Active Ageing and Quality of Life in Old Age 01 · Functional Health Increase in the Second Half of...
21
Active Ageing and Quality of Life in Old Age Clemens Tesch-Roemer German Centre of Gerontology Presentation at the Meeting of the UNECE Working Group on Ageing Geneva, 21.-22. November 2011
Transcript of Active Ageing and Quality of Life in Old Age 01 · Functional Health Increase in the Second Half of...

Active Ageing and Quality of Life in Old Age
Clemens Tesch-RoemerGerman Centre of Gerontology
Presentation at the Meeting of the UNECE Working Group on AgeingGeneva, 21.-22. November 2011

Related Processes
– UNECE Working Group on Ageing: „Quality of Life and Active Ageing“
– WHO: Strategy and Action Plan for Healthy Ageing in Europe, 2012-2016
Strategic priority areas for action: Healthy ageing over the life course, supportive environments, health & LTC systems fit for ageing populations, strengthening the statistical evidence base and research
Priority interventions: Falls prevention, promoting physical activity, vaccination of older people and infectious disease prevention in health care settings, public support to informal care giving with a focus on home care, including self-care, geriatric and gerontologic capacity building among the health and social care workforce
Supporting interventions: Prevention of social isolation and social exclusion, quality of care strategies for older people including dementia care and palliative care for long-term care patients, prevention of elder maltreatment
– European Year of „Active Ageing and Intergenerational Solidarity“
Page 2

Structure of the Presentation
1. The Argument
2. Early investments in active ageing3. Late investments in active ageing4. Investments in societal frameworks for active ageing
5. Some precautions6. Policy recommendations7. Questions
Page 3

1. The Argument
– Use a broad definition of active ageingActive ageing embraces both individual processes and societal opportunity structures for health, participation and security. Goal: enhancing quality of life as people age.
– Start earlyActive ageing begins with investments early in life (e.g. education, health behaviour, volunteering in childhood and adolescence).
– It’s never too lateEven in middle and late adulthood investments in active ageing are effective (e.g. health behaviour change, volunteering).
– Improve societal frameworksHealth, integration, and participation in late life (level, diversity and association with other variables) can be fostered by good societal frameworks (e.g. strength of welfare state).
– Don’t forget frail eldersLate in life a substantial proportion of the “old old” will need support because of multi-morbidity and frailty. Page 4

2. Early Investment in Active Ageing Idealized Effects
Page 5
Potential effects of early investmentsin active ageing
High early investment (e.g. extended education)
20 80 10040 60
Low early investment (e.g. brief education)
Hea
lth/In
tegr
atio
n/Pa
rtic
ipat
ion
Age
Note: The figures shows hypothetical effects of early investments in active ageing.

2. Early Investment in Active AgeingOverview of Results
– HealthLower socioeconomic status (education, income, occupational prestige) is related to worse health. Age as leveler or age as double jeopardy? Educational differences onset of diseaseincome/wealth differences maintenance of functional health.
– Social IntegrationLow educational status: More often no confidant, no partner and lack of social support. But: No education differences in kin support.
– ParticipationHigh educational status: Higher probability of gainful employment during the last decade before retirement, higher probability of volunteering in late life.
Page 6

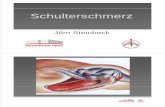
Germany: The Effects of Educational Status in Functional Health Increase in the Second Half of Life
40
50
60
70
80
90
100
Körp
erlic
heFu
nktio
nsfä
higk
eit
/SF-
36
40-54 Jahre 55-69 Jahre 70-85 Jahre
94 92
82
9386
74
8781
62
Niedrige BildungMit t lere BildungHohe Bildung
Wurm, Schöllgen & Tesch-Römer 2010: German Ageing Survey (DEAS)
Low Education: Persons without vocational training
Medium Education: Persons without vocational training or persons with highschool degree
High Education: Persons with university diploma or higher academic degree
40-54 Years 55-69 Years 70-85 Years
Func
tiona
l Hea
lth (S
F-36
)
Page 7

Effects of Educational Status Are Also Clearly Seen in the Frequency of Physical Activities
0
20
40
60
80
100
Pro
zent
Seltener/nie Einmalwöchentlich
Mehrmalswöchentlich
37
22
4254
1828
74
11 15
Niedrige BildungMittlere BildungHohe Bildung
Wurm, Schöllgen & Tesch-Römer 2010: German Ageing Survey (DEAS)
rarely/never once a week several times a week
Low EducationMedium EducationHigh EducationPe
rcen
t
Page 8

3. Late Investments in Active AgeingIdealized Effects
Page 9
Potential effects of late investmentsin active ageing
Low late investment (e.g. no health
behaviour intervention)
High late investment (e.g. health behaviour intervention)
20 80 10040 60
Note: The figures shows hypothetical effects of late investments in active ageing.
Hea
lth/In
tegr
atio
n/Pa
rtic
ipat
ion
Age

3. Late Investments in Active AgeingOverview of Results
– HealthPhysical activity positively affects health outcomes, cognitive capacity and subjective well-being – up to very old age (80+ years).
– Social IntegrationInterventions against loneliness in very old people rely on the provision of opportunities to meet other people, training for social skills and social cognitive intervention.
– Participation“Employability” of older workers can be improved by employers (e.g. further training, job rotation) and employees (e.g. investing in skills and health). Volunteering can be stimulated by offering choice of voluntary activities, the ability to plan one’s own time table and compensation for the activity. Page 10

Effects of Physical Activity on Health in Old Age I
– Intervention study: N ~700 very old participants (mean age 87 years)
– Strength training over 10 weeks for muscles at hips and knees
– Supplement: protein-containing dietary supplement
– Control group: Placebo
Source: S. G. Leveille, A. Z. LaCroix, G. E. Moore, and M. A. Fiatarone (1994). Exercise Training for Very Elderly People. The New England Journal of Medicine, Volume, 331(18), 1237-1238.
Muscle Strength
Page 11

Seite 12
Effects of Physical Activity on Health in Old Age II
Seite 12
Physical Activity– Intervention study: N ~700
very old participants (mean age 87 years)
– Strength training over 10 weeks for muscles at hips and knees
– Supplement: protein-containing dietary supplement
– Control group: Placebo
Page 12
Source: S. G. Leveille, A. Z. LaCroix, G. E. Moore, and M. A. Fiatarone (1994). Exercise Training for Very Elderly People. The New England Journal of Medicine, Volume, 331(18), 1237-1238.

4. Societal Frameworks For Active AgeingIdealized Effects
Page 13
Potential double effect of invest-ments in societalframeworks for active ageing (level and diversity)
20 80 10040 60
Hea
lth/In
tegr
atio
n/Pa
rtic
ipat
ion
Age
Low investmentin societal frameworks (e.g. weak welfare state)
High investment in societal frameworks (e.g. strong welfare state)
Differen
ce in
Leve
l
Differen
ce in
Dive
rsity
Note: The figures shows hypothetical effects of societal frameworks for active ageing.

4. Societal Frameworks For Active AgeingOverview of Results
– HealthSocietal wealth related to good health in old age. In poorer countries stronger age-related decline in health satisfaction and rise in self-reported disability.
– Social IntegrationCultural norms and societal wealth influence the relationship between social integration and well-being (e.g. effects of social integration may collapse when societal wealth is low and welfare state is weak).
– ParticipationEmployment rates of older workers (55-64 years) high in Northern Europe, the British Isles, and North America, lower in Central, Southern and Eastern Europe. – Volunteering rates high in Northern Europe and relatively low in Mediterranean countries. Page 14

Healthy Life Expectancy in Europe: Large Differences between Countries...
Page 15
0
4
8
12
16
20
24
year
s
EU
-27
Den
mar
kFi
nlan
dIc
elan
dN
orw
aySw
eden
Uni
ted
Kin
gdom
Irela
nd
Aust
riaBe
lgiu
mFr
ance
Ger
man
yLu
xem
bour
gN
ethe
rland
s
Bulg
aria
Cze
chR
ep.
Esto
nia
Hun
gary
Latv
iaLi
thua
nia
Pola
ndR
oman
iaS
lova
kia
Slov
enia
Cyp
rus
Gre
ece
Italy
Mal
taP
ortu
gal
Spai
n
Estimated number of years in good healthEstimated number of years in poor health
Males
NordicCountries
BritishIsles
CentralEuropeanCountries
EasternEuropeanCountries
SouthernEuropeanCountries
0
4
8
12
16
20
24
year
s
EU
-27
Den
mar
kFi
nlan
dIc
elan
dN
orw
aySw
eden
Uni
ted
Kin
gdom
Irela
nd
Aus
tria
Belg
ium
Fran
ceG
erm
any
Luxe
mbo
urg
Net
herla
nds
Bulg
aria
Cze
chR
ep.
Esto
nia
Hun
gary
Latv
iaLi
thua
nia
Pol
and
Rom
ania
Slov
akia
Slov
enia
Cyp
rus
Gre
ece
Italy
Mal
taP
ortu
gal
Spai
n
Females
NordicCountries
BritishIsles
CentralEuropeanCountries
EasternEuropeanCountries
SouthernEuropeanCountries
http:// ec.europa-eu/health/indicators/index_en.htmData from 2009
Males Females
Scandinavian
Countries
Transformatio
n
Countries
Scandinavian
Countries
Transformatio
n
Countries

...but Frailty in Old Age Belongs to Life Everywhere
Page 16
0
4
8
12
16
20
24
year
s
EU
-27
Den
mar
kFi
nlan
dIc
elan
dN
orw
aySw
eden
Uni
ted
King
dom
Irela
nd
Aus
tria
Belg
ium
Fran
ceG
erm
any
Luxe
mbo
urg
Net
herla
nds
Bulg
aria
Cze
chR
ep.
Esto
nia
Hun
gary
Latv
iaLi
thua
nia
Pol
and
Rom
ania
Slo
vaki
aSl
oven
ia
Cyp
rus
Gre
ece
Italy
Mal
taPo
rtuga
lSp
ain
Estimated number of years in good healthEstimated number of years in poor health
Males
NordicCountries
BritishIsles
CentralEuropeanCountries
EasternEuropeanCountries
SouthernEuropeanCountries
0
4
8
12
16
20
24
year
s
EU-2
7
Den
mar
kFi
nlan
dIc
elan
dN
orw
aySw
eden
Uni
ted
Kin
gdom
Irela
nd
Aust
riaBe
lgiu
mFr
ance
Ger
man
yLu
xem
bour
gN
ethe
rland
s
Bulg
aria
Cze
chR
ep.
Esto
nia
Hun
gary
Latv
iaLi
thua
nia
Pola
ndR
oman
iaS
lova
kia
Slov
enia
Cyp
rus
Gre
ece
Italy
Mal
taP
ortu
gal
Spa
in
Females
NordicCountries
BritishIsles
CentralEuropeanCountries
EasternEuropeanCountries
SouthernEuropeanCountries
http:// ec.europa-eu/health/indicators/index_en.htmData from 2009
Males Females

5. Some Precautions I
Page 17
Disability ThresholdIndi
vidu
al C
apac
ity
Age Death
Rate ofAgeing
Prototypical Life Coursewith Frailty Phase
Disability ThresholdIndi
vidu
al C
apac
ity
Age Death
Rate ofAgeing
Compression of Morbidity:- extension of life span- slowed rate of ageing- no frailty phase
Intervention
Effects:
Optimistic
Expectations
Indi
vidu
al C
apac
ity
Age Death
Disability Threshold
Rate ofAgeing
„Shifting“ of Morbidity:- extension of life span- unchanged rate of ageing- frailty phase
Intervention Effects:
RealisticExpectations?
?

5. Some Precautions II
– Exclusion of frail elders?An individualized focus on “successful ageing” could lead to the social exclusion of frail older people.
– Inclusive policiesPolicies for activating older people are necessary, but they should be complemented by policies on supporting frail and dependent older people to ensure their social inclusion and human dignity.
Page 18

6. Policy Recommendations
– Setting the framework for active ageingInvesting in educationProviding securityEncouraging inclusive images of ageing
– Fostering healthy biographiesPromoting a healthy lifestyleProviding effective services of health care and long-term care
– Supporting social integrationStrengthening diverse family types, extending social ties beyond familyGiving aid to caring families
– Encouraging societal participationReinforcing employability and stimulating employersCreating opportunities for volunteering
Page 19

7. Questions I
(1) How are responsibilities for active ageing shared between the individual and the society? Do individuals have a duty to make use of the opportunities provided for by the society?
(2) What should be done to avoid disadvantage to (older) people who cannot (or do not want to) invest in active ageing?
(3) Investing into active ageing: What should be done to promotelife-long learning?
(4) Investing into active and healthy ageing: What should be done to change health behaviour throughout the life-course?
(5) What should be done to change working conditions settings for improved health of older persons?
Page 20

7. Questions II
(6) What should be done to stimulate active ageing in different sub-groups (e.g. people with low education, people with low income, migrants)?
(7) What difference can new images of ageing make? How can images of ageing be changed?
(8) Bearing in mind that many ageing people – notably a high proportion of the very old – suffer from illness, chronic diseases, and frailty: What could be an inclusive understanding of active ageing?
(9) The proportion of ageing people without children is rising. If residential care homes are not a preferred option for such persons: What could be an equivalent to family care?
(10) What should be done to help older people with functional limitations to live independently at home?
Page 21