
ACS is a major public health challenge In the US: Over 1.5 million people experience ACS annually 1...
18
ACS is a major public health challenge In the US: Over 1.5 million people experience ACS annually 1 In the EU: ACS is the most common cause of death, accounting for more than 741,000 deaths each year 2 The 6-month post-discharge mortality rate is: 3 3.6% in patients with UA 4.8% in patients with STEMI 6.2% in patients with NSTEMI 1. American Heart Association, 2008; 2. British Heart Foundation Health Promotion Research Group, 2008; 3. Goldberg et al, 2004
-
Upload
abigail-henderson -
Category
Documents
-
view
213 -
download
0
Transcript of ACS is a major public health challenge In the US: Over 1.5 million people experience ACS annually 1...
ACS is a major public health challenge
In the US:
Over 1.5 million people experience ACS annually1
In the EU:
ACS is the most common cause of death, accounting for more than 741,000 deaths each year2
The 6-month post-discharge mortality rate is:3 3.6% in patients with UA 4.8% in patients with STEMI 6.2% in patients with NSTEMI
1. American Heart Association, 2008; 2. British Heart Foundation Health Promotion Research Group, 2008; 3. Goldberg et al, 2004
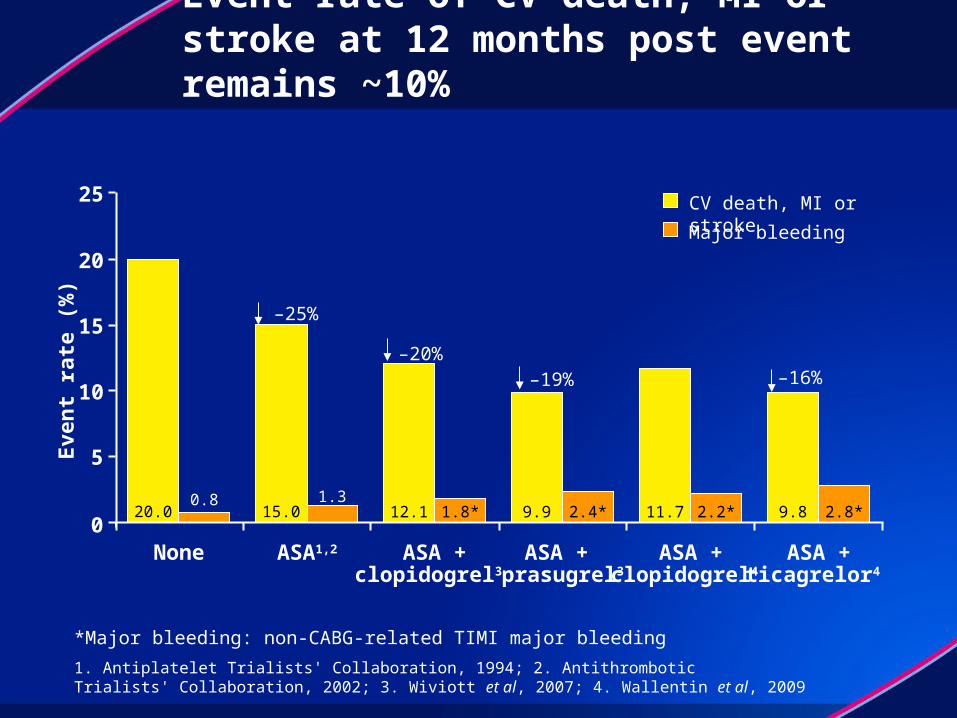
Event rate of CV death, MI or stroke at 12 months post event remains ~10%
*Major bleeding: non-CABG-related TIMI major bleeding
1. Antiplatelet Trialists' Collaboration, 1994; 2. Antithrombotic Trialists' Collaboration, 2002; 3. Wiviott et al, 2007; 4. Wallentin et al, 2009
20.0 2.8*2.2*0.8 1.3
1.8* 2.4*0
5
10
15
20
25
None
–25%
15.0
ASA1,2
–20%
12.1
ASA +clopidogrel3
ASA +
–19%
9.9
prasugrel3
11.7
ASA +clopidogrel4
Eve
nt
rate
(%
)
–16%
ASA +
9.8
ticagrelor4
CV death, MI or stroke
Major bleeding
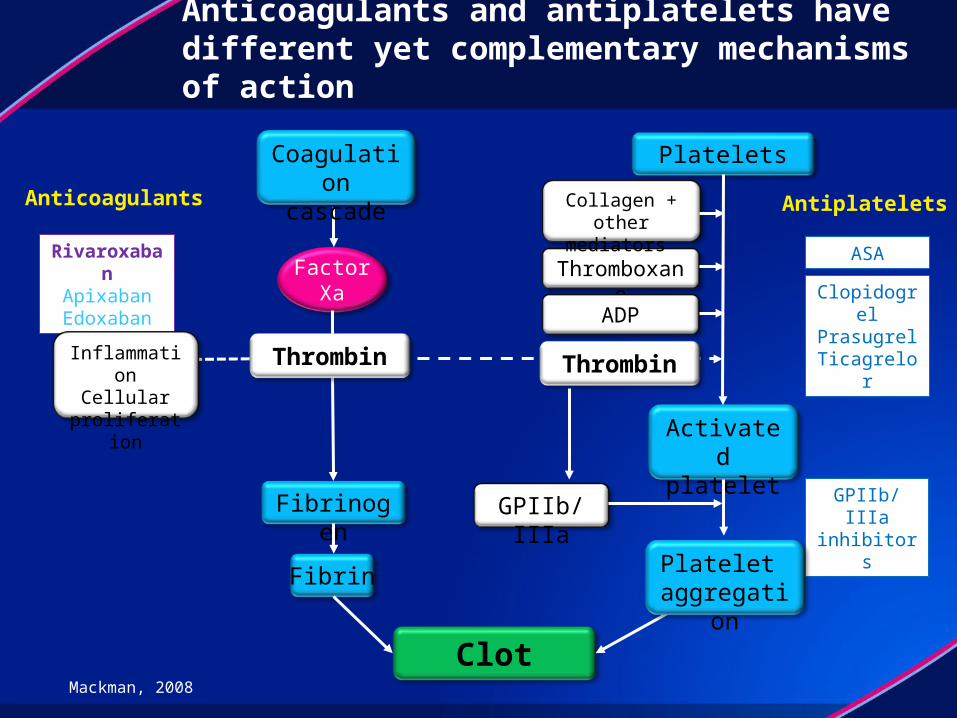
Anticoagulants and antiplatelets have different yet complementary mechanisms of action
RivaroxabanApixabanEdoxaban
Anticoagulants Antiplatelets
ASA
ClopidogrelPrasugrelTicagrelor
GPIIb/IIIa inhibitors
Fibrinogen
Fibrin
Clot
Platelets
FactorXa
GPIIb/IIIa
Thromboxane
ADP
InflammationCellular
proliferation
Collagen + other mediators
Activatedplatelet
Coagulationcascade
Mackman, 2008
Platelet aggregation
ThrombinThrombin
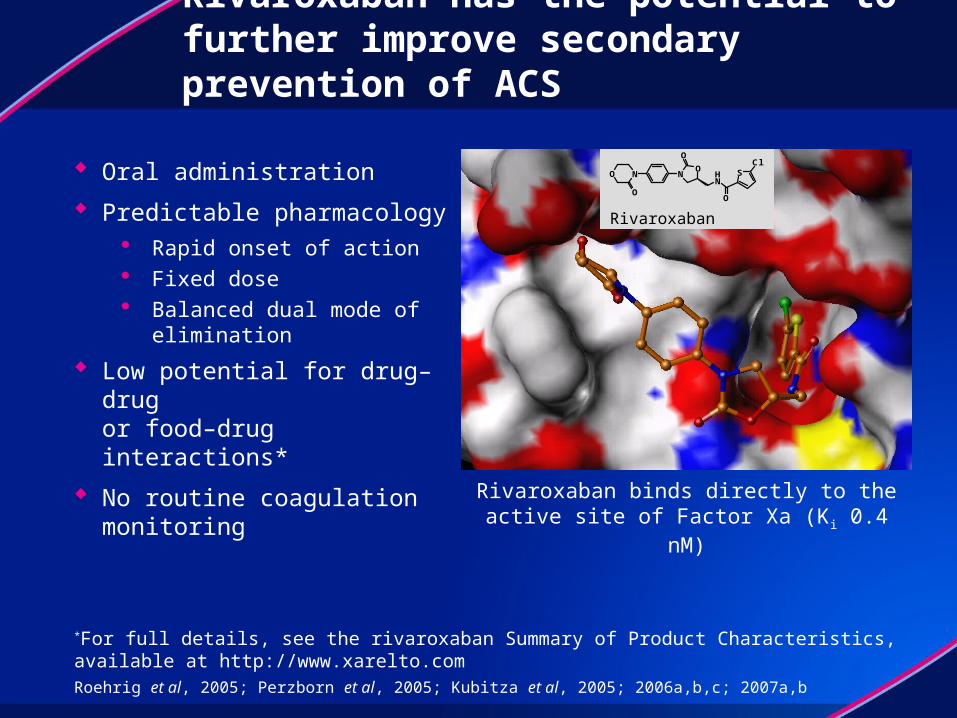
Rivaroxaban has the potential to further improve secondary prevention of ACS
Oral administration
Predictable pharmacology Rapid onset of action Fixed dose Balanced dual mode of
elimination
Low potential for drug–drug or food–drug interactions*
No routine coagulation monitoring
Roehrig et al, 2005; Perzborn et al, 2005; Kubitza et al, 2005; 2006a,b,c; 2007a,b
*For full details, see the rivaroxaban Summary of Product Characteristics, available at http://www.xarelto.com
Rivaroxaban binds directly to the active site of Factor Xa (Ki 0.4 nM)
Rivaroxaban
N NO
NH
O
SCl
O
O
O
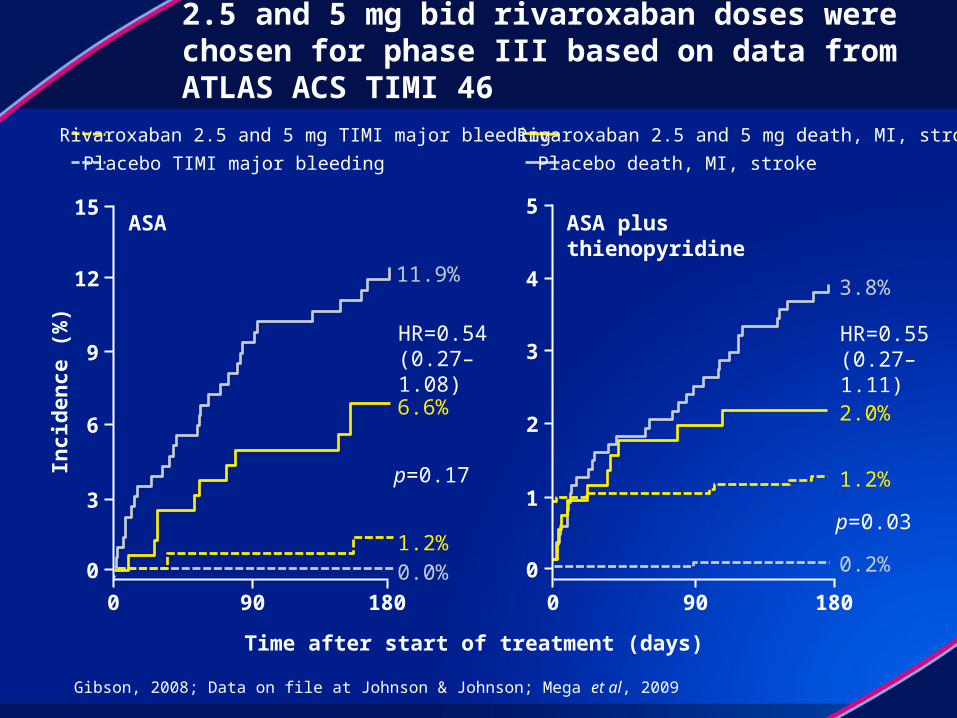
2.5 and 5 mg bid rivaroxaban doses were chosen for phase III based on data from ATLAS ACS TIMI 46
Gibson, 2008; Data on file at Johnson & Johnson; Mega et al, 2009
5
4
3
2
1
0
ASA plus thienopyridine
3.8%
2.0%
1.2%
0.2%
HR=0.55(0.27–1.11)
p=0.03
90 1800
15
12
9
6
3
0
ASA
11.9%
6.6%
1.2%0.0%
HR=0.54(0.27–1.08)
p=0.17
90 1800
Placebo TIMI major bleeding
Rivaroxaban 2.5 and 5 mg TIMI major bleeding Rivaroxaban 2.5 and 5 mg death, MI, stroke
Placebo death, MI, stroke
Inci
den
ce (
%)
Time after start of treatment (days)
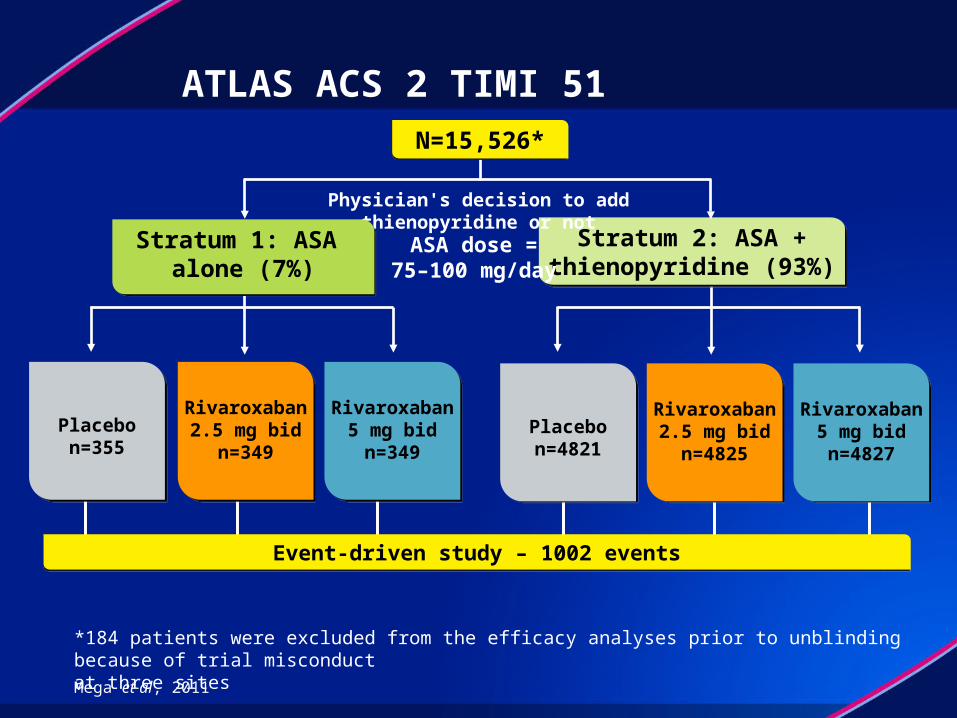
ATLAS ACS 2 TIMI 51
Rivaroxaban2.5 mg bid
n=4825
Rivaroxaban2.5 mg bid
n=4825
Placebon=4821
Placebon=4821
Rivaroxaban
5 mg bidn=4827
Rivaroxaban
5 mg bidn=4827
Event-driven study – 1002 eventsEvent-driven study – 1002 events
Stratum 2: ASA +thienopyridine (93%)
Stratum 2: ASA +thienopyridine (93%)
Rivaroxaban2.5 mg bid
n=349
Rivaroxaban2.5 mg bid
n=349
Placebon=355
Placebon=355
Rivaroxaban
5 mg bidn=349
Rivaroxaban
5 mg bidn=349
Physician's decision to add thienopyridine or not
N=15,526*N=15,526*
ASA dose =75–100 mg/day
Stratum 1: ASA alone (7%)
Stratum 1: ASA alone (7%)
Mega et al, 2011
*184 patients were excluded from the efficacy analyses prior to unblinding because of trial misconduct at three sites

Main inclusion and exclusion criteria
Inclusion criteria Diagnosis of STEMI, NSTEMI, or
UA with at least one of the following: ≥0.1 mV ST-segment deviation TIMI risk score ≥4
Patients aged ≥18 years; <55 years only with either: Diabetes mellitus or Prior MI
Patients received ASA 75–100 mg/day alone or ASA plus a thienopyridine Based on national/local
dosing guidelines
Exclusion criteria Increased bleeding risk, e.g.
Low platelet count History of intracranial
haemorrhage Active internal bleeding
Prior stroke or TIA in stratum 2 patients Atrial fibrillation: except single
episodes >2 years previously in patients aged <60 years with no evidence of cardiopulmonary disease
Gibson et al, 2011
Study endpoints/analyses
Primary efficacy endpoint: composite of cardiovascular death, MI and stroke (ischaemic, haemorrhagic or uncertain)
Main safety endpoint: incidence of major bleeding not associated with CABG surgery (according to TIMI bleeding definition)
Primary analysis: log-rank test stratified by thienopyridine use in mITT population with confirmation in an ITT analysis mITT: all randomized patients and events from randomization up to
earliest date of completion of treatment period (i.e. global treatment end date), 30 days after early discontinuation of study drug, or 30 days after randomization (patients randomized but not treated)
ITT: all randomized patients and events observed from randomization up to global treatment end date
Gibson et al, 2011
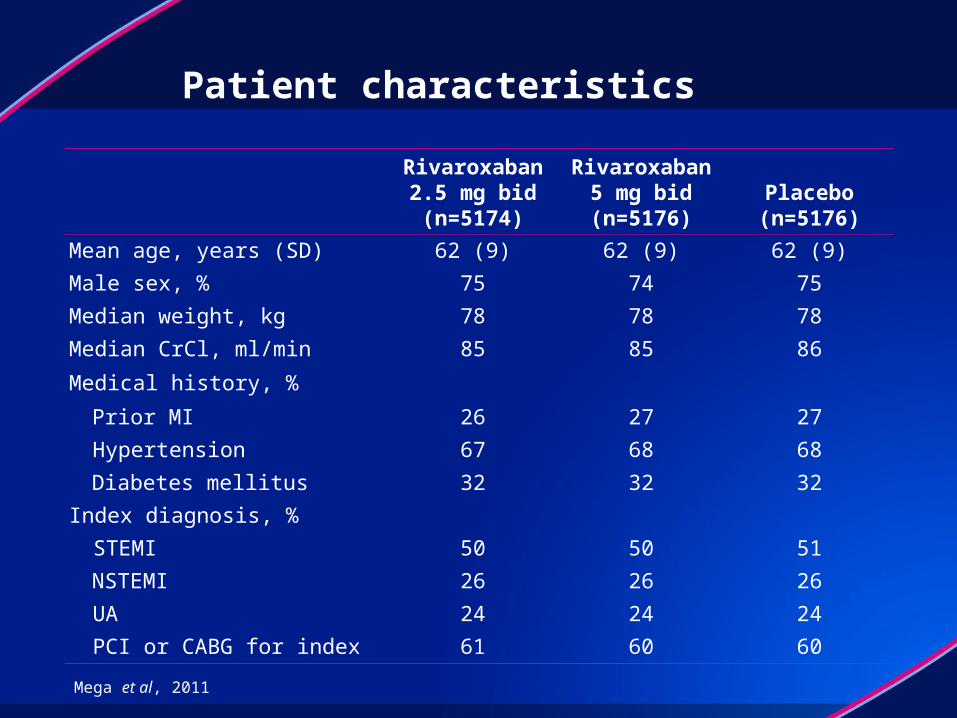
Patient characteristics
Rivaroxaban2.5 mg bid(n=5174)
Rivaroxaban5 mg bid(n=5176)
Placebo(n=5176)
Mean age, years (SD) 62 (9) 62 (9) 62 (9)
Male sex, % 75 74 75
Median weight, kg 78 78 78
Median CrCl, ml/min 85 85 86
Medical history, %
Prior MI 26 27 27
Hypertension 67 68 68
Diabetes mellitus 32 32 32
Index diagnosis, %
STEMI 50 50 51
NSTEMI 26 26 26
UA 24 24 24
PCI or CABG for index 61 60 60
Mega et al, 2011

Primary efficacy endpoint (CV death/MI/stroke)Both rivaroxaban doses, both strata
Number at riskPlacebo 5113 4307 3470 2664 1831 1079 421Rivaroxaban 10,229 8502 6753 5137 3554 2084 831
Months after randomization
HR=0.84 (0.74–0.96)ARR=1.7%
mITT p=0.008ITT p=0.002
NNT=56
10.7%
8.9%
2-year Kaplan–Meier estimate
Est
imat
ed c
um
ula
tive
rat
e (%
)
Rivaroxaban
Placebo
12
00 16
10
8
6
4
2
201284 24
Mega et al, 2011

Primary efficacy analysis: patient subgroupsBoth rivaroxaban doses, both strata
Mega et al, 2011
ASAASA + thienopyridine 0.86 (0.75 -0.98)
0.340.69 (0.45 -1.05)
STEMINSTEMIUA
0.85 (0.70- 1.03)
0.85 (0.68- 1.06)
0.82 (0.62- 1.07)
0.96
<65 years≥65 years
0.83 (0.70- 0.99)
0.84 (0.70- 1.01)
0.94
MaleFemale
0.87 (0.75- 1.01)
0.77 (0.60- 0.99)0.40
Weight <60 kgWeight 60 to <90 kgWeight ≥90 kg
0.83 (0.56- 1.25)
0.85 (0.72- 0.99)
0.83 (0.64- 1.08)
0.98
Prior MINo prior MI
0.83 (0.68- 1.01)
0.85 (0.72- 1.01)0.80
0.5 0.8 1.25 2.01.0
Diabetes mellitusNo diabetes mellitus
0.96 (0.77- 1.20)
0.78 (0.67- 0.92)0.14
CrCl <50 ml/minCrCl ≥50 ml/min
0.88 (0.62- 1.26)
0.84 (0.73- 0.96)0.82
0.57 (0.33- 0.97)North AmericaSouth AmericaWestern EuropeEastern EuropeAsiaOther
0.89 (0.59- 1.34)
0.90 (0.59- 1.37)0.83 (0.69- 1.00)
0.86 (0.63- 1.17)
0.92 (0.60- 1.39)
0.80
Overall 0.84 (0.74 0.96)
HR (95% CI) Pinteraction
Favours rivaroxaban Favours placebo

Primary efficacy endpointSeparate rivaroxaban doses, both strata
Rivaroxaban2.5 mg bid(n=5114)
Rivaroxaban5 mg bid(n=5115)
Placebo(n=5113)
Composite primary endpoint
K–M estimate at 2 years 9.1% 8.8% 10.7%
HR versus placebo (95% CI) 0.84 (0.72–0.97) 0.85 (0.73–0.98)
p value versus placebo 0.02 0.03
CV death
K–M estimate at 2 years 2.7% 4.0% 4.1%
HR versus placebo (95% CI) 0.66 (0.51–0.86) 0.94 (0.75–1.20)
p value versus placebo 0.002 0.63
MI
K–M estimate at 2 years 6.1% 4.9% 6.6%
HR versus placebo (95% CI) 0.90 (0.75–1.09) 0.79 (0.65–0.97)
p value versus placebo 0.27 0.02
Stroke (haemorrhagic and ischaemic)
K–M estimate at 2 years 1.4% 1.7% 1.2%
HR versus placebo (95% CI) 1.13 (0.74–1.73) 1.34 (0.90–2.02)
p value versus placebo 0.56 0.15
Mega et al, 2011
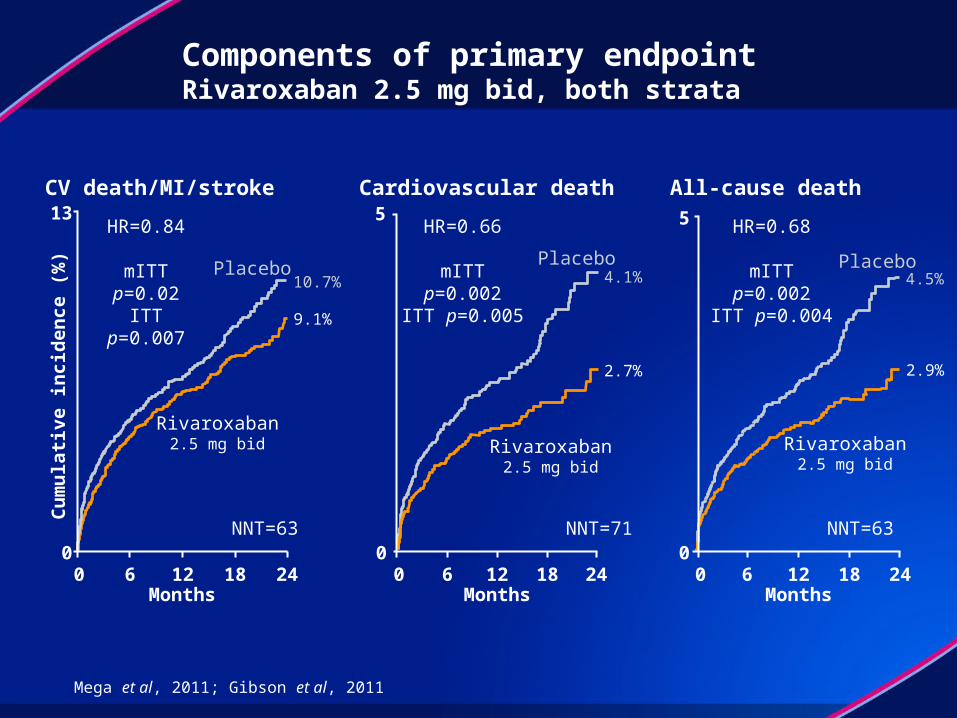
Components of primary endpointRivaroxaban 2.5 mg bid, both strata
0
Months
Cardiovascular death
NNT=71
5
0 24
4.1%
2.7%
Placebo
Rivaroxaban2.5 mg bid
HR=0.66
mITT p=0.002ITT p=0.005
181260
5
All-cause death
Months
4.5%
2.9%
240
Placebo
Rivaroxaban2.5 mg bid
HR=0.68
mITT p=0.002ITT p=0.004
18126
NNT=63
Months
CV death/MI/stroke
Cu
mu
lati
ve i
nci
de
nce
(%
)
HR=0.84
mITT p=0.02ITT p=0.007
10.7%
9.1%
Rivaroxaban2.5 mg bid
Placebo
13
0240 18126
NNT=63
Mega et al, 2011; Gibson et al, 2011

2-year Kaplan–Meier estimate
HR=0.69(0.51–0.93)RRR=31%
mITT p=0.02ITT p=0.008
2.9%
2.3%
Months after randomization
Rivaroxaban
Placebo
Est
imat
ed c
um
ula
tive
inci
den
ce (
%)
2
00 4 8 12 16 2420
3
1
Stent thrombosis*Both rivaroxaban, both strata
*Stent thrombosis events: definite, probable or possible (Academic Research Consortium definitions)Mega et al, 2011
Rivaroxaban2.5 mg bid
Rivaroxaban5 mg bid
2-year K–M estimate 2.2% 2.3%
HR versus placebo (95% CI) 0.65 (0.45–0.94) 0.73 (0.51–1.04)
p value vs placebo (mITT) 0.02 0.08

Principal safety endpointSeparate rivaroxaban doses, both strata
Rivaroxaban2.5 mg bid(n=5115)
Rivaroxaban5 mg bid(n=5110)
Placebo(n=5125)
Non-CABG TIMI major bleed
K–M estimate at 2 years 1.8% 2.4% 0.6%p value versus placebo <0.001 <0.001
ICH
K–M estimate at 2 years 0.4% 0.7% 0.2%p value versus placebo 0.04 0.005
Fatal bleeding
K–M estimate at 2 years 0.1% 0.4% 0.2%p value versus placebo 0.45 0.20
Fatal ICH
K–M estimate at 2 years 0.1% 0.2% 0.1%p value versus placebo – –
Mega et al, 2011
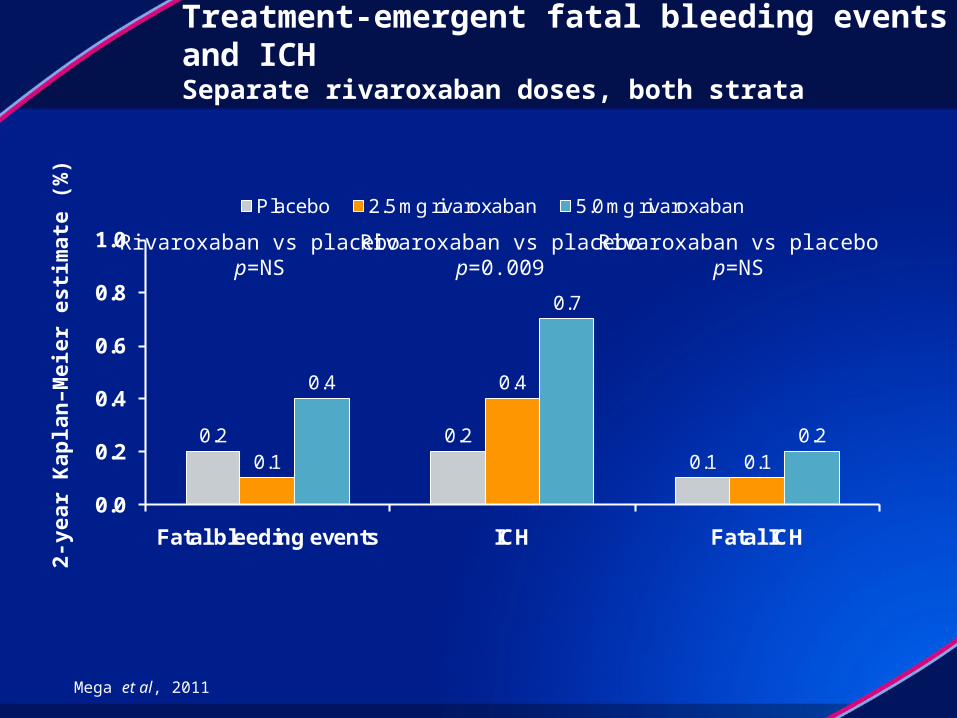
0.2 0.20.10.1
0.4
0.1
0.4
0.7
0.2
0.0
0.2
0.4
0.6
0.8
1.0
Fatal bleeding events ICH Fatal ICH
Placebo 2.5 mg rivaroxaban 5.0 mg rivaroxaban
Treatment-emergent fatal bleeding events and ICHSeparate rivaroxaban doses, both strata
Rivaroxaban vs placebop=NS
Rivaroxaban vs placebop=0.009
Rivaroxaban vs placebop=NS
2-ye
ar K
apla
n–M
eier
est
imat
e (%
)
Mega et al, 2011
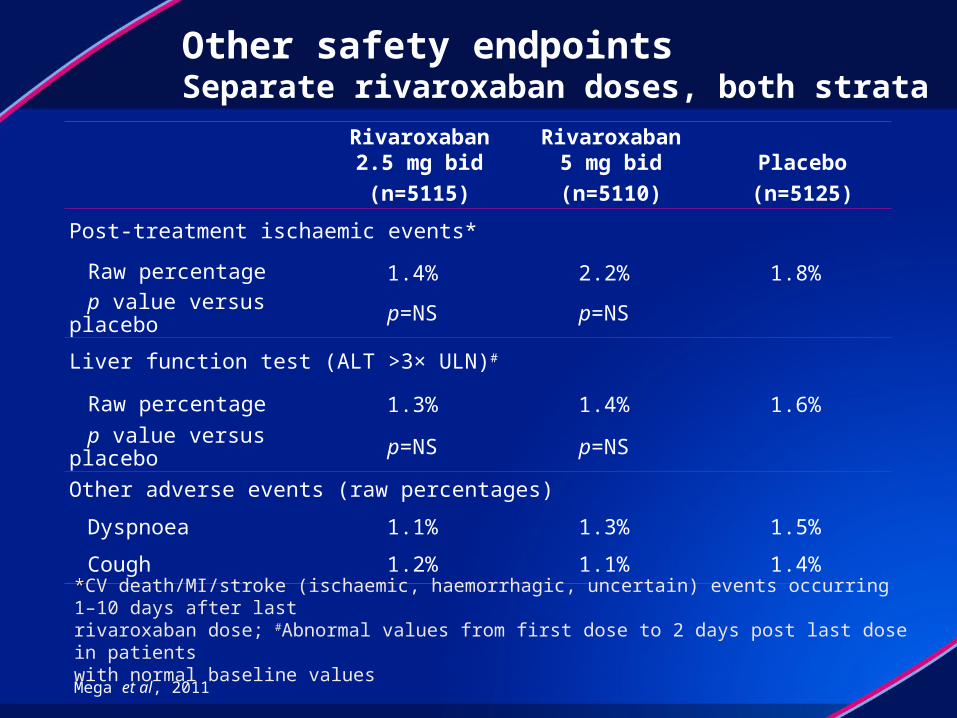
Other safety endpointsSeparate rivaroxaban doses, both strata
Rivaroxaban2.5 mg bid
(n=5115)
Rivaroxaban5 mg bid
(n=5110)
Placebo
(n=5125)
Post-treatment ischaemic events*
Raw percentage 1.4% 2.2% 1.8%
p value versus placebo p=NS p=NS
Liver function test (ALT >3× ULN)#
Raw percentage 1.3% 1.4% 1.6%
p value versus placebo p=NS p=NS
Other adverse events (raw percentages)
Dyspnoea 1.1% 1.3% 1.5%
Cough 1.2% 1.1% 1.4%
**CV death/MI/stroke (ischaemic, haemorrhagic, uncertain) events occurring 1–10 days after last rivaroxaban dose; #Abnormal values from first dose to 2 days post last dose in patients with normal baseline values
Mega et al, 2011
ATLAS ACS 2 TIMI 51: summary
Compared with placebo, rivaroxaban (2.5 or 5 mg bid) on top of ASA or ASA plus clopidogrel showed: Significant reductions in the rates of death, MI , and stroke Benefits in all types of ACS patients (UA, NSTEMI and STEMI ) More than a 30% reduction in risk of both CV and all-cause mortality
(2.5 mg bid) No increase in fatal bleeding and fatal ICH A non-bleeding safety profile similar to placebo
The addition of anticoagulation with rivaroxaban may represent a new treatment strategy in patients after recent ACS
Mega et al, 2011


















