+ Offline Optimal Ads Allocation in SNS Advertising Hui Miao, Peixin Gao.
Upload
clifton-atkinsonCategory
view
215download
1
Adoption of an Electronic Medical Record-Based Decision
Support Tool for Otitis Media
Alexander G. Fiks, MD, MSCE, Peixin Zhang, PhD, A. Russell Localio, PhD, Robert W. Grundmeier, MD, Charles Bailey, MD, PhD, Saira Khan, MPH, James Massey, RN, Stephanie Mayne, MHS, Evaline A. Alessandrini, MD, MSCE, Christopher B. Forrest, MD, PhD

DISCLOSURE STATEMENT Speaker: Alexander Fiks
Dr. Fiks is a co-inventor of the “Care Assistant” that was used to provide clinical decision support in this study. He holds no patent on the software and to date has earned no money from this invention.

Unapproved or Off-Label Disclosures for
Alexander Fiks
Presenter: I have documented that my presentation will not involve discussion of unapproved or off-label, experimental or investigational use.

Background
Physicians commonly fail to adhere to practice guidelines
Clinical decision support (CDS) systems provide intelligently filtered, appropriately timed, and actionable information to clinicians at the point of care
Such systems help overcome barriers to guideline-based treatment
However, like guidelines themselves, CDS systems are commonly ignored

Background
Otitis Media (OM) is one of the most common disorders in childhood
Acute Otitis Media (AOM): Active infection
Otitis Media with Effusion (OME): Fluid in the middle ear without active infection
OM is the third most common reason for a pediatric office visit and is the principal diagnosis in up to 12% of all office visits
The AAP, CDC, and AHRQ have developed guidelines for OM; however, studies have shown that adherence to guidelines remains low

Study Objectives
Within the context of a randomized clinical trial of an EHR-based CDS tool designed to improve OM guidelines:
1) To assess the impact of performance feedback on adoption of CDS
2) Measure the impact of CDS use on quality of care
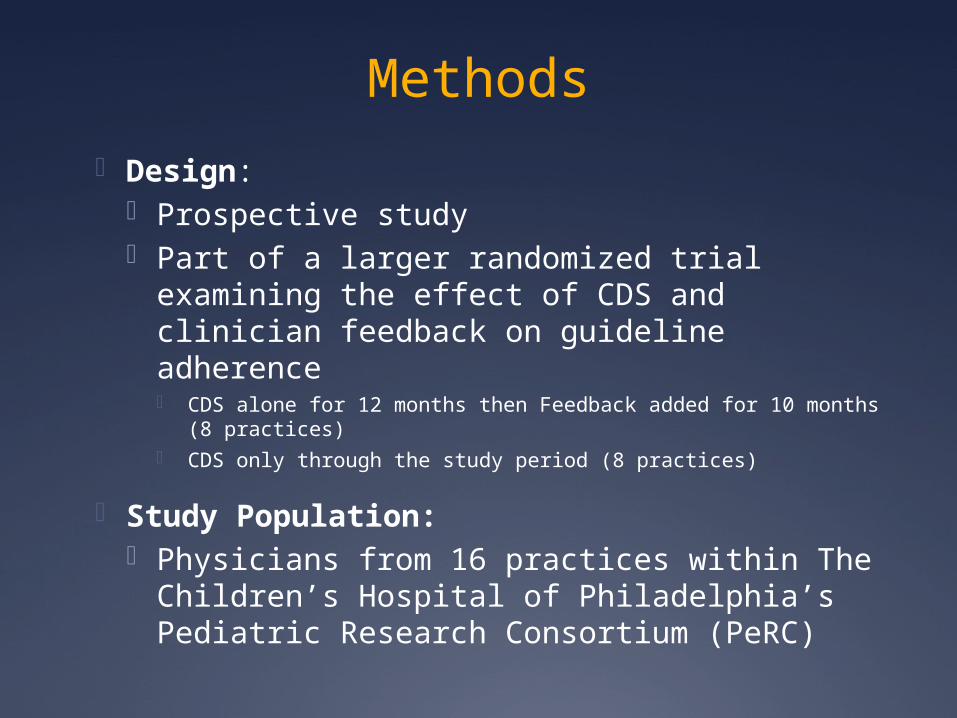
Methods
Design: Prospective study Part of a larger randomized trial examining
the effect of CDS and clinician feedback on guideline adherence CDS alone for 12 months then Feedback added for 10 months
(8 practices) CDS only through the study period (8 practices)
Study Population: Physicians from 16 practices within The
Children’s Hospital of Philadelphia’s Pediatric Research Consortium (PeRC)

Clinical Decision Support System
Developed by research team for the randomized clinical trial
Delivered using a web service
Appears seamlessly in the electronic health record for children with current ear complaints or history of OM care
Practices were trained regarding CDS use and OM guidelines in 1-hour, in-person sessions lead by pediatricians on the research team

Visual Display of OM Events during past 24 months
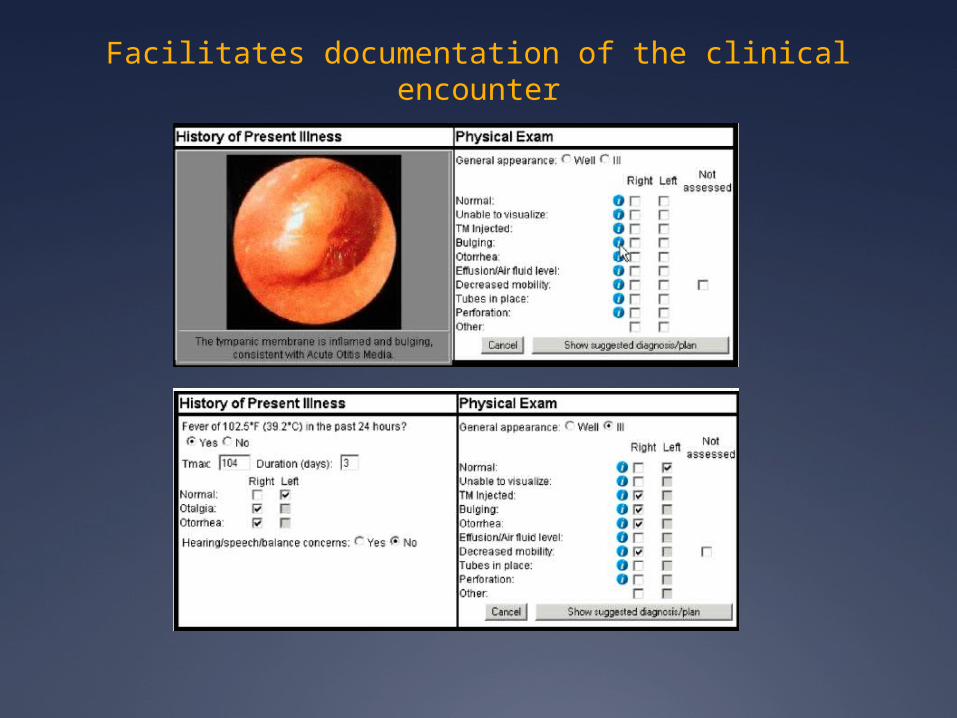
Facilitates documentation of the clinical encounter
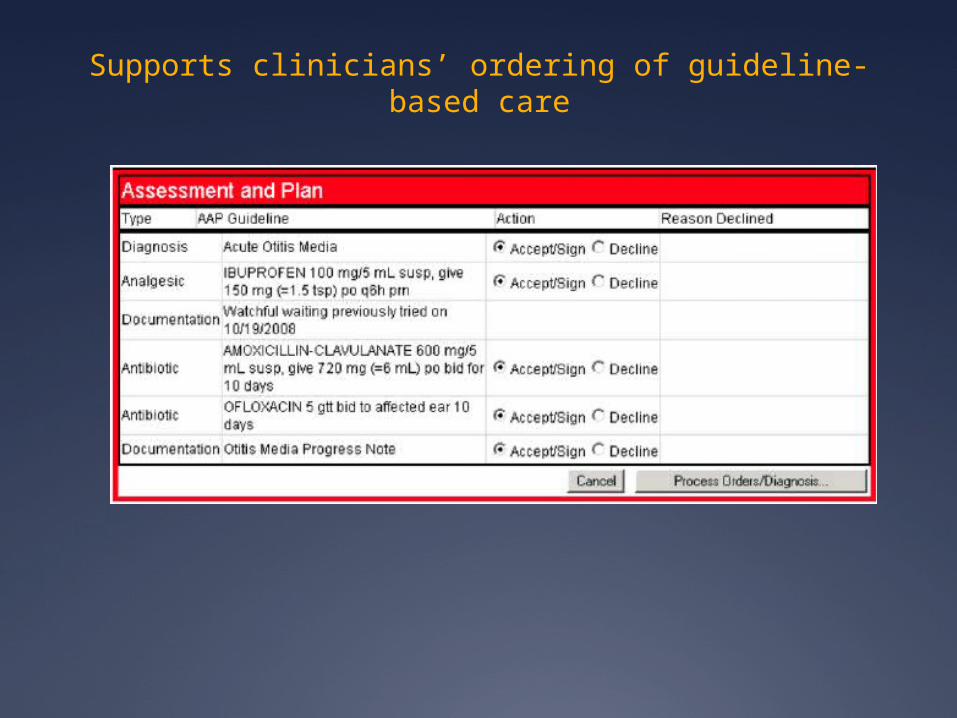
Supports clinicians’ ordering of guideline-based care

Clinician Feedback After 12 months of CDS
only, practices were cluster-randomized to receive feedback or not
Feedback documented physicians’ level of CDS use and monthly adherence to OM guidelines, change in adherence over time, and compared to others in their practice and health system

Methods
Aim 1: Outcome: Physician use of the decision support
tool at eligible visits Exposure: Absence or presence of feedback
Aim 2 Outcome: Adherence to OM Guidelines Exposure: CDS Use
Covariates: Visit, clinician, and patient-level characteristics
Study Sample: 41,391 visits at 16 practices with 108 clinicians

Overall CDS Use Frequency
-Clinicians used the CDS at a mean of 21.3% of eligible visits (median: 8.8%, range: 0-84.8%)-Practices used the CDS at a mean of 16.8% of eligible visits (median: 15.1%, range 0-51%)

Characteristics Associated with CDS Use
CDS more likely to be used by clinicians who diagnose OM less frequently (25% vs. 14% of visits, p=0.05)
CDS more likely to be used at visits with less complexity Sick visits versus preventive (17% vs. 8%, p<0.001) Visits with 1 diagnosis compared to 6 or more (21%
vs. 9%, p<.01) Children >24 months or age compared to those <6
months of age (18% vs. 14%, p=0.02)
CDS more likely to be used when an action was needed Visits with AOM (antibiotic ordering) versus OME (18%
vs. 13%, p<0.001)
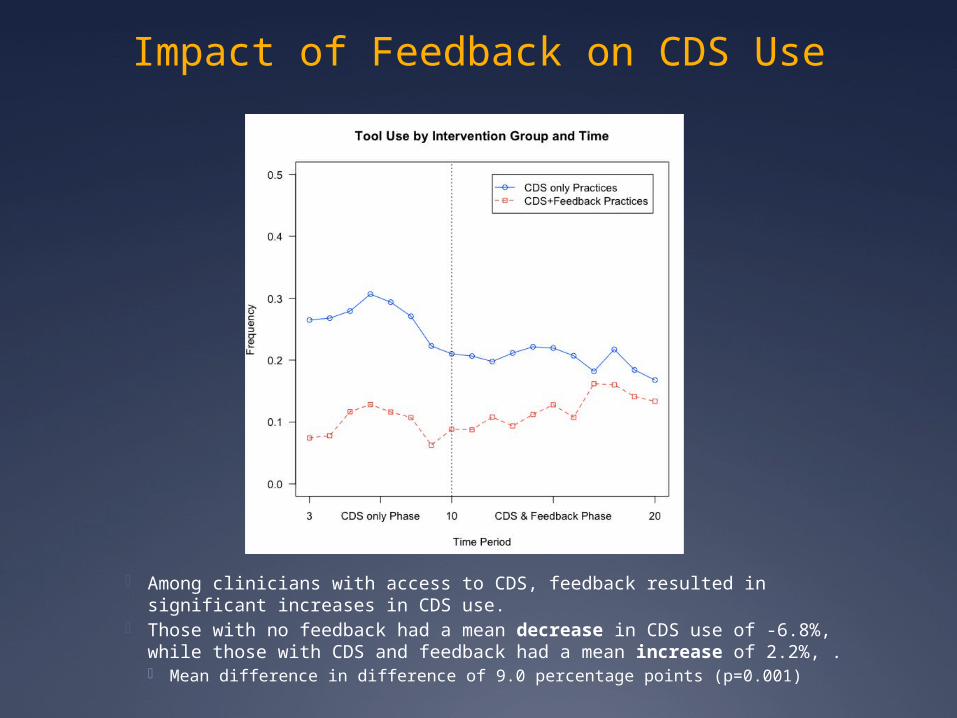
Impact of Feedback on CDS Use
Among clinicians with access to CDS, feedback resulted in significant increases in CDS use.
Those with no feedback had a mean decrease in CDS use of -6.8%, while those with CDS and feedback had a mean increase of 2.2%, . Mean difference in difference of 9.0 percentage points (p=0.001)

Impact of CDS Use on OM Guideline Adherence
For all OM: 48% relative increase in pain treatment (p<0.001)
For AOM: 5% increase in use of amoxicillin as a first-line therapy
(p=0.007) 5% increase in appropriate antibiotic for penicillin-allergic
patients (p=0.04) 17% increase in high dose amoxicillin (p=0.02)
For OME: 12% increase in adequate diagnostic evaluation (p=0.01)
Comprehensive Quality Measures: For visits at which at least 3 quality measures were relevant,
there was an increase in perfect care for AOM and OME (8%, p<0.001 and 9%, p=0.01, respectively)

For Whom is CDS Most Effective
We divided our sample of clinicians into those with low, medium, and high guideline adherence at baseline (tertiles).
CDS improved adherence in all groups
Clinicians with low adherence at baseline improved to the greatest extent 70% increase in pain treatment for low vs. 13% improvement
for high 30% increase in adequate AOM diagnostic documentation for
low vs. 12% decrease for high
Clinicians with low adherence also improved for the most metrics Improvement in 6/12 metrics for low vs. 4/12 for high

Limitations This study was conducted at a single health care
network in one region of the country
The study is not an evaluation of a clinical trial as randomized, but a description of CDS adoption among the study arm randomized to receive CDS
The limited time frame of the study prevents full understanding of: how long feedback programs can influence provider
behavior change what happens when feedback is removed how long feedback must persist to achieve optimal
effect

Study Conclusions
Even effective CDS is often ignored
Implementing clinician feedback along with CDS increases CDS adoption
CDS, when used, improves the quality of care for OM
Benefits are greatest for clinicians with low baseline quality
Results support the overall importance of CDS adoption for improving guideline adherence and the use of feedback to increase CDS adoption

Acknowledgements
We thank the network of primary care physicians, their patients and families for their contribution to clinical research through the Pediatric Research Consortium (PeRC) at CHOP.
This project was supported by the Agency for Healthcare Research and Quality (R18 HS017042) and the Eunice Kennedy Shriver National Institute of Child Health & Human Development (K23 HD059919) (AGF).

Questions?