ACS, NSTEMI, STEMI Diagnosis & Management NSTEMI, STEMI Diagnosis & Management Julian M. Aroesty, MD...
43
ACS, NSTEMI, STEMI Diagnosis & Management Julian M. Aroesty, MD Associate Clinical Professor of Medicine Harvard Medical School
Transcript of ACS, NSTEMI, STEMI Diagnosis & Management NSTEMI, STEMI Diagnosis & Management Julian M. Aroesty, MD...

ACS, NSTEMI, STEMIDiagnosis & Management
Julian M. Aroesty, MDAssociate Clinical Professor of Medicine
Harvard Medical School

ACS Acute Coronary Syndrome
• Usually erosion of plaque fibrous capWith partial obstruction
Unstable anginaNSTEMI
With complete obstruction STEMI

US CVD1900-2000
2000-2008 US CV mortality decr 23%Health UnitedStates 2009Nat Center for Health Statistics


Changes in lipids 1988 to 2010
Lipid 1988-94 2000-02 2007-2010Chol 206 203 196LDL 129 123 116HDL 50.7 51.3 52.5Triglyc 118 123 110Lipid Rx 3.4% 9.3% 15.5%C/H 4.06 3.96 3.73
B. Kit et al, NHNES JAMA Oct 2012


Obesity paradoxFiegel KM et al, Assoc of mortality with weight JAMA 2013; 309:71-82
Meta-anal, 97 studies, 2.9 mill pts, 270k deathsBMI all cause mort 95% confidence
<30 kg/M2 (nl wt) 1.00All obesity 1.18 1.12-1.25>35 kg/M2 1.29 1.18-1.4130 to <35 kg/M2 0.95 0.88-1.01Concl: Mod degrees of obesity may be protective
especially in chronic disease (DM, cardiac) or aged. BMI alone is only 1 mortality risk factor


US AMI mortality 19952006H Krumholz JAMA, 2009;32:767-773
2.8 million AMI pts, 3.2 million dischargesHospital specific 30d all cause mortality
1995 2006Mortality 19% 16%
South, central, west US 20% 16%Pacific 18% 16%

Risk 1st ACS is a STEMI v UA, NSTEMI L Blork Rx prior to 1st STEMI, Arch Int Med 2010 170:1375-81
103k pts, Rx prior to 1st STEMI, Swedish registry
4 meds -- ASA, beta blocker, ACE, statin0 – STEMI risk for pts taking none = 1.01 – STEMI risk for pts taking one = 0.762 – STEMI risk for pts taking two = 0.593,4 – STEMI risk for pts taking 3+ = 0.48

MI ASA, BB, ACE, statinFornasini M, Trends in evidence based Rx of AMI
Am J Med, 2010; 123: 166-172
• Use of all 4 in hospitalized pt w AMI• 6335 patients Worcester MA hospitals
1995 2005All men 4% 47%All women 2% 42%

TIMI Risk Score ACS/NSTEMI

Risk Straification ACSTIMI risk score, 30 day mortality
PDA download - www.timi.org

TIMI Risk IndexD Morrow, E Antman, R Giuliani Lancet 2001; 358:1571
• Simplified TIMI risk – using only 3 parameters, age, HR, SBP)
1. (Age/10) squared2. x HR3. divided by systolic blood pressure
www.timi.orgCorrelates reasonably with prognosis

LMWH v UFHJL Petersen Enox v UFH for non ST elev ACS
JAMA 2004; 292:89-96
• Overview, 22K pts, NSTEMI, 6 studiesUFH enox
30 d death, MI 11.0% 10.1%30 d mortality 14.9 14.7in hosp transfusion nsmajor bleed ns

LMWH v UFHESSENCE and TIMI 11Benoxaparin v unfractionated heparin
• Does not elevate PTT• Less likely to produce HIT• Greater bioavailability w subcut
injection (90% v 25%)• Same bleeding risk• Much more expensive

AMI salvage
0102030405060708090
100
1hr 3hr 6hr 6-24hr
hr to open art
% salvage of
at risk
myocardium
Concl: Almost ½ salvage lost at 3 hr and little further salvage after 6 hr

Time to lysis v lives saved/1000
Boersma E, Lancet 1996; 248:771
0
10
20
30
40
50
60
70
1 3 9 18 hrs
time to lysis
Lives saved per 1000 @35 d
AHA/ACC-Pain to open artery = < 90 min

90 min TIMI Flow v Mortality
• TIMI 0-TIMI 1 — no or partial filling beyond occlusion, 9.3% mortality
• TIMI 2 -- slow flow, 6.1% mortality• TIMI 3 — full perfusion of distal bed
with rapid clearing of contrast, 3.7%mortality

Thrombolysis Limitations
• Major hemorrhage in 5%, ICH 0.5%• Reperfusion of IRA in 70-80%• TIMI 3 flow in only 50%• Early reocclusion in 10%• Unproven for shock, prior CABG,
NQMI (NSTEMI) patients

STEMI - PCI vs ThrombolysisE. Keeley, Lancet 2003;361:13-20
T. Addo, Cardiology Review, 2003, 20:12-16
Meta-anal, 23 trials, 7739 pts, MI, CVA, death Outcome % PCI/lysis
4-6 weeks 6-18 moDeath 7.0/9.3 (-25%) 9.6/12.8(-25%)Non fatal MI 2.5/6.8 (-63%) 4.8/10.0(-52%)CVA 0.9/2.0 (-54%) ICH 0.05/1.1 (-95%)MACE 8.1/14.0 (-43%) 12/19.0(-37%)

STEMI PCIS King, Culprit vs immed multiple PCI, JACC interv 2010; 3:22
NYS registry stable AMI, propensity matched Mortality
Immediate culprit PCI mulitvess PCIIn hosp 0.9% 2.4%12 mo 4.2% 5.8%24 mo 4.9% 7.2%42 mo 5.7% 10.4%

Best Practice Goals
10 min ER arrival to 1st ECG30 min AMI Dx to fibrinolytic40 min ER to lytic (“door-lytic”)
60 min AMI Dx to PTCA inflation70-90 min Total ER to PTCA
(“door – revascularization”)

Sx onset to PCI DeLucca, JACC, 2003; 42:991
One year mortality v time to PCIhrs to balloon inflation
<2 2-4 4-6 >6
All pts 4.4 4.7 8.5 9.7Hi risk pts 5.7 6.3 11.9 13.0Low risk pts 1.5 1.2 0.8 0

STEMIASA, lytic +/- PlavixM Sabatine, NEJM 2005, 352:1179-89
3500 STEMI Rx in 12h, lytic, ASA, heparin + Plavix 30075/dMACE-occl IRA, death, reMI before angioAngio electively 2-8 days p random
30 day MACE Plavix/placebo 12/14 (-18%)1 yr MACE “ 15/22 (-32%)

STEMI Plavix loadG Dangas, HORIZONS-AMI, JACC 2009;54:1438-46
STEMI Rx with Plavix 300mg v 600mg load600mg 300mg
30d mortality (%) 1.9 3.1Reinfarction 1.3 2.3Stent thrombosis 1.7 2.8Bleeding rate nsConcl: Primary PCI for STEMI, 600mg loading
dose is superior w/o increased bleeding

ACS - pre Rx clopidogrelBellemain-Appaix A Meta-anal JAMA Dec 2012
• Plavix pre PCI yes% no% p• All mortality, maj blee 1.54 1.97 ns• Major bleed 3.6 3.1 ns• MACE 9.8 12.4 0.001
• Concl: PreACS clopidogrel little benefit for all ACS, still useful for STEMI

Prasugrel v Clopidogrel TRITON TIMI 38 NEJM 2010; 357:20
13K pts, hi risk ACS PCI, Effient v Plavix x 6-15 mo MACE=CV death, MI, CVA
clop % pras %MACE (%) 12.1 9.9AMI 9.7 7.4Life threat bleed 0.9 1.4Fatal bleed 0.1 0.4Prasugrel no benefit & incr bleed in: 1. wt <60 kg, 2. TIA or CVA, 3. age > 75.

STEMI - ticagrelor v clopidogrelConnon et al, PLATO study, Lancet 2010
13K ACS patients, 1 yr f/uMACE = CV death, MI, CVAASA+ticagrelor ASA+clopidogrel
MACE 9.3% (-15%) 11.0%Death 4.9% (-18%) 6.0%4+ bleed 3.2% (ns) 2.9%Caution: short acting, bid dosing, problem
with compliance, danger of missed dose?

CHAMPION-PHOENIXBhatt DL (rapid onset, reversible) NEJM March 2013
11k pts, stable ap, ACS/NSTEMI, STEMIiv cangrelor v po clopidogrelEnd point- 48hr MI, stent thrombosis, bleed
End point HR pPrimary efficacy 0.78 0.005Stent thrombosis 0.62 0.01MI 0.80 0.02Bleed increase no (study criteria) yes (ACUITY)

ASSENT-4, FINESSE“real world”
Goalshortest time to open MI arteryPCI not available early• Lytic only v lytic + xfer for PCI?
1. post lytic all immed to PCI hospital2. AllPCI3. Only if ischemic or hi risk AMIPCI

STEMI - Facilitated PCI“Drip and ship”
EC Keeley, Meta analysis Lancet 2006;367:1656
• Lysis immediate planned PCI for all MI• 17 random controlled trials, 4500 pts• 60 day endpoint• Mortality• Endpoint-
CVA, MI, maj bleed, urgent revasc

STEMI Facilitated PCIEC Keeley, Meta-analysis, Lancet 2006;367:1656
17 trials, 4500 patients Facil PCI PCIUrgent TVR % 4 1Death % 5 3Re MI % 3 2Major bleed % 7 5ICH % 0.7 0.1

Rescue PCI meta-analWijeysundera JACC 2007;49:422-430
rescue % conserv %mortality 7 10CHF 13 18Repeat MI 6 11
CVA 3 0.7minor bleed 17 4

ACS Rx Update 2013P Ogara et al Circulation 2012
Major recommendation changes-decrease total ischemic time:
• Improved patient recognition of ischemic Sx
• Early triage, ECG in field• Hypothermia for cardiac arrest patients• Increased emphasis on rehabilitation

Upstream anti platelet
Clopidogrel pre-drug, 2-4 hr to effect1. TRITON (<75 yo, > 60 kg, no Hx CVA)Prasugrel effective early, incr bleeding2. PLATO• Ticagrelor = prasugrel, < bleeding3. EARLY ACS• No benefit of early IIbIIIa (incr bleed w
CABG) v non upstream @ PCI
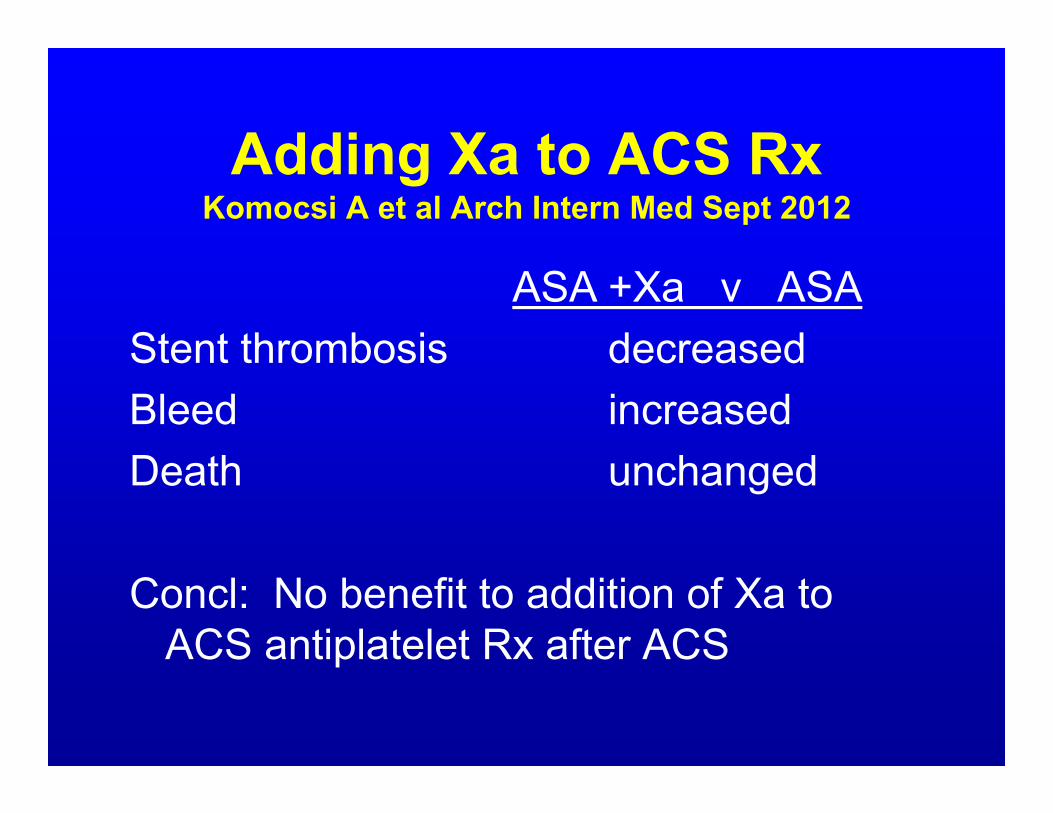
Adding Xa to ACS RxKomocsi A et al Arch Intern Med Sept 2012
ASA +Xa v ASAStent thrombosis decreasedBleed increasedDeath unchanged
Concl: No benefit to addition of Xa to ACS antiplatelet Rx after ACS

DM w CAD – PCI v CABGFREEDOM (BARI-2D)
(5 yr f/u) PCI CABG pDeath, MI, stroke 27 10 0.005All cause death 16 11 0.05MI 14 6 0.001Stroke 2.4 5.2 0.03Concl: Regardless of SYNTAX score,
CABG superior to PCI for diabetics with multivessel CAD

TIMI risk for ACS/NSTEMIincludes all except:
1. Age >75, h/o HTN, sex2. BP <100, age >65, LBBB3. HR > 100, anterior ST elevation4. DM, CHF (Killip II-IV), h/o angina
12

When was the largest effect on AMI mortality?
• 1. ’61-’77 – CCU• 2. ‘77-’88 – PCI, BB, lysis, stent• 3. ‘88-’92 – ACE, ASA• 4. ‘92-’03 – drug eluting stent
4

STEMILysis preferred
ACC/AHA Guidelines. JACC. 2004; 44:E1-E211
• <1 hr from symptom onset• Vascular access difficult• Door to balloon > 120 minutes• Lack access to skilled PCI• Time difference between PCI & lytic
is >90 minutes

STEMI PCI preferred
ACC/AHA Guidelines. JACC. 2004; 44:E1-E211
• Shock• Increased bleeding risk• Killip > Class III• Door to balloon <120 minutes• Skilled PCI available• Symptoms > 2-3 hours