Inflammatory Bowel Disease - ACCP
22
PSAP-VII • Gastroenterology and Nutrition 27 Inflammatory Bowel Disease Learning Objectives 1. Classify the severity of Crohn disease (CD) and ulcerative colitis (UC) on the basis of clinical fea- tures and endoscopic and biopsy findings. 2. For an individual patient, design an optimal pharmacotherapy plan for CD or UC. 3. Analyze risk factors for the development of adverse effects related to the treatment of CD or UC and develop a plan to avoid these effects. 4. Develop a pharmacotherapy plan for the treatment of complications of CD or UC. 5. Evaluate the role of adjunctive agents in the treat- ment of inflammatory bowel disease (IBD). 6. For an individual patient, design a health mainte- nance plan including appropriate surveillance, pro- phylaxis, and treatment of potential complications of IBD. 7. Apply evidence from the primary literature on adherence issues during induction versus mainte- nance of remission of CD or UC. Introduction Inflammatory bowel disease (IBD) includes chronic relapsing and remiing diseases such as ulcerative colitis (UC) and Crohn disease (CD). Ulcerative coli- tis, which involves mucosal inflammation, is confined mainly to the rectum and colon, with rare involvement of the terminal ileum. Crohn disease is a transmural inflammatory disease that can affect any part of the gastrointestinal (GI) tract from the mouth to the anus. Although the etiologies of both forms of IBD are unknown, the diseases have some common pathophysi- ologic features. Both diseases can affect any age group, and both exhibit a bimodal age of onset, with the peak incidence of diagnosis occurring in the second and third decades and a second peak between 60 and 80 years of age. e incidence and prevalence of UC (estimated to be 3–15 per 100,000 and 80–120 per 100,000, respec- tively) have remained constant for many decades. e incidence and prevalence of CD in the United States are estimated to be 4–9 per 100,000 and 20–50 per 100,000, respectively. In contrast to UC, the incidence and preva- lence of CD in the United States are increasing. Etiology Many theories regarding the etiology and pathogen- esis of IBD have been proposed. ese theories include infectious, psychosomatic, social, metabolic, vascular, genetic, allergic, autoimmune, and immune-mediated factors. Current theories do not indicate a single caus- ative factor; rather, the interplay of genetics, intesti- nal flora, environmental factors, and immune response most likely leads to the development of IBD. A familial occurrence of IBD has been established that suggests genetics is a causative factor. is has been supported by monozygotic twin concordance rates that are higher than those in dizygotic twins. Initial Inflammatory Bowel Disease By Sheila M. Wilhelm, Pharm.D., BCPS; and Pramodini Kale-Pradhan, Pharm.D. Reviewed by Nancy S. Yunker, Pharm.D., BCPS; and Anne L. Hume, Pharm.D., FCCP, BCPS Baseline Review Resources e goal of PSAP is to provide only the most recent (past 3–5 years) information or topics. Chapters do not pro- vide an overall review. Suggested resources for background information on this topic include: • DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, eds. Pharmacotherapy: A Pathophysiologic Approach, 8th ed. New York: McGraw-Hill, 2011:chap 41. • Podolsky DK. Inflammatory bowel disease. N Engl J Med 2002;347:417–29. • Danese S, Fiocchi C. Ulcerative colitis. N Engl J Med 2011;365:1713–25.
Transcript of Inflammatory Bowel Disease - ACCP

PSAP-VII • Gastroenterology and Nutrition 27 Inflammatory Bowel Disease
Learning Objectives 1. Classify the severity of Crohn disease (CD) and
ulcerative colitis (UC) on the basis of clinical fea-tures and endoscopic and biopsy findings.
2. For an individual patient, design an optimal pharmacotherapy plan for CD or UC.
3. Analyze risk factors for the development of adverse effects related to the treatment of CD or UC and develop a plan to avoid these effects.
4. Develop a pharmacotherapy plan for the treatment of complications of CD or UC.
5. Evaluate the role of adjunctive agents in the treat-ment of inflammatory bowel disease (IBD).
6. For an individual patient, design a health mainte-nance plan including appropriate surveillance, pro-phylaxis, and treatment of potential complications of IBD.
7. Apply evidence from the primary literature on adherence issues during induction versus mainte-nance of remission of CD or UC.
Introduction Inflammatory bowel disease (IBD) includes chronic relapsing and remitting diseases such as ulcerative colitis (UC) and Crohn disease (CD). Ulcerative coli-tis, which involves mucosal inflammation, is confined mainly to the rectum and colon, with rare involvement of the terminal ileum. Crohn disease is a transmural
inflammatory disease that can affect any part of the gastrointestinal (GI) tract from the mouth to the anus. Although the etiologies of both forms of IBD are unknown, the diseases have some common pathophysi-ologic features. Both diseases can affect any age group, and both exhibit a bimodal age of onset, with the peak incidence of diagnosis occurring in the second and third decades and a second peak between 60 and 80 years of age. The incidence and prevalence of UC (estimated to be 3–15 per 100,000 and 80–120 per 100,000, respec-tively) have remained constant for many decades. The incidence and prevalence of CD in the United States are estimated to be 4–9 per 100,000 and 20–50 per 100,000, respectively. In contrast to UC, the incidence and preva-lence of CD in the United States are increasing.
Etiology Many theories regarding the etiology and pathogen-esis of IBD have been proposed. These theories include infectious, psychosomatic, social, metabolic, vascular, genetic, allergic, autoimmune, and immune-mediated factors. Current theories do not indicate a single caus-ative factor; rather, the interplay of genetics, intesti-nal flora, environmental factors, and immune response most likely leads to the development of IBD. A familial occurrence of IBD has been established that suggests genetics is a causative factor. This has been supported by monozygotic twin concordance rates that are higher than those in dizygotic twins. Initial
Inflammatory Bowel Disease
By Sheila M. Wilhelm, Pharm.D., BCPS; and Pramodini Kale-Pradhan, Pharm.D.
Reviewed by Nancy S. Yunker, Pharm.D., BCPS; and Anne L. Hume, Pharm.D., FCCP, BCPS
Baseline Review Resources The goal of PSAP is to provide only the most recent (past 3–5 years) information or topics. Chapters do not pro-vide an overall review. Suggested resources for background information on this topic include:• DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, eds. Pharmacotherapy: A Pathophysiologic
Approach, 8th ed. New York: McGraw-Hill, 2011:chap 41.• Podolsky DK. Inflammatory bowel disease. N Engl J Med 2002;347:417–29.• Danese S, Fiocchi C. Ulcerative colitis. N Engl J Med 2011;365:1713–25.

PSAP-VII • Gastroenterology and Nutrition28Inflammatory Bowel Disease
discovery of the association between NOD2/CARD15 variants and ileal CD has led to further, genome-wide investigation and identification of several genes associ-ated with CD, UC, or both. Intestinal microbiota, especially Mycobacterium avium paratuberculosis and certain species of Escherichia coli, have been implicated as causative factors for IBD by initiating an immune response against the gut flora in patients who have an underlying susceptibility to developing the disease. Patients with IBD have higher concentrations of flora within the GI mucosa compared with patients without bowel inflammation; however, the qualitative mix of flora may affect the disease course because some intestinal bacteria such as lactobacilli, bifidobacteria, and streptococci possess an anti-inflam-matory effect. Inflammatory bowel disease has been more common in North America and Northern Europe. However, epi-demiologic research has indicated that IBD is becoming more prevalent where there were previously few cases of IBD such as the Asia-Pacific area. Environmental fac-tors such as diet, cigarette smoking, or infections may play a role in this trend. Cigarette smoking is definitively linked to IBD. In CD, cigarette smoking worsens the dis-ease and increases symptoms, relapses, hospitalizations, and surgeries. In UC, cigarette smoking has a protective effect on the clinical course. Smoking may affect IBD by altering one or more of the following: the inflamma-tory cascade, immune response, mucus production, gut motility, permeability and bloodflow, or platelet activa-tion. However, the mechanisms for the opposing effects of smoking on CD and UC are not fully understood. Derangement of the innate and adaptive immune responses may be the uniting factor in the etiology of IBD. Intestinal macrophages are generally noninflammatory cells, but in IBD, an increased proportion of macrophages produce proinflammatory cytokines including tumor necrosis factor alpha (TNF-α) and interleukin-23. When compared with individuals without IBD, those with CD have elevated intestinal helper T-1 cells (which produce interferon gamma and interleukin-12) and those with UC have elevated helper T-2 cells (which produce inter-leukin-5 and interleukin-13).
Diagnosis Clinical Signs and Symptoms Patients with IBD may experience diarrhea with or without rectal bleeding, abdominal tenderness or pain, and weight loss. Compared with CD, UC is more likely to present with blood in the stool, rectal urgency, or tenesmus.
Intestinal Complications Intestinal complications with CD reflect the trans-mural nature of the disease and include fissures or fis-tulas, linear clefts, and strictures that can lead to intes-tinal obstruction. Crohn disease also exhibits areas of disease within the GI tract, often with a cobblestone appearance, interspersed with healthy tissue, some-times referred to as skip lesions. Intra-abdominal and perianal abscesses complicate CD. In UC, mucosal and submucosal involvement results in crypt abscesses, but not the fistulas and other complications present in CD. Ulcerative colitis exhibits a continuous pattern of inflammation without healthy tissue between lesions. Clinical signs of complications of IBD can include pal-lor; cachexia; abdominal mass or tenderness; or abscess, especially with CD. Toxic megacolon is a rare and potentially fatal com-plication that is associated with UC more often than with CD. An estimated 10% of UC admissions and 2.3% of CD admissions occurred because of toxic megacolon at one hospital during a 19-year period. Toxic megaco-lon presents as dilation of the ascending and transverse colon to greater than 6 cm with a potential for colonic rupture. Management should include supportive med-ical care including intravenous fluids, electrolyte sup-plementation, broad-spectrum antibiotics, and, poten-tially corticosteroids. In addition, surgical interven-tion may be needed, especially if colonic perforation has occurred.
Extraintestinal Complications Inflammatory bowel disease is associated with sev-eral extraintestinal complications primarily related to systemic inflammation. Joint-related complications may include ankylosing spondylitis, sacroiliitis, and periph-eral arthritis of large or small joints. Cutaneous manifes-tations include erythema nodosum and pyoderma gan-grenosum. Ocular inflammation such as uveitis, episcler-itis, or scleroconjunctivitis occurs in up to 3% of patients with IBD and often presents with eye redness, burning, itching, pain, and vision changes. Significant symptoms and any vision changes require urgent referral to an oph-thalmologist. Ocular complications often respond well to treatment of the underlying IBD, with a possible need for topical ophthalmic therapy as well. Hepatic primary sclerosing cholangitis (PSC) affects 5% of patients with UC and 3.6% of patients with CD.
Abbreviations in This Chapter CD Crohn diseaseCRC Colorectal cancerGI GastrointestinalIBD Inflammatory bowel diseasePSC Primary sclerosing cholangitisTNF-α Tumor necrosis factor alphaTPMT Thiopurine S-methyltransferaseUC Ulcerative colitis

PSAP-VII • Gastroenterology and Nutrition 29 Inflammatory Bowel Disease
Hepatic PSC is marked by progressive inflammation, scarring, and destruction of the bile ducts. Patients with PSC often present with fatigue, itching, and jaundice, and this condition results in an elevated risk of cholan-giocarcinoma. Patients who develop PSC progress to end-stage liver disease and transplantation or death in a median of 12–18 years. Other complications of IBD related to malabsorption include anemia, cholelithiasis, nephrolithiasis, and metabolic bone disease.
Endoscopy and Imaging Imaging, endoscopic evaluation, and biopsy can con-firm the diagnosis of IBD and differentiate between UC and CD. Endoscopy is routinely used to diagnose, assess disease location, and obtain samples for his-tology. Depending on symptoms, upper endoscopy, colonoscopy, or proctosigmoidoscopy can be used. Video-capsule endoscopy entails swallowing a small capsule that transmits images as it passes through the GI tract. This noninvasive endoscopic method may be used in the diagnosis of UC or CD; however, in up to 13% of patients with CD, the video-capsule is retained, which may require surgical removal. Before using video-capsule endoscopy, imaging studies may assess whether small bowel strictures are present; these are a contrain-dication to using the capsule because of the elevated risk of capsule retention. A patency capsule has been devel-oped to assess small intestinal strictures; if the patency capsule is swallowed and retained, it will dissolve in 40–80 hours, and video-capsule endoscopy should not be used. Imaging studies including ultrasonography, computed tomography, or magnetic resonance imaging may be helpful in identifying disease location and intra-abdominal complications. Histologic sampling is useful to determine the depth of involvement and the patho-physiologic features of the disease.
Genetic Testing Genetic testing is not routinely recommended for the diagnosis of IBD. In the future, genetic analyses may help differentiate between CD and UC, as well as pre-dict disease risk, severity, course, and response to differ-ent treatments. An estimated 60 susceptibility loci have been associated with IBD, 20 of which are associated with both CD and UC; 23 are specific to CD, and 21 are specific to UC. Given the number of involved genes and the heterogeneity of the implicated genes, universal genetic screening would not be useful at this time.
Determining Disease Activity Location The extent of disease and specific location of lesions are important factors for determining disease activ-ity and appropriate treatment. The continuous lesions of UC are defined by their proximal border. Proctitis is
inflammation confined to the rectum; distal or left-sided disease extends to the splenic flexure encompassing the descending colon; and extensive disease extends proxi-mally beyond the descending colon and can encompass all or part of the colon with the potential for involving the terminal ileum as well. Although CD can occur anywhere in the GI tract, the ileum and colon are most often affected, which makes distinguishing CD from UC difficult in some patients. Unlike UC, perianal manifestations of CD may be pres-ent before bowel symptoms. Some patients may pres-ent with CD confined to the jejunum and ileum. This is rare and may be associated with multiple stenoses, bac-terial overgrowth, and protein-losing enteropathy. Gas-tric and duodenal CD may present with epigastric pain, nausea, and vomiting; these distinguish it from CD confined to the ileum and colon.
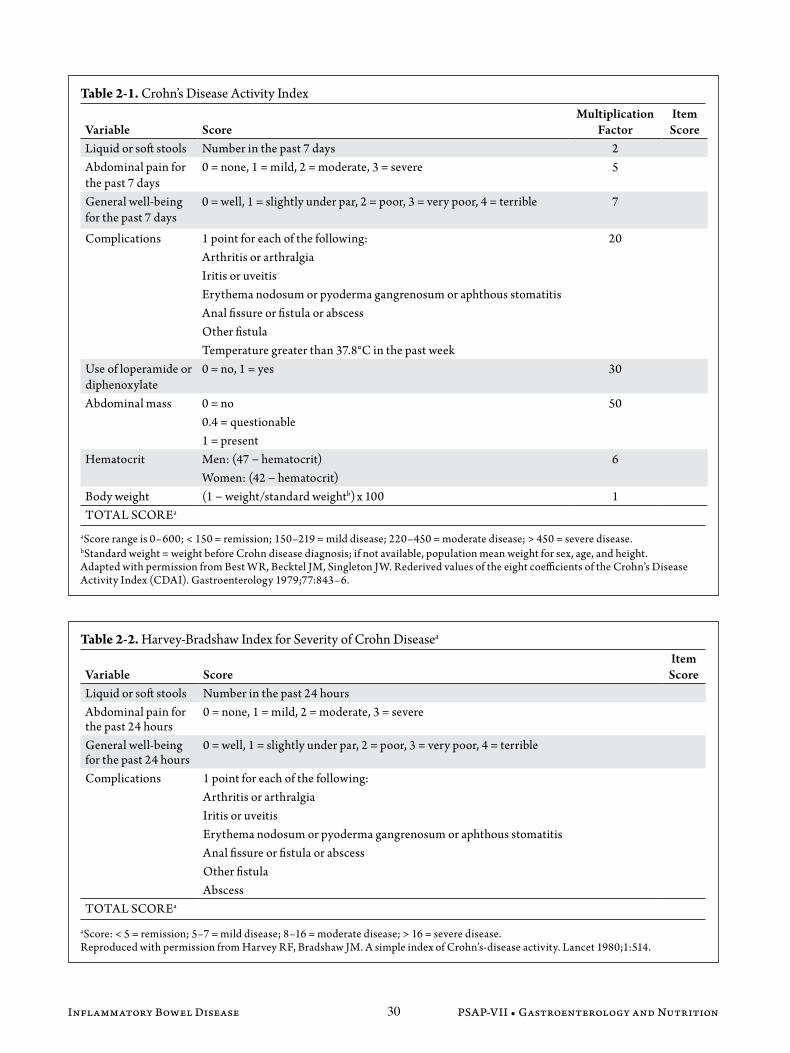
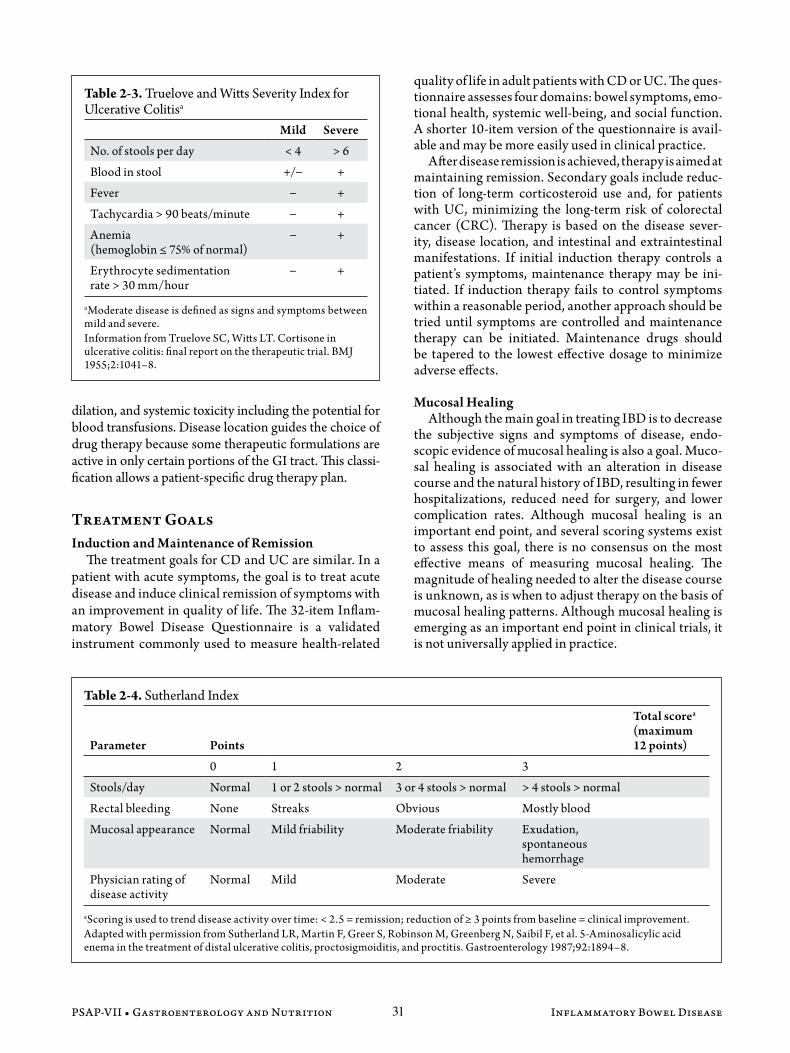
Severity Severity is another factor that determines disease activity and the preferred therapeutic approach. Several rating scales have been created to assess severity consis-tently and objectively. The scales incorporate subjective and objective patient-reported symptoms such as num-ber of bowel movements; presence or absence of blood in the stool; abdominal pain, cramping, or discomfort; and extraintestinal symptoms. Some scales incorporate lab-oratory findings such as hemoglobin or hematocrit and erythrocyte sedimentation rate. The patient’s or physi-cian’s global assessment may be considered. Some indices include an assessment of mucosal appearance based on endoscopic findings. For CD, the Crohn’s Disease Activ-ity Index (Table 2-1), Harvey-Bradshaw Index for Sever-ity of Crohn Disease (Table 2-2), and Perianal Disease Activity Index are used in clinical trials to determine dis-ease severity and assess improvement of subjects. In UC, the Truelove and Witts Severity Index (Table 2-3) and Sutherland Index (Table 2-4), also known as the Ulcer-ative Colitis Disease Activity Index, are used.
Disease Classification Treatment guidelines classify a Crohn’s Disease Activity Index of 150–219 as mild-moderate CD, a score of 220–450 as moderate-severe, and a score greater than 450 as severe-fulminant. According to treatment guide-lines and on the basis of the Truelove and Witts index, mild UC presents with less than four stools daily with or without blood, no systemic signs of toxicity, and a normal erythrocyte sedimentation rate, whereas mod-erate disease presents with more than four daily stools and limited signs of toxicity. Severe disease is defined as more than six bloody stools daily with systemic toxicity such as fever, tachycardia, anemia, and elevated eryth-rocyte sedimentation rate. Fulminant disease may pres-ent with more than 10 stools per day with continuous bleeding, abdominal tenderness and distension, colonic
PSAP-VII • Gastroenterology and Nutrition30Inflammatory Bowel Disease
Table 2-1. Crohn’s Disease Activity Index
Variable ScoreMultiplication
FactorItem Score
Liquid or soft stools Number in the past 7 days 2Abdominal pain for the past 7 days
0 = none, 1 = mild, 2 = moderate, 3 = severe 5
General well-being for the past 7 days
0 = well, 1 = slightly under par, 2 = poor, 3 = very poor, 4 = terrible 7
Complications 1 point for each of the following:Arthritis or arthralgiaIritis or uveitisErythema nodosum or pyoderma gangrenosum or aphthous stomatitisAnal fissure or fistula or abscessOther fistulaTemperature greater than 37.8°C in the past week
20
Use of loperamide or diphenoxylate
0 = no, 1 = yes 30
Abdominal mass 0 = no0.4 = questionable1 = present
50
Hematocrit Men: (47 − hematocrit)Women: (42 − hematocrit)
6
Body weight (1 − weight/standard weightb) x 100 1TOTAL SCOREa
aScore range is 0–600; < 150 = remission; 150–219 = mild disease; 220–450 = moderate disease; > 450 = severe disease.bStandard weight = weight before Crohn disease diagnosis; if not available, population mean weight for sex, age, and height.Adapted with permission from Best WR, Becktel JM, Singleton JW. Rederived values of the eight coefficients of the Crohn’s Disease Activity Index (CDAI). Gastroenterology 1979;77:843–6.
Table 2-2. Harvey-Bradshaw Index for Severity of Crohn Diseasea
Variable ScoreItem Score
Liquid or soft stools Number in the past 24 hoursAbdominal pain for the past 24 hours
0 = none, 1 = mild, 2 = moderate, 3 = severe
General well-being for the past 24 hours
0 = well, 1 = slightly under par, 2 = poor, 3 = very poor, 4 = terrible
Complications 1 point for each of the following:Arthritis or arthralgiaIritis or uveitisErythema nodosum or pyoderma gangrenosum or aphthous stomatitisAnal fissure or fistula or abscessOther fistulaAbscess
TOTAL SCOREa
aScore: < 5 = remission; 5–7 = mild disease; 8–16 = moderate disease; > 16 = severe disease.Reproduced with permission from Harvey RF, Bradshaw JM. A simple index of Crohn’s-disease activity. Lancet 1980;1:514.
PSAP-VII • Gastroenterology and Nutrition 31 Inflammatory Bowel Disease
dilation, and systemic toxicity including the potential for blood transfusions. Disease location guides the choice of drug therapy because some therapeutic formulations are active in only certain portions of the GI tract. This classi-fication allows a patient-specific drug therapy plan.
Treatment Goals Induction and Maintenance of Remission The treatment goals for CD and UC are similar. In a patient with acute symptoms, the goal is to treat acute disease and induce clinical remission of symptoms with an improvement in quality of life. The 32-item Inflam-matory Bowel Disease Questionnaire is a validated instrument commonly used to measure health-related
quality of life in adult patients with CD or UC. The ques-tionnaire assesses four domains: bowel symptoms, emo-tional health, systemic well-being, and social function. A shorter 10-item version of the questionnaire is avail-able and may be more easily used in clinical practice. After disease remission is achieved, therapy is aimed at maintaining remission. Secondary goals include reduc-tion of long-term corticosteroid use and, for patients with UC, minimizing the long-term risk of colorectal cancer (CRC). Therapy is based on the disease sever-ity, disease location, and intestinal and extraintestinal manifestations. If initial induction therapy controls a patient’s symptoms, maintenance therapy may be ini-tiated. If induction therapy fails to control symptoms within a reasonable period, another approach should be tried until symptoms are controlled and maintenance therapy can be initiated. Maintenance drugs should be tapered to the lowest effective dosage to minimize adverse effects.
Mucosal Healing Although the main goal in treating IBD is to decrease the subjective signs and symptoms of disease, endo-scopic evidence of mucosal healing is also a goal. Muco-sal healing is associated with an alteration in disease course and the natural history of IBD, resulting in fewer hospitalizations, reduced need for surgery, and lower complication rates. Although mucosal healing is an important end point, and several scoring systems exist to assess this goal, there is no consensus on the most effective means of measuring mucosal healing. The magnitude of healing needed to alter the disease course is unknown, as is when to adjust therapy on the basis of mucosal healing patterns. Although mucosal healing is emerging as an important end point in clinical trials, it is not universally applied in practice.
Table 2-3. Truelove and Witts Severity Index for Ulcerative Colitisa
Mild Severe
No. of stools per day < 4 > 6
Blood in stool +/− +
Fever − +
Tachycardia > 90 beats/minute − +
Anemia (hemoglobin ≤ 75% of normal)
− +
Erythrocyte sedimentation rate > 30 mm/hour
− +
aModerate disease is defined as signs and symptoms between mild and severe.Information from Truelove SC, Witts LT. Cortisone in ulcerative colitis: final report on the therapeutic trial. BMJ 1955;2:1041–8.
Table 2-4. Sutherland Index
Parameter Points
Total scorea (maximum 12 points)
0 1 2 3
Stools/day Normal 1 or 2 stools > normal 3 or 4 stools > normal > 4 stools > normal
Rectal bleeding None Streaks Obvious Mostly blood
Mucosal appearance Normal Mild friability Moderate friability Exudation, spontaneous hemorrhage
Physician rating of disease activity
Normal Mild Moderate Severe
aScoring is used to trend disease activity over time: < 2.5 = remission; reduction of ≥ 3 points from baseline = clinical improvement.Adapted with permission from Sutherland LR, Martin F, Greer S, Robinson M, Greenberg N, Saibil F, et al. 5-Aminosalicylic acid enema in the treatment of distal ulcerative colitis, proctosigmoiditis, and proctitis. Gastroenterology 1987;92:1894–8.

PSAP-VII • Gastroenterology and Nutrition32Inflammatory Bowel Disease
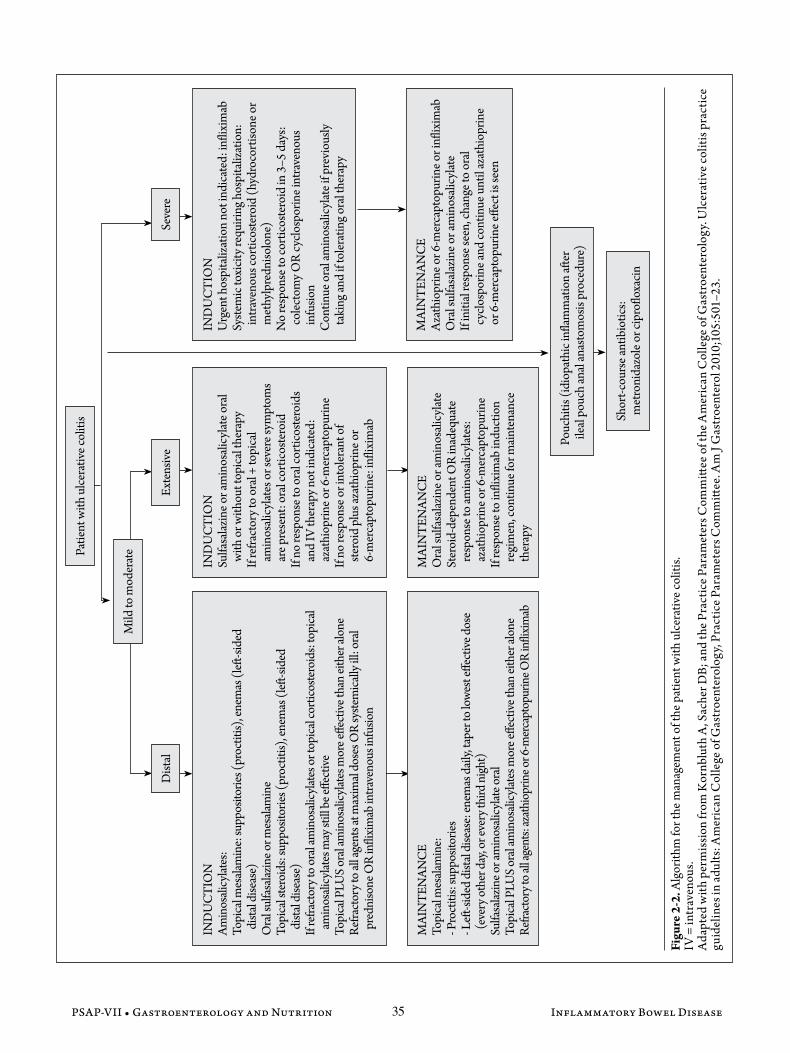
Treatment Pharmacotherapy Table 2-5 lists the drug therapy and common dos-ages used in the treatment of IBD. Figure 2-1 and Figure 2-2 outline approaches to the treatment of CD and UC, respectively.
Aminosalicylates Sulfasalazine is a combination of sulfapyridine and mesalamine. Mesalamine is the active compo-nent that provides anti-inflammatory effects in the GI tract, whereas the sulfapyridine portion is responsi-ble for most of the adverse effects with the drug. Sul-fasalazine may sometimes lead to anemia because of impaired folic acid absorption and folate deficiency; therefore, supplemental folic acid 1 mg/day is often recommended. Sulfasalazine is also associated with dose-related toxicities including nausea, vomiting, diarrhea, headache, and arthralgias. In addition, idio-syncratic reactions include hepatotoxicity, bone mar-row suppression, pancreatitis, pneumonitis, and inter-stitial nephritis. Sulfasalazine is contraindicated in patients with a sulfa allergy. Sulfasalazine is still used because of its low cost, but mesalamine alone is often used as first-line therapy because of its better adverse effect profile. Mesalamine is available as suppositories and enemas, as well as an oral therapy. The different formulations are often used in combination to allow targeted drug delivery in the GI tract. Topical therapy (rectal administration) provides more rapid symptom control than oral therapy, and it should be used pref-erentially for proctitis or distal disease with or with-out oral therapy, whereas oral therapy should be used for small bowel or colonic disease. Disease that has not responded to oral aminosalicylates may still respond to therapy with combined oral and topical therapy. These agents are useful for induction and maintenance therapy in IBD. Although aminosalicylates are well tol-erated, exacerbation of colitis may occur in up to 4% of patients when initiating these agents. This effect may not be recognized in patients receiving corticosteroids, which may mask the symptoms of colitis.
Corticosteroids Corticosteroids are used for the induction of remission in both CD and UC. Oral, intravenous, and topical forms of corticosteroids are used to treat IBD. Corticosteroids are associated with many adverse effects, especially when administered systemically. Acutely, they can cause hyper-glycemia, fluid retention, hypertension, insomnia, or mood changes. Chronic adverse effects include osteopo-rosis, thinning of the skin, cataracts, weight gain, and fat redistribution. Because of these chronic adverse effects and questionable efficacy, corticosteroids are not recom-mended for maintenance therapy.
Unlike hydrocortisone, methylprednisolone, and prednisone, oral budesonide undergoes extensive first-pass metabolism, with only 10% to 15% systemically absorbed; thus, its effects are confined to the GI tract with more limited systemic toxicity. Patients taking budesonide may still experience adverse effects simi-lar to those with conventional corticosteroids; however, the incidence is 35% lower because of the limited sys-temic exposure. Oral budesonide is typically used as a first-line agent either alone or combined with an ami-nosalicylate for induction or maintenance of remission in mild to moderate CD involving the ileum or ascend-ing colon (right-sided disease). Topical corticosteroids are effective for mild to moderate UC that is limited to the descending colon and rectum; however, they are less effective than topical aminosalicylates and should be reserved for patients whose disease fails to respond to aminosalicylate therapy.
Immunomodulators Thiopurines Azathioprine and 6-mercaptopurine are thiopurine immunosuppressants used to maintain the remission of both CD and UC. They are reserved for patients whose disease has not responded to other therapies or who are dependent on corticosteroids. Thiopurines are adminis-tered with other acute therapies (e.g., aminosalicylates, corticosteroids) because their effects are often delayed for several weeks to months. Thiopurines are associated with dose-related and idiosyncratic reactions. Dose-related reactions include nausea, malaise, infections, hepatitis, and myelosuppression. A complete blood cell count should be obtained before initiating therapy and every week for the first month, every 2 weeks for months 2 and 3, and then monthly. Idiosyncratic reac-tions include fever, rash, arthralgias, and pancreatitis. Thiopurine S-methyltransferase (TPMT) is an enzyme involved in the metabolism of thiopurines. Polymorphisms of TPMT are common and affect the accumulation of toxic metabolites associated with myelosuppression or hepatotoxicity. The activity of TPMT should be genotypically or phenotypically assessed before initiating therapy to determine whether a patient is a candidate for thiopurine therapy and, if so, the dosage that should be initiated. An estimated 0.3% of patients are homozygous for the nonfunctional-type alleles and have low-to-absent enzyme activity, which confers the highest risk of myelosuppression compared with other genotypes. From 6% to 11% are heterozygous and intermediate methylators, whereas 89% to 94% are homozygous for the wild-type allele and have normal to high enzyme activity.
Other Immunosuppressive Agents Continuous intravenous cyclosporine infusion at 2–4 mg/kg/day is used in patients with severe to fulminant

PSAP-VII • Gastroenterology and Nutrition 33 Inflammatory Bowel Disease
Tabl
e 2-
5. D
rug
Ther
apy
for I
nflam
mat
ory
Bow
el D
iseas
eP
rodu
ctTr
ade
Nam
eFo
rmul
atio
nIn
duct
ion
Dos
age
Mai
nten
ance
Dos
age
Site
of A
ctio
nA
min
osal
icyl
ates
Sulfa
sala
zine
Azu
lfidi
neTa
blet
, ent
eric
coat
ed ta
blet
1–1.
5 g f
our t
imes
/day
500
mg t
hree
or f
our t
imes
/day
Col
onM
esal
amin
eC
anas
aSu
ppos
itory
1 g/
day a
t bed
time
1 g/
day a
t bed
time
Rec
tum
Row
asa,
Sal
ofal
kEn
ema
4 g/
day a
t bed
time
4 g/
day a
t bed
time
Rec
tum
, des
cend
ing c
olon
Asa
col, A
saco
l H
DTa
blet
coat
ed w
ith E
udra
git S
(d
elay
ed-re
leas
e acr
ylic
resin
)80
0–16
00 m
g thr
ee ti
mes
/day
800
mg t
wic
e dai
ly o
r 400
mg f
our
times
/day
; Asa
col H
D n
ot in
dica
ted
Dist
al il
eum
, col
on
Lial
daM
ulti
Mat
rix t
able
t2.
4–4.
8 g o
nce d
aily
2.4
g onc
e dai
lyD
istal
ileu
m, c
olon
Pent
asa
Cap
sule
coat
ed in
ethy
lcel
lulo
se
mic
rogr
anul
es1
g fou
r tim
es/d
ay1
g fou
r tim
es/d
aySm
all b
owel
, col
on
Apr
isoIN
TEL
LIC
OR
caps
ule
Not
indi
cate
d1.
5 g o
nce d
aily
Dist
al il
eum
, col
onO
lsala
zine
Dip
entu
mD
imer
of m
esal
amin
e in
oral
caps
ule
1–3
g/da
y50
0 m
g tw
ice d
aily
Col
onBa
lsala
zide
Col
azal
Cap
sule
2.25
g th
ree t
imes
/day
Not
indi
cate
dC
olon
Cor
ticos
tero
ids
Pred
niso
neTa
blet
40–6
0 m
g/da
yN
ot in
dica
ted,
tape
r and
disc
ontin
ueN
onsp
ecifi
cH
ydro
cort
isone
Solu
-Cor
tef
Intr
aven
ous
100
mg t
hree
tim
es/d
ayN
ot in
dica
ted,
conv
ert t
o or
al th
erap
y an
d ta
per t
o di
scon
tinue
Non
spec
ific
Hyd
roco
rtiso
neC
orte
nem
aEn
ema
100
mg/
day a
t bed
time
Tape
r and
disc
ontin
ueR
ectu
m, d
esce
ndin
g col
onH
ydro
cort
isone
Cor
tifoa
mFo
am80
mg o
nce o
r tw
ice d
aily
80 m
g onc
e dai
ly, t
aper
and
disc
ontin
ueR
ectu
m, d
esce
ndin
g col
onH
ydro
cort
isone
Anu
sol-H
C,
othe
rsSu
ppos
itory
25 m
g tw
ice d
aily
Tape
r and
disc
ontin
ueR
ectu
m
Met
hylp
redn
isolo
neSo
lu-M
edro
lIn
trav
enou
s20
mg t
hree
tim
es/d
ay O
R
60 m
g onc
e dai
lyN
ot in
dica
ted,
conv
ert t
o or
al th
erap
y an
d ta
per t
o di
scon
tinue
Non
spec
ific
Bude
soni
deEn
toco
rt E
CEn
teric
-coa
ted
tabl
et9
mg o
nce d
aily
6 m
g onc
e dai
ly fo
r up
to 3
mon
ths
Ileum
, asc
endi
ng co
lon
Imm
unom
odul
ator
s
Non
spec
ific
Aza
thio
prin
e Im
uran
, Aza
san
Tabl
etN
ot in
dica
ted
1–3
mg/
kg o
nce d
aily
6-M
erca
ptop
urin
ePu
rine
thol
Tabl
etN
ot in
dica
ted
1–1.
5 m
g/kg
onc
e dai
lyM
etho
trex
ate
Trex
all
Subc
utan
eous
or i
ntra
mus
cula
r15
–25
mg o
nce w
eekl
y15
mg o
nce w
eekl
yC
yclo
spor
ine
Neo
ral,
Sand
imm
une
Intr
aven
ous o
r ora
l2–
4 m
g/kg
/day
intr
aven
ously
2.3–
3 m
g/kg
ora
lly ev
ery 1
2 ho
urs
Tacr
olim
usPr
ogra
fC
apsu
le0.
05 m
g/kg
twic
e dai
lyN
ot st
udie
dB
iolo
gic a
gent
sN
onsp
ecifi
cIn
flixi
mab
Rem
icad
eIn
trav
enou
s inf
usio
n5
mg/
kg w
eeks
0, 2
, and
65–
10 m
g/kg
ever
y 8 w
eeks
Ada
limum
abH
umira
Subc
utan
eous
160
mg w
eek
0, 8
0 m
g wee
k 2
40 m
g eve
ry o
ther
wee
kC
erto
lizum
ab p
egol
Cim
zia
Subc
utan
eous
40
0 m
g wee
ks 0
, 2, a
nd 4
400
mg e
very
4 w
eeks
Nat
aliz
umab
Tysa
bri
Intr
aven
ous i
nfus
ion
300
mg w
eek
030
0 m
g eve
ry 4
wee
ksA
ntim
icro
bial
sN
onsp
ecifi
cM
etro
nida
zole
Flag
ylTa
blet
10–2
0 m
g/kg
/day
in d
ivid
ed d
oses
10–2
0 m
g/kg
/day
in d
ivid
ed d
oses
Cip
roflo
xaci
nC
ipro
Tabl
et50
0 m
g tw
ice d
aily
500
mg t
wic
e dai
ly

PSAP-VII • Gastroenterology and Nutrition34Inflammatory Bowel Disease
Figu
re 2
-1. T
reat
men
t alg
orith
m fo
r the
pat
ient
with
Cro
hn d
iseas
e.
IV =
intra
veno
us; T
NF-
α =
tum
or n
ecro
sis fa
ctor
alph
a.In
form
atio
n fro
m L
icht
enst
ein
GR
, Han
auer
SB,
San
dbor
n W
J; Pr
actic
e Par
amet
ers C
omm
ittee
of t
he A
mer
ican
Col
lege
of G
astro
ente
rolo
gy. M
anag
emen
t of C
rohn
’s di
seas
e in
adul
ts. A
m J
Gas
troen
tero
l 200
9;10
4:46
5–83
.
Patie
nt w
ith C
rohn
dise
ase
MA
INT
ENA
NC
ETa
per s
tero
ids
Aza
thio
prin
e or 6
-mer
capt
opur
ine
or m
etho
trex
ate
Infli
xim
abIn
flixi
mab
+ a
zath
iopr
ine i
f no
resp
onse
to m
onot
hera
pyN
atal
izum
abIND
UC
TIO
NPr
edni
sone
x 7–
28 d
ays
If in
tole
rant
of o
r not
resp
onsiv
e to
pred
niso
ne: T
NF-
α an
tago
nist
: in
flixi
mab
; ada
limum
ab;
cert
oliz
umab
peg
olO
RM
etho
trex
ate
If n
o re
spon
se to
TN
F-α
anta
goni
st: n
atal
izum
ab
MA
INT
ENA
NC
ETr
ansit
ion
to o
ral t
hera
py,
tape
r cor
ticos
tero
ids
Aza
thio
prin
e or
6-m
erca
ptop
urin
eIn
flixi
mab
Infli
xim
ab +
aza
thio
prin
e for
pa
tient
s who
did
not
resp
ond
to m
onot
hera
pyN
atal
izum
ab
IND
UC
TIO
NIV
cort
icos
tero
id
If n
o re
spon
se to
IV
cort
icos
tero
ids:
cons
ider
IV
cycl
ospo
rine
or t
acro
limus
If u
nabl
e to
mai
ntai
n nu
triti
onal
in
take
, con
sider
ele
men
tal
feed
ing
or p
aren
tera
l nu
triti
on a
fter 5
–7 d
ays
Infli
xim
ab e
spec
ially
if
fistu
las n
ot cl
osin
g w
ith st
anda
rd th
erap
y (s
tero
ids,
antib
iotic
s, im
mun
omod
ulat
ors)
Fist
uliz
ing
dise
ase
Met
roni
dazo
le
with
or w
ithou
t ci
profl
oxac
in
Peria
nal d
iseas
eSe
vere
dise
ase
Mod
erat
e to
seve
re d
iseas
e
MA
INT
ENA
NC
EIf
ilea
l or a
scen
ding
colo
n:
bude
soni
de
Am
inos
alic
ylat
es m
ay n
ot b
e eff
ectiv
e for
mai
nten
ance
of
rem
issio
n, b
ut m
ay b
e trie
d
IND
UC
TIO
NM
esal
amin
eO
RIf
ileo
colo
nic o
r col
onic
dise
ase:
su
lfasa
lazi
ne
If n
o re
spon
se to
sulfa
sala
zine
, co
nsid
er m
etro
nida
zole
If il
eal o
r asc
endi
ng co
lon:
bu
deso
nide
with
or w
ithou
t an
amin
osal
icyl
ate
Mild
to m
oder
ate i
leal
, ile
ocol
onic
, or c
olon
ic d
iseas
e
PSAP-VII • Gastroenterology and Nutrition 35 Inflammatory Bowel Disease
Figu
re 2
-2. A
lgor
ithm
for t
he m
anag
emen
t of t
he p
atie
nt w
ith u
lcer
ativ
e col
itis.
IV =
intr
aven
ous.
Ada
pted
with
per
mis
sion
from
Kor
nblu
th A
, Sac
her D
B; a
nd th
e Pra
ctic
e Par
amet
ers C
omm
ittee
of t
he A
mer
ican
Col
lege
of G
astr
oent
erol
ogy.
Ulc
erat
ive c
oliti
s pra
ctic
e gu
idel
ines
in ad
ults
: Am
eric
an C
olle
ge o
f Gas
troe
nter
olog
y, Pr
actic
e Par
amet
ers C
omm
ittee
. Am
J G
astr
oent
erol
201
0;10
5:50
1–23
.
Shor
t-cou
rse a
ntib
iotic
s: m
etro
nida
zole
or c
ipro
floxa
cin
Pouc
hitis
(idi
opat
hic i
nflam
mat
ion
after
ile
al p
ouch
anal
anas
tom
osis
proc
edur
e)
Exte
nsiv
e
MAI
NT
ENAN
CE
Ora
l sul
fasa
lazin
e or a
min
osal
icyl
ate
Ster
oid-
depe
nden
t OR
inad
equa
te
resp
onse
to am
inos
alic
ylat
es:
azat
hiop
rine o
r 6-m
erca
ptop
urin
eIf
resp
onse
to in
flixi
mab
indu
ctio
n re
gim
en, c
ontin
ue fo
r mai
nten
ance
th
erap
y
IND
UC
TIO
NSu
lfasa
lazin
e or a
min
osal
icyl
ate o
ral
with
or w
ithou
t top
ical
ther
apy
If re
fract
ory t
o or
al +
topi
cal
amin
osal
icyl
ates
or s
ever
e sym
ptom
s ar
e pre
sent
: ora
l cor
ticos
tero
idIf
no re
spon
se to
ora
l cor
ticos
tero
ids
and
IV th
erap
y not
indi
cate
d:
azat
hiop
rine o
r 6-m
erca
ptop
urin
eIf
no re
spon
se o
r int
oler
ant o
f ste
roid
plu
s aza
thio
prin
e or
6-m
erca
ptop
urin
e: in
flixi
mab
Dist
al
MAI
NT
ENAN
CE
Topi
cal m
esala
min
e:- P
roct
itis:
supp
osito
ries
- Left
-side
d di
stal d
iseas
e: en
emas
dai
ly, ta
per t
o lo
west
effec
tive d
ose
(eve
ry o
ther
day
, or e
very
third
nig
ht)
Sulfa
salaz
ine o
r am
inos
alicy
late o
ral
Topi
cal P
LUS
oral
amin
osali
cylat
es m
ore e
ffect
ive th
an ei
ther
alon
eRe
fract
ory t
o all
agen
ts: az
athi
oprin
e or 6
-mer
capt
opur
ine O
R in
flixim
ab
IND
UC
TIO
NAm
inos
alicy
lates
:To
pica
l mes
alam
ine:
supp
osito
ries (
proc
titis)
, ene
mas
(left
-side
d
dista
l dise
ase)
Ora
l sul
fasa
lazin
e or m
esala
min
eTo
pica
l ste
roid
s: su
ppos
itorie
s (pr
octit
is), e
nem
as (l
eft-si
ded
di
stal d
iseas
e)If
refra
ctor
y to
oral
amin
osali
cylat
es o
r top
ical c
ortic
oste
roid
s: to
pica
l am
inos
alicy
lates
may
still
be e
ffect
iveTo
pica
l PLU
S or
al am
inos
alicy
lates
mor
e effe
ctive
than
eith
er al
one
Refra
ctor
y to
all ag
ents
at m
axim
al do
ses O
R sy
stem
ically
ill:
oral
pr
edni
sone
OR
infli
xim
ab in
trave
nous
infu
sion
MAI
NT
ENAN
CE
Aza
thio
prin
e or 6
-mer
capt
opur
ine o
r infl
ixim
abO
ral s
ulfa
salaz
ine o
r am
inos
alic
ylat
eIf
initi
al re
spon
se se
en, c
hang
e to
oral
cy
clos
porin
e and
cont
inue
unt
il az
athi
oprin
e or
6-m
erca
ptop
urin
e effe
ct is
seen
IND
UC
TIO
NU
rgen
t hos
pita
lizat
ion
not i
ndic
ated
: infl
ixim
abSy
stem
ic to
xici
ty re
quiri
ng h
ospi
taliz
atio
n:
intra
veno
us co
rtic
oste
roid
(hyd
roco
rtiso
ne o
r m
ethy
lpre
dniso
lone
)N
o re
spon
se to
cort
icos
tero
id in
3–5
day
s: co
lect
omy O
R cy
clos
porin
e int
rave
nous
in
fusio
nC
ontin
ue o
ral a
min
osal
icyl
ate i
f pre
viou
sly
taki
ng an
d if
tole
ratin
g ora
l the
rapy
Seve
re
Mild
to m
oder
atePa
tient
with
ulce
rativ
e col
itis

PSAP-VII • Gastroenterology and Nutrition36Inflammatory Bowel Disease
UC whose disease has not responded to 3–5 days of intravenous corticosteroid therapy and as an alternative to colectomy. The suggested target cyclosporine whole blood concentrations are 150–250 ng/mL with a 2-mg/kg/day infusion, and 300–350 ng/mL with a 4-mg/kg/day infusion. Cyclosporine may be converted to oral therapy of 4–6 mg/kg/day and used with thiopurine immunomodulator bridge therapy to control symptoms until the full effect of thiopurine is noted. Cyclosporine is associated with nephrotoxicity, neurotoxicity, hyper-tension, and electrolyte disturbances. If cyclosporine is used with a corticosteroid and a thiopurine, prophylaxis against Pneumocystis jiroveci should be considered with trimethoprim/sulfamethoxazole or dapsone. Tacrolimus has shown promise as a treatment of the fistulas associated with CD, as well as for disease that has not responded to corticosteroids or infliximab, although data comparing tacrolimus with standard therapies are limited. Target trough tacrolimus blood concentrations of 5–15 ng/mL have been reported with initial dosages of 0.05 mg/kg twice daily. This has been associated with clinical response, but not remission, compared with pla-cebo. Tacrolimus has an adverse effect profile similar to cyclosporine. Methotrexate is useful for the induction and main-tenance of remission of CD and has a corticosteroid-sparing effect. It may be useful in patients who have ste-roid-dependent CD. The drug is not effective for UC. Methotrexate is associated with hepatic fibrosis and pneumonitis in addition to bone marrow suppression and should be avoided during pregnancy. A complete blood cell count and liver and kidney function tests should be completed when therapy is initiated and every 1–2 months during therapy. Chest radiography and pul-monary function tests should be checked at baseline and periodically during treatment. Liver biopsy may be considered before therapy initiation in patients with risk factors for liver dysfunction such as history of exces-sive alcohol use, history of abnormal liver function, or chronic hepatitis B or C.
Biologic Therapies Infliximab, adalimumab, and certolizumab target TNF-α and are useful for the treatment of patients with moderate to severe CD that is refractory to other thera-pies and for the treatment of fistulas caused by CD. Inf-liximab is also recommended for mild to moderate exten-sive UC refractory to other therapies or for severe UC without the need for immediate hospitalization. Inflix-imab is administered as a continuous 2-hour intravenous infusion, which may be given in an outpatient infusion center. Up to 30% of patients treated with infliximab do not respond to therapy; they are considered primary non-responders. Of those whose disease responds to treat-ment, 30% become intolerant of the drug and 40% expe-rience infliximab-resistant disease within the first year of
therapy; they are referred to as secondary nonresponders. In secondary nonresponders, if antibodies to infliximab are undetectable and low concentrations of infliximab are present, the dosage may be increased or the dosing inter-val decreased to regain response. Another TNF-α antago-nist such as adalimumab or certolizumab pegol may also be substituted for infliximab. Patients whose disease no longer responds to infliximab and who have detectable antibodies to the drug may respond well to adalimumab or certolizumab pegol, with an expected response rate of 8% to 15% lower than that of patients who are naive to biologic therapy. Infliximab-related infusion reactions can be pre-vented with acetaminophen, diphenhydramine, and possibly corticosteroids. Adalimumab and certoli-zumab, which are self-administered as subcutaneous injections, may result in injection site reactions. Serum sickness reactions may occur if infliximab infusions are separated by long periods rather than dosed on a sched-uled basis. Other adverse effects include lupus, hemo-lytic anemia, and a few cases of demyelinating syn-dromes (e.g., multiple sclerosis, optic neuritis, Guillain-Barré syndrome). Hepatosplenic T-cell lymphoma is a serious but rare adverse effect of infliximab; the majority of cases of hepatosplenic T-cell lymphoma were in young male patients, and all cases had received azathioprine or 6-mercaptopurine concurrently with infliximab. Inf-liximab can worsen heart failure, especially at higher doses; doses greater than 5 mg/kg are contraindicated in patients with New York Heart Association class III and IV heart failure. All the TNF-α antagonists may predispose patients to infections; therefore, patients with active infection should not receive a TNF-α antag-onist. Before initiating therapy with one of these agents, patients should be screened for tuberculosis and hepati-tis B and C. Infliximab has been studied in combination with aza-thioprine in CD and UC. In one study of patients with CD, infliximab combined with azathioprine resulted in more corticosteroid-free remission at 26 weeks than either therapy alone. Combination therapy also resulted in fewer infliximab antibodies than infliximab alone and a similar number of infections compared with either therapy alone. Natalizumab targets alpha 4 integrin and is reserved for patients with CD who do not respond to or tolerate other therapies, including patients who develop TNF-α antibodies. Natalizumab is contraindicated in combina-tion with other immunosuppressants and TNF-α antag-onists as well as in patients with underlying hepatic injury. Natalizumab is associated with adverse effects similar to those of the TNF-α antagonists. A poten-tially fatal progressive multifocal leukoencephalopathy has been associated with the use of this drug, including at least one case in a patient receiving natalizumab for CD. Because of this risk, natalizumab is only available

PSAP-VII • Gastroenterology and Nutrition 37 Inflammatory Bowel Disease
through the restricted-access TOUCH prescribing pro-gram, which requires prescribers, pharmacies, infusion centers, and patients to register with and meet all the conditions of the program.
Antibiotics Several antimicrobial drugs have been used treat IBD. Metronidazole is recommended for perianal CD and pouchitis, an inflammation of the pouch created after colectomy (e.g., the ileal pouch anal anastomosis) in UC. Peripheral neuropathy is a common adverse effect of chronic metronidazole therapy and has also been reported in patients receiving large doses acutely. Cip-rofloxacin can be used alone and in combination with metronidazole for perianal CD and pouchitis. Other anti-microbials including rifaximin, antimycobacterial agents, amoxicillin clavulanate, trimethoprim/sulfamethoxazole, and tetracycline have also been studied alone and in com-bination for both CD and UC with mixed results. Apart from metronidazole and ciprofloxacin, specific recom-mendations for the potential roles of antimicrobial thera-pies cannot be made at this time.
Adjunctive Therapy Polyunsaturated Fatty Acids Polyunsaturated fatty acids such as omega-3 fatty acids display anti-inflammatory effects through scav-enging of free radicals and inhibition of the metabolites of arachidonic acid. Omega-3 fatty acids have been stud-ied in IBD but have not been found to be effective.
Probiotics Animal models of IBD have identified reduced GI concentrations of bifidobacteria in CD and lactoba-cilli in UC. On the basis of these models, several stud-ies have shown efficacy of probiotic supplementation for induction and maintenance of remission of IBD. Limi-tations of these studies include small sample size, and varied study designs and outcome measures, as well as an array of strains, dosages, and durations of probiotics. A combination of lactobacilli, bifidobacteria, and Strep-tococcus salivarius (VSL#3) prevented an initial attack and relapse of pouchitis after the induction of remission with antibiotics. Further evidence supporting the use of probiotics in CD and UC is lacking. Probiotics appear to be safe in available studies. Patients receiving immuno-suppressive agents and probiotics have a theoretical ele-vated risk of infections; however, this has not been clini-cally reported. Because these agents are not regulated by the U.S. Food and Drug Administration (FDA), con-cern exists about the consistency of the products. If a patient is interested in probiotic supplementation, prod-ucts shown to be effective in trials should be obtained if possible. The long-term safety and efficacy of probiotics, as well as the potential economic impact of these agents, need to be evaluated.
Nicotine Tobacco use influences the progression of IBD. Nic-otine therapy has been evaluated for treatment of UC, although the evidence is conflicting. Most studies used a nicotine transdermal patch with dosages ranging from 15 mg/day to 25 mg/day. Tolerability of nicotine ther-apy is an issue, with many patients experiencing adverse effects such as nausea, light-headedness, and itching, which leads to discontinuation. Nicotine has limited use in UC, and no specific treatment recommendations are available. Nicotine replacement therapy may be a reasonable approach for patients with UC who intend to stop smoking, and providing nicotine to these patients may attenuate the risk of disease exacerbation upon smoking cessation.
Top-down vs. Step-up Treatment Approaches Current practice includes an escalating, step-up approach to the treatment of UC or CD. Therapy is ini-tiated with agents such as mesalamine, antimicrobials, topical corticosteroids—and systemic corticosteroids in more severe disease. Immunosuppressive therapy is reserved for maintenance therapy for those who have experienced a relapse of their disease or whose disease has not responded to corticosteroid therapy. Biologic agents have generally been recommended after the fail-ure or intolerance of immunosuppressive therapy. Ini-tial therapy with mesalamine is more effective for the induction and maintenance of remission in UC than in CD. Systemic corticosteroids are effective for induction of remission in both UC and CD. The top-down approach involves early therapy with immunomodulator or biologic agents versus conven-tional induction therapy. In CD, early aggressive inter-ventions may result in early mucosal healing and altered disease progression, potentially reducing long-term structural damage. Theoretically, this may reduce the risk of developing strictures, intestinal obstruction, and fistulas. These effects may be evident particularly in patients with more aggressive disease that requires even-tual surgical intervention. Crohn disease progresses in a stepwise fashion, beginning with inflammatory lesions that are most likely to respond to therapy and continu-ing to potentially irreversible structural damage such as strictures, obstructions, and fistulas. Biologic agents may be more successful in patients with disease that is of a shorter duration, possibly because of the lower likeli-hood of the presence of structural damage. In contrast, long-term UC is not associated with the same irrevers-ible structural damage of CD. In UC, disease of longer duration is associated with dysplasia and an increased risk of CRC. The risk of CRC in patients with UC is 2% after 10 years, 8% after 20 years, and 18% after 30 years of disease compared with a 0.5% incidence in patients without UC. Early mucosal healing may result in a long-term reduction in the risk of CRC. The best evidence for

PSAP-VII • Gastroenterology and Nutrition38Inflammatory Bowel Disease
reduction in long-term CRC risk is with 5-aminosalic-ylates, which reduce risk by as much as 53% to 75% in some studies. At this time, evidence does not support infliximab use in patients who have had UC for a short duration (i.e., less than 3 years) versus a longer dura-tion. Currently, a rationale for top-down therapy does not exist in UC. Many questions remain regarding applying a top-down approach. Whether mucosal healing requires ongoing maintenance with a biologic agent is unclear. Moreover, although the natural history of CD may be altered with this approach, complications including structural damage and subsequent surgery may sim-ply be delayed versus being actually prevented given the data available. This approach requires further study because the biologic and immunomodulator agents have safety and tolerability considerations different from the initial therapies used in the step-up approach. In addi-tion, an evaluation of the economic impact of applying these agents early in the course of disease is needed.
Surgery Patients with IBD often require surgical intervention to control symptoms of the disease. Up to one-third of patients with CD will require major abdominal surgery within 5 years of diagnosis because of intractable hem-orrhage, perforation, obstruction, abscess, GI cancer, or disease refractory to medical therapy. Application of a top-down approach to therapy and early initiation of immunomodulator or TNF-α antagonists may mod-ify the disease course and the need for surgery; surgery rates are inversely proportional to the use of immuno-modulators and TNF-α antagonists within 5 years of diagnosis of CD. In CD, surgical resection is most often performed for refractory disease. Surgery is not curative for CD and, because it is used to treat active disease, is associated with high recurrence of symptoms. In contrast, colectomy in UC is a curative procedure. Similar to CD, indications for surgery in UC include excessive hemorrhage, perforation, cancer, severe coli-tis, toxic megacolon, or disease that is unresponsive to conventional medical therapy. Several options exist for restorative procedures in patients undergoing col-ectomy. These include a conventional ileostomy; the formation of an internal Koch pouch from the termi-nal ileum combined with a continent ileostomy, which eliminates the need for an external pouch to be worn by the patient; or the formation of a J-pouch or ileoanal pouch that functions as a new rectum.
Health Maintenance Cancer Surveillance and Prevention Patients with IBD are at an increased risk of CRC compared with the general population. In the past, the risk of CRC with CD was not considered significantly
increased; however, newer data suggest the risk is increased to a degree similar to UC, with a lifetime cumulative CRC risk of 7% in CD and 8% in UC. Unlike CD, patients with UC have long been recognized to be at an increased risk of developing CRC. The risk factors for CRC include positive family history of this cancer, extensive colitis, long disease duration (10 years or lon-ger), and presence of PSC. Patients who have had UC for 8–10 years should undergo an annual or biannual surveillance colonoscopy with several biopsies. Patients with UC complicated by PSC have almost 5 times the risk of developing CRC than do patients with UC alone. Surveillance colonoscopy should be initiated as soon as the diagnosis of PSC is made, regardless of the dura-tion of UC. Colectomy may be a preventive strategy for patients with UC for longer than 10 years or for those with premalignant changes/severe dysplasia on sur-veillance mucosal biopsies. Aminosalicylates may con-fer a chemoprotective effect against CRC, although the optimal dosage, duration, and time of initiation for this potential benefit are unknown. Patients with UC receiv-ing dosages of at least 1.2 g of mesalamine per day have a 77% lower risk of developing CRC compared with indi-viduals receiving lower dosages. In addition to CRC, the risk of cervical dysplasia on Pap smear may be higher in women with UC than in the general population. Some studies have reported this finding only in patients with UC receiving immu-nosuppressive therapy, whereas other studies have not found this increase in dysplasia among women with IBD. Unfortunately, only 70% of women with IBD undergo recommended screening for cervical dysplasia. Women with IBD should be screened regularly for cer-vical dysplasia.
Osteoporosis Screening and Prevention A reduction in bone mineral density may be pres-ent in patients with IBD. The etiology may be the direct inflammatory effects of the disease on bone, malab-sorption of vitamin D, or corticosteroid use. The overall prevalence is estimated to be 10% to 14%, and patients with CD and UC have comparable risks of low bone mineral density. Men and women are equally affected. All patients with IBD should be educated regarding ways to prevent low bone mineral density such as reg-ular weight-bearing exercise, smoking cessation, and avoidance of excessive alcohol use. Calcium 1200 mg and vitamin D 800–1000 units/day are recommended. Dual-energy x-ray absorptiometry is recommended for patients with IBD, especially if they are receiving corticosteroids or have other risk factors for low bone mineral density. Patients with confirmed osteoporo-sis should receive therapy with calcium and vitamin D, together with a bisphosphonate, denosumab, calci-tonin, selective estrogen receptor modulator, estrogen, teriparatide, or testosterone.

PSAP-VII • Gastroenterology and Nutrition 39 Inflammatory Bowel Disease
Vaccinations Patients with IBD who are prescribed immunosup-pressive or biologic therapies are at increased risk of developing infections. Many of these infections can be prevented by the use of vaccinations. Most of these patients are not optimally vaccinated, with only 28% receiving the yearly influenza vaccine and 9% receiv-ing the pneumococcal vaccine. Although immunosup-pression may attenuate the vaccine response, vaccina-tion does not worsen the course of IBD in patients. The Advisory Committee on Immunization Practices rec-ommends pneumococcal, influenza, meningococcal, Haemophilus influenza B, tetanus, diphtheria, pertussis, and human papillomavirus vaccines as appropriate for the patient’s age. Hepatitis A and B vaccines are recom-mended for patients receiving immunosuppressive ther-apy if additional risk factors are present (e.g., occupa-tional exposure, high-risk sexual behavior, other chronic disease such as end-stage liver or kidney disease). Live virus vaccines such as varicella are contraindicated in these patients.
Venous Thromboembolism Prophylaxis Inflammatory bowel disease increases the risk of deep venous thrombosis and pulmonary embolism among acutely ill patients admitted to the hospital. In addition, large case-control cohort studies have indicated that active IBD requiring the recent use of corticosteroids or hospitalization significantly increases venous throm-boembolism risk. The risk may be 2–3 times that of the general population. Patients with IBD who are admit-ted to the hospital with congestive heart failure or respi-ratory disease or those who are confined to bed should receive prophylaxis with a low-molecular-weight hepa-rin, low-dose unfractionated heparin, or fondaparinux. Patients who have contraindications to these agents should be provided with mechanical thromboprophy-laxis such as graduated compression stockings or inter-mittent pneumatic compression.
Role of the Pharmacist Adherence Adherence to drug therapy is a major issue in man-aging patients with IBD. Many factors associated with treatment, disease, and the individual patient influence adherence. These factors may differ with time as treat-ments change, disease symptoms relapse and remit, and patient factors vary. Suboptimal adherence to drug therapy results in higher relapse rates, which reduce the quality of life of these patients. Adherence to mesala-mine in one study increased when adherence was dis-cussed and monitored. Consistent interaction with the pharmacist over time allows the identification and res-olution of adherence issues and can improve patient outcomes.
Adherence is of concern with patient-administered therapy. However, this is also an issue with intrave-nous infusion therapy; in one study, the nonadherence rate with infliximab was 34.3% during the first year of therapy. This resulted in significantly increased medical costs and a higher hospitalization rate for these patients compared with patients who adhered to therapy.
Patient Education A pharmacist can play a vital role in the manage-ment and education of a patient with IBD. Because this is a chronic illness requiring ongoing therapy, continu-ing opportunities are provided to discuss the patient’s drug therapy, evaluate potential drug-related prob-lems including adverse effects or drug interactions, and resolve any issues. The pharmacist may also educate the patient regarding health issues such as the need for vac-cinations and adequate calcium and vitamin D intake. The pharmacist is in a position to ensure that patients are able to receive needed therapy, especially some of the more expensive biologic agents, by navigating insur-ance issues or patient assistance programs. In the inpa-tient setting, pharmacists are instrumental in ensuring that appropriate prophylaxis for venous thromboembo-lism is used.
Conclusion Inflammatory bowel disease is a complex, chronic, relapsing and remitting disease. Although similari-ties exist between CD and UC, the approaches to drug therapy differ. Current therapy is aimed at inducing and maintaining clinical remission and possibly muco-sal healing and improving health-related quality of life. Adherence to drug therapy remains a major concern, offering the pharmacist an excellent opportunity to improve patient outcomes.
Annotated Bibliography 1. Kornbluth A, Sacher DB; Practice Parameters Com-
mittee of the American College of Gastroenterology. Ulcerative colitis practice guidelines in adults: Ameri-can College of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol 2010;105:501–23.
This is the newest set of guidelines from the Amer-ican College of Gastroenterology and the Practice Parameters Committee. The approach to treatment (induction and maintenance) on the basis of location (distal vs. extending proximal to ascending colon) and severity is discussed. Since the publication of the previ-ous guidelines in 2004, infliximab has been approved for use in UC. The newer guidelines discuss the role of infliximab in UC, as well as the once-daily dosing of mesalamine with the Multi Matrix formulation. Health maintenance issues such as CRC screening and vacci-nations are also discussed. Specific drugs are discussed

PSAP-VII • Gastroenterology and Nutrition40Inflammatory Bowel Disease
in detail, together with their adverse effects and spe-cial considerations. The potential of mesalamine as a chemopreventive agent when used for the long-term maintenance of remission is discussed. The use of urso-deoxycholic acid in patients with UC and PSC for the prevention of CRC is controversial; these guidelines suggest using a 13-mg/kg/day to 15-mg/kg/day dose, whereas the PSC guidelines do not recommend the use of ursodeoxycholic acid for this application. Patients with severe colitis may be experiencing superimposed infection with enteric pathogens, Clostridium difficile, or cytomegalovirus, of which the clinician should be aware and make sure to screen patients appropriately. Overall, these guidelines are helpful in directing therapies and assisting clinicians with the best course of action.
2. Lichtenstein GR, Hanauer SB, Sandborn WJ; Practice Parameters Committee of American College of Gastro-enterology. Management of Crohn’s disease in adults. Am J Gastroenterol 2009;104:465–83.
This is the newest set of guidelines from the Ameri-can College of Gastroenterology and the Practice Param-eters Committee. The approach to induction and main-tenance treatment of CD on the basis of location and severity is discussed. The new guidelines discuss the role of oral budesonide therapy for ileocolonic mild to mod-erate disease. New in these guidelines, infliximab, adali-mumab, and certolizumab pegol are all recommended in the treatment of moderate to severe CD or fistuliz-ing disease as well as the maintenance of remission. The enhanced efficacy of infliximab alone or in combination with azathioprine versus azathioprine alone in moder-ate to severe disease is discussed. These guidelines also include more specific recommendations for determining TPMT status before initiating azathioprine and 6-mer-captopurine. Controversy still exists regarding whether a top-down versus step-up approach to therapy is best, as well as the optimal dosage and route of mesalamine and its potential benefit in CD. The long-term safety and effi-cacy of budesonide in maintaining remission with doses greater than 6 mg remains to be established. Moreover, a determination of the optimal dosing of thiopurine anti-metabolites (especially in patients with varied TPMT polymorphisms) and methotrexate is needed. The safety concerns with natalizumab should also be studied. More-over, the role of probiotics and alternative therapies should be determined. Finally, the success of medical therapy as measured with novel end points, both clini-cal and endoscopic, as well as the determination of prog-nostic factors predicting the natural history of the dis-ease, should be evaluated. Overall, these guidelines aid in directing therapy and assisting clinicians with the best course of action.
3. Pineton de Chambrun G, Peyrin-Biroulet L, Lemann M, Colombel JF. Clinical implications of mucosal heal-ing for the management of IBD. Nat Rev Gastroenterol Hepatol 2010;7:15–29.
This article reviews the definitions and scoring sys-tems for mucosal healing and summarizes studies of drug therapy and their ability to achieve mucosal
healing. Clinical signs and symptoms have been used as traditional end points of therapy. However, recent evi-dence indicates that mucosal healing might be a better therapeutic end point because it is associated with alter-ation of the disease course through reductions in long-term structural damage that decrease hospitalizations and lifetime risk of surgery. Two validated endoscopic scoring systems are available for CD, the Crohn’s Disease Endoscopic Index of Severity and the Simple Endoscopic Score for Crohn’s Disease. Several endoscopic scoring systems are available for UC; however, none has been val-idated. Each of the UC instruments uses different endo-scopic variables, some of which include bleeding, pres-ence of ulcers and inflammation, overall appearance of mucosa, friability, erythema, granularity, and exudation. A formal definition of mucosal healing based on one or more of the available scoring systems has not been uni-versally accepted, and more clinical trials are required to develop standardized endoscopic scoring systems, espe-cially for UC. The authors propose an ideal definition of mucosal healing as complete endoscopic healing of CD or UC lesions. In clinical trials, efficacy is defined as changes in clinical disease activity scores, and if mucosal healing is included, it is as a secondary end point. Pharmacologic therapies are difficult to compare with respect to inducing mucosal healing because clinical trials use various endo-scopic scoring instruments, definitions of healing, and timing of endoscopic assessment. To apply mucosal heal-ing as a clinical end point, a universal definition needs to be developed and applied to clinical trials.
4. Chapman R, Fevery J, Kalloo A, Nagorney DM, Boberg KM, Schneider B, et al. American Association for the Study of Liver Diseases Diagnosis and manage-ment of primary sclerosing cholangitis. Hepatology 2010;51:660–78.
Primary sclerosing cholangitis and IBD often occur together; 60% to 80% of patients with PSC also have IBD, especially UC. These guidelines for the diagnosis and management of PSC include a discussion of the patient with both PSC and IBD. Primary sclerosing cholangitis increases the risk of CRC in patients with UC. Patients with UC alone should begin CRC surveillance with annual or biannual colonoscopies with biopsies begin-ning 8–10 years after UC diagnosis; in contrast, patients with UC and PSC should begin CRC surveillance at the time of diagnosis. Ursodeoxycholic acid may reduce CRC risk in patients with UC and PSC; however, most data are from retrospective trials. In addition, high-dose ursode-oxycholic acid (28–30 mg/kg/day) is associated with increases in the need for liver transplantation and in mor-tality. These PSC guidelines do not recommend ursode-oxycholic acid for the prevention of CRC. This is in con-trast to the UC guidelines, which recommend ursodeoxy-cholic acid for this use at the well-tolerated lower dosage of 13–15 mg/kg/day. Several other drugs have been stud-ied (e.g., colchicine, pentoxifylline, tacrolimus, cyclospo-rine, methotrexate, mycophenolate) and have shown no benefit in PSC. Hepatic osteodystrophy is a term used for the metabolic bone disorders associated with chronic liver diseases, including PSC. Bone density measurement
PSAP-VII • Gastroenterology and Nutrition 41 Inflammatory Bowel Disease
is recommended at the diagnosis of PSC and every 2–3 years thereafter. Calcium and vitamin D supplementa-tion should be recommended to patients with hepatic osteopenia, which is characterized by a T-score of 1–2.5 standard deviations below the density observed in young normal individuals, with the addition of bisphosphonate therapy for patients with hepatic osteoporosis (T-score below −2.5).
5. D’Haens G, Sandborn WJ, Feagan BG, Geboes K, Hanauer SB, Irvine EJ, et al. A review of activity indices and efficacy end points for clinical trials of medical ther-apy in adults with ulcerative colitis. Gastroenterology 2007;132:7663–86.
This review discusses instruments used for measuring disease activity in UC. The review includes the Truelove and Witts Severity Index, the St. Mark’s Index (Powell Tuck Index), the Clinical Activity Index (also known as the Rachmilewitz Index), the Activity Index (also known as the Seo Index), the physician global assessment, the Lichtiger Index (also known as the Modified Truelove and Witts Severity Index), the Investigators Global Eval-uation, the Simple Clinical Colitis Activity Index, the Improvement Based On Individual Symptom Scores, and the Ulcerative Colitis Clinical Score. Several instru-ments for measuring disease activity on the basis of endo-scopic findings are discussed, as are instruments for mea-suring disease activity on the basis of composite clinical and endoscopic disease such as the Sutherland Index and the Mayo Score. Scoring a patient’s disease severity using these instruments is discussed, as are the definitions of clinical improvement and remission, if they are defined for a given scale. The Inflammatory Bowel Disease Ques-tionnaire for measuring quality of life has been used in few trials of patients with UC, whereas it has been validated in CD. Use of these indices in clinical trials and practice is discussed, with extensive tables outlining the use of the various scoring systems in trials. Despite their widespread use, these indices do not take into account the patient’s abdominal pain, nocturnal bowel movements, urgency, or incontinence.
6. Sandborn WJ, Feagan BG, Hanauer SB, Lochs H, Lof-berg R, Modigliani R, et al. A review of activity indices and efficacy end points for clinical trials of medical ther-apy in adults with Crohn’s disease. Gastroenterology 2002;122:512–30.
This review describes instruments for measuring CD activity. The Crohn’s Disease Activity Index, a validated scoring system to assess the severity of CD, is reviewed in detail and involves several patient-reported and lab-oratory variables such as abdominal pain, number of stools per day, use of antidiarrheal drugs, general well-being, accompanying complications, presence of abdom-inal mass, and low hemoglobin or body weight. To accu-rately assess this score, the patient is required to main-tain a symptom diary for 7 days before assessment. The Inflammatory Bowel Disease Questionnaire, which mea-sures quality of life in CD, is discussed, as are endoscopic scoring systems (Crohn’s Disease Endoscopic Index of Severity and the Rutgeerts score). The authors contend
that trials reporting quality-of-life results based on the IBDQ often report the mean or median increase across the population rather than the proportion of patients who achieve a meaningful increase in scores (defined as a change of 16 points or an absolute score of 170). Two scoring systems for histologic disease activity are pre-sented; however, these correlate poorly with other assess-ments of disease activity, so their usefulness is unclear. Although these indices are commonly used in clinical tri-als to assess the efficacy of therapies, end points based on these measurements vary from study to study and are not standardized. Clinical trials applying definitions of endoscopic and histologic improvement are needed. The applicability to practice is unclear because some of the instruments are cumbersome to apply.
7. Al Hadithy AFY, de Boer NKH, Derijks LJJ, Escher JC, Mulder CJJ, Brouwers JRBJ. Thiopurines in inflamma-tory bowel diseases: pharmacogenetics, therapeutic drug monitoring and clinical recommendations. Dig Liver Dis 2005;37:282–97.
This review discusses the continued interest in the use of azathioprine and 6-mercaptopurine in the manage-ment of IBD and focuses on the TPMT enzyme involved in the metabolism of these agents. Diminished activ-ity of this enzyme decreases the methylation of thiopu-rines and results in higher rates of formation of 6-thiogua-nine metabolites, potentially resulting in myelosuppres-sion, whereas high TPMT activity leads to overproduc-tion of the toxic metabolite 6-methylmercaptopurine and an elevated risk of hepatotoxicity. Another enzyme sys-tem involved in thiopurine metabolism is inosine triphos-phate pyrophosphatase. Deficiency of this enzyme yields elevated concentrations of the metabolite 6-thioinosine triphosphate and a higher risk of pancreatitis. A complete graphic depiction of the thiopurine metabolic pathway is included, which helps the clinician determine whether the patient is at higher risk of experiencing bone marrow suppression or hepatotoxicity, or if the patient is at risk of developing pancreatitis. Among white patients, three variant alleles (TPMT*2, *3A, and *3C) are most often associated (more than 80% of the time) with a defective phenotype. Of these three alleles, the third, TPMT*3A, results in the largest reduction in enzyme activity. Knowl-edge of a patient’s genotype or phenotype of the TPMT enzyme may help direct the choice of therapy as well as FDA-recommended dosing and evaluation before initiat-ing therapy. However, the authors caution that myelosup-pression caused by thiopurines is multifactorial and may still occur even if a patient’s TPMT status does not indi-cate that he or she is at higher risk of this effect.
8. Ha C, Dassopoulos T. Thiopurine therapy in inflamma-tory bowel disease. Expert Rev Gastroenterol Hepatol 2010;4:575–88.
This article builds on the Al Hadithy et al 2005 article. A more detailed discussion is presented on the clinical management of patients with genetic polymorphisms of the TPMT enzyme and the implications of high and low TPMT activity levels. In addition to the avoidance of azathioprine in patients with low-to-absent TPMT

PSAP-VII • Gastroenterology and Nutrition42Inflammatory Bowel Disease
metabolism, initial dosing recommendations of 1 mg/kg/day for intermediate TPMT metabolizers and 3 mg/kg/day for normal metabolizers are suggested. The article also reviews the value of measuring metabolite concentrations such as 6-thioguanine, especially in patients whose disease has not adequately responded to thiopurine therapy. In addition, the authors suggest an approach to measuring 6-thioguanine metabolites and using this information to characterize patients who do not respond to thiopurine. These patients can be classi-fied into three groups: those who do not adhere to ther-apy, those with therapeutic 6-thioguanine concentra-tions who still experience disease symptoms and require alternative therapies, and those with 6-methyl-mercap-topurine ribonucleotide dominant metabolism who will likely not respond to thiopurine dose escalation and may benefit from the addition of allopurinol, which would shift metabolism to 6-thioguanine and increase the effectiveness of the thiopurine. The concentration of the metabolite, 6-methyl-mercaptopurine, in con-junction with 6-thioguanine measurement, would con-firm the need for allopurinol cotherapy. Although thio-purines are in FDA pregnancy category D, they appear to have minimal risks to the fetus from the limited data available. The authors suggest that these risks are out-weighed by their benefits. The evolving place in therapy of the thiopurines is reviewed as well, especially the use of azathioprine in conjunction with TNF-α antagonists.
9. Gan SI, Beck PL. A new look at toxic megacolon: an update and review of incidence, etiology, pathogen-esis, and management. Am J Gastroenterol 2003;98: 2363–71.
This review discusses the pathogenesis, diagnosis, and management of toxic megacolon. Diagnostic cri-teria are discussed including the Jalan criteria, which are based on the patient’s presenting with three of the following: fever greater than 101.5°F, heart rate greater than 120 beats/minute, white blood cell count greater than 10.5 × 10/mm3, or anemia; plus, the patient should present with at least one of the following: dehydra-tion, mental status changes, electrolyte disturbances, or hypotension. Additional diagnostic criteria include radiographic evidence of dilation of the transverse or ascending colon to greater than 6 cm. Management of toxic megacolon includes intravenous fluids, intrave-nous corticosteroids, broad-spectrum antibiotics, and discontinuation of narcotic or anticholinergic agents. On the basis of current evidence, immunosuppressive therapy, oral corticosteroids, and aminosalicylates do not play a role in the management of the disease. Use of intravenous corticosteroids is an area of some contro-versy; patients may develop toxic megacolon after intra-venous corticosteroid therapy is initiated for a severe or fulminant flare of IBD; however, corticosteroids do not actually precipitate toxic megacolon. Use of corticosteroids may mask physical signs of colonic per-foration; therefore, it is necessary to continue to mon-itor for this complication to avoid delaying necessary surgical intervention. Surgical management is indicated for patients with perforation, uncontrollable bleeding,
or progressive dilation. Preoperative parenteral nutri-tion as an adjunctive therapy may be beneficial; how-ever, the use of parenteral nutrition as a primary therapy for toxic megacolon does not alter the surgical interven-tion or mortality rate.
10. Rutgeerts P, Sandborn WJ, Feagan BG, Reinisch W, Olson A, Johanns J, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med 2005;353:2462–76.
This publication reports the results of two landmark randomized, double-blind, placebo-controlled stud-ies, the Active Ulcerative Colitis Trials 1 and 2 (ACT 1 and 2). In these trials, 364 patients with active-mod-erate to severe UC, despite receiving treatment with an aminosalicylate, corticosteroid, thiopurine, or a com-bination, were randomized to receive intravenous inf-liximab 5 mg/kg, infliximab 10 mg/kg, or placebo at weeks 0, 2, and 6 and every 8 weeks thereafter through week 46 (ACT 1) or 22 (ACT 2). Clinical response, clinical remission, and mucosal healing were the main end points in the studies. In ACT 1, clinical response was reported as 69%, 52%, and 45% with infliximab 5 mg compared with 37%, 30% and 20% with placebo at weeks 8, 30, and 54, respectively (p<0.002). In ACT 2, clinical response was reported as 64% and 47% with infliximab 5 mg compared with 29% and 26% with pla-cebo at weeks 8 and 30, respectively (p<0.002). The response was similar with infliximab 10 mg in both tri-als (p<0.002 for all comparisons). Infusion reactions were more common in patients who tested positive for antibodies against infliximab. At week 54 in ACT 1, 35.7% of patients with positive tests for antibodies experienced infusion reactions compared with 9.8% of patients with negative or inconclusive tests. At week 30 in ACT 2, 50% of patients with positive tests for anti-bodies experienced infusion reactions compared with 9.7% of patients with negative or inconclusive tests (sta-tistics not reported). This study is the landmark trial that was instrumental in obtaining FDA approval for infliximab use in UC.
11. Sokol H, Seksik P, Carrat F, Nion-Larmurier I, Vienne A, Beaugerie L, et al. Usefulness of co-treatment with immunomodulators in patients with inflammatory bowel disease treated with scheduled infliximab main-tenance therapy. Gut 2010;59:1363–8.
This retrospective database study assessed 121 patients with IBD, 98 with CD, and 23 with UC who received infliximab plus at least 6 months of concurrent immu-nomodulator maintenance therapy with azathioprine or methotrexate. Disease activity for patients receiving inf-liximab with immunosuppressive cotherapy was com-pared with that for patients receiving infliximab alone. Flares of IBD (19.3% vs. 32.0%; p=0.003), perianal com-plications (4.1% vs. 11.8%; p=0.03), and switch to adali-mumab because of drug-induced lupus, loss of efficacy, serum sickness, or serious infusion reaction (1.1% vs. 5.3%; p=0.006) were less common with azathioprine or methotrexate cotherapy than without. In addition, the maximal infliximab dose per kilogram was lower when

PSAP-VII • Gastroenterology and Nutrition 43 Inflammatory Bowel Disease
immunosuppressive cotherapy was used (p<0.001), implying that dose titration was required less often during cotherapy. Abdominal surgery was rare in this study, with no patients on cotherapy and two patients on infliximab alone requiring surgery (p=0.29). The benefit of cotreat-ment with azathioprine or methotrexate in patients undergoing treatment with infliximab should be bal-anced with the potential adverse effects such as infections or malignancies. This study was underpowered to assess the impact of combination therapy on the development of these adverse effects. In this retrospective study, the investigators were unable to control for discontinuation of immunosuppressant cotherapy, which may have influ-enced the results.
12. D’Inca R, Bertomoro P, Mazzocco K, Vettorato MG, Rumiati R, Sturniolo GC. Risk factors for non-adher-ence to medication in inflammatory bowel disease patients. Aliment Pharmacol Ther 2008;27:166–72.
Inflammatory bowel disease requires maintenance drug therapy throughout life to control the disease and maintain remission; therefore, adherence to pre-scribed drugs is essential. This study identified poten-tial risk factors of nonadherence in patients with IBD by administering an anonymous 24-item questionnaire to 485 outpatients with IBD (45% CD, 55% UC) at a ter-tiary care center. Of the 485 patients, 61% adhered to their treatment; this was similar between patients with CD and UC (60% and 63%, respectively). Patient age influenced adherence, with patients younger than 40 years having lower adherence rates (43% vs. 34% for > 40 years; odds ratio [OR] = 1.5; 95% confidence inter-val [CI], 1.01–2.13). Disease duration less than 5 years was also associated with nonadherence (24% vs. 15%; OR = 2.1; 95% CI, 1.30–3.39), and patients who were younger than 40 years with a disease duration of less than 5 years had nonadherence levels of 75% (OR = 4.1; 95% CI, 2.13–7.96). Other factors associated with non-adherence were forgetfulness (61% vs. 44%; OR = 2.0; 95% CI, 1.39–2.93), disease remission (25% vs. 10%; OR = 2.9; 95% CI, 1.82–4.95), and full-time employ-ment (55% vs. 26%; OR = 3.5; 95% CI, 2.27–5.26). Patients receiving oral therapy reported better adher-ence than those receiving rectal therapy (60% vs. 32%; OR = 0.25; 95% CI, 0.11–0.60). Patients younger than 40 years who were more willing to discuss their disease with their physician had a better adherence rate (47% vs. 36%; OR = 1.5; 95% CI, 1.03–2.23); this effect did not hold true for patients older than 40 years. Patient sex, marital status, type of education, and type of dis-ease (CD or UC) did not correlate with adherence. In addition, the type and number of drugs prescribed were not associated with adherence in this study.
13. Bermejo F, López-San Román A, Algaba A, Guerra I, Valer P, García-Garzón S, et al. Factors that modify therapy adherence in patients with inflammatory bowel disease. J Crohns Colitis 2010;4:422–6.
This study used a survey to assess adherence to IBD therapy in 107 patients with IBD (64% CD, 36% UC). An estimated 70% of patients had disease in remission.
Sixty-nine percent (95% CI, 60% to 77%) of the patients showed some type of nonadherence, either involuntary (carelessness or forgetfulness) or voluntary (interrupt-ing therapy when feeling better or worse). Reasons for nonadherence were mostly self-reported forgetfulness or “careless[ness] about having taken it” on a standard-ized four-item true-or-false survey. Only 16% (95% CI, 9% to 22%) reported interrupting therapy because of symptoms. Patient factors associated with lower adher-ence included having to take three or more doses per day (OR = 3; 95% CI, 1.1–8.4; p=0.03) and reporting feeling insufficiently informed about their disease (OR = 4.9; 95% CI, 1.1–23.8; p=0.04). Therapy with azathio-prine was associated with better adherence (OR = 0.29; 95% CI, 0.11–0.74; p=0.01), both voluntary and invol-untary. Factors that did not correlate with adherence in this study were patient sex, whether a patient had CD or UC, the disease duration, and the clinical activity of the disease. In clinical trials, adherence to therapy ranges from 70% to 95%, which is much higher than in clini-cal practice. Before labeling a patient as having a disease that does not respond and adjusting therapy, therapy adherence should be assessed.
14. Grijalva CG, Chen L, Delzell E, Baddley JW, Beukel-man T, Winthrop KL. Initiation of tumor necrosis fac-tor-antagonists and the risk of hospitalization for infec-tion in patients with autoimmune diseases. JAMA 2011;306:2331–9.
This retrospective cohort study of more than 15,000 patients compared the use of TNF-α antagonists for rheumatoid arthritis, IBD, or psoriasis and spondy-loarthropathies with the use of nonbiologic agents in matched control patients. The primary outcome was the risk of serious infections requiring hospitalization in the first 12 months after therapy initiation. Overall, 1172 serious infections were identified, most (53%) of which were pneumonia and skin and soft tissue infections. Among the 2323 patients with IBD, hospitalization rates because of infection were 10.91 per 100 person-years in the TNF-α antagonist group and 9.60 per 100 person-years in the comparator group (adjusted hazard ratio = 1.10; 95% CI, 0.83–1.46). Hazard ratios were adjusted for baseline corticosteroid use in each group on the basis of prednisone-dosing equivalents. Base-line use of corticosteroids was associated with a dose-related increase in serious infections, but this did not reach statistical significance. The study assessed only serious infections resulting in hospitalization rather than all infections. Moreover, this retrospective study used Medicaid and Medicare databases to extract data, which may have resulted in misclassified or incomplete data. Because the data were retrieved from large aggre-gate databases, the results could not be categorized on the basis of the specific TNF-α antagonists used. The comparator group of patients with IBD received aza-thioprine or 6-mercaptopurine, which allowed a com-parison of immunosuppressive agents with the TNF-α antagonists. Although TNF-α antagonists are associ-ated with infections, in this study, the risk of infections

PSAP-VII • Gastroenterology and Nutrition44Inflammatory Bowel Disease
in the IBD population was not significant and therefore should not preclude their use.
15. Colombel JF, Sandborn WJ, Reinisch W, Manzaris GJ, Kornbluth A, Rachmilewitz D. Infliximab, azathi-oprine, or combination therapy for Crohn’s disease. N Engl J Med 2010;362:1383–95.
The 26-week-long Study of Biologic and Immu-nomodulator-Naive Patients with Crohn’s Disease (SONIC) compared combination azathioprine and inf-liximab maintenance therapy with either agent alone in 508 patients with active CD who had not received these therapies. Of these patients, 40% were receiving systemic corticosteroids or budesonide. The primary end point of remission at week 26 was achieved in 30%, 44.4%, and 56.8% in the azathioprine, infliximab, and combination groups, respectively (azathioprine vs. inf-liximab, p=0.006; infliximab vs. combination, p=0.02; azathioprine vs. combination, p<0.001). Mucosal heal-ing at 26 weeks was achieved in 16.5%, 30.1%, and 43.9% of patients in the azathioprine, infliximab, and combination groups, respectively (azathioprine vs. inf-liximab, p=0.02; infliximab vs. combination, p=0.06; azathioprine vs. combination, p<0.001). Of the study population 208 patients opted to continue to week 50; those who did not were considered treatment fail-ures at week 50. When all 508 patients were analyzed at week 50, corticosteroid-free remission was achieved in 24.1%, 34.9%, and 46.2% of the azathioprine, inflix-imab, and combination groups, respectively, which was statistically significant for all comparisons (p=0.03 for infliximab vs. azathioprine; p=0.04 for combination vs. infliximab and p<0.001 for combination vs. azathio-prine). However, among the 280 patients in the exten-sion phase, 54.7%, 60.8%, and 72.2% were in cortico-steroid-free remission at 50 weeks, which was signifi-cant for azathioprine versus combination therapy only (p=0.01). Significantly fewer patients receiving com-bination therapy developed infusion reactions (5% vs. 16.6%; p<0.001) or antibodies to infliximab (0.9% vs. 14.6%; p value not reported) compared with those receiving infliximab alone. Rates of serious infection were not significantly different among the groups (5.6% azathioprine, 4.9% infliximab, and 3.9% combination therapy). This trial shows the superiority and relative safety of combination therapy compared with azathio-prine or infliximab alone, as well as the superiority of infliximab compared with azathioprine. Although the combination therapy appears safe, practitioners must consider the risks of the rare adverse effect hepato-splenic T-cell lymphoma, which has only been reported in patients on combination therapy.

PSAP-VII • Gastroenterology and Nutrition 45 Inflammatory Bowel Disease
21. A 26-year-old man has a history of bipolar disor-der and a seizure disorder for which he takes lith-ium and phenytoin. His social history includes smoking 1 pack/day and having a glass of wine with dinner each day. His current concern is more than four bloody loose stools per day for the last 3 days. His temperature is 98.6°F; laboratory data include white blood cell (count) (WBC) 8 × 103 cells/mm3, hemoglobin 14 g/dL, and erythrocyte sedimenta-tion rate 11 mm/hour (normal, < 15 mm/hour). Stool specimen ruled out any infectious causes. Sigmoidoscopy shows continuous inflammatory changes confined to the rectum and sigmoid colon without signs of cobblestone appearance. Crypt abscesses were present. Biopsy results indicate the involvement of mucosa and submucosa. Which one of the following would be the best classifica-tion of this patient’s inflammatory bowel disease (IBD)?A. Mild Crohn disease (CD).B. Moderate CD.C. Mild ulcerative colitis (UC).D. Moderate UC.
22. A 47-year-old man is consistently late in refilling his mesalamine prescription. He was given a diagno-sis of UC about 23 years ago. He is currently pre-scribed mesalamine 400 mg orally twice daily to maintain his remission. His most recent UC flare occurred 2 years ago, and he has been asymptom-atic since then. Which one of the following is the best approach to counseling this patient regard-ing his nonadherence to therapy?A. Maintenance therapy for UC is not necessary,
and continuing therapy will not affect your long-term colorectal cancer (CRC) risk.
B. Continuing mesalamine for maintenance of remission reduces your risk of CRC, but you need at least 1.2 g/day to achieve this benefit.
C. Maintenance therapy for UC is recommended, but it will not affect your long-term CRC risk.
D. Continuing mesalamine for maintenance of remission is recommended, and it will reduce your risk of CRC without respect to dosage.
Questions 23-26 pertain to the following case.F.W. is a 70-year-old man (weight 48 kg, height 65″) admitted to the internal medicine service with the chief concerns of dyspnea on exertion that makes it difficult for him to ambulate, 2+ pitting pedal edema, and epi-gastric pain. His medical history is significant for CD
for 32 years and heart failure for 3 years with an ejec-tion fraction of 32% measured during the past month. F.W. states that he has an allergy to sulfa drugs. His home oral drugs include aspirin 325 mg/day, furose-mide 20 mg/day, lisinopril 10 mg/day, metoprolol succi-nate 50 mg/day, and mesalamine (Pentasa) 500 mg four times/day. F.W. states that he ran out of his drugs about 10 days ago. He has been taking oral ibuprofen 600 mg four times/day for the past 7 days for a sprained ankle. His laboratory findings are significant for hemoglobin 8 g/dL (baseline hemoglobin 12 g/dL), hematocrit 23%, platelet count 70,000/mm3, serum creatinine 2.4 mg/dL, and blood urea nitrogen 30 mg/dL.
23. Which one of the following is the best recommen-dation for F.W.?A. Enoxaparin subcutaneously 40 mg/day.B. Fondaparinux subcutaneously 2.5 mg/day.C. Unfractionated heparin subcutaneously 5000
units every 8 hours.D. Use of an intermittent pneumatic compression
device.
24. F.W. responds to furosemide diuresis, and he is reinitiated on his maintenance drugs, including lisinopril and metoprolol. He no longer requires ibuprofen, and his aspirin dosage is adjusted to 81 mg/day. His endoscopy shows no evidence of upper gastrointestinal (GI) tract bleeding. On day 3 of his hospitalization, F.W. has moderate abdominal pain and four loose stools within 24 hours. Clostridium difficile toxin is negative. Colonoscopy reveals active CD lesions extending from the ileum to the begin-ning of the transverse colon. Which one of the fol-lowing is the best change to F.W.’s drug regimen at this time?A. Sulfasalazine 1 g four times/day.B. Mesalamine enema 4 g daily at bedtime.C. Mesalamine 800 mg four times/day plus
budesonide 9 mg once daily.D. Mesalamine 800 mg four times/day plus
hydrocortisone 100-mg enema twice daily.
25. Several months later, F.W. presents with moderate to severe CD and receives induction therapy with oral prednisone 60 mg/day. He is tested and found to have low-to-absent thiopurine S-methyltransfer-ase (TPMT) activity. Which one of the following would be best for F.W. at this time?A. Avoid using azathioprine.B. Initiate azathioprine 50 mg day.
Self-Assessment Questions

PSAP-VII • Gastroenterology and Nutrition46Inflammatory Bowel Disease
C. Initiate azathioprine 150 mg/day and cyclosporine 100 mg twice daily.
D. Initiate azathioprine 150 mg/day.
26. F.W.’s heart failure is well controlled, but now, he has developed a draining enterocutaneous fistula. He has been maintained for the past 2 years on mesala-mine 1.2 g/day, and he receives an intravenous inf-liximab infusion of 250 mg every 8 weeks. During the past three cycles of infliximab, the effects have lasted only 4–6 weeks. F.W. has developed antibod-ies to infliximab. Which one of the following is the best recommendation for changing F.W.’s drug therapy?A. Administer the infusion of infliximab 250 mg
every 4 weeks.B. Increase the infusion of infliximab to 500 mg
every 8 weeks.C. Use adalimumab 160 mg day 1, 80 mg day 15,
and then 40 mg subcutaneously every other week.
D. Replace infliximab with intravenous natalizumab 300 mg every 4 weeks.
Questions 27–29 pertain to the following case.A.L. is a 24-year-old woman with a 5-year history of UC. She presents to the emergency department with severe abdominal pain and 5 days of bloody diarrhea consisting of eight stools per day. Her medical history is significant for bipolar disorder. Her social history is sig-nificant for tobacco, 1 pack/day for 6 years. She is cur-rently enrolled full-time as a nursing student. On phys-ical examination, she has decreased bowel sounds and a rigid, diffusely tender, and distended abdomen. Her vital signs are as follows: temperature 101.9°F, blood pressure 98/62 mm Hg, and heart rate 127 beats/min-ute. Her laboratory test results are within normal limits except for a WBC of 22 × 103 cells/mm3. A pregnancy test is negative. Abdominal radiography reveals trans-verse colonic dilation to 8 cm. Her home drug therapy includes mesalamine 800 mg three times/day, azathio-prine 50 mg once daily, and olanzapine 10 mg once daily. Four days before admission, A.L. was seen by her physi-cian, who prescribed oxycodone 5 mg every 6 hours as needed for pain and prednisone 40 mg/day.
27. In addition to discontinuing oxycodone and aza-thioprine, which one of the following is best to recommend for A.L.?A. Increase prednisone to 80 mg/day and
increase mesalamine to 1600 mg three times/day.
B. Discontinue mesalamine and prednisone; initiate intravenous hydrocortisone 100 mg every 8 hours.
C. Discontinue mesalamine; increase prednisone to 80 mg/day and initiate an intravenous infusion of cyclosporine 2 mg/kg/day.
D. Discontinue mesalamine and prednisone; initiate an intravenous infusion of infliximab 5 mg/kg.
28. A.L. has a follow-up appointment 3 months later in November. Her symptoms are well controlled on Multi Matrix System (MMX) mesalamine 2.4 g orally daily and azathioprine 50 mg orally daily. She is progressing through her nursing program and will begin her clinical rotations in January. In reviewing A.L.’s vaccination history, you notice that her last tetanus, diphtheria, pertussis vaccines were administered 12 years ago. She has no docu-mented history of chickenpox. She has not received human papillomavirus (HPV) vaccinations. She denies receiving any other vaccines. In addition to tetanus/diphtheria and pneumococcal vaccina-tions, which one of the following vaccine options would be best for A.L. to receive?A. Influenza injectable, HPV, hepatitis B.B. Influenza nasal spray, HPV, hepatitis A.C. Influenza injectable, varicella, hepatitis A.D. Influenza nasal spray, varicella, hepatitis B.
29. At a follow-up visit, A.L. indicates that she would like to stop smoking. Which one of the following counseling points and interventions would be best to provide to A.L.?A. Tell her that that smoking cessation may
worsen UC symptoms; use varenicline 0.5 mg/day titrated to 1 mg twice daily.
B. Tell her that smoking cessation may worsen UC symptoms; use a nicotine patch 21 mg/day and taper.
C. Tell her that smoking cessation may improve UC symptoms; use varenicline 0.5 mg/day titrated to 1 mg twice daily.
D. Tell her that smoking cessation may improve UC symptoms; use a nicotine patch 21 mg/day and taper.
Questions 30–32 pertain to the following case.C.M. is a 37-year-old woman (weight, 59 kg) with no known allergies. She presents to the ambulatory clinic with 7 weeks of new abdominal cramping and two to four loose bloody stools per day. She reports taking only acetaminophen as needed for headaches. Colonoscopy is consistent with UC with superficial inflammation that is continuous from the rectum to the splenic flex-ure. C.M. is currently afebrile with a blood pressure of 116/78 mm Hg and a heart rate of 80 beats/minute. Laboratory findings are within normal limits.

PSAP-VII • Gastroenterology and Nutrition 47 Inflammatory Bowel Disease
30. Which one of the following would be best to rec-ommend for C.M.?
A. Mesalamine suppository rectally 500 mg twice daily plus MMX mesalamine 2.4 g orally daily.
B. Mesalamine enema rectally 2 g/day plus sulfasalazine 1 g orally four times/day.
C. Hydrocortisone enema rectally 100 mg/day plus mesalamine 1.6 g orally three times/day.
D. Prednisone 60 mg orally daily plus sulfasalazine 1 g orally four times/day.
31. Several months later, C.M. presents to the hospital with abdominal pain in her right upper quadrant, fatigue, and weight loss (4 kg in the past month). Current workup includes alkaline phosphatase 200 IU/L, alanine transaminase 130 IU/L, aspar-tate transaminase 150 IU/L, total bilirubin 2.2 mg/dL, and direct bilirubin less than 0.1 mg/dL. Clin-ical presentation, laboratory testing, and imaging are consistent with primary sclerosing cholangitis (PSC). Which one of the following would be best to recommend for C.M. at this time?
A. Colonoscopy at diagnosis and every 1–2 years thereafter; dual-energy x-ray absorptiometry scan at 2–3 years and every 3 years thereafter.
B. Colonoscopy at 8–10 years and every 1–2 years thereafter; dual-energy x-ray absorptiometry scan at 2–3 years and every 3 years thereafter.
C. Colonoscopy at 4–6 years, followed by prophylactic colectomy; dual-energy x-ray absorptiometry scan at diagnosis and every 2–3 years thereafter.
D. Colonoscopy at diagnosis and every 1–2 years thereafter; dual-energy x-ray absorptiometry scan at diagnosis and every 2–3 years thereafter.
32. Which one of the following is the best recommen-dation to treat C.M.’s PSC?
A. Ursodeoxycholic acid 500 mg three times/day.B. Colchicine 0.6 mg/day.C. Ursodeoxycholic acid 250 mg three times/day.D. Pentoxifylline 400 mg three times/day.
33. A 27-year-old man comes to the emergency depart-ment with 2 days of cramping severe abdominal pain, fever, fatigue, and 12 bloody stools per day. He has had CD for 5 years that is complicated by arthri-tis. He has been maintained on mesalamine (Pen-tasa) 1 g twice daily. His vital signs on admission are temperature 100.6°F, heart rate 110 beats/min-ute, respiratory rate 18 breaths/minute, and blood pressure 118/69 mm Hg. Which one of the follow-ing is best to recommend for this patient?
A. Increase the mesalamine dosage to 4 g/day.B. Initiate an intravenous infusion of infliximab 5
mg/kg.C. Administer intravenous hydrocortisone 100
mg every 8 hours.D. Initiate a continuous intravenous infusion of
cyclosporine 4 mg/hour.
34. A 44-year-old man is hospitalized with moder-ate to severe CD located in the colon and termi-nal ileum. His disease has not responded to oral prednisone 40 mg/day for 5 days and intravenous methylprednisolone 60 mg every 12 hours for 5 days. He has no known allergies or significant medical history. He still has a high temperature and severe symptoms. He has normal kidney and liver function, and he has no infection. Which one of the following would be the best therapy to ini-tiate in this patient?
A. Certolizumab 400 mg subcutaneously .B. Metronidazole 500 mg orally three times/day.C. Hydrocortisone 100 mg intravenously every 8
hours.D. Azathioprine 50 mg orally once daily.
35. A 52-year-old woman (weight, 75 kg) presents to the clinic with abdominal pain, swelling of the anal sphincter, and anal fissures on examination. She has bleeding and pain with defecation. Her medical history is significant for CD for the past 20 years. She has not required maintenance therapy for the past few years. Which one of the following would be best to initiate at this time?
A. Mesalamine 2.4 g orally twice daily.B. Mesalamine suppository rectally 500 mg twice
daily.C. Metronidazole orally 500 mg three times/day.D. Prednisone orally 40 mg/day.
36. In a trial, 144 patients receiving standard therapy for mild to moderate UC were randomized to receive adjunctive therapy with a probiotic mixture or pla-cebo. The probiotic mixture used was VSL#3, a com-bination of four strains of Lactobacillus, three strains of Bifidobacterium, and one strain of Streptococ-cus spp. Significantly more patients in the probiotic group achieved the primary end point of a reduc-tion in the Ulcerative Colitis Disease Activity Index of 50% or more compared with placebo (63.1% vs. 40.8%; p=0.031). Which one of the following best describes the number needed to treat to achieve the primary end point in one patient?
A. 1.8.B. 4.5.

PSAP-VII • Gastroenterology and Nutrition48Inflammatory Bowel Disease
C. 22.3.D. 54.7.
37. A 70-year-old man (weight, 65 kg) has a medical history of UC, heart failure (ejection fraction 30%, 1 month ago), and hypertension. His oral drug regi-men includes prednisone 30 mg/day, azathioprine 50 mg/day, carvedilol 6.25 mg twice daily, lisino-pril 20 mg/day, aspirin 81 mg/day, furosemide 20 mg/day, and calcium plus vitamin D 1200 mg/800 international units/day. His heart failure markedly limits his physical activity with fatigue and dyspnea on minimal exertion, but he is comfortable at rest. When he has attempted to taper his corticosteroid dosage, he has experienced relapsing UC with the reduced dosage. He is concerned about long-term adverse effects from prednisone and would like to try another therapy and attempt to taper off the corticosteroid. Which one of the following would be best to recommend for this patient?A. He is not a candidate for infliximab
therapy because heart failure is an absolute contraindication to therapy.
B. Initiate infliximab 325 mg, titrate to 650 mg, and monitor for worsening heart failure symptoms.
C. Initiate infliximab 325 mg and monitor for worsening heart failure symptoms.
D. He is not a candidate for infliximab therapy based on his NYHA classification of heart failure severity.
Questions 38 and 39 pertain to the following case.P.T. is a 50-year-old woman (weight 50 kg) with moder-ate to severe extensive UC for 14 years that is currently in remission. Her oral drug regimen includes mesala-mine 800 mg three times/day and azathioprine 50 mg/day; she receives an intravenous infusion of infliximab 250 mg every 8 weeks. She has been forgetful and has missed two of her appointments. Recent laboratory test data show that she tested positive for antibodies to inf-liximab. She has no symptoms today.
38. Which one of the following would be best for P.T. at this time?A. Increase the infliximab dose to 500 mg.B. Monitor for flu-like symptoms upon
readministration.C. Reduce the infliximab dosing interval to every
6 weeks.D. Change the regimen to intravenous
natalizumab 300 mg.
39. Six months later, P.T. presents with a flare-up of her UC because of self-reported nonadherence to
therapy. Which one of the following patient fac-tors specific to P.T. is most likely increasing her nonadherence?A. Forgetfulness, several daily doses, disease
remission.B. Patient age, disease duration, immune
modulator therapy.C. Forgetfulness, immune modulator, route of
therapy.D. Patient age, disease remission, route of
therapy.
40. A patient has been maintained on certolizumab pegol for his CD. Because he recently changed jobs and his new insurance carrier will not cover the cost of certolizumab pegol, he will be initiated on methotrexate. Which one of the following would be best to assess in this patient before changing therapy?A. Tuberculin purified protein derivative,
hepatitis B and C antibodies, and chest radiography.
B. Chest radiography, complete blood cell count, and liver aminotransferases.
C. 2D echocardiography, hepatitis B and C antibodies, and complete blood cell count.
D. Tuberculin purified protein derivative, 2D echocardiography, and liver aminotransferases.