
ACCP Cardiology PRN Journal Clubaccpcardsprnjournalclub.pbworks.com/w/file/fetch... ·...
34
ACCP Cardiology PRN Journal Club March 29 th , 2016
Transcript of ACCP Cardiology PRN Journal Clubaccpcardsprnjournalclub.pbworks.com/w/file/fetch... ·...
ACCP Cardiology PRN Journal Club
March 29th, 2016

Announcements
• Thank you attending the ACCP Cardiology PRN Journal Club– Thank you if you attended before or have been attending
• We have created a PB Works Site that will house our recordedcalls, handouts, and Summary/Q&A documents. The link ishttps://accpcardsprnjournalclub.pbworks.com/
• If there are any suggestions, please let us know.

Aspirin and Tranexamic Acid for Coronary Artery Surgery (ATACAS)
Trial: Stopping vs. Continuing Aspirin before Coronary Artery Surgery
Zachary Noel, PharmD, BCPSPGY2 Cardiology Resident
University of Kentucky Healthcare
Danielle Blais, PharmD, BCPS Cardiology Specialty Pharmacist
Ohio State University Medical Center

Background: Effect of Aspirin on Platelets
• Average platelet lifespan 7-10 days
• Aspirin (ASA) prevents formation of thromboxane A2 via cyclooxygenase (COX) inhibition– Single 100mg dose provides maximal COX
inhibition in 60 minutes
– Effect persists for lifespan of platelet
• Discontinuation of aspirin for ~3-5 days restores 50% of the active platelet pool
Aspirin. Circulation. 2000;101:1206-1218

Background: Aspirin Use in Coronary Artery Disease• Aspirin is one of the cornerstone therapies for
secondary prevention of coronary artery disease (CAD)
• Interventional therapies for CAD include percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG)
• Optimal perioperative ASA dose and timing prior to CABG is not known– Risk of thrombotic events with discontinuation vs. risk
of bleeding complications with continuation is not well defined

Perioperative Use of Aspirin in Coronary Artery Surgery
-5 +2 Discontinuing likely associated with greater thrombotic risk
-4 0
Unknown whether continuing aspirin during this period reduces thrombotic events, but may be associated with modest increases in blood loss
Restarting ASA within 24-48 hours post-op associated with improved graft patency, fewer ischemic events, and mortality benefit
Delayed ASA initiation associated with worse outcomes
Aspirin Use Perioperatively
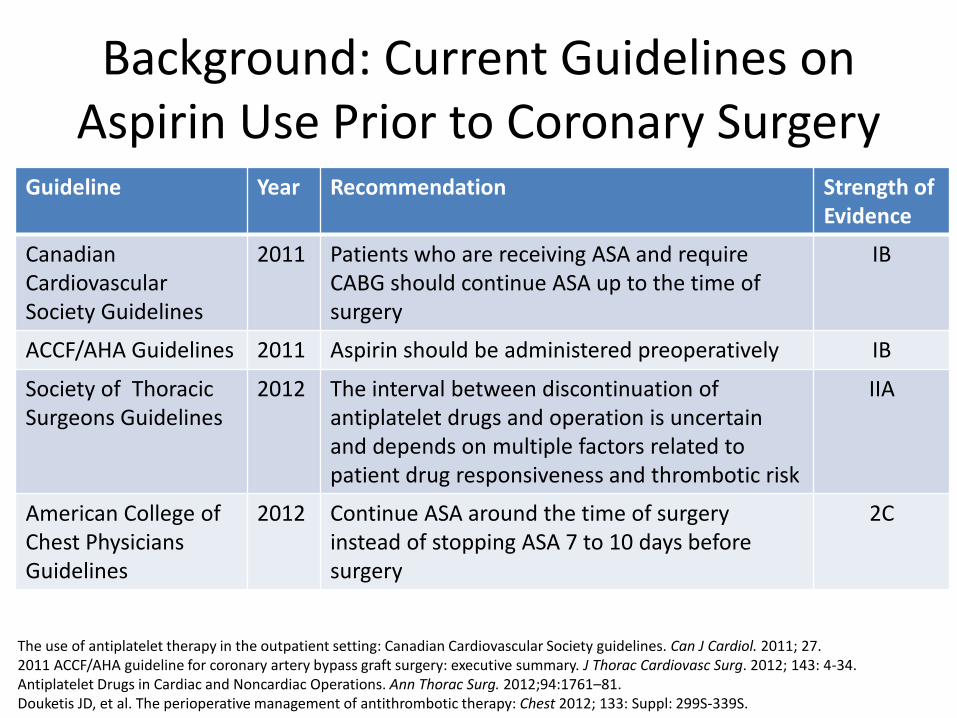
Background: Current Guidelines on Aspirin Use Prior to Coronary Surgery
Guideline Year Recommendation Strength of Evidence
CanadianCardiovascular Society Guidelines
2011 Patients who are receiving ASA and require CABG should continue ASA up to the time of surgery
IB
ACCF/AHA Guidelines 2011 Aspirin should be administered preoperatively IB
Society of Thoracic Surgeons Guidelines
2012 The interval between discontinuation of antiplatelet drugs and operation is uncertain and depends on multiple factors related to patient drug responsiveness and thrombotic risk
IIA
American College of Chest Physicians Guidelines
2012 Continue ASA around the time of surgery instead of stopping ASA 7 to 10 days before surgery
2C
The use of antiplatelet therapy in the outpatient setting: Canadian Cardiovascular Society guidelines. Can J Cardiol. 2011; 27.2011 ACCF/AHA guideline for coronary artery bypass graft surgery: executive summary. J Thorac Cardiovasc Surg. 2012; 143: 4-34.Antiplatelet Drugs in Cardiac and Noncardiac Operations. Ann Thorac Surg. 2012;94:1761–81.Douketis JD, et al. The perioperative management of antithrombotic therapy: Chest 2012; 133: Suppl: 299S-339S.

Background TrialsStudy Methods ASA Dose Results
Preoperative Aspirin Therapy Is Associated With ImprovedPostoperative Outcomes in CABG
Retrospective cohort of patients receiving ASA within 5 days of surgery
81-325mg Reduction in in-hospital mortalitywith no difference in bleeding
Effect of Timing of Chronic Preoperative Aspirin Discontinuation in CABG
Retrospective review of those taking ASA >6 days or ≤5 days before CABG
Unknown No difference in mortality or thrombotic events but more transfusions in the late use group
Aspirin and coronary artery surgery: a systematic review andmeta-analysis
Systematic review and meta-analysis of pre-operative ASA use prior to CABG
81-325mg Lower incidence of MI but higher blood loss and surgical re-exploration in those taking ASA before surgery
Circulation. 2005;112 [suppl I]:I-286–I-292.Circulation. 2011;123:577-583.British Journal of Anaesthesia. 2015, 376–85

ATACAS Trial
• Aspirin and Tranexamic Acid for Coronary Artery Surgery (ATACAS) Trial
• Designed to evaluate patients at risk for thrombotic complications undergoing elective CABG to determine whether:
1. ASA should be continued up until the day of CABG
2. TXA should be routinely used in CABG
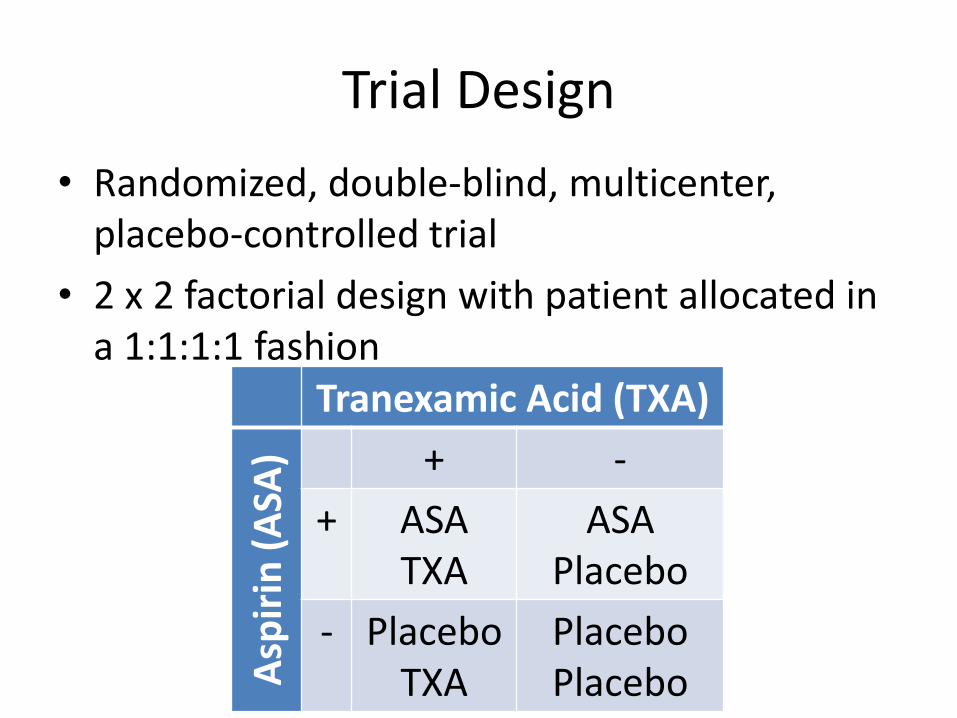
Trial Design
Tranexamic Acid (TXA)
Asp
irin
(A
SA) + -
+ ASATXA
ASAPlacebo
- PlaceboTXA
Placebo Placebo
• Randomized, double-blind, multicenter, placebo-controlled trial
• 2 x 2 factorial design with patient allocated in a 1:1:1:1 fashion
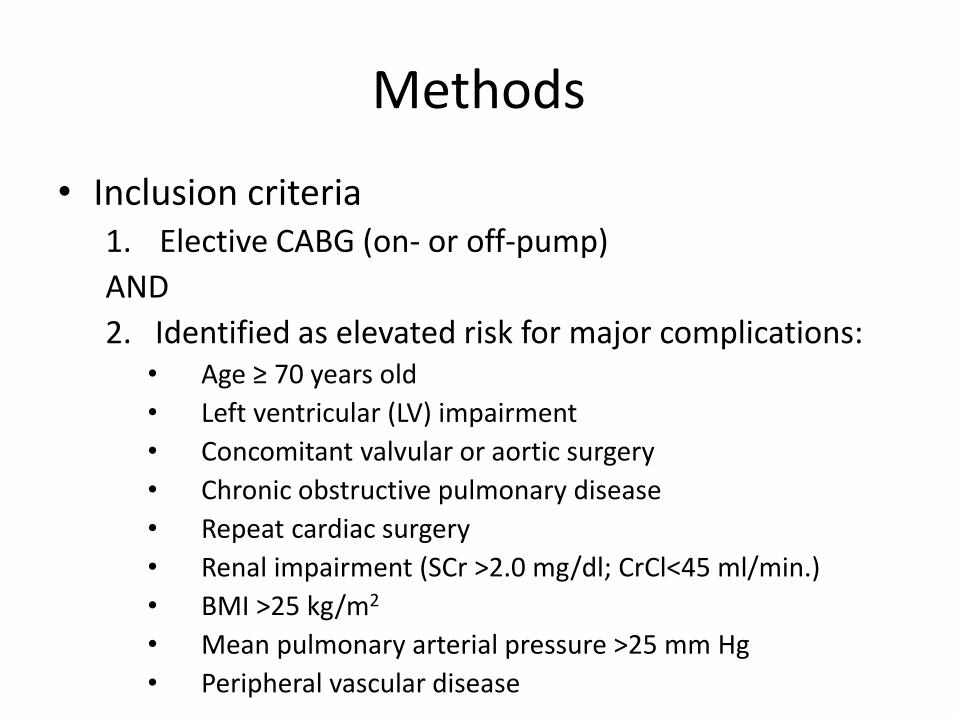
Methods
• Inclusion criteria1. Elective CABG (on- or off-pump)
AND
2. Identified as elevated risk for major complications:• Age ≥ 70 years old
• Left ventricular (LV) impairment
• Concomitant valvular or aortic surgery
• Chronic obstructive pulmonary disease
• Repeat cardiac surgery
• Renal impairment (SCr >2.0 mg/dl; CrCl<45 ml/min.)
• BMI >25 kg/m2
• Mean pulmonary arterial pressure >25 mm Hg
• Peripheral vascular disease

Methods
• Exclusion Criteria– ASA use within 5 days of surgery– Warfarin or clopidogrel use within 7 days of surgery– Glycoprotein IIb/IIIa antagonists within 24 hours of surgery– History of bleeding disorder– Thrombocytopenia– Severe renal impairment (serum creatinine >3.3 mg/dl;
creatinine clearance <25 ml/min.)– Poor English language comprehension– Clinician preference towards antifibrinolytic therapy– Thromboembolic disease– Urgent CABG – Allergy of contraindication to ASA or TXA– Pregnancy
Procedures
• Randomized in a 1:1 fashion to:
– ASA 100mg 1-2 hours preoperatively
OR
- Placebo
- Postoperative antiplatelet therapy was administered in accordance with local practices
- Patients followed for 30 days

Standardization
• Standardized protocols for heparinization, ACT goal, protamine reversal, and red blood cell transfusions were employed
• Stepwise algorithm for excessive bleeding:1. Protamine 50-100mg2. Consider aprotinin3. 5U platelet transfusion if platelets < 100,000/L4. 5U fresh frozen plasma if INR >1.4 or fibrinogen
<150 g/L5. Cryoprecipitate if fibrinogen <100 g/L6. Recombinant factor VIIa 90ug/kg, aprotinin, or
desmopressin if above strategies ineffective
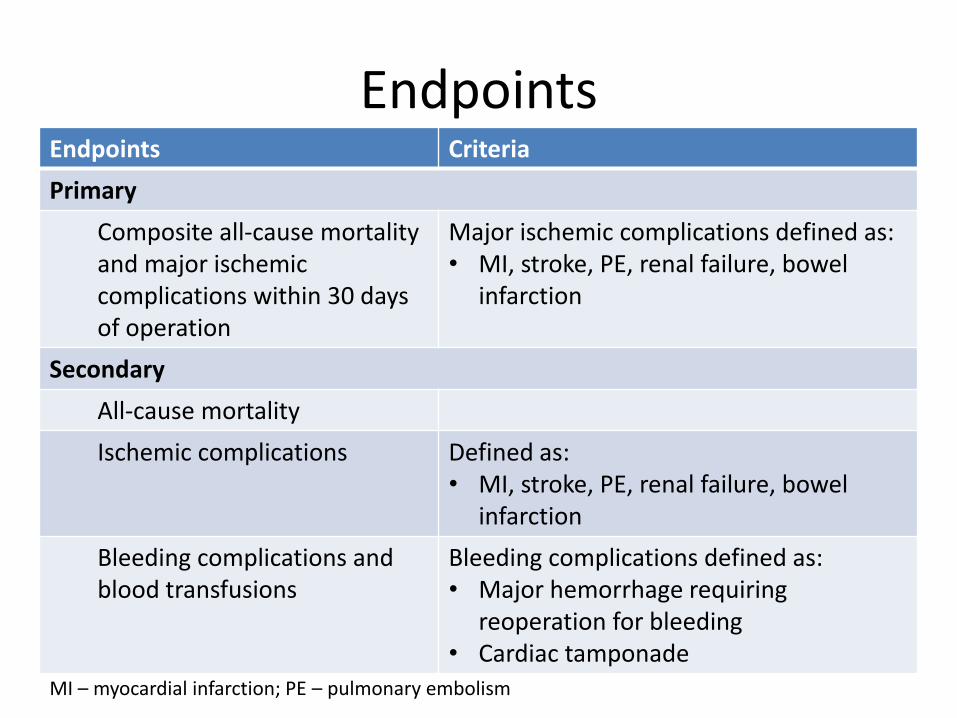
EndpointsEndpoints Criteria
Primary
Composite all-cause mortality and major ischemic complications within 30 days of operation
Major ischemic complications defined as:• MI, stroke, PE, renal failure, bowel
infarction
Secondary
All-cause mortality
Ischemic complications Defined as:• MI, stroke, PE, renal failure, bowel
infarction
Bleeding complications and blood transfusions
Bleeding complications defined as:• Major hemorrhage requiring
reoperation for bleeding• Cardiac tamponade
MI – myocardial infarction; PE – pulmonary embolism

Prespecified Subgroup Populations
• Age • Sex• Diabetes• Prior MI• Unstable angina• European System for Cardiac Operative Risk
Evaluation (EuroSCORE)• LV function• Bleeding risk during surgery• On-pump/off-pump procedure• Aortic total ischemic time
Statistical Analysis
• Intent-to-treat analysis
• Power calculations
– 4484 patients needed to detect a 30% difference in the primary outcome (alpha 0.05; beta 0.1)
– Prespecified goal to enroll 4600 patients

Results
• Over 11,000 were screened but only 5700 were eligible
• 2127 patients were enrolled between 2006 to 2013
TXA (1053)
ASA
(1
04
7) + -
+ 517 523
- 525 524
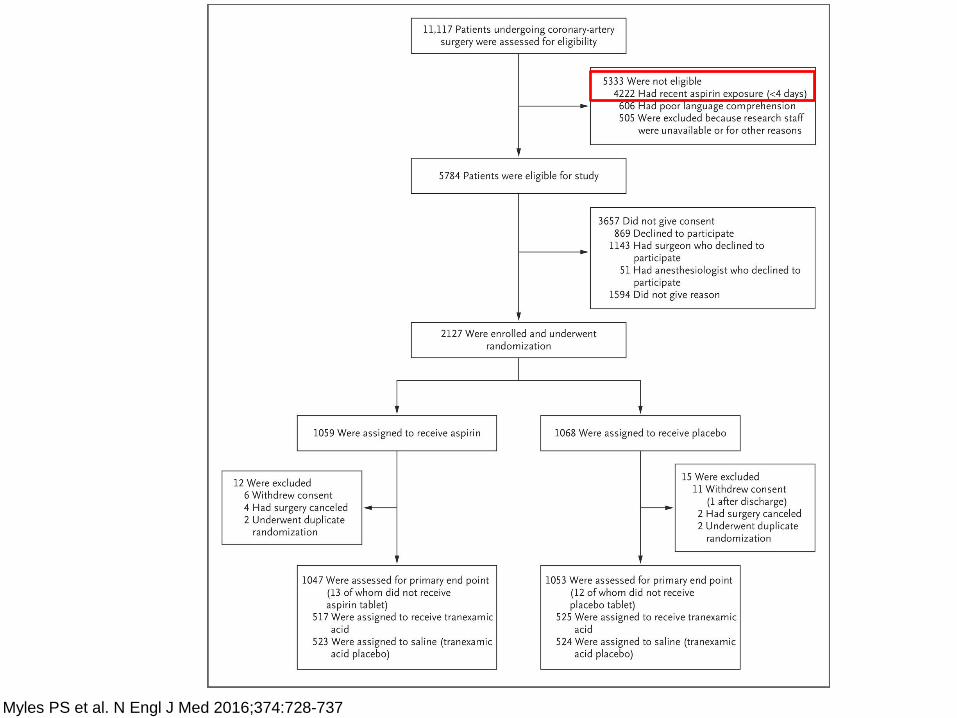
Myles PS et al. N Engl J Med 2016;374:728-737

Results
• Due to lower than expected enrollment rates but higher than anticipated primary outcome rates, the trial was stopped in July 2013
• Revised power analysis based on enrollment at that time could detect with 96% power a 30% relative risk reduction
– Minimal between group difference that could be detected with 80% power was 24% lower relative risk

Baseline Characteristics
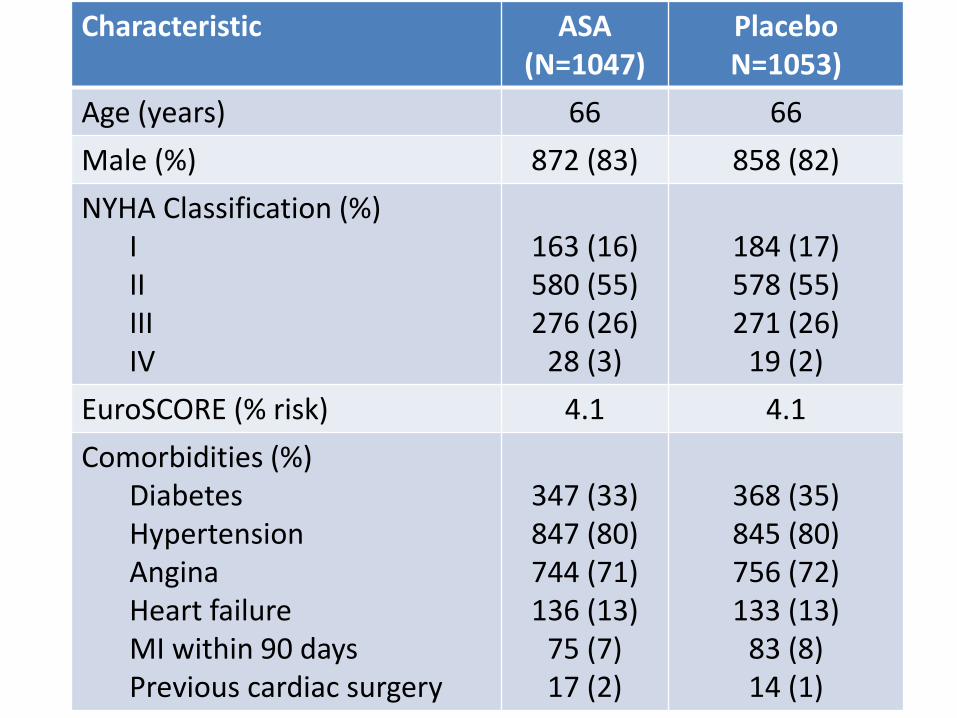
Characteristic ASA(N=1047)
PlaceboN=1053)
Age (years) 66 66
Male (%) 872 (83) 858 (82)
NYHA Classification (%)IIIIIIIV
163 (16)580 (55)276 (26)
28 (3)
184 (17)578 (55)271 (26)
19 (2)
EuroSCORE (% risk) 4.1 4.1
Comorbidities (%)DiabetesHypertensionAnginaHeart failureMI within 90 daysPrevious cardiac surgery
347 (33)847 (80)744 (71)136 (13)
75 (7)17 (2)
368 (35)845 (80)756 (72)133 (13)
83 (8)14 (1)

Baseline Characteristics (cont.)Characteristic ASA
(N=1047)Placebo
(N=1053)
Surgery Status (%)Non-electiveOn-pump surgeryOff-pump surgeryIsolated CABG surgeryCombined CABG-valve surgery
120 (12)1013 (97)
34 (3)775 (74)233 (22)
111 (11)1022 (97)
29 (3)801 (76)209 (20)
Surgical CharacteristicsMedian number of graftsMedian cross clamp time (min.)Duration of surgery (hrs)
3673.8
3663.8
Postoperative ASA use within 24 hours (%) 819 (78) 799 (76)
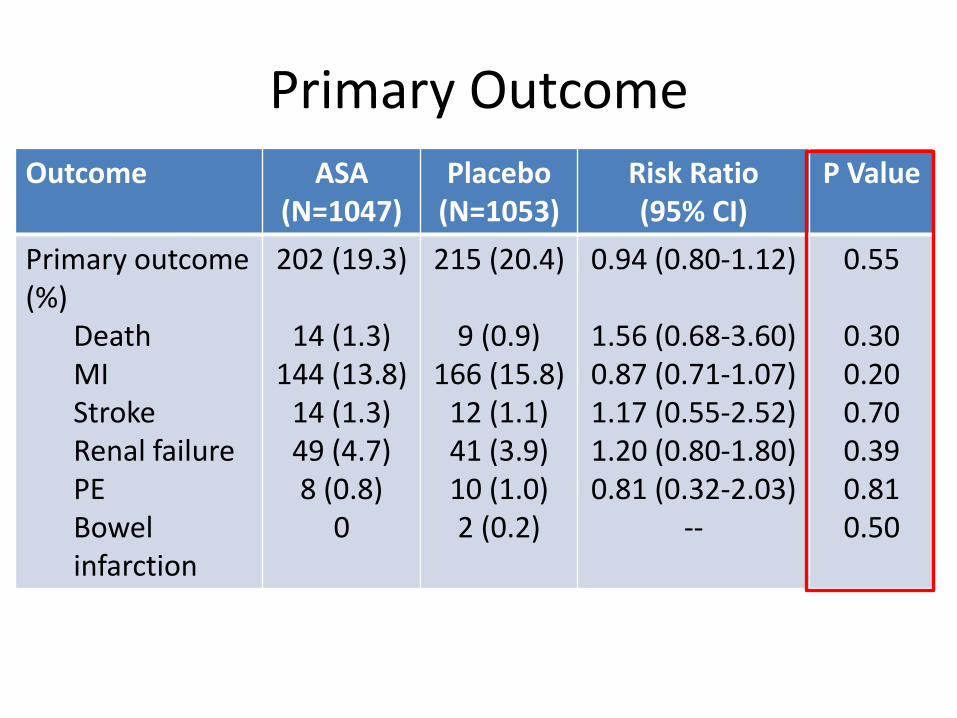
Primary Outcome
Outcome ASA (N=1047)
Placebo(N=1053)
Risk Ratio (95% CI)
P Value
Primary outcome (%)
DeathMIStrokeRenal failurePEBowel infarction
202 (19.3)
14 (1.3)144 (13.8)
14 (1.3)49 (4.7)8 (0.8)
0
215 (20.4)
9 (0.9)166 (15.8)
12 (1.1)41 (3.9)10 (1.0)2 (0.2)
0.94 (0.80-1.12)
1.56 (0.68-3.60)0.87 (0.71-1.07)1.17 (0.55-2.52)1.20 (0.80-1.80)0.81 (0.32-2.03)
--
0.55
0.300.200.700.390.810.50

Bleeding Outcomes
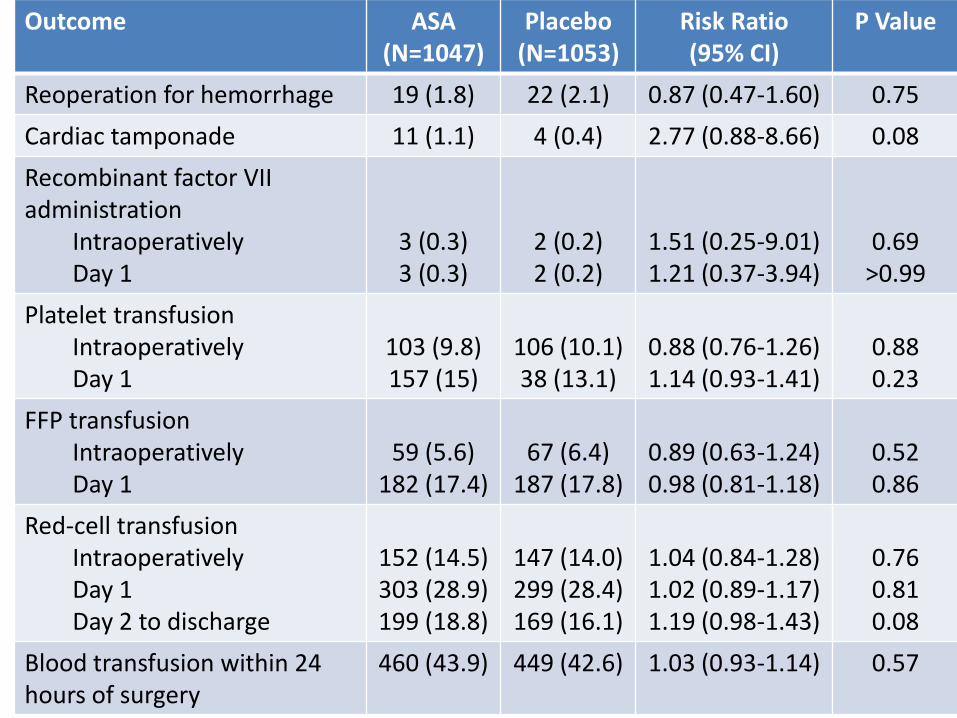
Outcome ASA (N=1047)
Placebo(N=1053)
Risk Ratio (95% CI)
P Value
Reoperation for hemorrhage 19 (1.8) 22 (2.1) 0.87 (0.47-1.60) 0.75
Cardiac tamponade 11 (1.1) 4 (0.4) 2.77 (0.88-8.66) 0.08
Recombinant factor VII administration
IntraoperativelyDay 1
3 (0.3)3 (0.3)
2 (0.2)2 (0.2)
1.51 (0.25-9.01)1.21 (0.37-3.94)
0.69>0.99
Platelet transfusionIntraoperativelyDay 1
103 (9.8)157 (15)
106 (10.1)38 (13.1)
0.88 (0.76-1.26)1.14 (0.93-1.41)
0.880.23
FFP transfusionIntraoperativelyDay 1
59 (5.6)182 (17.4)
67 (6.4)187 (17.8)
0.89 (0.63-1.24)0.98 (0.81-1.18)
0.520.86
Red-cell transfusionIntraoperativelyDay 1Day 2 to discharge
152 (14.5)303 (28.9)199 (18.8)
147 (14.0)299 (28.4)169 (16.1)
1.04 (0.84-1.28)1.02 (0.89-1.17)1.19 (0.98-1.43)
0.760.810.08
Blood transfusion within 24 hours of surgery
460 (43.9) 449 (42.6) 1.03 (0.93-1.14) 0.57

Subgroup Analyses
• No significant difference in the prespecifiedsubgroups, including age, diabetes, history of MI, unstable angina, EuroSCORE, surgery type or cross clamp time
• Statistically significant increase in 30 day mortality among males in the aspirin group (RR 2.94; 95% CI 1.11-13.9; p value 0.046)
Study Limitations
• Change in practice guidelines during study
• Selection bias
• Institution specific protocols
• Postoperative MI detection

Trial Conclusions
• There was no association between ASA use immediately prior to CABG and risk of death, thrombotic complications, or bleeding complications
Clinical Implications
• Results confirm that what most institutions already do - continue ASA before surgery - is not harmful
• These results do not suggest a decrease in death or thrombotic events when ASA is administered immediately preoperatively, contrary to other studies and meta-analyses
• These results do not suggest an increase in post-operative bleeding when ASA is administered immediately preoperatively, contrary to other studies and meta-analyses

Conclusion
• Because the majority of patients undergoing CABG are on ASA for CAD and there does not appear to be an increased risk of bleeding complications postoperatively in those taking ASA, combined with the well-established benefits of starting ASA within 24-48 hours postoperatively, continuing ASA before CABG is practical and safe; however, it does not appear to have clinical benefit in reducing death and thrombotic complications

Thank You
• Danielle Blais, PharmD, BCPS
• Craig Beavers, PharmD, FAHA, AACC, BCPS (AQ-Cardiology), CACP
• Carrie Oliphant, PharmD, FCCP, BCPS-AQ Cardiology
• Ted Berei, PharmD, MBA

Questions?
Thank you for attending!
If you would like to have your resident present, would like to
be a mentor, or have questions or comments please e-mail
the journal club at [email protected]
Join us next month when we hear the EMPA-REG Trial from
Dr. Michelle Lew, PharmD, BCPS PGY-2 Cardiology resident at
USC with Dr. Craig Beavers, PharmD, FAHA, AACC, BCPS (AQ-
Cardiology), CACP as her mentor.


















