Adrenocortical Hormones Prof. dr. Zoran Valić Department of Physiology University of Split School...

If you can't read please download the document
-
Upload
sabastian-janeway -
Category
Documents
-
view
230 -
download
2
Transcript of Adrenocortical Hormones Prof. dr. Zoran Valić Department of Physiology University of Split School...
- Slide 1
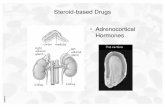
Adrenocortical Hormones Prof. dr. Zoran Vali Department of Physiology University of Split School of Medicine Slide 2 two adrenal glands, at the superior poles of the two kidneys (about 4g) 1) medulla central 20% (functionally related to the sympathetics epinephrine & norepinephrine) 2) cortex 80% (corticosteroids synthesized from the steroid cholesterol; similar chemical formulas) Slide 3 Slide 4 Mineralocorticoids, Glucocorticoids, and Androgens androgens of only slight importance, although extreme quantities can be secreted masculinizing effects MC affect electrolytes (minerals) of the extracellular fluids (Na + and K + ) GC increase BGC, but protein and fat also more than 30 steroids have been isolated two important: aldosterone and cortisol, Slide 5 Synthesis and Secretion of Adrenocortical Hormones adrenal cortex has three distinct layers: 1) zona glomerulosa thin layer underneath capsule, 15% of cortex, aldosterone synthase (angiotensin II and K + ) 2) zona fasciculata 75% of cortex, cortisol and corticosterone, small amounts of adrenal androgens and estrogens (ACTH) 3) zona reticularis deep layer of cortex, DHEA and androstenedione (ACTH, cortical androgen-stimulating hormone, ?) Slide 6 Slide 7 Slide 8 all human steroid hormones are synthesized from cholesterol cells can synthesize de novo cholesterol (from acetate), 80% comes from LDL cells coated pits endocytosis ACTH receptors for LDL and activity of enzymes LDL degradation cholesterol pregnenolone (desmolase, rate-limiting step, in mitochondria) Slide 9 Slide 10 90-95% of the cortisol in plasma binds to cortisol-binding globulin or transcortin, less to albumin long half-life (60-90 min) 60% of circulating aldosterone combined with plasma proteins (half-life 20 min) degraded in liver conjugation especially to glucuronic acid and sulfates (25% excreted in the bile, remaining by kidneys) Slide 11 Functions of Mineralocorticoids Aldosterone total loss of MC rapid in NaCl and in K + (death within 3 days without therapy), EC fluid volume and blood volume acute "lifesaving" hormones aldosterone 90% MC activity cortisol 3000x less activity, but 2000x concentration Slide 12 aldosterone reabsorption of Na + and secretion of K + (principal cells of the collecting tubules) aldosterone EC fluid volume & MAP, cNa + stays the same (osmotic absorption of water, stimulation of thirst) transient Na + retention occurs pressure natriuresis and pressure diuresis (ECF 5- 15% MAP 15 to 25 mmHg) Slide 13 Slide 14 aldosterone escape in the meantime hypertension develops when aldosterone secretion becomes zero large amounts of salt are lost and ECF severe extracellular fluid dehydration and low blood volume circulatory shock death Slide 15 excess aldosterone causes hypokalemia (from 4,5 to 2 mmol/L; transport into cells) and muscle weakness (alteration of the electrical excitability); too little aldosterone causes hyperkalemia and cardiac toxicity (rise of 60-100%, arrhythmia heart failure) excess aldosterone secretion of H + (intercalated cells of the cortical collecting tubules, metabolic alkalosis) Slide 16 aldosterone transport Na + & K + in sweat glands and salivary glands important in hot environments greatly enhances Na + absorption by the intestines, especially in the colon; in the absence diarrhea Slide 17 Slide 18 Cellular Mechanism of Aldosterone Action still not fully understood 1) lipid soluble diffuses readily to the interior of the tubular epithelial cells 2) in cytoplasm combines with a highly specific cytoplasmic mineralocorticoid receptor protein 3) aldosterone-receptor complex diffuses into the nucleus DNA RNA 4) mRNA diffuses back into the cytoplasm ribosomes protein formation Slide 19 one or more enzymes membrane transport proteins for Na +, K +, H + especially increases Na + /K + -ATPaze which serves as the principal part of the pump for Na + & K + exchange at the basolateral membranes of the renal tubular cells increases epithelial sodium channel (ENaC) protein inserted into the luminal membrane Slide 20 sequence of events (30-45 minimal, maximal effect after several hours) possible nongenomic actions increase formation of cAMP (fast less than 2 minutes), but also involves phosphatidylinositol second messenger system Slide 21 Slide 22 Regulation of Aldosterone Secretion deeply intertwined with the regulation of ECF electrolyte concentrations, volume of ECF, blood volume and MAP almost entirely independent of the regulation of cortisol and androgens 1) K + in ECF 2) angiotensin II concentration in ECF 3) Na + in ECF very slightly decreases 4) ACTH necessary for secretion, not for control Slide 23 in turn, the aldosterone acts on the kidneys: 1) help them excrete the excess K + 2) increase the blood volume and MAP effects of Na + & ACTH usually minor (total absence of ACTH can significantly reduce aldosterone secretion "permissive" role) Slide 24 Slide 25 Functions of Glucocorticoids MC can save the life of an acutely adrenalectomized animal, metabolic systems remain considerably deranged animal cannot resist physical or even mental stress (infection = death) on a long run GC equally important as MC 95% of activity cortisol (hydrocortisone) smaller effect corticosterone Slide 26 Effects of Cortisol on Carbohydrate Metabolism stimulation of gluconeogenesis ( 6-10x) enzymes required to convert amino acids into glucose mobilization of amino acids from the extrahepatic tissues mainly from muscle increase in glycogen storage in the liver cells glucose utilization by cells cause of this decrease is unknown depress the oxidation of NADH to form NAD + Slide 27 BGC & adrenal diabetes rate of gluconeogenesis & rate of glucose utilization high levels of GC reduce the sensitivity of many tissues to insulin unknown, high levels of fatty acids BGC greater of 50% adrenal diabetes (tissues are resistant to the effects of insulin) Slide 28 Effects of Cortisol on Protein Metabolism of the protein stores in all body cells except those of the liver synthesis & catabolism decreased amino acid transport into extrahepatic tissues; formation of RNA and subsequent protein synthesis (muscle and lymphoid tissue) liver and plasma proteins (from liver) enhancement of amino acid transport into liver cells the liver enzymes for protein synthesis Slide 29 AA in blood, transport into extrahepatic cells, transport into hepatic cells transport into muscle cells (isolated tissues) synthesis of protein in those cells catabolism continues normally mobilization of AA from the nonhepatic tissues increasing the liver enzymes required for the hepatic effects Slide 30 Effects of Cortisol on Fat Metabolism mobilization of fatty acids from adipose tissue free fatty acids in the plasma and their utilization for energy enhance the oxidation of fatty acids in the cells mechanism unknown, diminished transport of glucose ( -glycerophosphate) in times of starvation or other stresses shift to utilization of fatty acids for energy (requires several hours to develop) Slide 31 obesity caused by excess cortisol peculiar type of obesity (despite fatty acid mobilization) deposition of fat in the chest (buffalo-like torso) and head regions (moon face) obesity results from excess stimulation of food intake fat being generated more rapidly than mobilized and oxidized Slide 32 Cortisol Is Important in Resisting Stress and Inflammation physical or neurogenic stress marked in ACTH secretion by anterior pituitary gland within minutes secretion of cortisol Slide 33 Slide 34 1) trauma of almost any type 2) infection 3) intense heat or cold 4) injection of norepinephrine 5) surgery 6) injection of necrotizing substances beneath skin 7) restraining an animal so that it cannot move 8) almost any debilitating disease Slide 35 unknown why cortisol secretion is of significant benefit GC cause rapid mobilization of amino acids and fats from cellular stores release of energy and glucose synthesis use of amino acids in damaged tissues synthesis of purines, pyrimidines, and creatine phosphate from amino acids preferential mobilization of labile proteins Slide 36 Anti-Inflammatory Effects of High Levels of Cortisol trauma or infection inflammation inflammation can be more damaging than trauma or disease itself (rheumatoid arth.) cortisol: 1) block the early stages of the inflammation process before inflammation even begins 2) rapid resolution of the inflammation and increased rapidity of healing Slide 37 1) stabilization of lysosomal membranes proteolytic enzymes 2) decreased permeability of the capillaries secondary 3) decreased migration of white blood cells into the inflamed area and phagocytosis of the damaged cells prostaglandins and leukotrienes 4) suppression of immune system lymphocyte reproduction 5) attenuation of fever release of interleukin-1 Slide 38 reducing all aspects of inflammatory process block most of the factors that promote the inflammation rate of healing is enhanced (mobilization of amino acids, increased glucogenesis, increased amounts of fatty acids) useful in: rheumatoid arthritis, rheumatic fever, and acute glomerulonephritis Slide 39 blocks the inflammatory response to allergic reactions anaphylaxis decreases the number of eosinophils and lymphocytes in the blood; decreases the output of both T cells and antibodies (fulminating tuberculosis / preventing immunological rejection) increases the production of red blood cells Slide 40 cortisol binds with its protein receptor in the cytoplasm easily diffuse through the cell membrane hormone-receptor complex interacts with glucocorticoid response elements at DNA transcription rapid nongenomic effects Slide 41 Slide 42 Regulation of Cortisol Secretion ACTH (corticotropin or adrenocorticotropin) enhances secretion of cortisol ACTH is a large polypeptide of 39 amino acids (24 has all effects of total molecule) corticotropin-releasing factor (CRF, 41 amino acids, paraventricular nucleus) Slide 43 ACTH activate adenylyl cyclase cAMP (in 3 min), activation of the protein kinase A initial conversion of cholesterol to pregnenolone (rate-limiting step) ACTH hypertrophy and proliferation of the adrenocortical cells in the zona fasciculata and zona reticularis physical or mental stress ACTH Slide 44 Slide 45 cortisol has direct negative feedback effects: hypothalamus CRH anterior pituitary gland ACTH stress stimuli are the prepotent circadian rhythm of glucocorticoid secretion measurements of blood cortisol levels Slide 46 Slide 47 when ACTH is secreted several other hormones are secreted simultaneously (preprohormone POMC) melanocyte-stimulating hormone (MSH), - lipotropin and -endorphin under normal conditions small secretion MSH stimulates formation of the black pigment melanin (pars intermedia in some lower animals, ACTH is normally more important than MSH in determining the amount of melanin in the skin in humans) Slide 48 Slide 49 Adrenal Androgens especially during fetal life most important dehydroepiandrosterone in female: growth of pubic and axillary hair some of the adrenal androgens are converted to testosterone in extra-adrenal tissues Slide 50 Abnormalities of Adrenocortical Secretion hypoadrenalism (adrenal insufficiency) Addison's disease hyperadrenalism Cushing's syndrome primary aldosteronism Conn's syndrome adrenogenital syndrome Slide 51 Hypoadrenalism Addison's disease adrenal cortices do not produce hormones most frequently caused by primary atrophy or injury of the adrenal cortices in 80% autoimmunity, tuberculosis, or cancer lack of MC ECF volume, hyponatremia, hyperkalemia & mild acidosis plasma volume, Ht, CO death (shock, 4 days) lack of GC disturbances in BGC, fats and proteins sluggishness of energy mobilization; deteriorating effects of different types of stress Slide 52 melanin pigmentation of the mucous membranes and skin melanin is not always deposited evenly but occasionally is deposited in blotches (thin skin areas lips and the thin skin of the nipples) tremendous rates of ACTH & MSH secretion due to normal negative feedback treatment daily administration of small quantities of MC & GC Slide 53 Slide 54 Slide 55 Hyperadrenalism Cushing's Syndrome hypersecretion by adrenal cortex (adenomas of anterior pituitary, abnormal function of hypothalamus, "ectopic secretion" of ACTH by a tumor, adenomas of adrenal cortex) adenomas of anterior pituitary Cushing's disease dexamethasone test (incorrect diagnosis) iatrogenic Cushing's syndrome fat deposition buffalo torso, "moon face", acne and hirsutism, 80% hypertension Slide 56 increase in BGC after meals to 11 mmol/L (enhanced gluconeogenesis and decreased glucose utilization) greatly decreased tissue proteins everywhere in the body with the exception of liver and plasma severe weakness, suppressed immune system, large purplish striae (collagen), osteoporosis treatment removal of a tumor (before drugs that block steroidogenesis) Slide 57 Slide 58 Slide 59 Primary Aldosteronism Conn's Syndrome small tumor of the zona glomerulosa cells secretes large amounts of aldosterone hypokalemia, mild metabolic alkalosis, ECF volume & blood volume, hypertension occasional periods of muscle paralysis caused by the hypokalemia (depressant effect of hypokalemia on action potential transmission) diagnostic criteria decreased plasma renin treatment surgical removal of the tumor Slide 60 Adrenogenital Syndrome tumor secretes excessive quantities of androgens intense masculinizing effects in a female: growth of a beard, a much deeper voice, occasionally baldness, masculine distribution of hair on the body and the pubis, growth of the clitoris in prepubertal male: early masculinization in adult male: difficult to make a diagnosis excretion of 17-ketosteroids in the urine increase Slide 61 Slide 62 etverogodinji djeak