Dr ahmed esawy 6 bowel imaging chronic mesenteric ischemia cmi abdominal angina aa
Upload
buck-wilsonCategory
view
223download
1
Acute Mesenteric Acute Mesenteric Ischemia:Ischemia:
Diagnostic approach and managementDiagnostic approach and management
Dr. Law Siu KingDr. Law Siu KingDepartment of Department of
surgery surgery United Christian United Christian
HospitalHospital
www.surgical-tutor.org.uk
Acute mesenteric Acute mesenteric ischemiaischemia
It is a syndrome It is a syndrome in which inadequate blood flow through in which inadequate blood flow through
the mesenteric circulation causes the mesenteric circulation causes ischemia and eventual gangrene of the ischemia and eventual gangrene of the bowel wall. bowel wall.
Acute mesenteric Acute mesenteric ischemiaischemia
It is uncommon but life-threatening It is uncommon but life-threatening diseasedisease
Incidence ~1 in every 1000 hospital Incidence ~1 in every 1000 hospital admissionsadmissions11
Mortality remains as high as 60-80% Mortality remains as high as 60-80% 11
1. Mark et al Semin Vasc Surg 23:9-20 ,2010
Acute Mesenteric Acute Mesenteric IschemiaIschemia
Early Diagnosis is importantEarly Diagnosis is important to decrease mortality to decrease mortality 11
1.Inderbitzi et al Eur J Surg 1992;158: 123-126
Acute mesenteric Acute mesenteric ischemiaischemia
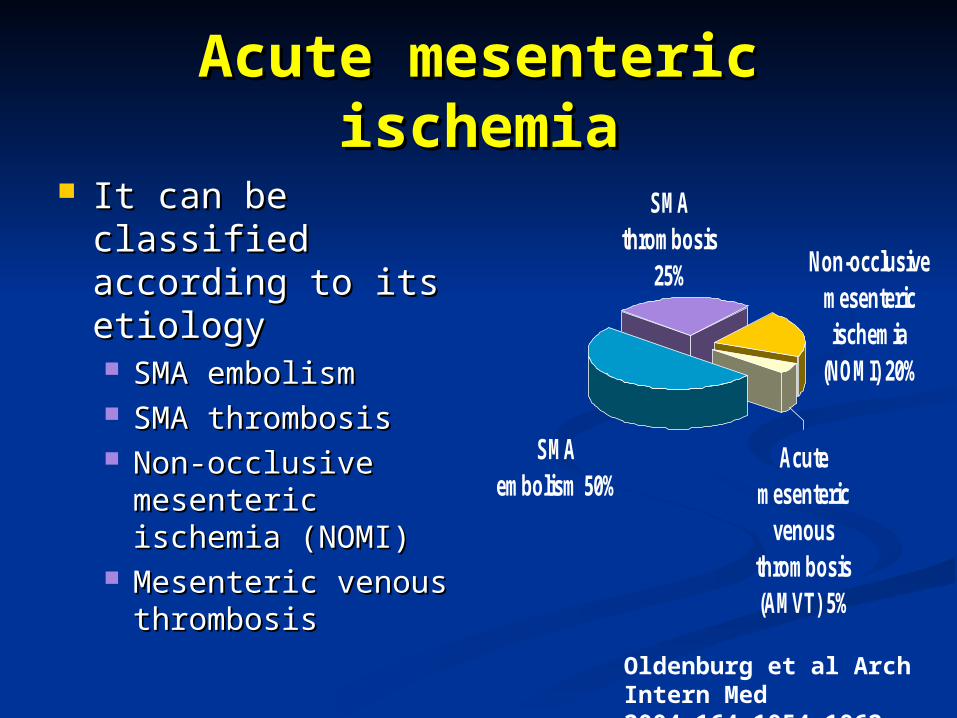
It can be classified It can be classified according to its according to its etiologyetiology SMA embolismSMA embolism SMA thrombosisSMA thrombosis Non-occlusive Non-occlusive
mesenteric mesenteric ischemia (NOMI)ischemia (NOMI)
Mesenteric venous Mesenteric venous thrombosisthrombosis
SMAthrombosis
25%
SMAembolism 50%
Acutemesenteric
venousthrombosis(AMVT) 5%
Non-occlusivemesentericischemia
(NOMI) 20%
Oldenburg et al Arch Intern Med 2004;164:1054-1062
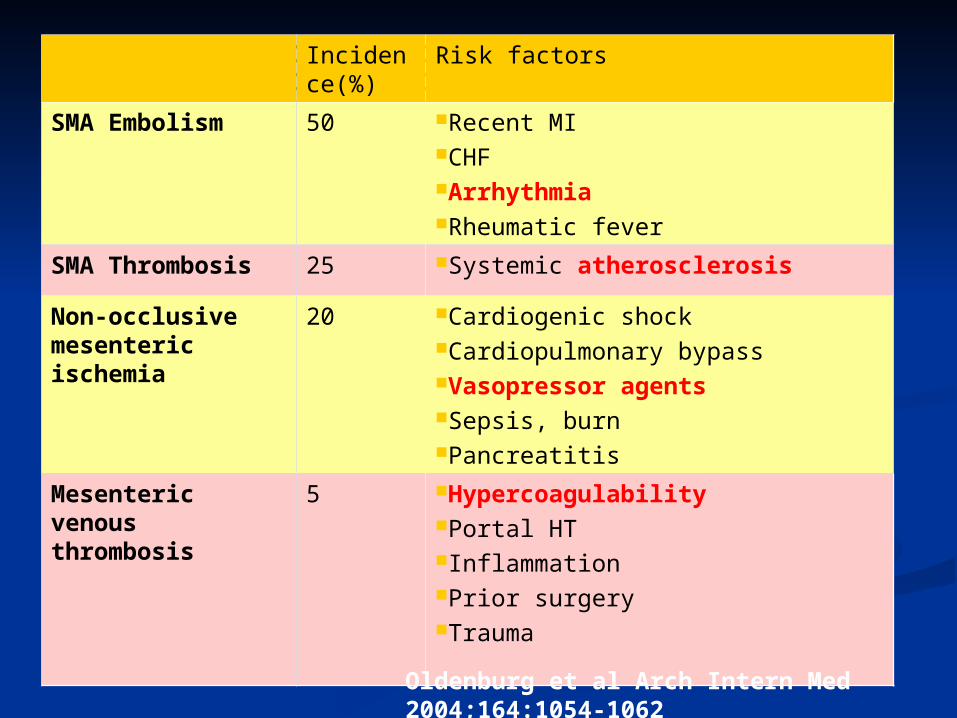
Incidence(%)
Risk factors
SMA Embolism 50 Recent MICHFArrhythmiaRheumatic fever
SMA Thrombosis 25 Systemic atherosclerosis
Non-occlusive mesenteric ischemia
20 Cardiogenic shockCardiopulmonary bypassVasopressor agentsSepsis, burnPancreatitis
Mesenteric venous thrombosis
5 HypercoagulabilityPortal HTInflammationPrior surgeryTrauma
Oldenburg et al Arch Intern Med 2004;164:1054-1062
PresentationPresentation
Classical description of early Classical description of early symptomsymptom Abdominal pain that is out of proportion Abdominal pain that is out of proportion
to physical findingsto physical findings However, classic presentation may absence However, classic presentation may absence
in 20-25% of cases.in 20-25% of cases.
Kazmers et al Ann Vas surg 12:187-197,1998
PresentationPresentation
EarlyEarly Prominent Prominent
symptoms of GI symptoms of GI emptying ( nausea, emptying ( nausea, vomiting , vomiting , diarrhea )diarrhea )
LateLate Bloody diarrhea Bloody diarrhea Abdominal Abdominal
distensiondistension FeverFever ShockShock PeritonitisPeritonitis
Early diagnosis requires high
index of suspicion Park et al J Vas 2002;
35:445-52
Sereedharan et al Singapore Med J 2007;48(4):319
Patient presents with severe abdominal pain consistent with ischemic bowel
Obtain history and perform physical examination.Pain is out of proportion to physical findings is a significant clue.
Look for risk factors for acute mesenteric ischemia.
InvestigationInvestigation
Blood test:Blood test: Most common Most common
laboratory laboratory abnormalities are:abnormalities are: haemoconcentrationhaemoconcentration LeucocytosisLeucocytosis Metabolic acidosisMetabolic acidosis Lactic acidosis (in more Lactic acidosis (in more
advanced case)advanced case) Other serum markersOther serum markers
Raised Raised amylaseamylase ALPALP
Imaging:Imaging: AXR:AXR: Features suggestive Features suggestive
bowel infarctionbowel infarction dilated thickened bowel dilated thickened bowel
loopsloops a ground-glass a ground-glass
appearanceappearance ““Thumb-printingThumb-printing””, , toxic dilatation toxic dilatation gas in bowel wall, gas in bowel wall,
portal veins or portal veins or peritoneumperitoneum
25% patients had 25% patients had normal AXRnormal AXR
Neither sensitive nor specific.
But Ix help exclude other DDxMark et al Semvassurg 200912002
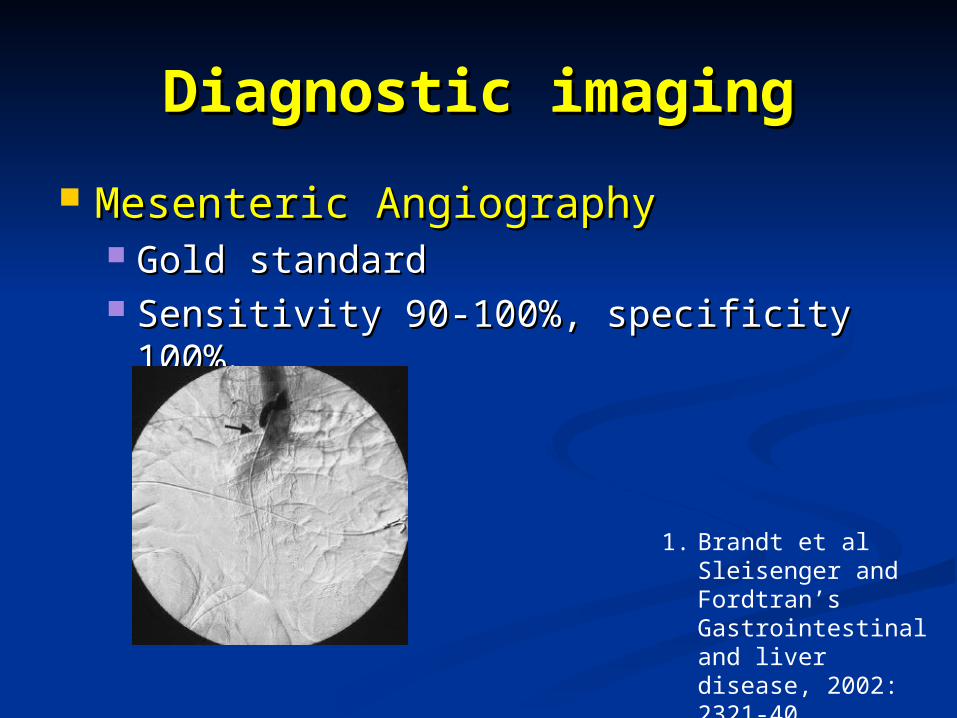
Diagnostic imagingDiagnostic imaging
Mesenteric AngiographyMesenteric Angiography Gold standardGold standard Sensitivity 90-100%, specificity 100%Sensitivity 90-100%, specificity 100%11
1. Brandt et al Sleisenger and Fordtran’s Gastrointestinal and liver disease, 2002: 2321-40
2. Hiroshi et al Surg Today (2005) 35:185–195
2
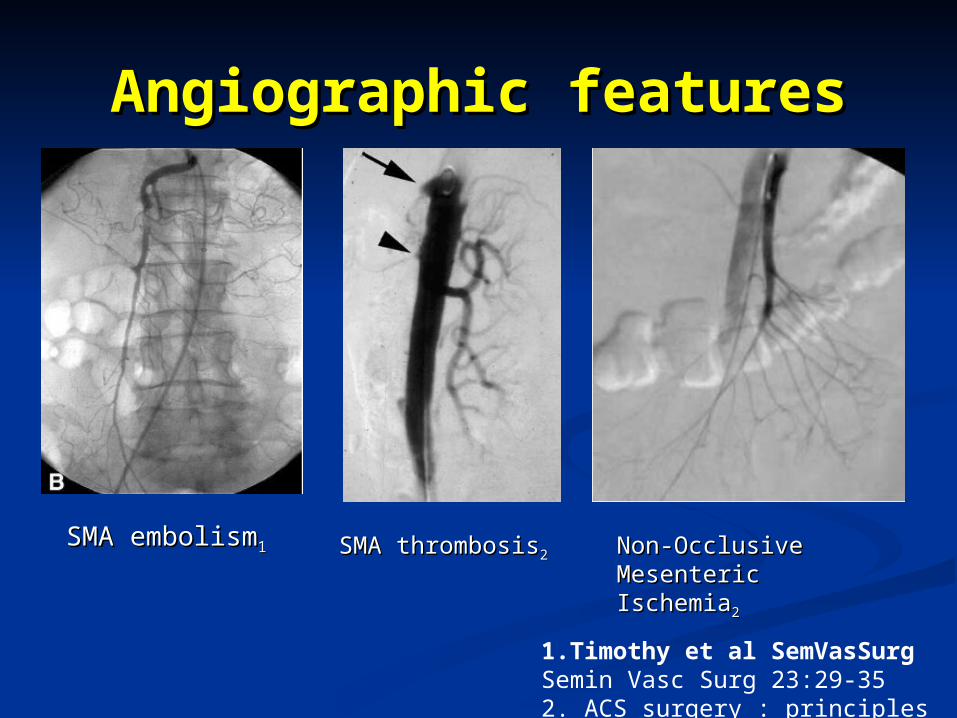
Angiographic featuresAngiographic features
SMA embolismSMA embolism11 SMA thrombosisSMA thrombosis22 Non-Occlusive Non-Occlusive Mesenteric IschemiaMesenteric Ischemia22
1.Timothy et al SemVasSurg Semin Vasc Surg 23:29-352. ACS surgery : principles and practice
Other imaging modalitiesOther imaging modalities
Standard CT abdomen Standard CT abdomen with contrastwith contrast Specificity 92%, Specificity 92%,
sensitivity 64%sensitivity 64%11
Sensitivity acute MVT Sensitivity acute MVT (100%), chronic (100%), chronic MVT(93%)MVT(93%)
Multidetector CT Multidetector CT arteriography (MDCTA)arteriography (MDCTA) Specificity 94%Specificity 94% Sensitivity 96%Sensitivity 96%22
Exclude other pathologyExclude other pathology
Duplex USGDuplex USG Excellent specificity (92-100% )Excellent specificity (92-100% ) But sensitivity is limited (70-89%)But sensitivity is limited (70-89%) Operator dependentOperator dependent
Magnetic resonance angiographyMagnetic resonance angiography Without cx of iodinated contrastWithout cx of iodinated contrast Sensitivity 100%, Specificity 91%Sensitivity 100%, Specificity 91%
1.Taourel et al Radiology 1996; 199 :632-6
2.Kirkpatrick et al Radiology 229:91-98, 2003
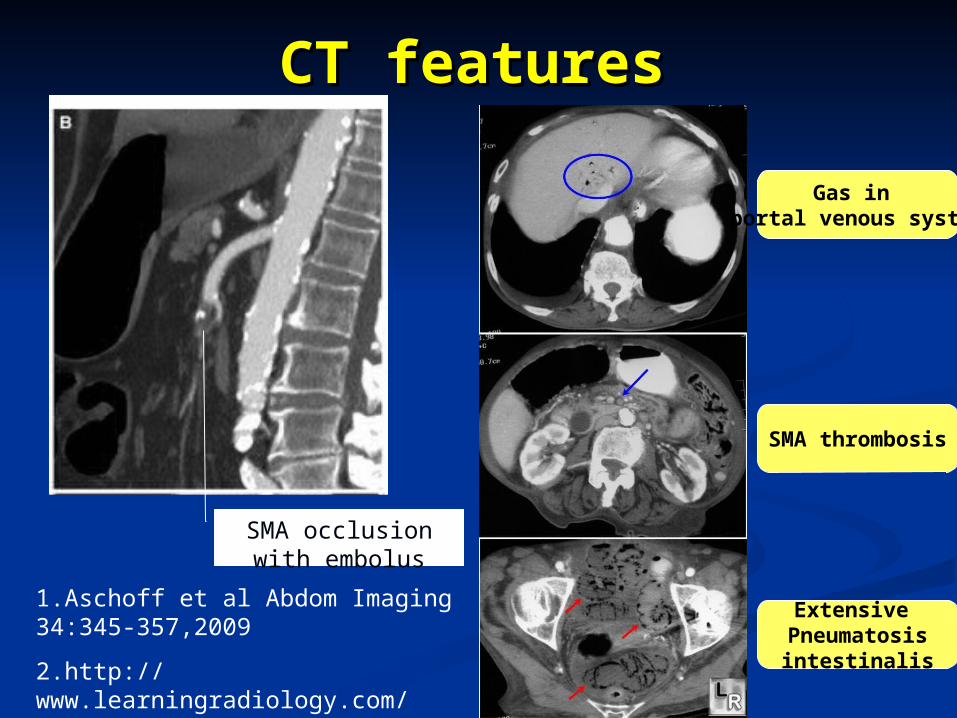
CT featuresCT features
SMA occlusion with embolus
1.Aschoff et al Abdom Imaging 34:345-357,2009
Gas in portal venous system
SMA thrombosis
Extensive Pneumatosisintestinalis2.http://
www.learningradiology.com/notes/ginotes/mesentericischemiapage.htm
CTA vs Conventional CTA vs Conventional Angiography?Angiography?
CTACTA AdvantagesAdvantages
Non-invasiveNon-invasive readily availablereadily available Allow exclude other Allow exclude other
DDx of acute abdomenDDx of acute abdomen Preferred modality for Preferred modality for
Dx MVT (90% Dx MVT (90% sensitivity )sensitivity )
Conventional Conventional AngiographyAngiography Advantage:Advantage:
High sensitivity and High sensitivity and specificityspecificity
Therapeutic role for Therapeutic role for infusion therapyinfusion therapy
Disadvantage:Disadvantage: InvasiveInvasive Less easily availableLess easily available second-line study in second-line study in
patients with a strong patients with a strong suspicion of MVT suspicion of MVT
Increase use of CTA in diagnosis of acute mesenteric ischemia
Bradbury et al The British Journal of surgery 82(11): 1446-1459,1995
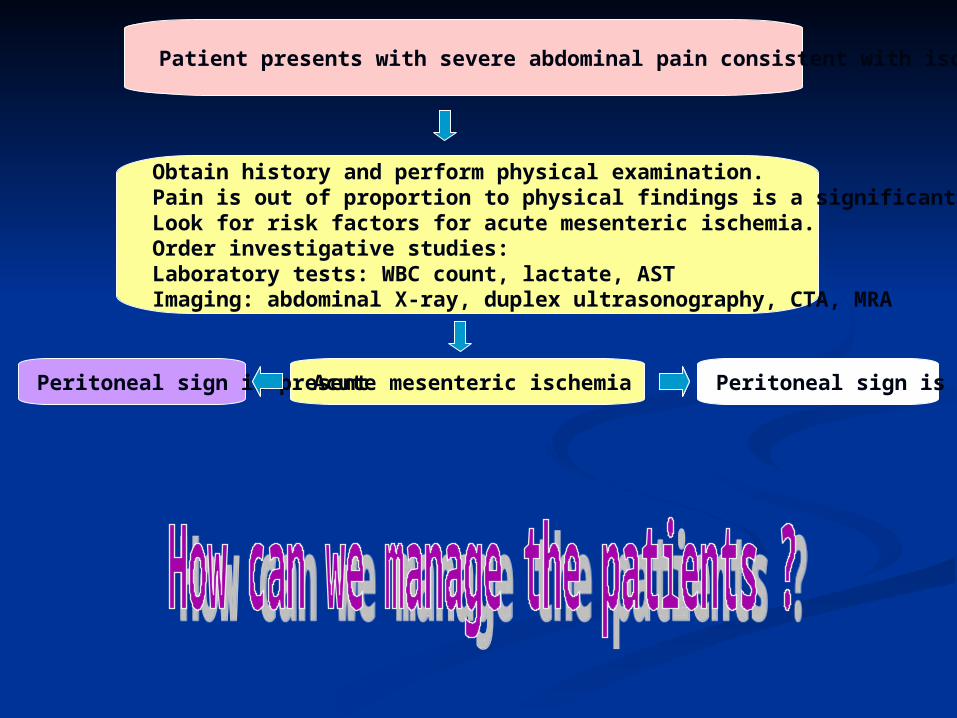
Patient presents with severe abdominal pain consistent with ischemic bowel
Obtain history and perform physical examination.Pain is out of proportion to physical findings is a significant clue.Look for risk factors for acute mesenteric ischemia.Order investigative studies:Laboratory tests: WBC count, lactate, ASTImaging: abdominal X-ray, duplex ultrasonography, CTA, MRA
Acute mesenteric ischemiaPeritoneal sign is present Peritoneal sign is absence
Principles of Principles of managementmanagement
Early recognition and interventionEarly recognition and intervention Fluid resuscitation and correction of Fluid resuscitation and correction of
electrolytes disturbanceelectrolytes disturbance Nasogastric tube Nasogastric tube
for decompression of bowelfor decompression of bowel Broad spectrum antibiotics Broad spectrum antibiotics
to cover bacterial translocationto cover bacterial translocation Hemodynamic status monitoring( Foley Hemodynamic status monitoring( Foley
catheter, CVP, A line )catheter, CVP, A line ) Definitive Tx depends on its etiologyDefinitive Tx depends on its etiology
Surgical explorationSurgical exploration
Surgical exploration if evidence of Surgical exploration if evidence of intestinal infarction/ with intestinal infarction/ with peritonitisperitonitis.. Allow assessment of Allow assessment of bowel viabilitybowel viability Identify underlying Identify underlying causes of diseasecauses of disease Resection necrotic bowelResection necrotic bowel Perform Perform revascularizationrevascularization if appropriate if appropriate
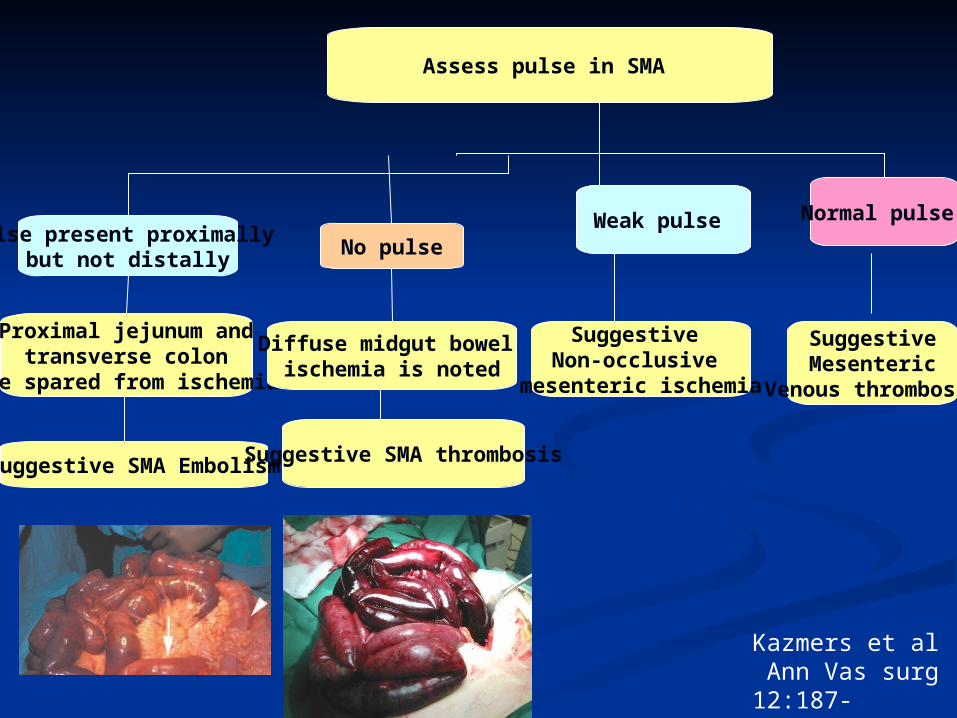
Assess pulse in SMA
Weak pulse Normal pulse
Proximal jejunum and transverse colon
are spared from ischemia
Diffuse midgut bowel ischemia is noted
Suggestive SMA Embolism Suggestive SMA thrombosis
Suggestive Non-occlusive
mesenteric ischemia
SuggestiveMesenteric
Venous thrombosis
Weak pulse No pulse
Pulse present proximally but not distally
Kazmers et al Ann Vas surg 12:187-197,1998
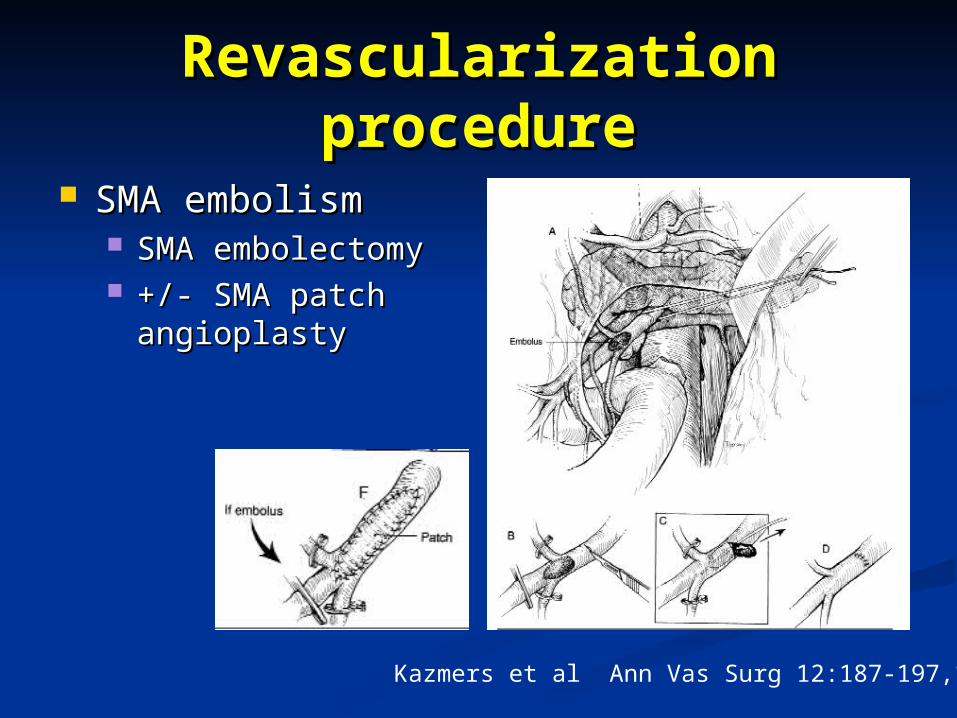
Revascularization Revascularization procedureprocedure
SMA embolismSMA embolism SMA embolectomySMA embolectomy +/- SMA patch +/- SMA patch
angioplastyangioplasty
Kazmers et al Ann Vas Surg 12:187-197,1998
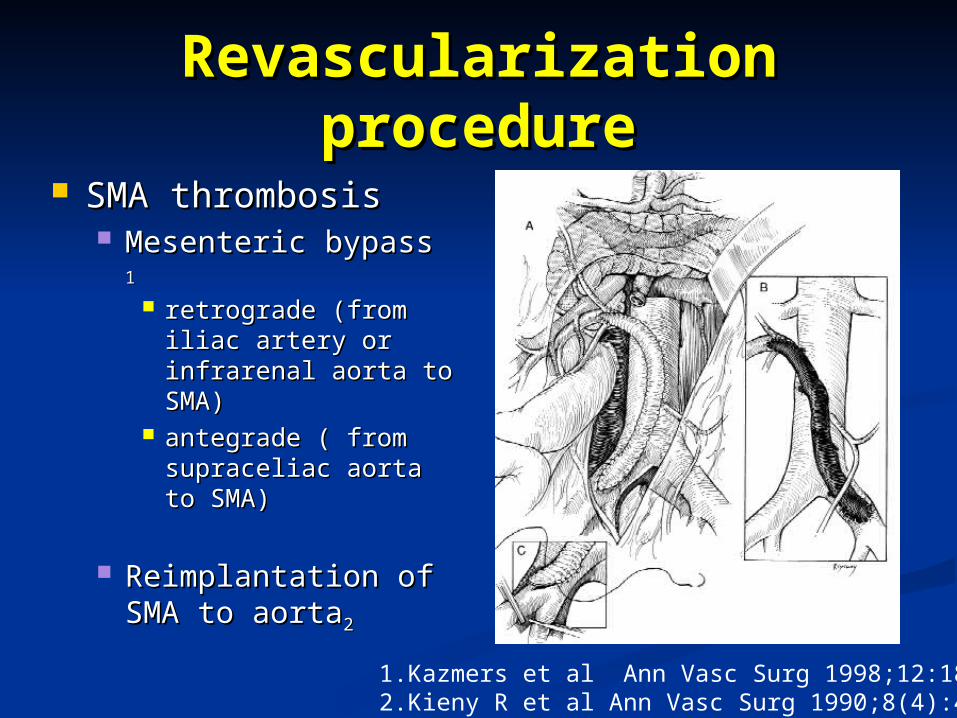
Revascularization Revascularization procedureprocedure
SMA thrombosisSMA thrombosis Mesenteric bypass Mesenteric bypass 11
retrograde (from retrograde (from iliac artery or iliac artery or infrarenal aorta to infrarenal aorta to SMA) SMA)
antegrade ( from antegrade ( from supraceliac aorta to supraceliac aorta to SMA) SMA)
Reimplantation of Reimplantation of SMA to aortaSMA to aorta22
1.Kazmers et al Ann Vasc Surg 1998;12:187-1972.Kieny R et al Ann Vasc Surg 1990;8(4):495-500
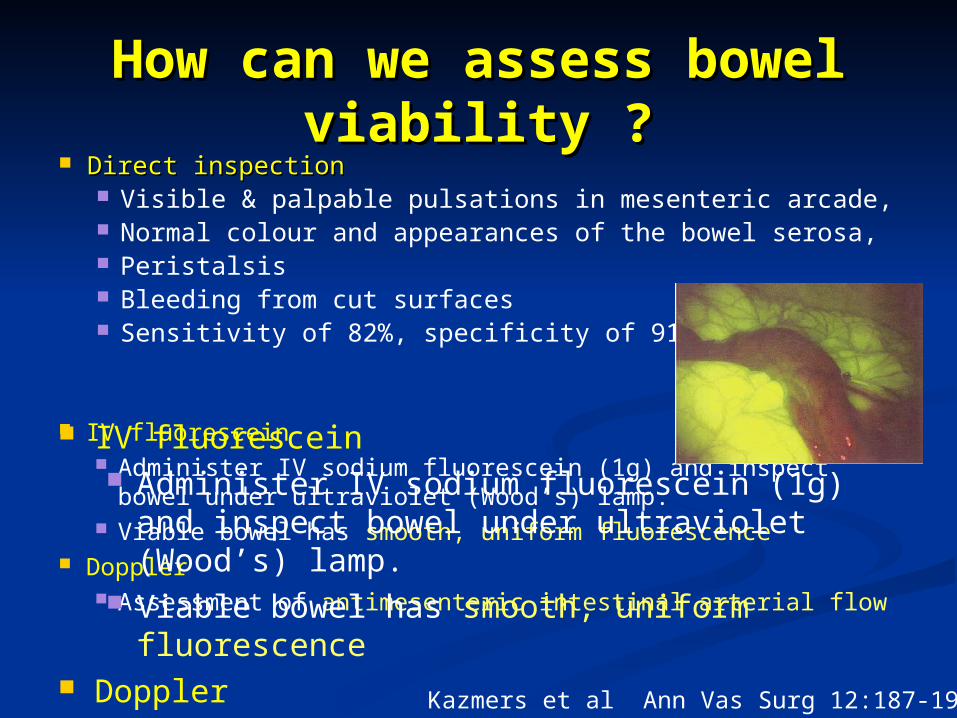
How can we assess bowel How can we assess bowel viability ?viability ?
Direct inspectionDirect inspection Visible & palpable pulsations in mesenteric arcade, Normal colour and appearances of the bowel serosa, Peristalsis Bleeding from cut surfaces Sensitivity of 82%, specificity of 91%
IV fluorescein Administer IV sodium fluorescein (1g) and inspect bowel
under ultraviolet (Wood’s) lamp. Viable bowel has smooth, uniform fluorescence
Doppler Assessment of antimesenteric intestinal arterial flow
Kazmers et al Ann Vas Surg 12:187-197,1998
IV fluorescein Administer IV sodium fluorescein (1g) and
inspect bowel under ultraviolet (Wood’s) lamp. Viable bowel has smooth, uniform
fluorescence Doppler
Assessment of antimesenteric intestinal arterial flow
Who should have second Who should have second look laparotomy? look laparotomy?
Some surgeons Some surgeons advocate advocate routine routine second-look second-look laparotomylaparotomy at 24- at 24-48hr48hr Claimed reduced Claimed reduced
mortality ratemortality rate
Other adopt a Other adopt a selective approachselective approach and perform a and perform a second laparotomy second laparotomy when patient when patient deterioates deterioates clinically.clinically. Can avoid Can avoid
unnecessary second unnecessary second operation if patient operation if patient remains wellremains well
Bradbury et al The British Journal of Surgery Vol 82(11), November 1995
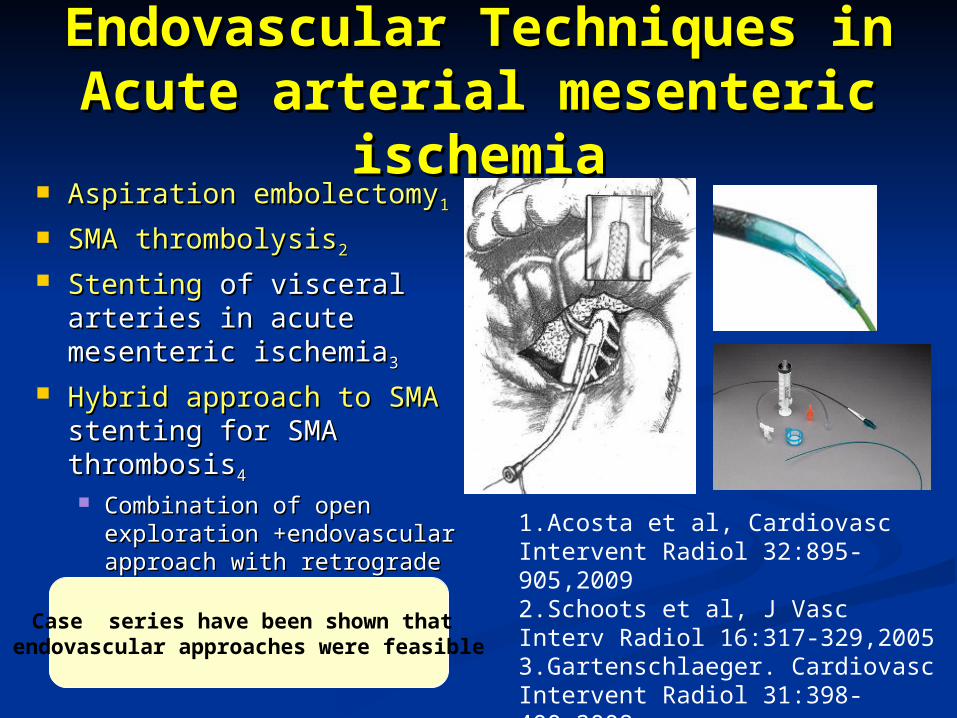
Endovascular Techniques in Endovascular Techniques in Acute arterial mesenteric Acute arterial mesenteric
ischemiaischemia Aspiration embolectomyAspiration embolectomy11
SMA thrombolysisSMA thrombolysis22
StentingStenting of visceral of visceral arteries in acute arteries in acute mesenteric ischemiamesenteric ischemia33
Hybrid approach to SMAHybrid approach to SMA stenting for SMA stenting for SMA thrombosisthrombosis44
Combination of open Combination of open exploration +endovascular exploration +endovascular approach with retrograde approach with retrograde open mesenteric stentopen mesenteric stent
1.Acosta et al, Cardiovasc Intervent Radiol 32:895-905,20092.Schoots et al, J Vasc Interv Radiol 16:317-329,20053.Gartenschlaeger. Cardiovasc Intervent Radiol 31:398-400,20084.Wyers et al, J Vasc Surg 45:269-275,2007
Case series have been shown that endovascular approaches were feasible
Management of Mesenteric Management of Mesenteric venous thrombosisvenous thrombosis
Anticoagulation Anticoagulation is mainstay of is mainstay of treatmenttreatment
Workup for hypercoagulability .Workup for hypercoagulability . Laparotomy if peritoneal signs Laparotomy if peritoneal signs
develop. develop. Resection of necrotic bowelResection of necrotic bowel Thrombectomy ( few case reports only ) Thrombectomy ( few case reports only )
1.Bradbury et al The British Journal of Surgery Vol 82(11), November 1995
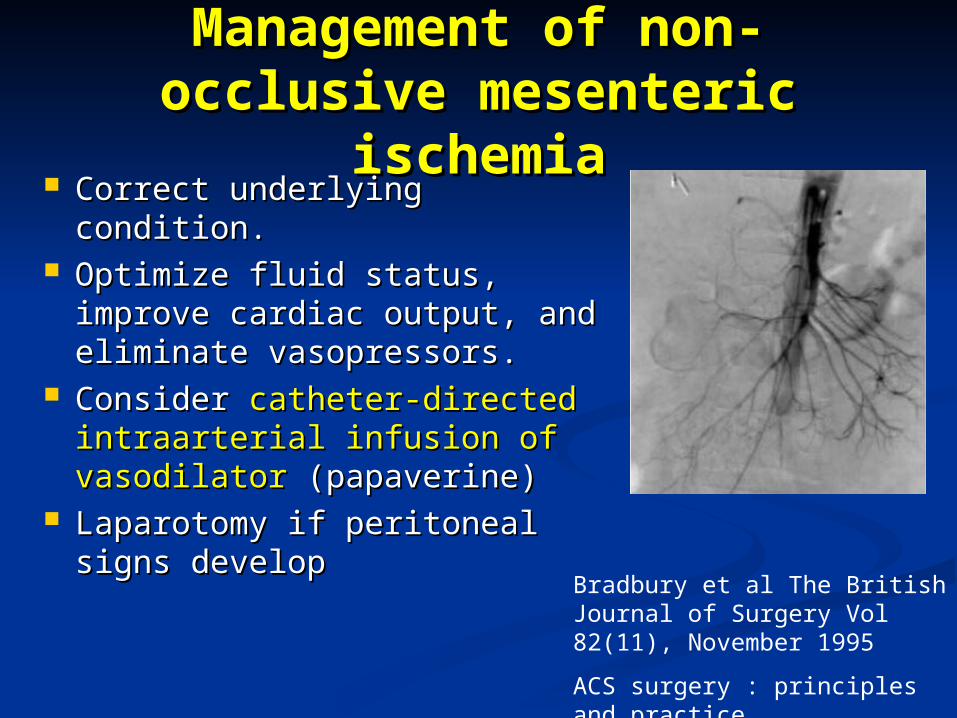
Management of non-Management of non-occlusive mesenteric occlusive mesenteric
ischemiaischemia Correct underlying Correct underlying
condition.condition. Optimize fluid status, Optimize fluid status,
improve cardiac output, improve cardiac output, and eliminate vasopressors.and eliminate vasopressors.
Consider Consider catheter-directed catheter-directed intraarterial infusion of intraarterial infusion of vasodilatorvasodilator (papaverine) (papaverine)
Laparotomy if peritoneal Laparotomy if peritoneal signs developsigns develop
Bradbury et al The British Journal of Surgery Vol 82(11), November 1995
ACS surgery : principles and practice
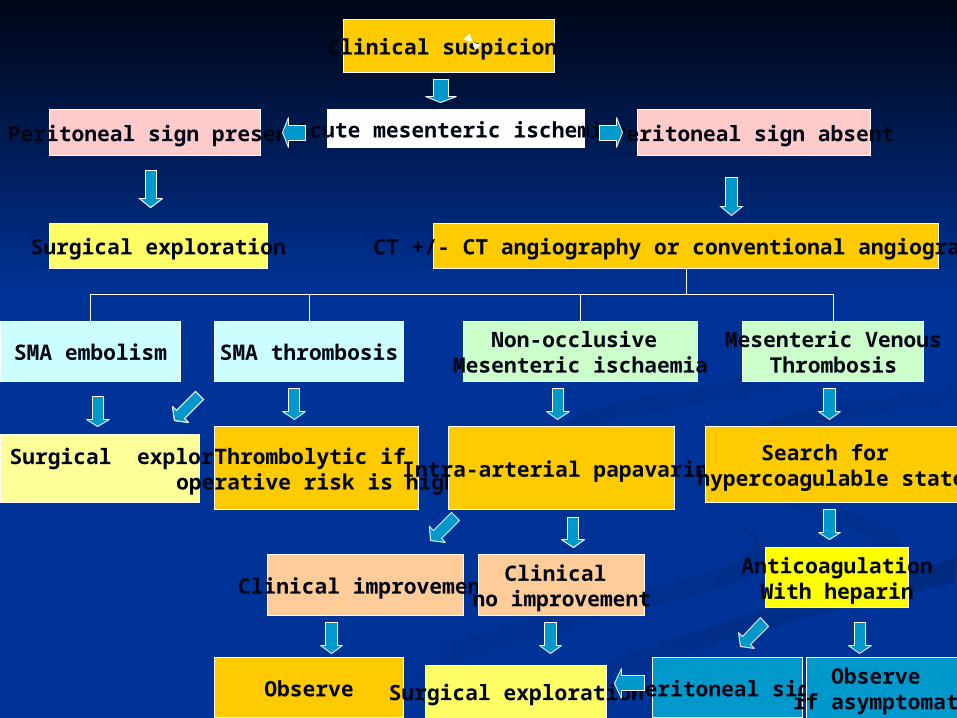
Clinical suspicion
Acute mesenteric ischemiaPeritoneal sign present Peritoneal sign absent
Surgical exploration CT +/- CT angiography or conventional angiography
SMA embolism SMA thrombosisNon-occlusive
Mesenteric ischaemiaMesenteric Venous
Thrombosis
Surgical exploration Thrombolytic if operative risk is high
Intra-arterial papavarineSearch for
hypercoagulable state
Clinical improvementClinical
no improvement
Observe Surgical exploration
AnticoagulationWith heparin
Peritoneal signObserve
if asymptomatic

Thank YouThank You

Q&AQ&A