s also a kind of lead-in to mynext question. I personally really enjoyedthe session that Steve participated in onclinical trial design and the panel dis-cussion during the noon session. Someof the things that I thought were reallyinteresting about that included our col-league from the NIH who came andtalked about NIH funding, particularlyin the PVDOMICS grant that just
recently got reviewed and also in theNIH’s support for translational research,through translational program projectgrants and other mechanisms. I thoughtthat the discussion that Dr McLaughlinled, with Steve and Dr RohamZamanian, was really enlightening andopened the door for participation with alot of members in the audience. Whatdid you all think about the clinical trialdesign panel discussion? And did youhave any new thoughts that came out asa result of that discussion?
Dr Benza: You know, unfortunatelythat was during my flight crisis and Imissed that very engaging conversation.Although interestingly—.
Dr Kawut: If you missed it, how do youknow it was engaging?
Dr Benza: Well, I’m going to tell youthat right now (laughter) because that’sthe interesting part about it. It was soengaging that members of the audiencewho were there sent me video clips ofwhat I was missing as I was stranded inthe airport (laughter) via their smartphones. Now, that’s a waste of perfectlygood battery power. So that was quiteinteresting, but it did sound like it was avery worthwhile event to have witnessed.
Dr Fagan: I also kind of popped in it, alittle bit. But I think one of the thingsthat we need to think more broadlyabout is the patient outcome componentto the designing of clinical trials. We alltalk about that in terms of the thingswe’re going to use to determine whatmakes a drug effective. I think thatdiscussions that lead to defining effec-tiveness in a much more creative,patient-centered way are the things thatwill be important in any programs,either individual clinical trials, thePVDOMICS, you know., The othertranslational item to look at is what wasmentioned earlier—the patient-relatedoutcomes components to that. Ulti-mately, those are the most importantoutcomes, most of us would agree. Andfiguring out ways to incorporate them,not just time to clinical worsening, notjust these things that can be objectivelymeasured, but also the subjective compo-
143Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

nents in terms of the outcomes forpatients I think are important. I think allof us recognize that we need to be morecreative and more patient-focused inmeasuring the outcomes.
Dr Benza: Yes, Karen, that is reallyquite perceptive. And as I mentionedearlier, I had distributed these surveysduring the conference about patient pref-erences. It’s amazing how there is asignificant population of our patientswho feel they’re not engaged enough inthe decision-making with regard to theirtherapeutics and how the therapies makethem feel. I think that needs to be areally critical piece of how we judgewhat therapeutics to use, when to usethem, and should be kept in the fore-front of our minds when we make thesedecisions.
Dr Kawut: As I think both Ray andKaren have pointed out, this is a multi-dimensional disease. To say that if weimprove your PVR you’re going toautomatically feel better is overly reduc-tionist, right? This is a disease thatincorporates dyspnea, fatigue, anxiety,depression, weakness. People havesymptoms in complicated domains whichwe’re not particularly good at measuringor potentially even asking about. I thinkcapturing these other important patientdimensions will be critical to really getdrugs that really improve how patientsfeel, function, and survive.
Dr Sager: One of the aspects I enjoyedas part of the clinical trial design sectionis the issue of trial recruitment. PAHclinical trials traditionally include onlysmall numbers of participants due to therare nature of PAH. Hopefully with thenew accreditation process of the Pul-monary Hypertension Care Centers(PHCC) through the PHA, therequirement that comprehensive carecenters provide access to patients toenroll in clinical trials will increase thenumber and breadth of clinical trialsavailable to patients.
Ms Traiger: Also, these clinical trialsare going to become longer in the future.So I think a lot of us worry that we’regoing to run out of patients for trials,
because these are not going to be 12- or16-week trials anymore, potentially.There was also a discussion about sub-studies or tacking smaller studies ontolarger grants, so that we could studymultiple questions perhaps within onestudy. I think that’s where the quality oflife measurements can come in, as wellas more patient-centered outcomes.
Dr Hemnes: Yes, I thought those werereally important points that came out ofthat clinical trial design discussion. Oneof the things that I thought aboutmoving forward is applying all thosethings that we discussed there to non-Group 1 pulmonary hypertension that Ithink in the future will be a greater areaof research in clinical trials. And I thinkpatient-reported outcomes are probablygoing to be even more important in thatrelatively heterogeneous population withinthe other non-Group 1 PH groups. Theyalso may address some of the issues withlower numbers of patients that are inGroup 1 pulmonary hypertension. So Ithought those were quite relevant andfertile areas for future thoughts.
Dr Benza: I think that’s criticallyimportant because as we all recognize,WHO Group 1 is really a very, very tinypiece of the pie. WHO Group 2 and 3far exceed the number of people that wecurrently treat with PAH. And so theapplication of what we’ve learned inPAH to these broader populations, Ithink, would be very valuable to makesure we do it right the first time and getthe answers that we want up frontinstead of recreating the wheel when westart doing clinical trials in those areas.
Dr Kawut: One of the most importantthings about the conference and reallyone of the reasons I go to it is to seepeople living with pulmonary hyper-tension in a more normal setting than inthe physician’s office. It is too easy thatmy vision of a patient with pulmonaryhypertension can become someonesitting on an examining table or in thechair with me in front of the computer,trying to lamely type in a note. I thinkthe conference is a great way of drivinghome the point that people with pul-monary hypertension live full lives and
don’t let the disease define them. Seeingpeople from children to seniors at mealsor at parties having a good time isalways very helpful to me. The con-ference therefore plays an important rolein my relationships with my patients andin what drives me to do what I do.
Dr Fagan: It’s absolutely important. Wehave now for the last 2 times had someof our PhD graduate students come tothe conference just to see some of thepatients living with PAH who, for them,are much more abstract ideas. And thenthey come to conference and they have areally tangible idea of what a PH patientlooks like. It gives them a great deal ofenthusiasm as they go back to continuetheir work. It’s the graduate studentswho went this year, much like 2 yearsago, who came back and felt tremen-dously invigorated and refreshed toattack their projects in the lab with a lotmore meaning. So one of the things thatwe really enjoyed is that we’ve been ableto do that and to get these people whoare not going to have a clinical expe-rience with a professional and, to quoteone of them, he came back changed,that’s the only word he could use todescribe it; he felt changed.
Ms Traiger: I was in the sports barwhen the Team PHenomenal Hopecrossed the finish line. And it was reallya very moving experience for me, becausethe room was just jam packed withmostly patients and PHA staff. It wasreally palpable how much that eventmeant to those patients—that thisbicycle team went across the country basi-cally for them. I found that very moving.
Dr Sager: A remarkable aspect of thisyear’s conference that struck me that Ihad not experienced at previousconferences was the close attention andawareness of the international PHcommunity to our US-based PHA orga-nization. As most of you know, my rootsare from South Africa and the SouthAfrican Pulmonary Hypertension Asso-ciation delegation contacted me at theconference to help develop the PH pro-grams in South Africa. Up until only afew years ago there were no treatmentsavailable to patients in South Africa and
144 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

with the help and connections withPHA, they have steadily built a program.They base the development of their pro-grams off many of the protocols we havedeveloped here in the USA. Many coun-tries do not have access to the researchand the in-depth management or accessto the latest therapies that we take forgranted in the USA. This is humblingand makes one pause as we are very for-tunate to have access to many moresophisticated diagnostics and therapeuticoptions than other countries. The worldis watching us at these conferences andit was quite an eye-opener for me.
Dr Fagan: Along those lines, I actuallyattended some parts of the InternationalLeaders Summit, which was held theday before conference. I had a chance tospeak with the leaders of PHA organiza-tions across the world. And one of thethings that I really found quite inter-esting to our international colleagues isthat this close-knit relationship that weas physicians and researchers have withour patient community is actually notthe norm. In many of these countries,they have no or very, very limitedengagement with their professional com-munities. So hopefully, that’s one of the
things that the rest of the world iswatching for us and that we hopefullyare modeling the powerful impact thathaving physicians, researchers, and thepatient and caregiver communitiesinteract, how we’re much greater thanjust the sum of our parts when we dothat.
Dr Hemnes: I think that’s a wonderfulcomment and a really great place tostop, because I think we all aregreater than the sum of our parts, andthat’s what this whole conference wasabout.
145Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

ASK THE EXPERT
Should Providers Routinely “Prescribe” Support GroupParticipation for Their Patients with PAH?
Section EditorSean M. Studer, MD, MSc, FCCPClinical Associate ProfessorNew York UniversityNew York, NY
The use of the medical prescriptiondemonstrates a significant evolution fromthe first uses of the symbol �, an abbre-viation for the Latin word recipemeaning “to take,”1 until the presenttime. Early historical treatments thatphysicians prescribed were typicallymedical remedies compounded by thepharmacist. This was followed by ordersfor dispensing pre-packaged, manufac-tured medications in the post-compounding era. The current intentionof a medical prescription has broadenedfurther to now be considered, “. . . ahealth-care program implemented by aphysician or other qualified practitionerin the form of instructions that governthe plan of care for an individualpatient.”2 In the spirit of this definition,non-medication prescriptions, includingthose for specific levels of exercise,dietary guidelines, and treatment modal-ities such as massage therapy, arespecifically prescribed by medical practi-tioners to emphasize their belief in itsvalue for treating a medical condition.This concept of formalizing recommen-dations regarding non-medicationtreatments as a prescription to patientshas been previously studied. In NewZealand the so-called “Green Pre-scription” utilized by generalpractitioners who wrote an exercise pre-scription to improve the level of physicalactivity of their patients showed a signif-icant impact over verbal counselingalone.3 Similarly, an investigationemploying a “bibliotherapy prescription,”which instructed patients suffering from
depression to read a self-help bookentitled Feeling Good, demonstrated thata behavioral prescription was as effectiveas standard therapy, which oftenincluded medications.4 So, in the settingof treatment of patients with pulmonaryarterial hypertension (PAH) and anAdvances issue devoted to the PulmonaryHypertension (PHA) Association’sInternational PH Conference of 2014,we might consider the following ques-tion: Should providers routinely“prescribe” support group participationfor their patients with PAH?
Limited data suggest that recom-mending support group participation totheir patients is not currently a majoritypractice among health care providerstreating PAH. Of all patients who madeinitial contact with PHA through thepeer support program since February2013, 48% specified how they learned ofPHA. Of those patients, 17% indicatedthat they learned about PHA from theirhealthcare provider compared to 42% ofparticipants who indicated that theylearned of PHA through an internetsearch.5 While other support groups (ie,non-PHA support groups) may be rec-ommended by practitioners to theirpatients, recommending or prescribing asupport group is not typical following aPAH diagnosis. For support group pre-scribing to become routine practice,practitioners would likely seek infor-mation similar to other treatments theynow prescribe: data supporting safety,and effectiveness, which is subsequently
affirmed by positive experiences fromtheir patients.
Without high quality studiesdescribing the safety or risk of supportgroup participation for patients withPAH, practitioners are free to hypoth-esize regarding the possible downsides ofsupport group participation, which seemlikely to be minimal. Patients may reador hear misinformation, misinterpretwell-meaning information, and becomeacquainted with patients whose PAHworsens over time. These and other pos-sibilities should be considered; theyargue for recommending participation ina support group with a good medicalfoundation as well as one that recom-mends that those who may becomedistressed after participation address allconcerns with their PAH team andother medical providers. Proceeding withthe premise that support groups withthese good foundations are available topatients, might we expect that partici-pation is likely to be effective inimproving their disease outcomes? Aswith the question of safety, studies spe-cifically addressing disease outcomemeasures in PAH are lacking, requiringthat one consider data regarding supportgroup effects on other chronic, life-threatening diseases.
Breast cancer, like PAH, is a life-threatening disease predominantlyaffecting women that has some researchdata regarding the effects of supportgroups on illness outcome. The datahave been somewhat inconsistent interms of specific benefits observed;however, in one large prospective studysupportive–expressive group therapyimproved mood and the perception ofCorrespondence: [email protected]
146 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

pain, particularly in women who wereinitially more distressed. This same trialdid not evidence prolonged survival inwomen with metastatic breast cancer inthe support group arm, however, as wasseen in prior other smaller trials.6 Incontrast, a large meta-analysis of cardio-vascular disease patients that included 23trials (2024 patients versus 1156 con-trols) observed that group psychosocialsupport improved anxiety anddepression, biomarkers such as systolicblood pressure, heart rate, and choles-terol level, decreased event recurrencerate, and also reduced mortality. Theauthors recommended that psychosocialsupport components be included incardiac rehabilitation programs.7 Obvi-ously, this is just a small sampling of thedata regarding support interventions,however, it suggests that measurablebenefits regarding illness trajectory maybe attained from support group partici-pation.
While medical practitioners rely onquantifiable data, such as shown in thesestudies related to breast cancer and cor-onary artery disease, in deciding toprescribe specific treatments, the patientresponse to these treatments may rein-force or discourage continuedprescribing. Extensive positive data areavailable in this area of the patient-reported outcomes for support groupexperiences, although generally not in ascientifically/statistically analyzedformat.5 The individual data points,which in this case are the patient testi-monials, may be the most influential.Many practitioners who have cared forpatients with PAH have listened todescriptions of the peer-to-peer sharingthat has provided irreplaceable affir-mation, information, and inspiration
from fellow support group participants.The experience of support group may beso transformative that some patientshave been moved to write and publishtheir experiences. One such account ofan individual diagnosed with PAH whoattended her first PHA InternationalConference in 2004–which was a patientsupport group on a grand scale–wroteregarding the experience of meetingothers with this rare disease, “I am oneof the few but I am not aloneanymore . . . I don’t have to hold ontothis disease and feel it is only me. I canloosen the grip and share the load withothers.” Although routine support groupattendance may not be well-suited foreveryone (and some may attend once oronly sporadically), for many the benefitsare immeasurable and probably worthyof prescribing for most patients withPAH.
In summary, the medical prescriptionhas evolved from its original intent as arecipe for compounding medicinal agentsto its present form, which may includebehavioral recommendations for diseasemanagement. Data suggest that prescrip-tions from medical practitioners toincrease physical activity are effective inpromoting exercise compared to verbalrecommendations alone. Investigations ofprescribing self-help reading for patientswith depression showed benefits thatapproached those achieved with standardcare. The absence of studies of psycho-social support group effects in PAHleads us to look at support group effectsin the setting of other serious, chronicillnesses such as breast cancer and cor-onary disease. Support groupparticipation in these areas may have arange of significant patient benefitsincluding the potential to improve sur-
vival. These measurable benefits onpatient’s disease course are welcomefindings for chronic illnesses that mayaccompany the patient-reported salutaryeffects on mood, anxiety, and decreasedfeelings of isolation reported for patientswith PAH. So, while many patients maystill identify support resources via theinternet, a written recommendation toparticipate in a support group mayincreasingly be considered (to use an oldsaying) “just what the doctor ordered.”
References1. http://askville.amazon.com/symbol-prescription-written-Rx/AnswerViewer.do?requestId�7923703.Accessed November 5, 2014.2. Belknap SM, Moore H, Lanzotti SA, et al.Application of software design principles anddebugging methods to an analgesia prescriptionreduces the risk of severe injury from the medicaluse of opioids. Clin Pharmacol Ther 2008;84:385-392.3. Swinburn BA, Walter L, Aroll B, et al. Thegreen prescription study: a randomized controlledtrial of written exercise advice in general practice.Am J Publ Health 1998; 88:288-291.4. Naylor EV, Antonuccio DO, Litt M, et al.Bibliotherapy as a treatment for depression inprimary care. J Clin Psychol Med Settings 2010; 17:258-271.5. Pulmonary Hypertension Association, data onfile (A. Green and M.P. Gray, personal communi-cation, November 6, 2014)6. Linden W, Stossel C, Maurice J. Psychosocialinterventions for patients with coronary artery dis-ease: A meta-analysis. Arch Intern Med. 1996; 156:745-752.7. Goodwin PJ, Leszcz M, Ennis M, et al. Theeffect of group psychosocial support on survival inmetastatic breast cancer. N Engl J Med 2001; 345:1719-1726.8. http://www.phassociation.org/LocalSupport-Groups/Stories. Accessed November 13, 2014.9. Morrill JB. Living with Pulmonary Hyperten-sion: 34 Years and Counting. Shirley, ME:Moosehead Communications; 2010.
147Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

PH PROFESSIONAL NETWORK
An Allied Health Professional’s Experience at PHA’sInternational Conference
Section EditorMary Bartlett, MS, RN, CS, FNP
Chris Archer-Chicko, MSN, CRNP-BCPenn Presbyterian Medical CenterPhiladelphia, Pennsylvania
I have attended several PulmonaryHypertension Association (PHA) inter-national conferences over the years.During that time, the PHA has grownand evolved as an organization,becoming a vital resource for the entirepulmonary hypertension (PH) com-munity (patients/families, health careproviders, and researchers). This was myninth PHA international conference. Aswith previous conferences, I arrived filledwith excitement for PHA’s 2014 RacingToward a Cure conference.
The scientific sessions this yearfocused on new treatments and targets inPH. Dr Norbert Weissmann fromGermany discussed nitric oxide inhi-bition as a potential therapy for chronicobstructive pulmonary disease (COPD)(Group 3 PH) patients. Dr Marc Simonpresented current clinical trials involvingnitric oxide therapeutics in pulmonaryvascular disease. Dr Steven Kawut par-ticipated in panel discussion on clinicaltrial design, emphasizing the importanceof upholding ethical standards during thedesign and conduct of research inpatients with PH. Dr Ioana Preston pre-sented information on new drugs in thepipeline for PH. The latest conceptsregarding active research efforts willenable all members of the PH com-munity to offer patients hope for a cure.
The PHA conference officially openedduring lunch on Friday, with all attendeesgathered in the grand ballroom. I appre-
ciated seeing the eager PH patients andtheir families: this was the first PHAconference for many of them. Theexcitement in the room was palpableduring a video presentation of Dr PattyGeorge leading her Team PHenomenalHope as they biked across the countryraising awareness and funds for PHresearch. I especially enjoyed seeing mypatients who had traveled from Phila-delphia. (I must admit: I checked themdaily during the conference to ensure theywere feeling okay.) The conference is alsoa wonderful opportunity to catch up withnurse and physician colleagues from PHcenters across the country.
I led a session on Saturday titled Carefor the Adult PH Caregiver, which wasa panel discussion on what caregiversshould know about PH as a diseaseprocess, and how to manage multiplepriorities with a chronic illness. Panelistsincluded a clinical PH nurse, socialworker, and PH physician, offering theaudience differing perspectives on navi-gating life with an ongoing condition.We presented to a full room of PHpatients and caregivers—all seeking solu-tions for managing the difficulties ofchronic illness. There was laughter aswell as tears of relief as caregiversexpressed their fears to a supportiveaudience. It was a very helpful sessionfor many, and the audience appearedrelieved to know they are not facing thischallenge alone.
I particularly enjoyed hearing Dr RayBenza present “Etiology, Diagnosis, andManagement of Right VentricularFailure in PH.” He reviewed physiologicconcepts of managing acute and chronicright heart failure. Dr Stephen Matthaidiscussed the challenges of PH asso-ciated with connective tissue disease, andDr Steven Kawut reviewed PH in lungdisease.
My favorite session during each PHAconference is the PH fashion show. Ilove seeing PH patient models (men,women, and children) strut the catwalkwith confidence, knowing their infusionpumps or oxygen tubes are skillfullyhidden under their clothing. DebbieCastro and Lucas van Wormer served asemcees, describing the outfits and addingsome humor. It is such a fun session andthe audience always cheers enthusiasti-cally. The patient models had their hairand makeup done this year, and theylooked fantastic. It is wonderful to seethem beam with the assurance that theycan face the world as a regular person—not just a patient with an illness. Ihighly recommend adding this session toyour PHA conference agenda in 2016.
Racing Toward a Cure was a greatsuccess. From the scientific sessions tothe closing, the PHA conference offerededucation and support for the entire PHcommunity. I learned about newresearch, targets, and therapies, and Ispent meaningful time with nurse andphysician colleagues. I will eagerly antic-ipate attending the next conference inDallas in 2016!Correspondence: [email protected]
148 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

THINK INHALED PROSTACYCLINBEFORE THEY’RE IN TOO DEEP
When treating PAH, time is of the essence1-3
PAH may be progressing even if patients do not appear symptomatic4,5
Delayed treatment may limit long-term improvements in 6MWD, as shown by data from uncontrolled open-label studies6-14
Learn from PAH experts about a potential impact of delayed treatment at PAH2deep.com.References: 1. Badesch DB, Raskob GE, Elliott CG, et al. Chest. 2010;137(2):376-387. 2. Humbert M, Sitbon O, Chaouat A, et al. Am J Respir Crit Care Med. 2006;173(9):1023-1030. 3. Benza RL, Miller DP, Gomberg-Maitland M, et al. Circulation. 2010;122(2):164-172. 4. Schiebler ML, Bhalla S, Runo J, et al. J Thorac Imaging. 2013;28(3):178-195. 5. Barst R. Int J Clin Pract. 2010;64(suppl 168):23-32. 6. Benza RL, Seeger W, McLaughlin VV, et al. J Heart Lung Transplant. 2011;30(12):1327-1333. 7. Frost AE, McLaughlin VV, Oudiz RJ, et al. Poster presented at: American Thoracic Society International Meeting; May 18-23, 2007; San Francisco, CA. 8. Oudiz RJ, Brundage BH, Galiè N, et al, for the PHIRST Study Group. J Am Coll Cardiol. 2012;60(8):768-774. 9. Waxman AB, on behalf of the ARIES Study Group. Chest. 2009; 136(4 meeting abstracts):56S. 10. McLaughlin VV, and the ARIES Study Group. Poster presented at: American Thoracic Society; May 16-21, 2008; Toronto, Ontario. 11. Sitbon O, Badesch DB, Channick RN, et al. Chest. 2003;124(1):247-254. 12. Badesch DB, Barst RJ, Galiè N, Black CM, Rubin LJ. Circulation. 2006;114:II_578. 13. Gatzoulis MA, Beghetti M, Galiè N, et al, on behalf of the BREATHE-5 Investigators. Int J Cardiol. 2008;127(1):27-32. 14. Benza RL, Gotzkowsky SK, Jenkins AE, Rubin LJ. Poster presented at: 10th International Pulmonary Hypertension Conference and Scientific Sessions; June 22-24, 2012; Orlando, FL.
© 2014 United Therapeutics Corporation. All rights reserved. US/DS/MAR14/063
IN THE TREATMENT OF PULMONARY ARTERIAL HYPERTENSION (PAH)

Pulmonary Hypertension Association | www.PHAOnlineUniv.org
������������� ����
Free CME Programs, Journal, News and PH Resources
Free CME Programs, Journal, News and PH Resources
PHA Online University��������������������������� !�� �� ������"��#��$����������%�������� �����%������ ������#��$���%��� !��� &���������� �'��'����������(�%������ $������ ������ ���������the latest advances in the *����
���PHA Online University(��� ���� ������%������ ���� �+
• �������������� ������������� ��
• ������������������������ �����������Advances in Pulmonary Hypertension
• ������� ������� ��������� �������� ���� ���������������
• ���� ����� ��� �����! ����������� ������� ����"������ ���#��$��������
• % ����� �� �����#� �� �����!��� �������� ���� ��� ������������ ���
����������������������#�����������!��������������������������������
��� ����������������
Topics include:
• ������% ���� ��&�'����������
• (����������&�'��������
• ���%�����)�*+������,� ����
• ��� �����% ������
• ���#� ���-�����
and more!

Go to www.letairis.com to learn more.
Please see accompanying brief summary of full Prescribing Information, including Boxed WARNING on the risk of embryo-fetal toxicity.
© 2014 Gilead Sciences, Inc. All rights reserved. LETP0115 April 2014Letairis is a registered trademark of Gilead Sciences, Inc. Gilead and the Gilead logo are trademarks of Gilead Sciences, Inc.
The goals that matter to you matter to patients
goals
Lisa P.Letairis patient

Letairis®(ambrisentan) 5 mg and 10 mg Tablets, for oral useBrief summary of full prescribing information. See full prescribing information. Rx only.
BOXED WARNING: EMBRYO-FETAL TOXICITYDo not administer Letairis to a pregnant female because it may cause fetal harm. Letairis is very likely to produce serious birth defects if used by pregnant female, as this effect has been seen consistently when it is administered to animals [see Contraindications, Use in Specific Populations].
Exclude pregnancy before the initiation of treatment with Letairis. Females of Reproductive Potential must use acceptable methods of contraception during treatment with Letairis and for one month after treatment. Obtain monthly pregnancy tests during treatment and 1 month after discontinuation of treatment [see Use in Special Populations].
Because of the risk of embryo-fetal toxicity, females can only receive Letairis through a restricted program called the Letairis REMS Program [see Warnings and Precautions].
INDICATIONS AND USAGE: Letairis is indicated for the treatment of pulmonary arterial hypertension (PAH) (WHO Group 1) to improve exercise ability and delay clinical worsening. Studies establishing effectiveness included predominantly patients with WHO Functional Class II-III symptoms and etiologies of idiopathic or heritable PAH (64%) or PAH associated with connective tissue diseases (32%).
DOSAGE AND ADMINISTRATION: Adult Dosage: Initiate treatment at 5 mg once daily, and consider increasing the dose to 10 mg once daily if 5 mg is tolerated. Tablets may be administered with or without food. Tablets should not be split, crushed, or chewed. Doses higher than 10 mg once daily have not been studied in patients with pulmonary arterial hypertension (PAH). Pregnancy Testing in Females of Reproductive Potential: Initiate treatment with Letairis in Females of Reproductive Potential only after a negative pregnancy test. Obtain monthly tests during treatment [see Use in Specific Populations].
CONTRAINDICATIONS: Pregnancy: Letairis may cause fetal harm when administered to a pregnant female. Letairis was consistently shown to have teratogenic effects when administered to animals. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to a fetus [see Warnings and Precautions, Use in Specific Populations]. Idiopathic Pulmonary Fibrosis: Letairis is contraindicated in patients with Idiopathic Pulmonary Fibrosis (IPF) including IPF patients with pulmonary hypertension (WHO Group 3) [see Clinical Studies].WARNINGS AND PRECAUTIONS: Letairis REMS Program: For all females, Letairis is available only through a restricted program called the Letairis REMS, because of risk of embryo-fetal toxicity [see Contraindications, Warnings and Precautions, Use in Specific Populations]. Notable requirements of the Letairis REMS Program include that the Prescribers must be certified with the program by enrolling and completing training. All females, regardless of reproductive potential, must enroll in the Letairis REMS Program prior to initiating Letairis. Male patients are not enrolled in the REMS. Females of Reproductive Potential must comply with the pregnancy testing and contraception requirements [see Use in Specific Populations]. Pharmacies that dispense Letairis must be certified with the program and must dispense to female patients who are authorized to receive Letairis. Further information is available at www.letairisrems.com or 1-866-664-5327. Fluid Retention: Peripheral edema is a known class effect of endothelin receptor antagonists, and is also a clinical consequence of PAH and worsening PAH. In the placebo controlled studies, there was an increased incidence of peripheral edema in patients treated with doses of 5 or 10 mg Letairis compared to placebo [see Adverse Reactions]. Most edema was mild to moderate in severity, and it occurred with greater frequency and severity in elderly patients. In addition, there have been post-marketing reports of fluid retention in patients with pulmonary hypertension, occurring within weeks after starting Letairis. Patients required intervention with a diuretic, fluid management, or, in some cases, hospitalization for decompensating heart failure. If clinically significant fluid retention develops, with or without associated weight gain, further evaluation should be undertaken to determine the cause, such as Letairis or underlying heart failure, and the possible need for specific treatment or discontinuation of Letairis therapy. Pulmonary Veno-occlusive Disease: If patients develop acute pulmonary edema during initiation of therapy with vasodilating agents such as Letairis, the possibility of pulmonary veno-occlusive disease should be considered, and if confirmed Letairis should be discontinued. Decreased Sperm Counts: Decreased sperm counts have been observed in human and animal studies with another endothelin receptor antagonist and in animal fertility studies with ambrisentan. Letairis may have an adverse effect on spermatogenesis. Counsel patients about potential effects on fertility [see Specific Populations, Nonclinical Toxicology]. Hematological Changes: Decreases in hemoglobin concentration and hematocrit have followed administration of other endothelin receptor antagonists and were observed in clinical studies with Letairis. These decreases were observed within the first few weeks of treatment with Letairis, and stabilized thereafter. The mean decrease in hemoglobin from baseline to end of treatment for those patients receiving Letairis in the 12 week placebo controlled studies was 0.8 g/dL. Marked decreases in hemoglobin (>15% decrease from baseline resulting in a value below the lower limit of normal) were observed in 7% of all patients receiving Letairis (and 10% of patients receiving 10 mg) compared to 4% of patients receiving placebo. The cause of the decrease in hemoglobin is unknown, but it does not appear to result from hemorrhage or hemolysis. In the long-term open-label extension of the two pivotal clinical studies, mean decreases from baseline (ranging from 0.9 to 1.2 g/dL) in hemoglobin concentrations persisted for up to 4 years of treatment. There have been postmarketing reports of decreases in hemoglobin concentration and hematocrit that have resulted in anemia requiring transfusion. Measure hemoglobin prior to initiation of Letairis, at one month, and periodically thereafter. Initiation of Letairis therapy is not recommended for patients with clinically significant anemia. If a clinically significant decrease in hemoglobin is observed and other causes have been excluded, consider discontinuing Letairis.
ADVERSE REACTIONS: Clinically significant adverse reactions that appear in other sections of the labeling include: Embryo-fetal toxicity [see Warnings and Precautions, Use in Specific Populations] Fluid Retention [see Warnings and Precautions] Pulmonary Edema with PVOD [see Warnings and Precautions] Decreased Sperm Count [see Warnings and Precautions] Hematologic changes [see Warnings and Precautions]. Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. Safety data for Letairis were obtained from two 12 week, placebo controlled studies in patients with
pulmonary arterial hypertension (PAH) (ARIES-1 and ARIES-2) and four nonplacebo controlled studies in 483 patients with PAH who were treated with doses of 1, 2.5, 5, or 10 mg once daily. The exposure to Letairis in these studies ranged from 1 day to 4 years (N=418 for at least 6 months and N=343 for at least 1 year). In ARIES-1 and ARIES-2, a total of 261 patients received Letairis at doses of 2.5, 5, or 10 mg once daily and 132 patients received placebo. The adverse reactions that occurred in >3% more patients receiving Letairis than receiving placebo are shown in Table 1.
Table 1 Adverse Reactions with Placebo-Adjusted Rates >3%
Placebo (N=132) Letairis (N=261)
Adverse reaction n (%) n (%) Placebo-adjusted (%)
Peripheral edema 14 (11) 45 (17) 6
Nasal congestion 2 (2) 15 (6) 4
Sinusitis 0 (0) 8 (3) 3
Flushing 1 (1) 10 (4) 3
Most adverse drug reactions were mild to moderate and only nasal congestion was dose dependent. Few notable differences in the incidence of adverse reactions were observed for patients by age or sex. Peripheral edema was similar in younger patients (<65 years) receiving Letairis (14%; 29/205) or placebo (13%; 13/104), and was greater in elderly patients (≥65 years) receiving Letairis (29%; 16/56) compared to placebo (4%; 1/28). The results of such subgroup analyses must be interpreted cautiously. The incidence of treatment discontinuations due to adverse events other than those related to PAH during the clinical trials in patients with PAH was similar for Letairis (2%; 5/261 patients) and placebo (2%; 3/132 patients). The incidence of patients with serious adverse events other than those related to PAH during the clinical trials in patients with PAH was similar for placebo (7%; 9/132 patients) and for Letairis (5%; 13/261 patients). During 12-week controlled clinical trials, the incidence of aminotransferase elevations >3x upper limit of normal (ULN) were 0% on Letairis and 2.3% on placebo. In practice, cases of hepatic injury should be carefully evaluated for cause. Use in Patients with Prior Endothelin Receptor Antagonist (ERA) Related Serum Liver Enzyme Abnormalities: In an uncontrolled, open label study, 36 patients who had previously discontinued endothelin receptor antagonists (ERAs: bosentan, an investigational drug, or both) due to aminotransferase elevations >3x ULN were treated with Letairis. Prior elevations were predominantly moderate, with 64% of the ALT elevations <5x ULN, but 9 patients had elevations >8 x ULN. Eight patients had been re-challenged with bosentan and/or the investigational ERA and all eight had a recurrence of aminotransferase abnormalities that required discontinuation of ERA therapy. All patients had to have normal aminotransferase levels on entry to this study. Twenty-five of the 36 patients were also receiving prostanoid and/or phosphodiesterase type 5 (PDE5) inhibitor therapy. Two patients discontinued early (including one of the patients with a prior 8x ULN elevation). Of the remaining 34 patients, one patient experienced a mild aminotransferase elevation at 12 weeks on Letairis 5 mg that resolved with decreasing the dosage to 2.5 mg, and that did not recur with later escalations to 10 mg. With a median follow-up of 13 months and with 50% of patients increasing the dose of Letairis to 10 mg, no patients were discontinued for aminotransferase elevations. While the uncontrolled study design does not provide information about what would have occurred with re-administration of previously used ERAs or show that Letairis led to fewer aminotransferase elevations than would have been seen with those drugs, the study indicates that Letairis may be tried in patients who have experienced asymptomatic aminotransferase elevations on other ERAs after aminotransferase levels have returned to normal. Postmarketing Experience: The following adverse reactions were identified during postapproval use of Letairis. Because these reactions were reported voluntarily from a population of uncertain size, it is not possible to estimate reliably the frequency or to establish a causal relationship to drug exposure: anemia [see Warnings and Precautions], fluid retention [see Warnings and Precautions], heart failure (associated with fluid retention), hypersensitivity (e.g., angioedema, rash), nausea, and vomiting. Elevations of liver aminotransferases (ALT, AST) have been reported with Letairis use; in most cases alternative causes of the liver injury could be identified (heart failure, hepatic congestion, hepatitis, alcohol use, hepatotoxic medications). Other endothelin receptor antagonists have been associated with elevations of aminotransferases, hepatotoxicity, and cases of liver failure [see Adverse Reactions].
DRUG INTERACTIONS: Multiple dose co-administration of ambrisentan and cyclosporine resulted in an approximately 2-fold increase in ambrisentan exposure in healthy volunteers; therefore, limit the dose of ambrisentan to 5 mg once daily when co-administered with cyclosporine [see Clinical Pharmacology].
USE IN SPECIFIC POPULATIONS: Pregnancy Category X: Risk Summary: Letairis may cause fetal harm when administered to a pregnant woman and is contraindicated during pregnancy. Letairis was teratogenic in rats and rabbits at doses which resulted in exposures of 3.5 and 1.7 times respectively the human dose of 10 mg per day. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, advise the patient of the potential hazard to a fetus [see Contraindications, Warnings and Precautions]. Animal Data: Letairis was teratogenic at oral doses of ≥15 mg/kg/day (AUC 51.7 h•μg/mL) in rats and ≥7 mg/kg/day (24.7 h•μg/mL) in rabbits; it was not studied at lower doses. These doses are of 3.5 and 1.7 times respectively the human dose of 10 mg per day (14.8 h•μg/mL) based on AUC. In both species, there were abnormalities of the lower jaw and hard and soft palate, malformation of the heart and great vessels, and failure of formation of the thymus and thyroid. A preclinical study in rats has shown decreased survival of newborn pups (mid and high doses) and effects on testicle size and fertility of pups (high dose) following maternal treatment with ambrisentan from late gestation through weaning. Doses tested were 17x, 51x, and 170x (on a mg/kg:mg/m2 basis) the maximum oral human dose of 10 mg and an average adult body weight of 70 kg.Nursing Mothers: It is not known whether ambrisentan is present in human milk. Because many drugs are present in human milk and because of the potential for serious adverse reactions in nursing infants from Letairis, a decision should be made whether to discontinue nursing or discontinue Letairis, taking into account the importance of the drug to the mother. Pediatric Use: Safety and effectiveness of Letairis in pediatric patients have not been established. Geriatric Use: In the two placebo controlled clinical studies of Letairis, 21% of patients were ≥65 years old and 5% were ≥75 years old. The elderly (age ≥65 years) showed less improvement in walk distances with Letairis than younger patients did, but the results of such subgroup analyses must be interpreted cautiously. Peripheral edema was more common in the elderly than in younger patients. Females and Males of Reproductive Potential: Pregnancy Testing: Female patients of reproductive potential must have a negative pregnancy test prior to initiation of treatment, monthly pregnancy test during treatment, and 1 month after stopping treatment with Letairis. Advise patients to contact their health care provider if they become pregnant or suspect they may be pregnant. Perform a pregnancy test if pregnancy is suspected for any reason. For positive pregnancy tests, counsel patient on the potential risk to the fetus and patient options [see Boxed

For detailed information, please see full Prescribing Information.To learn more: call 1-800-GILEAD-5 (Option 2) or visit www.letairis.com.Manufactured and marketed by: Gilead Sciences, Inc., Foster City, CA 94404, USA © 2014 Gilead Sciences, Inc. All rights reserved. LETP0103 January 2014 Letairis is a registered trademark of Gilead Sciences, Inc. Gilead and the Gilead logo are trademarks of Gilead Sciences, Inc. Other brands noted herein are the property of their respective owners.
Warning and Dosage and Administration]. Contraception: Female patients of reproductive potential must use acceptable methods of contraception during treatment with Letairis and for 1 month after stopping treatment with Letairis. Patients may choose one highly effective form of contraception (intrauterine devices (IUD), contraceptive implants, or tubal sterilization) or a combination of methods (hormone method with a barrier method or two barrier methods). If a partner’s vasectomy is the chosen method of contraception, a hormone or barrier method must be used along with this method. Counsel patients on pregnancy planning and prevention, including emergency contraception, or designate counseling by another healthcare provider trained in contraceptive counseling [see Boxed Warning]. Infertility: Males In a 6-month study of another endothelin receptor antagonist, bosentan, 25 male patients with WHO functional class III and IV PAH and normal baseline sperm count were evaluated for effects on testicular function. There was a decline in sperm count of at least 50% in 25% of the patients after 3 or 6 months of treatment with bosentan. One patient developed marked oligospermia at 3 months and the sperm count remained low with 2 follow-up measurements over the subsequent 6 weeks. Bosentan was discontinued and after 2 months the sperm count had returned to baseline levels. In 22 patients who completed 6 months of treatment, sperm count remained within the normal range and no changes in sperm morphology, sperm motility, or hormone levels were observed. Based on these findings and preclinical data [see Nonclinical Toxicology] from endothelin receptor antagonists, it cannot be excluded that endothelin receptor antagonists such as Letairis have an adverse effect on spermatogenesis. Counsel patients about the potential effects on fertility [see Warnings and Precautions]. Renal Impairment: The impact of renal impairment on the pharmacokinetics of ambrisentan has been examined using a population pharmacokinetic approach in PAH patients with creatinine clearances ranging between 20 and 150 mL/min. There was no significant impact of mild or moderate renal impairment on exposure to ambrisentan [see Clinical Pharmacology]. Dose adjustment of Letairis in patients with mild or moderate renal impairment is therefore not required. There is no information on the exposure to ambrisentan in patients with severe renal impairment. The impact of hemodialysis on the disposition of ambrisentan has not been investigated. Hepatic Impairment: Pre-existing hepatic impairment: The influence of pre-existing hepatic impairment on the pharmacokinetics of ambrisentan has not been evaluated. Because there is in vitro and in vivo evidence of significant metabolic and biliary contribution to the elimination of ambrisentan, hepatic impairment would be expected to have significant effects on the pharmacokinetics of ambrisentan [see Clinical Pharmacology]. Letairis is not recommended in patients with moderate or severe hepatic impairment. There is no information on the use of Letairis in patients with mild pre-existing impaired liver function; however, exposure to ambrisentan may be increased in these patients. Elevation of Liver Transaminases: Other endothelin receptor antagonists (ERAs) have been associated with aminotransferase (AST, ALT) elevations, hepatotoxicity, and cases of liver failure [see Adverse Reactions]. In patients who develop hepatic impairment after Letairis initiation, the cause of liver injury should be fully investigated. Discontinue Letairis if aminotransferase elevations >5x ULN or if elevations are accompanied by bilirubin >2x ULN, or by signs or symptoms of liver dysfunction and other causes are excluded.
OVERDOSAGE: There is no experience with overdosage of Letairis. The highest single dose of Letairis administered to healthy volunteers was 100 mg and the highest daily dose administered to patients with PAH was 10 mg once daily. In healthy volunteers, single doses of 50 mg and 100 mg (5 to 10 times the maximum recommended dose) were associated with headache, flushing, dizziness, nausea, and nasal congestion. Massive overdosage could potentially result in hypotension that may require intervention.
PATIENT COUNSELING INFORMATION: See FDA-approved patient labeling (Medication Guide). Embryo-fetal toxicity: Instruct patients on the risk of fetal harm when Letairis is used in pregnancy [see Warnings and Precautions; Use in Special Populations]. Female patients must enroll in the Letairis REMS Program. Instruct Females of Reproductive Potential to immediately contact their physician if they suspect they may be pregnant. Letairis REMS Program: For female patients, Letairis is only available through a restricted program called the Letairis REMS [see Contraindications, Warnings and Precautions]. Male patients are not enrolled in the Letairis REMS. Inform female patients (and their guardians, if applicable) of the following notable requirements: All female patients must sign an enrollment form. Advise female patients of reproductive potential that they must comply with the pregnancy testing and contraception requirements [see Use in Specific Populations]. Educate and counsel Females of Reproductive Potential on the use of emergency contraception in the event of unprotected sex or known or suspected contraceptive failure. Advise pre-pubertal females to report any changes in their reproductive status immediately to their prescriber. Review the Letairis Medication Guide and REMS educational material with female patients. A limited number of pharmacies are certified to dispense Letairis. Therefore, provide patients with the telephone number and website for information on how to obtain the product. Hepatic Effects: Some members of this pharmacological class are hepatotoxic. Patients should be educated on the symptoms of potential liver injury (such as anorexia, nausea, vomiting, fever, malaise, fatigue, right upper quadrant abdominal discomfort, jaundice, dark urine or itching) and instructed to report any of these symptoms to their physician. Hematological Change: Patients should be advised of the importance of hemoglobin testing. Administration: Patients should be advised not to split, crush, or chew tablets.
GS22-081-013
To download your free guides, visit: www.PHAssociation.org/ForYourPatients
RESOURCES FOR COPING WITH PULMONARY HYPERTENSION
PHA offers ongoing education and information for patients and PHA offers ongoing education and information for patients andcaregivers at every stage of their PH journeys. We now provide resources to help your patients and caregivers cope with themental, emotional and social impacts of living with PH.
Coping with Pulmonary Hypertension Guides are available for:
Newly Diagnosed Patients Long-Term Survivors Parents
Caregivers Teens

In the treatment of pulmonary arterial hypertension (PAH, WHO Group I )
IMPORTANT SAFETY INFORMATION
BOXED WARNING: EMBRYO-FETAL TOXICITY
Do not administer OPSUMIT to a pregnant female because it may cause fetal harm.
Females of reproductive potential: Exclude pregnancy before the start of treatment, monthly during treatment, and 1 month after stopping treatment. Prevent pregnancy during treatment and for one month after stopping treatment by using acceptable methods of contraception.
For all female patients, OPSUMIT is available only through a restricted program called the OPSUMIT Risk Evaluation and Mitigation Strategy (REMS).
CONTRAINDICATIONS
Pregnancy: OPSUMIT may cause fetal harm when administered to a pregnant woman. OPSUMIT is contraindicated in females who are pregnant. If OPSUMIT is used during pregnancy, apprise the patient of the potential hazard to a fetus.
WARNINGS AND PRECAUTIONS Embryo-fetal Toxicity and OPSUMIT REMS Program
Due to the risk of embryo-fetal toxicity, OPSUMIT is available for females only through a restricted program called the OPSUMIT REMS Program. For females of reproductive potential, exclude pregnancy prior to initiation of therapy, ensure use of acceptable contraceptive methods, and obtain monthly pregnancy tests.
Notable requirements of the OPSUMIT REMS Program include:
Prescribers must be certified with the program by enrolling and completing training.
All females, regardless of reproductive potential, must enroll in the OPSUMIT REMS Program prior to initiating OPSUMIT. Male patients are not enrolled in the REMS.
Females of reproductive potential must comply with the pregnancy testing and contraception requirements.
Pharmacies must be certified with the program and must only dispense to patients who are authorized to receive OPSUMIT.
Hepatotoxicity
Other ERAs have caused elevations of aminotransferases, hepatotoxicity, and liver failure. The incidence of elevated aminotransferases in the SERAPHIN study >3 × ULN were 3.4% for OPSUMIT vs 4.5% for placebo, and >8 × ULN were 2.1% vs 0.4%, respectively. Discontinuations for hepatic adverse events were 3.3% for OPSUMIT vs 1.6% for placebo.
Obtain liver enzyme tests prior to initiation of OPSUMIT and repeat during treatment as clinically indicated.
Advise patients to report symptoms suggesting hepatic injury (nausea, vomiting, right upper quadrant pain, fatigue, anorexia, jaundice, dark urine, fever, or itching).
If clinically relevant aminotransferase elevations occur, or if elevations are accompanied by an increase in bilirubin >2 × ULN, or by clinical symptoms of hepatotoxicity, discontinue OPSUMIT. Consider re-initiation of OPSUMIT
HELP HER WRITE FUTURE CHAPTERSOnce-daily OPSUMIT® (macitentan) is the first and only oral PAH therapy indicated to
both delay disease progression and reduce hospitalization for PAH
OPSUMIT is an endothelin receptor antagonist (ERA) indicated for the treatment of pulmonary arterial hypertension (PAH, WHO Group I) to delay disease progression.
Disease progression included: death, initiation of intravenous (IV) or subcutaneous prostanoids, or clinical worsening of PAH (decreased 6-minute walk distance, worsened PAH symptoms and need for additional PAH treatment).
OPSUMIT also reduced hospitalization for PAH.
Effectiveness was established in a long-term study in PAH patients with predominantly WHO Functional Class II-III symptoms treated for an average of 2 years.
– Patients were treated with OPSUMIT monotherapy or in combination with phosphodiesterase-5 inhibitors or inhaled prostanoids.
– Patients had idiopathic and heritable PAH (57%), PAH caused by connective tissue disorders (31%), and PAH caused by congenital heart disease with repaired shunts (8%).

OPSUMIT is a registered trademark of Actelion Pharmaceuticals, Ltd.© 2014 Actelion Pharmaceuticals US, Inc. All rights reserved. MAC-00408 0514 www.OpsumitHCP.com
when hepatic enzyme levels normalize in patients who have not experienced clinical symptoms of hepatotoxicity.
Hemoglobin Decrease
Decreases in hemoglobin concentration and hematocrit have occurred following administration of other ERAs and in clinical studies with OPSUMIT. These decreases occurred early and stabilized thereafter.
In the SERAPHIN study, OPSUMIT caused a mean decrease in hemoglobin (from baseline to 18 months) of about 1.0 g/dL vs no change in the placebo group. A decrease in hemoglobin to below 10.0 g/dL was reported in 8.7% of the OPSUMIT group vs 3.4% for placebo. Decreases in hemoglobin seldom require transfusion.
Initiation of OPSUMIT is not recommended in patients with severe anemia. Measure hemoglobin prior to initiation of treatment and repeat during treatment as clinically indicated.
Pulmonary Edema with Pulmonary Veno-occlusive Disease (PVOD)
Should signs of pulmonary edema occur, consider the possibility of associated PVOD. If confirmed, discontinue OPSUMIT.
Decreased Sperm Counts
Other ERAs have caused adverse effects on spermatogenesis. Counsel men about potential effects on fertility.
ADVERSE REACTIONS
Most common adverse reactions (more frequent than placebo by ≥3%) were anemia (13% vs 3%), nasopharyngitis/pharyngitis (20% vs 13%), bronchitis (12% vs 6%), headache (14% vs 9%), influenza (6% vs 2%), and urinary tract infection (9% vs 6%).
DRUG INTERACTIONS
Strong inducers of CYP3A4 such as rifampin significantly reduce macitentan exposure. Concomitant use of OPSUMIT with strong CYP3A4 inducers should be avoided.
Strong inhibitors of CYP3A4 like ketoconazole approximately double macitentan exposure. Many HIV drugs like ritonavir are strong inhibitors of CYP3A4. Avoid concomitant use of OPSUMIT with strong CYP3A4 inhibitors. Use other PAH treatment options when strong CYP3A4 inhibitors are needed as part of HIV treatment.
Please see Brief Summary of Prescribing Information, including BOXED WARNING for embryo-fetal toxicity, on adjacent pages.
Patient dramatization

Rx only
BRIEF SUMMARYThe following is a brief summary of the full Prescribing Information for OPSUMIT® (macitentan). Please review the full Prescribing Information prior to prescribing OPSUMIT.
WARNING: EMBRYO-FETAL TOXICITY• Do not administer OPSUMIT to a pregnant female because it may cause
fetal harm [see Contraindications (Pregnancy), Warnings and Precautions (Embryo-fetal Toxicity), Use in Specifi c Populations (Pregnancy)].
• Females of reproductive potential: Exclude pregnancy before the start of treatment, monthly during treatment, and 1 month after stopping treatment. Prevent pregnancy during treatment and for one month after stopping treatment by using acceptable methods of contraception [see Use in Special Populations (Females and Males of Reproductive Potential)].
• For all female patients, OPSUMIT is available only through a restricted program called the OPSUMIT Risk Evaluation and Mitigation Strategy (REMS) [see Warnings and Precautions (OPSUMIT REMS Program)].
INDICATIONS AND USAGEPulmonary Arterial HypertensionOPSUMIT® is an endothelin receptor antagonist (ERA) indicated for the treatment of pulmonary arterial hypertension (PAH, WHO Group I) to delay disease progression. Disease progression included: death, initiation of intravenous (IV) or subcutaneous prostanoids, or clinical worsening of PAH (decreased 6-minute walk distance, worsened PAH symptoms and need for additional PAH treatment). OPSUMIT also reduced hospitalization for PAH.Effectiveness was established in a long-term study in PAH patients with predominantly WHO Functional Class II-III symptoms treated for an average of 2 years. Patients were treated with OPSUMIT monotherapy or in combination with phosphodiesterase-5 inhibitors or inhaled prostanoids. Patients had idiopathic and heritable PAH (57%), PAH caused by connective tissue disorders (31%), and PAH caused by congenital heart disease with repaired shunts (8%).
CONTRAINDICATIONSPregnancyOPSUMIT may cause fetal harm when administered to a pregnant woman. OPSUMIT is contraindicated in females who are pregnant. OPSUMIT was consistently shown to have teratogenic effects when administered to animals. If OPSUMIT is used during pregnancy, apprise the patient of the potential hazard to a fetus [see Warnings and Precautions (Embryo-fetal Toxicity) and Use in Specifi c Populations (Pregnancy) ].
WARNINGS AND PRECAUTIONSEmbryo-fetal ToxicityOPSUMIT may cause fetal harm when administered during pregnancy and is contraindicated for use in females who are pregnant. In females of reproductive potential, exclude pregnancy prior to initiation of therapy, ensure use of acceptable contraceptive methods and obtain monthly pregnancy tests [see Dosage and Administration section 2.2 in full Prescribing Information and Use in Specifi c Populations (Pregnancy, Females and Males of Reproductive Potential) ].OPSUMIT is available for females through the OPSUMIT REMS Program, a restricted distribution program [see Warnings and Precautions (OPSUMIT REMS Program) ].
OPSUMIT REMS ProgramFor all females, OPSUMIT is available only through a restricted program called the OPSUMIT REMS Program, because of the risk of embryo-fetal toxicity [see Contraindications (Pregnancy), Warnings and Precautions (Embryo-fetal Toxicity), and Use in Specifi c Populations (Pregnancy, Females and Males of Reproductive Potential) ].Notable requirements of the OPSUMIT REMS Program include the following:• Prescribers must be certifi ed with the program by enrolling and completing training.• All females, regardless of reproductive potential, must enroll in the OPSUMIT REMS
Program prior to initiating OPSUMIT. Male patients are not enrolled in the REMS.• Females of reproductive potential must comply with the pregnancy testing and
contraception requirements [see Use in Specifi c Populations (Females and Males of Reproductive Potential) ].
• Pharmacies must be certifi ed with the program and must only dispense to patients who are authorized to receive OPSUMIT.
Further information is available at www.OPSUMITREMS.com or 1-866-228-3546. Information on OPSUMIT certifi ed pharmacies or wholesale distributors is available through Actelion Pathways at 1-866-228-3546.
HepatotoxicityOther ERAs have caused elevations of aminotransferases, hepatotoxicity, and liver failure. The incidence of elevated aminotransferases in the study of OPSUMIT in PAH is shown in Table 1.
Table 1: Incidence of Elevated Aminotransferases in the SERAPHIN Study
OPSUMIT 10 mg(N=242)
Placebo(N=249)
>3 × ULN 3.4% 4.5%
>8 × ULN 2.1% 0.4%
In the placebo-controlled study of OPSUMIT, discontinuations for hepatic adverse events were 3.3% in the OPSUMIT 10 mg group vs. 1.6% for placebo. Obtain liver enzyme tests prior to initiation of OPSUMIT and repeat during treatment as clinically indicated.Advise patients to report symptoms suggesting hepatic injury (nausea, vomiting, right upper quadrant pain, fatigue, anorexia, jaundice, dark urine, fever, or itching). If clinically relevant aminotransferase elevations occur, or if elevations are accompanied by an increase in bilirubin >2 × ULN, or by clinical symptoms of hepatotoxicity, discontinue OPSUMIT. Consider re-initiation of OPSUMIT when hepatic enzyme levels normalize in patients who have not experienced clinical symptoms of hepatotoxicity.
Hemoglobin DecreaseDecreases in hemoglobin concentration and hematocrit have occurred following administration of other ERAs and were observed in clinical studies with OPSUMIT. These decreases occurred early and stabilized thereafter. In the placebo-controlled study of OPSUMIT in PAH, OPSUMIT 10 mg caused a mean decrease in hemoglobin from baseline to up to 18 months of about 1.0 g/dL compared to no change in the placebo group. A decrease in hemoglobin to below 10.0 g/dL was reported in 8.7% of the OPSUMIT 10 mg group and in 3.4% of the placebo group. Decreases in hemoglobin seldom require transfusion. Initiation of OPSUMIT is not recommended in patients with severe anemia. Measure hemoglobin prior to initiation of treatment and repeat during treatment as clinically indicated [see Adverse Reactions (Clinical Trial Experience) ].
Pulmonary Edema with Pulmonary Veno-occlusive Disease (PVOD)Should signs of pulmonary edema occur, consider the possibility of associated PVOD. If confi rmed, discontinue OPSUMIT.
Decreased Sperm CountsOther ERAs have caused adverse effects on spermatogenesis. Counsel men about potential effects on fertility [see Use in Specifi c Populations (Females and Males of Reproductive Potential) and Nonclinical Toxicology (Carcinogenesis, Mutagenesis, Impairment of Fertility) ].
ADVERSE REACTIONSClinically signifi cant adverse reactions that appear in other sections of the labeling include:• Embryo-fetal Toxicity [see Warnings and Precautions (Embryo-fetal Toxicity) ]• Hepatotoxicity [see Warnings and Precautions (Hepatotoxicity) ]• Decrease in Hemoglobin [see Warnings and Precautions (Hemoglobin Decrease) ]
Clinical Trial ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not refl ect the rates observed in clinical practice.Safety data for OPSUMIT were obtained primarily from one placebo-controlled clinical study in 742 patients with PAH (SERAPHIN study). The exposure to OPSUMIT in this trial was up to 3.6 years with a median exposure of about 2 years (N=542 for 1 year; N=429 for 2 years; and N=98 for more than 3 years). The overall incidence of treatment discontinuations because of adverse events was similar across OPSUMIT 10 mg and placebo treatment groups (approximately 11%).Table 2 presents adverse reactions more frequent on OPSUMIT than on placebo by ≥3%.
Table 2: Adverse Reactions
Adverse Reaction OPSUMIT 10 mg(N=242)
Placebo(N=249)
Anemia 13% 3%
Nasopharyngitis/pharyngitis 20% 13%
Bronchitis 12% 6%
Headache 14% 9%
Infl uenza 6% 2%
Urinary tract infection 9% 6%
DRUG INTERACTIONSStrong CYP3A4 InducersStrong inducers of CYP3A4 such as rifampin signifi cantly reduce macitentan exposure. Concomitant use of OPSUMIT with strong CYP3A4 inducers should be avoided [see Clinical Pharmacology (Pharmacokinetics) ].
OPSUMIT® (macitentan)

Strong CYP3A4 InhibitorsConcomitant use of strong CYP3A4 inhibitors like ketoconazole approximately double macitentan exposure. Many HIV drugs like ritonavir are strong inhibitors of CYP3A4. Avoid concomitant use of OPSUMIT with strong CYP3A4 inhibitors [see Clinical Pharmacology (Pharmacokinetics) ]. Use other PAH treatment options when strong CYP3A4 inhibitors are needed as part of HIV treatment [see Clinical Pharmacology (Pharmacokinetics) ].
USE IN SPECIFIC POPULATIONSPregnancyPregnancy Category X.Risk SummaryOPSUMIT may cause fetal harm when administered to a pregnant woman and is contraindicated during pregnancy. Macitentan was teratogenic in rabbits and rats at all doses tested. A no-effect dose was not established in either species. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, advise the patient of the potential hazard to a fetus [see Contraindications (Pregnancy)].
Animal DataIn both rabbits and rats, there were cardiovascular and mandibular arch fusion abnormalities. Administration of macitentan to female rats from late pregnancy through lactation caused reduced pup survival and impairment of the male fertility of the offspring at all dose levels tested.
Nursing MothersIt is not known whether OPSUMIT is present in human milk. Macitentan and its metabolites were present in the milk of lactating rats. Because many drugs are present in human milk and because of the potential for serious adverse reactions from macitentan in nursing infants, nursing mothers should discontinue nursing or discontinue OPSUMIT.
Pediatric useThe safety and effi cacy of OPSUMIT in children have not been established.
Geriatric useOf the total number of subjects in the clinical study of OPSUMIT for PAH, 14% were 65 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects.
Females and Males of Reproductive PotentialFemalesPregnancy Testing: Female patients of reproductive potential must have a negative pregnancy test prior to starting treatment with OPSUMIT and monthly pregnancy tests during treatment with OPSUMIT. Advise patients to contact their health care provider if they become pregnant or suspect they may be pregnant. Perform a pregnancy test if pregnancy is suspected for any reason. For positive pregnancy tests, counsel patients on the potential risk to the fetus [see Boxed Warning and Dosage and Administration section 2.2 in full Prescribing Information].Contraception: Female patients of reproductive potential must use acceptable methods of contraception during treatment with OPSUMIT and for 1 month after treatment with OPSUMIT. Patients may choose one highly effective form of contraception (intrauterine devices (IUD), contraceptive implants or tubal sterilization) or a combination of methods (hormone method with a barrier method or two barrier methods). If a partner’s vasectomy is the chosen method of contraception, a hormone or barrier method must be used along with this method. Counsel patients on pregnancy planning and prevention, including emergency contraception, or designate counseling by another healthcare provider trained in contraceptive counseling [see Boxed Warning].MalesTesticular effects: Like other endothelin receptor antagonists, OPSUMIT may have an adverse effect on spermatogenesis [see Warnings and Precautions (Decreased Sperm Counts) and Nonclinical Toxicology (Carcinogenesis, Mutagenesis, Impairment of Fertility ].
OVERDOSAGEOPSUMIT has been administered as a single dose of up to and including 600 mg to healthy subjects (60 times the approved dosage). Adverse reactions of headache, nausea and vomiting were observed. In the event of an overdose, standard supportive measures should be taken, as required. Dialysis is unlikely to be effective because macitentan is highly protein-bound.
CLINICAL PHARMACOLOGYPharmacokineticsSpecial PopulationsThere are no clinically relevant effects of age, sex, or race on the pharmacokinetics of macitentan and its active metabolite.Renal impairment : Exposure to macitentan and its active metabolite in patients with severe renal impairment (CrCl 15-29 mL/min) compared to healthy subjects was increased by 30% and 60%, respectively. This increase is not considered clinically relevant.Hepatic impairment: Exposure to macitentan was decreased by 21%, 34%, and 6% and exposure to the active metabolite was decreased by 20%, 25%, and 25% in subjects with mild, moderate, or severe hepatic impairment (Child-Pugh Class A, B, and C), respectively. This decrease is not considered clinically relevant.
Drug Interactions
In vitro studiesAt plasma levels obtained with dosing at 10 mg once daily, macitentan has no relevant inhibitory or inducing effects on CYP enzymes, and is neither a substrate nor an inhibitor of the multi-drug resistance protein (P-gp, MDR-1). Macitentan and its active metabolite are neither substrates nor inhibitors of the organic anion transporting polypeptides (OATP1B1 and OATP1B3) and do not significantly interact with proteins involved in hepatic bile salt transport, i.e., the bile salt export pump (BSEP) and the sodium-dependent taurocholate co-transporting polypeptide (NTCP).
In vivo studiesEffect of other drugs on macitentan: The effect of other drugs on macitentan and its active metabolite are studied in healthy subjects and are shown in Figure 1 below.Figure 1
Effects of other strong CYP3A4 inhibitors such as ritonavir on macitentan were not studied, but are likely to result in an increase in macitentan exposure at steady state similar to that seen with ketoconazole [see Drug Interactions (Strong CYP3A4 Inhibitors) ].Effect of macitentan on other drugsWarfarin: Macitentan once daily dosing did not alter the exposure to R- and S-warfarin or their effect on international normalized ratio (INR).Sildenafil: At steady-state, the exposure to sildenafil 20 mg t.i.d. increased by 15% during concomitant administration of macitentan 10 mg once daily. This change is not considered clinically relevant.
NONCLINICAL TOXICOLOGYCarcinogenesis, Mutagenesis, Impairment of FertilityCarcinogenesis : Carcinogenicity studies of 2 years’ duration did not reveal any carcinogenic potential at exposures 75-fold and 140-fold the human exposure (based on AUC) in male and female mice, respectively, and 8.3- and 42-fold in male and female rats, respectively.Mutagenesis: Macitentan was not genotoxic in a standard battery of in vitro and in vivo assays that included a bacterial reverse mutation assay, an assay for gene mutations in mouse lymphoma cells, a chromosome aberration test in human lymphocytes, and an in vivo micronucleus test in rats. Impairment of Fertility : Treatment of juvenile rats from postnatal Day 4 to Day 114 led to reduced body weight gain and testicular tubular atrophy at exposures 7-fold the human exposure. Fertility was not affected.Reversible testicular tubular dilatation was observed in chronic toxicity studies at exposures greater than 7-fold and 23-fold the human exposure in rats and dogs, respectively. After 2 years of treatment, tubular atrophy was seen in rats at 4-fold the human exposure. Macitentan did not affect male or female fertility at exposures ranging from 19- to 44-fold the human exposure, respectively, and had no effect on sperm count, motility, and morphology in male rats. No testicular fi ndings were noted in mice after treatment up to 2 years.
Animal ToxicologyIn dogs, macitentan decreased blood pressure at exposures similar to the therapeutic human exposure. Intimal thickening of coronary arteries was observed at 17-fold the human exposure after 4 to 39 weeks of treatment. Due to the species-specifi c sensitivity and the safety margin, this fi nding is considered not relevant for humans.There were no adverse liver findings in long-term studies conducted in mice, rats, and dogs at exposures of 12- to 116-fold the human exposure.
Manufactured for: Actelion Pharmaceuticals US, Inc.5000 Shoreline Court, Ste. 200 South San Francisco, CA 94080, USAACT20131018
Reference: 1. OPSUMIT full Prescribing Information. Actelion Pharmaceuticals US, Inc. October 2013. ® OPSUMIT is a registered trademark of Actelion Pharmaceuticals, Ltd. © 2013 Actelion Pharmaceuticals US, Inc. All rights reserved. MAC-00217 1013
SildenafilCmax
AUCtau
Cmax
0.0 0.5 1.0 1.5 2.0 2.5 0.0 0.5 1.0 1.5
AUCinf
Ctrough
AUCtau
Ctrough
AUCtau
Cyclosporine-A
Ketoconazole
Avoid
Avoid
Change relative to macitentan alone Change relative to macitentan alone
No dose adjustment
No dose adjustment
Rifampin
MacitentanPoint estimate and 90% CI
Active metabolitePoint estimate and 90% CIInteracting drug Recommendation
OPSUMIT® (macitentan) OPSUMIT® (macitentan)

NEWS TO USE
New! Diagnostic NotepadA new Diagnostic Notepad developed bymembers of the Early Diagnosis Cam-paign is now available for request byPHA members. Each page containsimages of the heart and lungs and spaceto record notes and test results, and isdesigned to provide a visual aid for con-versations with your patients. The backof each page also contains links toPHA’s web resources. For moreinformation, please [email protected].(35 sheets/pad)
PHA’s 2015 PHPN Symposium:SUBMIT AN ABSTRACT!PHA’s 2015 PH Professional NetworkSymposium will be held September17-19, 2015 in Arlington, Va. This is anevent primarily for nurses, nurse practi-tioners, physician assistants, pharmacists,respiratory therapists, social workers, andother healthcare professionals. Attendeeswill have the opportunity to networkwith other healthcare professionals atSymposium meet-ups and committeegatherings and earn continuing educationcredits. Abstracts or case studies for the
Symposium Poster Session must besubmitted by May 15, 2015.For more about abstracts visitwww.PHAssociation.org/Symposium/Abstracts. Registration for attending thesymposium opens March 2015.
New! Courses on PHA OnlineUniversity:Drugs, Toxins, and PAHRoham Zamanian, MD, Stanford Uni-
versitywww.PHAOnlineUniv.org/
DrugsToxinsPAH1. Discuss drugs and toxins that are def-
inite and likely risk factors for PAH2. Explain how selective serotonin
reuptake inhibitor use is related toPAH
3. Describe possible mechanisms for thedevelopment of drug-and-toxin-related PAH
Gender and PAHEric Austin, MD, Vanderbilt Universitywww.PHAOnlineUniv.org/
GenderAndPAH1. Identify the major risk factors for
PAH
2. Recognize how PAH disproportion-ately affects females, with morefemales currently affected for mosttypes of PAH
3. Recognize that while the prevalenceof PAH is higher among females,this does not necessarily mean thatfemales have more sever disease or amore rapid disease progression
Pulmonology Clinical VignettesVarious Authorswww.PHAOnlineUniv.org/
PulmonologyClinicalVignettes1. Discuss the hemodynamic, echocar-
diographic and clinical factorsassociated with Group 3 pulmonaryhypertension
2. Identify clinical and pathologicalfindings in pulmonary veno-occlusivedisease
3. Evaluate the hemodynamic profile ofportopulmonary hypertension andother high flow conditions
4. Elucidate critical care management ofPulmonary Arterial Hypertensionpatient
ERRATUM
In “Ask the Expert” on page 92 of Volume 13, Number 2, the sentence beginning on the 15th line of the right-hand columnshould read: “In AMBITION, first-line treatment with a combination endothelin receptor antagonist (ERA, ambrisentan) andconcomitant phosphodiesterase type 5 inhibitor (PDE-5i, tadalafil) was compared with either medication alone as first-linetherapy for World Health Organization (WHO)/New York Heart Associaton (NYHA) functional class II-III symptoms.”
Advances in Pulmonary Hypertension regrets this error. The online version has been corrected and can be viewed athttp://www.phaonlineuniv.org/Journal
158 Advances in Pulmonary Hypertension Volume 13, Number 3; 2014

Be a part of PHA. Join one of PHA’s medical memberships to directly connect with your
PH-treating colleagues and to take advantage of the unique educational offerings available to members.
JO I N N O W! 301-565-3004W W W.PHAS S O C I A T I O N.O R G/ME D I C A LME M B E R S H I P
Be a part of PHA.Be a part of PHA.Be a part of PHA Join one of PHA’s medical memberships Join one of PHA’s medical memberships
PH Clinicians and Researchersphysicians and PhD-level researchers interested in pulmonary hypertension
PH Professional NetworkRNs, NPs, PAs, respiratory therapists,
pharmacists, social workers and other allied
BENEFITS INCLUDE:
Receive unlimited access to PHA Online University, the premieronline resource for PH education and CE-accredited courses about the diagnosis, treatment and advanced management of PH
Sessions at a discounted price
Host a Building Medical Education in PH event at your institutionH
through with PHA’s monthly e-newsletter PH Roundup
Keep abreast of news and information on the entire PH community in Pathlight, PHA’s quarterly newsletter
Connect directly with hundreds of knowledgeable PH-treatingcolleagues with PHCR and PHPN email groups
Through Education, Research and Advocacy
SETTING THE PACE IN THE PH
RACE
An educational and networking event for PH-treating healthcare professionalsAn educational and n
2015 Symposium Highlights:
• althcare professionals at meet-ups and committee gatherings. NeNeeNNNeNeNeNeNeNeNeNeNeNeNeNeeeeeeeNeeetwtwwwwwwwwwwwwoorooooooooooooo k with oththhhhhhhhhhhhhhhhhhhhhhhhhhhhher hea
• tion credits through multi-disciplinary education sessions led by Earnrnrn c cccccccccooononoooooonooooooooonooooooo tinuing eeddeddeeeeeeeede ucat
• case study for the Symposium Poster Session. SSuSuSSuSuSuSuSSSuSuSuSuSSSSuSSuSuSSuSSSSSuSSSSSSSSSSuSSSSuSSuSSSuuuuuuubmbbb it aaaaan abbbbbbbststststtststststststtstststtststsssss rrrrar ct or c
For more information and the latest updates visit: www.PHAssociation.org/Symposium
19, 2015Septeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeemmmmbbbbbbbbbbbbbbbbbbbbber 17 – l GatewayMarrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrriottttttttttttttttttttttttttttttttttttt Crystal
Arllllllllllllllllliiiiiiiiiiiiiiiiiiiiiiiiiingtoonnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnn, Va.
REGISTRATION OPENS
MARCH 2015!

The Pulmonary Hypertension Association and Caring Voice Coalition
have teamed up to create the Specialty Pharmacy Feedback Form – an opportunity for you and your patients to let SPs know what
they’re doing well and where they can improve.
Your comments will help improve PH patients’ access to their
prescribed treatments.
www.PHAssociation.org/SpecialtyPharmacyForm
DO YOU HAVE FEEDBACK FOR THE SPECIALTY PHARMACIES YOU WORK WITH?PHA’s Specialty Pharmacy Feedback Form is a resource for your PH team and your PH patient. Please share the information below.
HEALTH PROFESSIONALS
PHA’S EMPOWERED PATIENT ONLINE TOOLKIT
Available online at:www.PHAssociation.org/OnlineToolkit
The Empowered Patient Toolkit can help your patients:
PrPrepeparare for emergency situationsns
Track medicaatit ons and medical contn acts
Get the most outt o f doctors’ visits
Record symptoms ana d questions bettween appointmennnts
Keep insurance infoormation organizedd
Plan for travel
And more!
Any help that a patient or a caregiver can
get for tracking their medical
documents is great, because it can get
overwhelming.


To order additional copies, call or contact PHA at 1-866-474-4742 or www.PHAssociation.org. All issues of Advances in Pulmonary Hypertension are also available online at www.PHAOnlineUniv.org/Journal
Advances inPulmonary HypertensionPulmonary Hypertension Association801 Roeder Road, Suite 1000 Silver Spring, MD 20910-4496
New Application Deadline: February 12, 2015New Application Deadline: June 12, 2015
Resubmission Deadline: March 12, 2015Resubmission Deadline: July 12, 2015
Learn about all of PHA's research opportunities at
NON-PROFIT ORGUS POSTAGE PAIDPERMIT 476Bolingbrook, IL