Acute renal failure in intensive care
3
INTENSIVE CARE © 2006 Elsevier Ltd 116 ANAESTHESIA AND INTENSIVE CARE MEDICINE 7:4 Acute renal failure (ARF) is a common problem in the ICU, with an incidence of 10–25%. In the critically ill, its cause is usually multifactorial, and it is best considered a syndrome rather than a specific disease. Definition ARF is diagnosed clinically as sudden renal impairment with con- comitant electrolyte, acid–base and fluid balance derangement. The physiology of the kidney is described in Anaesthesia and Intensive Care Medicine 4:7. Classically the criteria have been oliguria (a fall in urine volume to less than 500 ml/day), rising plasma urea and creatinine concentrations, and rising plasma potassium and phosphate levels. ARF may also occur with normal urine flow, when it is associated with an improved prognosis. Creatinine is a more accurate marker of ARF than urea, which can be raised by dehydration, or breakdown of soft tissue or gastrointestinal blood. Serum creatinine is not usually raised above normal until there is a 50% reduction in glomerular filtration rate (GFR). Creatinine production is related to lean body mass, and can be markedly raised by rhabdomyolysis. More precise definition of ARF has proved difficult. The Acute Dialysis Quality Initiative has proposed a multilevel classification system with the acronym RIFLE (Risk of renal dysfunction, Injury to the kidney, Failure or Loss of kidney function, and End-stage kidney disease) (Figure 1). The RIFLE criteria were only intended to be used as a definition for ARF, but have been applied to clinical evaluation. Several groups have found the clinical severity of the RIFLE criteria to correlate with increasing mortality. Patients in the RIFLE-F category appear to have a significantly higher mortal- ity than those in the RIFLE-R and RIFLE-I categories. The RIFLE classification does not include details of the underlying disease leading to ICU admission, nor the severity of illness scores at the time of onset of ARF. Clinical classification The traditional classification of renal failure has been into pre-renal, intrarenal, and post-renal. Pre-renal occurs when the renal perfusion pressure falls below the autoregulatory threshold for maintenance of normal GFR. Hypovolaemia, hypotension, poor cardiac output, or excessive vasodilatation are the principal causes. Localized lesions may also reduce perfusion, such as renal artery stenosis. In pre-renal failure, patients produce concentrated urine with relatively low sodium content, and respond to optimization of haemodynamic parameters. The exception to this is the hepatorenal syndrome for which treatment of the hepatic failure is needed. Intrarenal, intrinsic, or parenchymal may be glomerular or tubulointerstitial. Acute glomerulonephritis from a variety of causes may cause ARF. Tubulointerstitial causes are more common, mostly due to nephrotoxins or ischaemia leading to acute tubular necrosis. Intrinsic renal failure is associated with isotonic urine that has a high sodium concentration, and possibly an active urinary sedi- ment if a glomerulonephritis is present. Post-renal or obstructive: intraluminal or extraluminal obstruction at any site from the collecting tubules to the urethra may cause ARF. If obtained, the urine is isotonic and high in sodium. Patients with absolute anuria should always be assumed to have an obstructive cause until proved otherwise. Check for a blocked catheter in such circumstances. The post-renal pathologies need surgical assess- ment and have a different natural history from the more common pre-renal and intrarenal insults seen on ICU. Imaging is required initially with ultrasound. The abdominal compartment syndrome should be considered in patients who develop oliguria following abdominal surgery. If intra-abdominal pressure exceeds 25 mm Hg from accumulation of blood, gut oedema or tense ascites, renal blood flow is impaired and oliguria may occur. Treatment may require surgical abdominal decompression. Acute renal failure in intensive care Jonathan Ingham Jonathan Ingham is Consultant in Critical Care Medicine and Anaesthesia at Torbay Hospital, Devon, UK. He qualified from Oxford University and trained in anaesthesia and intensive care in Portsmouth, Plymouth and Perth, Australia. RIFLE classification of acute renal failure proposed by the Acute Dialysis Quality Initiative GFR criteria Urine output criteria Risk ↑Creatinine x 1.5 or GFR↓ > 25% Urine output < 0.5 ml/kg/hour for 6 hours Injury ↑Creatinine x 2 or GFR↓ > 50% Urine output < 0.5 ml/kg/hour for 12 hours Failure ↑Creatinine x 3 or absolute value > 350 µmol/l with acute rise of 44 µmol/litre or GFR↓ > 75% Urine output < 0.3 ml/kg/hour for 24 hours or anuria for 12 hours Loss Persistent acute renal failure Complete loss of kidney function > 4 weeks End-stage kidney disease Complete loss of kidney function > 3 months 1
-
Upload
jonathan-ingham -
Category
Documents
-
view
214 -
download
1
Transcript of Acute renal failure in intensive care

INTENSIVE CARE
© 2006 Elsevier Ltd116ANAESTHESIA AND INTENSIVE CARE MEDICINE 7:4
Acute renal failure (ARF) is a common problem in the ICU, with an incidence of 10–25%. In the critically ill, its cause is usually multifactorial, and it is best considered a syndrome rather than a specific disease.
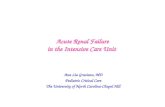
DefinitionARF is diagnosed clinically as sudden renal impairment with con-comitant electrolyte, acid–base and fluid balance derangement. The physiology of the kidney is described in Anaesthesia and Intensive Care Medicine 4:7. Classically the criteria have been oliguria (a fall in urine volume to less than 500 ml/day), rising plasma urea and creatinine concentrations, and rising plasma potassium and phosphate levels. ARF may also occur with normal urine flow, when it is associated with an improved prognosis. Creatinine is a more accurate marker of ARF than urea, which can be raised by dehydration, or breakdown of soft tissue or gastrointestinal blood. Serum creatinine is not usually raised above normal until there is a 50% reduction in glomerular filtration rate (GFR). Creatinine production is related to lean body mass, and can be markedly raised by rhabdomyolysis. More precise definition of ARF has proved difficult. The Acute Dialysis Quality Initiative has proposed a multilevel classification system with the acronym RIFLE (Risk of renal dysfunction, Injury to the kidney, Failure or Loss of kidney function, and End-stage kidney disease) (Figure 1). The RIFLE criteria were only intended to be used as a definition for ARF, but have been applied to clinical evaluation. Several groups have found the clinical severity of the RIFLE criteria to correlate with increasing mortality. Patients in the RIFLE-F category appear to have a significantly higher mortal-ity than those in the RIFLE-R and RIFLE-I categories. The RIFLE classification does not include details of the underlying disease leading to ICU admission, nor the severity of illness scores at the time of onset of ARF.
Clinical classification The traditional classification of renal failure has been into pre-renal, intrarenal, and post-renal.
Pre-renal occurs when the renal perfusion pressure falls below the autoregulatory threshold for maintenance of normal GFR. Hypovolaemia, hypotension, poor cardiac output, or excessive vasodilatation are the principal causes. Localized lesions may also reduce perfusion, such as renal artery stenosis. In pre-renal failure, patients produce concentrated urine with relatively low sodium content, and respond to optimization of haemodynamic parameters. The exception to this is the hepatorenal syndrome for which treatment of the hepatic failure is needed.
Intrarenal, intrinsic, or parenchymal may be glomerular or tubulointerstitial. Acute glomerulonephritis from a variety of causes may cause ARF. Tubulointerstitial causes are more common, mostly due to nephrotoxins or ischaemia leading to acute tubular necrosis. Intrinsic renal failure is associated with isotonic urine that has a high sodium concentration, and possibly an active urinary sedi-ment if a glomerulonephritis is present.
Post-renal or obstructive: intraluminal or extraluminal obstruction at any site from the collecting tubules to the urethra may cause ARF. If obtained, the urine is isotonic and high in sodium. Patients with absolute anuria should always be assumed to have an obstructive cause until proved otherwise. Check for a blocked catheter in such circumstances. The post-renal pathologies need surgical assess-ment and have a different natural history from the more common pre-renal and intrarenal insults seen on ICU. Imaging is required initially with ultrasound. The abdominal compartment syndrome should be considered in patients who develop oliguria following abdominal surgery. If intra-abdominal pressure exceeds 25 mm Hg from accumulation of blood, gut oedema or tense ascites, renal blood flow is impaired and oliguria may occur. Treatment may require surgical abdominal decompression.
Acute renal failure in intensive care Jonathan Ingham
Jonathan Ingham is Consultant in Critical Care Medicine and Anaesthesia
at Torbay Hospital, Devon, UK. He qualified from Oxford University and
trained in anaesthesia and intensive care in Portsmouth, Plymouth and
Perth, Australia.
RIFLE classification of acute renal failure proposed by the Acute Dialysis Quality Initiative
GFR criteria Urine output criteria
Risk ↑Creatinine x 1.5 or GFR↓> 25%
Urine output < 0.5
ml/kg/hour for
6 hours
Injury ↑Creatinine x 2 or
GFR↓ > 50%
Urine output < 0.5
ml/kg/hour for
12 hours
Failure ↑Creatinine x 3 or
absolute value > 350
µmol/l with acute rise of
44 µmol/litre or GFR↓ > 75%
Urine output < 0.3
ml/kg/hour for 24
hours or anuria for 12
hours
Loss Persistent acute renal failure
Complete loss of kidney function > 4 weeks
End-stage kidney disease
Complete loss of kidney function > 3 months
1
INTENSIVE CARE
© 2006 Elsevier Ltd117ANAESTHESIA AND INTENSIVE CARE MEDICINE 7:4
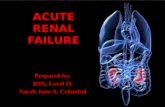
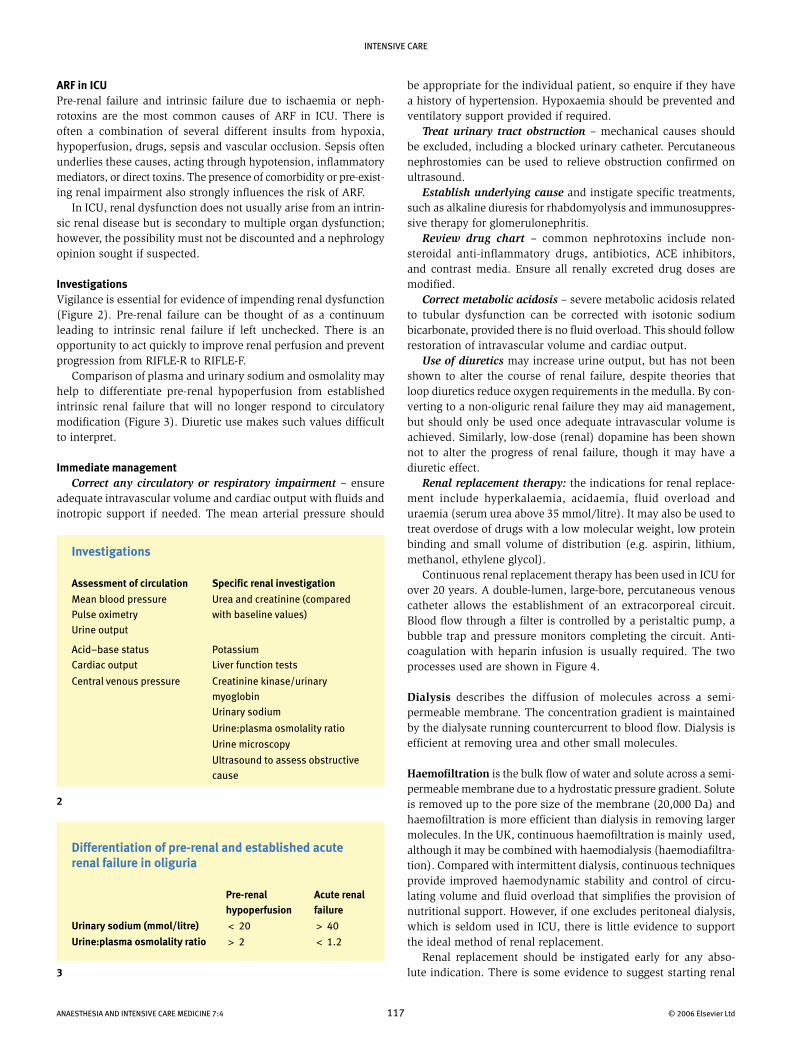
be appropriate for the individual patient, so enquire if they have a history of hypertension. Hypoxaemia should be prevented and ventilatory support provided if required. Treat urinary tract obstruction – mechanical causes should be excluded, including a blocked urinary catheter. Percutaneous nephrostomies can be used to relieve obstruction confirmed on ultrasound. Establish underlying cause and instigate specific treatments, such as alkaline diuresis for rhabdomyolysis and immunosuppres-sive therapy for glomerulonephritis. Review drug chart – common nephrotoxins include non-steroidal anti-inflammatory drugs, antibiotics, ACE inhibitors, and contrast media. Ensure all renally excreted drug doses are modified. Correct metabolic acidosis – severe metabolic acidosis related to tubular dysfunction can be corrected with isotonic sodium bicarbonate, provided there is no fluid overload. This should follow restoration of intravascular volume and cardiac output. Use of diuretics may increase urine output, but has not been shown to alter the course of renal failure, despite theories that loop diuretics reduce oxygen requirements in the medulla. By con-verting to a non-oliguric renal failure they may aid management, but should only be used once adequate intravascular volume is achieved. Similarly, low-dose (renal) dopamine has been shown not to alter the progress of renal failure, though it may have a diuretic effect. Renal replacement therapy: the indications for renal replace-ment include hyperkalaemia, acidaemia, fluid overload and uraemia (serum urea above 35 mmol/litre). It may also be used to treat overdose of drugs with a low molecular weight, low protein binding and small volume of distribution (e.g. aspirin, lithium, methanol, ethylene glycol). Continuous renal replacement therapy has been used in ICU for over 20 years. A double-lumen, large-bore, percutaneous venous catheter allows the establishment of an extracorporeal circuit. Blood flow through a filter is controlled by a peristaltic pump, a bubble trap and pressure monitors completing the circuit. Anti-coagulation with heparin infusion is usually required. The two processes used are shown in Figure 4.
Dialysis describes the diffusion of molecules across a semi-permeable membrane. The concentration gradient is maintained by the dialysate running countercurrent to blood flow. Dialysis is efficient at removing urea and other small molecules.
Haemofiltration is the bulk flow of water and solute across a semi-permeable membrane due to a hydrostatic pressure gradient. Solute is removed up to the pore size of the membrane (20,000 Da) and haemofiltration is more efficient than dialysis in removing larger molecules. In the UK, continuous haemofiltration is mainly used, although it may be combined with haemodialysis (haemodiafiltra-tion). Compared with intermittent dialysis, continuous techniques provide improved haemodynamic stability and control of circu-lating volume and fluid overload that simplifies the provision of nutritional support. However, if one excludes peritoneal dialysis, which is seldom used in ICU, there is little evidence to support the ideal method of renal replacement. Renal replacement should be instigated early for any abso-lute indication. There is some evidence to suggest starting renal
ARF in ICUPre-renal failure and intrinsic failure due to ischaemia or neph-rotoxins are the most common causes of ARF in ICU. There is often a combination of several different insults from hypoxia, hypoperfusion, drugs, sepsis and vascular occlusion. Sepsis often underlies these causes, acting through hypotension, inflammatory mediators, or direct toxins. The presence of comorbidity or pre-exist-ing renal impairment also strongly influences the risk of ARF. In ICU, renal dysfunction does not usually arise from an intrin-sic renal disease but is secondary to multiple organ dysfunction; however, the possibility must not be discounted and a nephrology opinion sought if suspected.
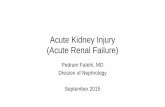
InvestigationsVigilance is essential for evidence of impending renal dysfunction (Figure 2). Pre-renal failure can be thought of as a continuum leading to intrinsic renal failure if left unchecked. There is an opportunity to act quickly to improve renal perfusion and prevent progression from RIFLE-R to RIFLE-F. Comparison of plasma and urinary sodium and osmolality may help to differentiate pre-renal hypoperfusion from established intrinsic renal failure that will no longer respond to circulatory modification (Figure 3). Diuretic use makes such values difficult to interpret.
Immediate management Correct any circulatory or respiratory impairment – ensure adequate intravascular volume and cardiac output with fluids and inotropic support if needed. The mean arterial pressure should
Investigations
Assessment of circulation Specific renal investigation
Mean blood pressure
Pulse oximetry
Urine output
Urea and creatinine (compared
with baseline values)
Acid–base status
Cardiac output
Potassium
Liver function tests
Central venous pressure Creatinine kinase/urinary
myoglobin
Urinary sodium
Urine:plasma osmolality ratio
Urine microscopy
Ultrasound to assess obstructive
cause
2
Differentiation of pre-renal and established acute renal failure in oliguria
Pre-renal hypoperfusion
Acute renal failure
Urinary sodium (mmol/litre) < 20 > 40
Urine:plasma osmolality ratio > 2 < 1.2
3

INTENSIVE CARE
© 2006 Elsevier Ltd118ANAESTHESIA AND INTENSIVE CARE MEDICINE 7:4
Patients with ARF and multi-organ failure have a mortality of 63–80% compared with 38% in those with isolated ARF. Similarly, ARF secondary to acute tubular necrosis from any cause carries a higher mortality than if ARF is part of a specific multisystem disease (e.g. vasculitis). Renal function usually returns to 90% of normal after recovery from critical illness. Few patients with ARF requiring renal replacement therapy on ICU who survive to discharge require long-term dialysis. Most of those who do will have had pre-existing renal impairment.
4
replacement early may reduce mortality. The use of pre-emptive haemofiltration in patients with severe sepsis may be beneficial due to the removal of inflammatory mediators, but to date has not been demonstrated to improve outcome. Recent evidence has suggested that ensuring an adequate dose of renal replacement may reduce mortality and improve recovery of renal function. The Acute Dialysis Quality Initiative will address these questions.
Outcome and recoveryDespite improvements in its management and the routine avail-ability of renal replacement therapy, ARF in ICU is still associated with a high mortality of 23–80%. The wide range of mortality reflects differing study inclusion criteria and in particular differing underlying aetiologies. Whether the high mortality relates to the occurrence of ARF and its complications or to the severity of the underlying pathology, of which ARF is merely a marker, is unclear. It is probably a combination of both factors. However, the severity of ARF matters. Those patients with ARF who progress to require renal replacement therapy carry a higher mortality. The underlying aetiology is also an important factor.
Haemodialysis and haemofiltration
Haemodialysis
Haemofiltration
Frompatient
Topatient
Urea Phosphate K+ Creatinine
Urea Phosphate K+ Creatinine
UreaPhosphateK+ Creatinine
UreaPhosphateK+ Creatinine
Dialysis fluid
Replacementfluid
Dialysate
Frompatient
Topatient
Urea K+ H2O Phosphate H2O Creatinine H2O
Na+ PhosphateK+ Creatinine
K+ Na+Phosphate Urea
Urea H2OPhosphate H2OK+ H2O Na+ H2O
Haemofiltrate
FURTHER READINGAbosaif N Y, Tolba Y A, Heap M et al. The outcome of acute renal failure
in the intensive care unit according to RIFLE: model application,
sensitivity and predictability. Am J Kidney Dis 2005; 46: 1038–48.
Gettings L G, Reynolds H N, Scalea T et al. Outcome in post-traumatic
acute renal failure when continuous renal replacement is applied
early vs late. Intens Care Med 1999; 25: 805–13.
Ronco C, Bellomo R, Homel P et al. Effect of different doses in continuous
veno-venous haemofiltration on outcomes of acute renal failure: a
prospective randomised trial. Lancet 2000; 356: 26–30.
Tillyard A, Keays R, Soni N. The diagnosis of Acute renal failure in
intensive care: mongrel or pedigree Anaesthesia 2005; 60: 903–14.
www.ADQI.net