Update on Renal Cell Carcinoma - North Kansas City Hospital...Renal Cell Carcinoma •Prevelance...
76
Update on Renal Cell Carcinoma Gerald Park, M.D. North Kansas City Hospital February 23, 2012
Transcript of Update on Renal Cell Carcinoma - North Kansas City Hospital...Renal Cell Carcinoma •Prevelance...
-
Update on Renal Cell Carcinoma
Gerald Park, M.D.
North Kansas City Hospital February 23, 2012
http://www.kcurology.com/index.html
-
Renal Cell Carcinoma
• Prevelance – 2-3% of adult malignancies – Rose 2% annually last 65yrs
• Average age 65 • ACS estimate 2012: New cases: 64,770, Deaths: 13,570. • Male:female 3:2 • African-American 10-20% higher • Renal cell carcinoma (RCC) is the tenth leading cause of
cancer deaths in males in the United States. • Overall, 5-year relative survival increased from 51% to
67% between 1975-1977 and 1996-2004.
-
• Develop from the proximal convoluted tubules • Structural alterations of the short arm of chromosome
3 (3p) • Histology
– Clear cell (most common) – Papillary – Chromophobe – Collecting duct – Unclassified
• Sarcomatoid features- no longer a separate entity but can be found in all histologic subtypes- poor prognosis
Pathophysiology
-
Pathophysiology
• Very vascular/ angiogenesis • Poor response to chemo,
radiation • Limited response to
immunotherapy • Surgical tumor- most
definitive form of treatment
• Spontaneous regression- case reports
-
Presentation
• Triad – Flank pain
– Gross hematuria
– Palpable abdominal mass
• Incidental – Imaging for other reasons (abd pain, etc.)
• Paraneoplastic syndromes (Internist’s tumor) – Hypercalcemia, hypertension, polycythemia, Stauffer’s
syndrome (nonmetastatic hepatic dysfunction), elevated ESR
-
Risk Factors
• Tobacco • Obesity • Hypertension • Acquired renal cystic disease
– End-Stage Renal Failure- 5 to 20 fold – Renal transplant recipients (native kidneys)
• Familial (4% of all RCC) – vHL, hereditary papillary RCC, hereditary RCC, Birt-Hogg-Dube (familial
oncocytoma)
• Von Hippel-Lindau syndrome – Retinal angiomas, CNS hemangioblastomas, pheochromocytoma, pancreatic
cysts/islet cell tumors, cystadenoma of epididymis, inner ear tumors, 40% of VHL pts develop RCC
• Tuberous sclerosis – autosomal dominant disorder (adenoma sebaceum- distinctive skin lesion, epilepsy, mental retardation, renal cysts, AMLs)
-
Diagnosis
• Imaging – CT- c/s IV contrast
• solid, enhancing >15 HU. HU below -20 indicate fat (Angiomyolipoma)
– US- cyst vs solid
– MRI- enhance with Gadolinium
– Arteriogram- historical, rarely used
– DMSA (dimercaptosuccinic acid) renal scan • psuedotumor (hypertrophied column of Bertin, renal
dysmorphism, unusually shaped kidney)
-
Solid, Enhancing
-
Angiomyolipoma
-
Solid vs Cystic
-
Benign cyst vs Cystic RCC
• Bosniak classification – I: most common (1/3 to 1/2 of >50y/o), zero risk of
CA, surveillance not needed, rarely symptomatic
– II: thin septa, thin calcifications, no enhancement, hyperdense with no enhancement, 0-5% risk of CA, periodic surveillance
– III: thick/irregular septa, thick/irregular calcifications, mild/mod heterogeneity, no enhancement, 50% risk of CA, surgical excision
– IV: thick/nodular areas, marked heterogeneity, enhancement, 75-90% risk of CA, surgical excision
-
Bosniak I
-
Bosniak II
-
Bosniak III
-
Bosniak IV
-
Diagnosis
• Radiographic- CT/ MRI- solid, heterogeneous, enhancing mass
– Cancer till proven otherwise
• 80% of solid tumors are malignant
• Cytology, ureteroscopy- if mass is central and concern for Urothelial CA (TCC)
-
Biopsy
• Traditionally- rarely done – Concern of tumor seeding, bleeding, infection, AV fistula, false-negatives
(difficult to distinguish RCC, adenoma, oncocytoma) – RCC is surgically treated, no other definitive treatments
• Concern of lymphoma, metastasis (from lung, breast, GI, melanoma), abscess
• Contemporary series – Smaller gauge needles, better image guidance, better histopathology – Seeding
-
Metastatic Evaluation
• CT abd/pelvis- liver, adrenal gland, LN
• CXR- lungs (CT if indicated)
• Chemistries (CBC, CMP/LFTs, LDH)
• MRI- renal vein/ IVC tumor thrombus
• Bone scan (pain, elevated alkaline phosphatase)
• CT/MRI of brain- if clinically indicated
• PET scan- role remains to be proven
-
TNM Staging (2010)
• TNM- American Joint Committee on Cancer- 7th Edition 2010- Changes from 6th Edition 2002
• T2 lesions have been divided into T2a (greater than 7 cm but less than or equal to 10 cm) and T2b (>10 cm).
• Ipsilateral adrenal involvement is reclassified as T4 if contiguous invasion and M1 if not contiguous. (previously T3a)
• Renal vein involvement is reclassified as T3a. (previously T3b)
• Nodal involvement is simplified to N0 versus N1. (previously N1-single, N2-more than one)
AJCC: Kidney. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer,
2010, pp 479-89.
-
Primary Tumor (T)
TX - Primary tumor cannot be assessed
T0 - No evidence of primary tumor
T1a - Tumor 4 cm in greatest dimension, limited to the kidney
T1b - Tumor > 4 cm but 7 cm in greatest dimension, limited to the kidney
T2a - Tumor > 7 cm but 10 cm in greatest dimension, limited to the kidney
T2b - Tumor > 10 cm, limited to the kidney
T3a - Tumor grossly extends into renal vein or its segmental (muscle-containing) branches, or tumor invades perirenal and/or renal sinus fat but not beyond Gerota’s fascia
T3b - Tumor grossly extends into vena cava below the diaphragm
T3c - Tumor grossly extends into vena cava above the diaphragm or invades the wall of the vena cava
T4 - Tumor invades beyond Gerota’s fascia (including contiguous extension into ipsilateral adrenal gland)
-
T1a (
-
T1b (4-7 cm)
-
T2 (>7 cm)
-
T3a (perinephric fat)
-
T3a (tumor in renal vein)
-
T3b (tumor in IVC below diaphragm)
-
T3c (tumor in IVC above diaphragm)
-
T4 (Tumor invades beyond Gerota’s fascia-including contiguous extension into
ipsilateral adrenal gland)
-
Regional Lymph Nodes (N)
NX Regional lymph nodes cannot be assessed.
N0 No regional lymph node metastasis.
N1 Metastases in regional lymph node(s).
M0 No distant metastasis.
M1 Distant metastasis
Distant Metastases (M)
-
Stage/ Prognostic Groups
Stage T N M
I T1 N0 M0
II T2 N0 M0
III T1 or T2 N1 M0
T3 N0 or N1 M0
IV T4 Any N M0
Any T Any N M1
-
TNM- 5yr survival
TNM 2002
• T1- 80-100%
• T2 70-80%
• T3a (fat)- 60-80%
• T3a (adrenal)- 0-40%
• T3b-c (venous)- 40-60%
• T4- 0-20%
TNM 2010
• T1- 95%
• T2- 88%
• T3- 59%
• T4- 20%
-
AJCC T at Diagnosis
0%
20%
40%
60%
80%
100%
1995 2000 2005 2010
T4
T3B
T3A
T2B
T2A
T1B
T1A
-
Prognostic Indicators
• Stage – Tumor size, venous involvement, adrenal invasion – Nodal involvement
• Grade – Fuhrman
• Tumor necrosis • Microvascular invasion • Sarcomatoid features • Collecting system invasion • Symptoms and Performance Status
-
• T1 lesions – 20% are benign
– Potentially aggressive variant is only observed in 20-30% of all RCCs in this size range
– 234 pts (8 studies) mean 2.6 cm - growth 0.28 cm /yr
– Metastatic progression 286 pts- 3 mets (1%)
• Elderly
• Decreased life expectancy
• Comorbidities that would increase the risk of interventions
• Lack of curative salvage therapies if metastases develop
• Possible loss of window of opportunity for NSS
• Substantial limitations of the current AS literature
Treatment- Surveillance
-
• Types – Cryotherapy (freezing)
• Liquid nitrogen or argon used to form an iceball that disrupts the cell membrane
– RadioFrequency Ablation (RFA)- (heating) • High-frequency (460-500 kHz) alternating current that
produces resistive friction that is converted to heat causing cell destruction
• Approaches – Laparoscopic
– Percutaneous (US, CT guided)
Treatment- Thermal Ablation
-
RFA vs Cryoablation
• Risks/ complications – Bleeding, infection, urine leak/fistula, recurrence
– Higher recurrence rate than conventional surgery
• Local tumor progression (meta-analysis 1375pts) – RFA vs cryo: 12.9 vs 5.2%
– Repeat ablation treatment- RFA vs cryo: 8.5 vs 1.3%
– Overall progession to mets disease 1.8%
-
Radio Frequency Ablation
-
Treatment-Surgery
• Radical Nephrectomy – Traditional standard of care for RCC (open, lap)
– Laparoscopic recommended over open technique
– Independent risk factor in developing CKD
• Nephron-Sparing Surgery (Partial Nephrectomy) – Traditionally used for solitary kidney, CKD, Bilateral
Disease (when RN would render pt on dialysis)
– Equivalent oncologic outcomes in T1 disease
– Open, Laparoscopic, Robotic
– NSS now recommended for T1a, some T1b
-
Treatment Surgery-NSS Principles
• Good surgical margin
• Minimize ischemia time
– Warm vs cold
– Clamp, selective clamp, no clamp
• Preservation of renal parenchyma
• Reconstruction
– Closure of collecting system
– Hemostasis
-
Surgery (Robotic)
• 3-D, High Definition Imaging, 10x magnification • Laparoscopic Wristed Instrumentation
– Precision, no tremors, greater range of motion
• Quicker Learning curve over traditional laparoscopy
• Offers advantages of complex surgical techniques with minimally invasive benefits – Dissection of renal hilum
• renal vascular anamoly- 25-35%
– Reconstruction of collecting system, closure of renal defect, hemostasis
-
Treament-Surgery (Robotic)
• Robotic Partial Nephrectomy – Series of 450 cases
• EBL= 213 ml
• Operative time= 188 min
• Ischemia time= 20 min
• 8% required transfusion
• 1.6% had urine leak
• Average tumor size 2.9cm
• 2 positive margins – Re-resected
Spana, et al, J Urology, August 2011
-
Follow-up
• Recurrences
– 20-30% have relapses
– Lung- most common site- 50-60%
– Median time 1-2 yrs, most within 3yrs
• Adjuvant Therapy
– Not shown to reduce recurrences
– Not recommended
– Clinical trials
-
AUA Guidelines for Renal Masses 2009
• Nephron-sparing surgery (NSS) should be considered in all patients with a clinical T1 renal mass as an overriding principle. – T1a- standard is Partial Nephrectomy – T1b- standard is Radical or Partial Nephrectomy – Equivalent oncologic control as Radical Nephrectomy – Increased risk of CKD associated with RN – Direct correlation between CKD and morbid cardiovascular
events and mortality
• Radical Nephrectomy is used only when NSS is not feasible or advisable (based on size, location, surgeon judgment)
• Laparoscopic approach is the standard for RN
-
AUA Guidelines for Renal Masses 2009
• Active surveillance is a reasonable option for the management of localized renal masses (less than 3-4cm)
– Should be discussed with all patients
– Primary consideration for patients with decreased life expectancy or extensive comorbidities that would make them high risk for intervention
-
AUA Guidelines for Renal Masses 2009
• Thermal ablation (cryoablation or RFA)
– High surgical risk who wants active treatment and accepts the need for long-term radiographic surveillance after treatment.
– Increased risk of local recurrence vs surgery
– Potential need for reintervention
– Lack of well proven radiographic parameters
– Usually for tumors
-
NCCN Guidelines Version 2.2012
• Suspicious mass – H&P
– CBC, CMP, LDH
– CT or MRI c/s IV contrast
– Chest Imaging
– Bone scan, if clinically indicated
– Brain MRI, if clinically indicated
– Consider urine cytology, ureteroscopy- if urothelial carcinoma suspected (eg central mass)
– Consider needle biopsy, if clinically indicated
-
NCCN Guidelines Version 2.2012
• Stage IA (
-
NCCN Guidelines Version 2.2012
• Stage II, III – Radical Nephrectomy
• Stage IV – Potentially surgically resectable solitary metastatic site
• Nephrectomy + surgical metastasectomy
– Potentially surgically resectable primary with multiple metestatic sites • Cytoreductive nephrectomy in select patients prior to systemic
therapy
– Medically or surgically unresectable • Clinical trial • Chemotherapy, Immunotherapy • Best supportive care
-
NCCN Guidelines Version 2.2012
• Follow-up for Stage I, II, III
– Observation or Clinical trial
– Every 6mo for 2y, then annually for 5y:
• H&P
• CMP, LDH
– At 2-6mo, then as indicated:
• Chest and abdominal imaging
-
NCCN Guidelines Version 2.2012 Surgical Considerations
• Nephron-sparing surgery – T1a, selected T1b – Solitary kidney, renal insufficiency, bilateral renal masses,
familial renal cell
• Open, laparoscopic, or robotic techniques for radical and partial Nx
• Regional lymph node dissection is optional, but recommended for adenopathy (preop imaging or intraop)
• Adrenal gland resection may be omitted if uninvolved and tumor is not high risk on basis of size and location
• Special teams may be required for extensive IVC involvement
-
NCCN Guidelines Version 2.2012 Surgical Considerations
• Observation or Ablative techniques – Considered for T1 who are not surgical candidates – Biopsy can be done to obtain/confirm Dx of malignancy
and guide surveillance and thermal ablation – Rigorous comparison with surgical resection has not been
done – Thermal ablative techniques are associated with a higher
local recurrence rate then conventional surgery
• Generally, candidates for cytoreductive nephrectomy prior to sytemic therapy: – Excellent performance status (ECOG PS
-
Predictors of short survival
• Poor-prognosis if >= 3 predictors
– LDH > 1.5 times upper limit of normal
– Hgb < lower limit of normal
– Corrected serum Calcium > 10mg/dl
– Interval of less than a year from original diagnosis to the start of systemic therapy
– Karnofsky performance score = 2 sites of organ metastasis
-
Diagnosis by Gender (NKCH Registry 1995 – 2011)
0
10
20
30
40
1995
1997
1999
2001
2003
2005
2007
2009
2011
No
. o
f p
ati
en
ts
Male Female
-
Age at Diagnosis (NKCH)
0
10
20
30
40
30-39 40-49 50-59 60-69 70-79 80+
No
. o
f P
ati
en
ts
1995 2000 2005 2010
-
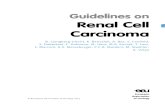
Types of Nephrectomy (NKCH compared to NCDB)
0
10
20
30
40
50
60
70
80
90
100
2000
NKCH
2000
NCDB
2004
NKCH
2004
NCDB
2008
NKCH
2008
NCDB
% o
f cases
Partial neph Simple neph Rad neph Neph/other org
-
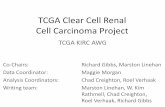
0
50
100
150
200
Partial Simple Radical
Surgical Type
No
. o
f C
ases
Open Lap Robot
Comparison of Surgical Method Surgeries 2005 – 2011 (NKCH)
-
2005 2006 2007 2008 2009 2010 2011
Partial Open 3 5 3 1
Partial Lap 1 5 2
Partial Robot 10 18 24 11
Simple Open 3 2
Simple Lap 3 2
Simple Robot 1
Radical Open 20 4 6 1 1 3 4
Radical Lap 6 27 22 7 8 5 3
Radical Robot 13 11 16 22
Neph + other organs Open 1
Change in Surgical Method Over Time (NKCH)
-
Adoption of Partial Nephrectomy
• Rate of Partial Nephectomy
– All renal masses: 15.3% (2002) to 24.7% (2008)
– T1a: 20.8% (1999) to 45.2% (2006)
2002 2004 2006 2008 2010
Partial (National)
15.3% 16.6 19.7 24.7
Partial (NKCH)
16.2 34.3 48.9
Patel et. al., J Urology, March 2012
-
Quiz
• A 51 y/o healthy male has an incidentally found solid, heterogeneous, enhancing renal mass in the right lower pole that is 4 cm in size. The most appropriate treatment is: – A. Open Radical Nephrectomy
– B. Laparoscopic Radical Nephrectomy
– C. Biopsy
– D. RFA
– E. Robotic Partial Nephrectomy