AAAH 1st Conference October 29,2006 1 Globalization/International Trade and Implications on HRH:...
38
AAAH 1st Conference Octo ber 29,2006 1 Globalization/ International Trade and Implications on HRH: Supply, Demand and Migration F. Marilyn E. Lorenzo RN,DrPH Professor College of Public Health, Institute of Health Policy and Development Studies, National Institutes of Health University of the Philippines, Manila
-
Upload
roxanne-wilkinson -
Category
Documents
-
view
215 -
download
1
Transcript of AAAH 1st Conference October 29,2006 1 Globalization/International Trade and Implications on HRH:...

AAAH 1st Conference October 29,2006
1
Globalization/International Trade and Implications on HRH: Supply,
Demand and MigrationF. Marilyn E. Lorenzo RN,DrPH
ProfessorCollege of Public Health, Institute of Health Policy and
Development Studies, National Institutes of Health University of the Philippines, Manila
AAAH 1st Conference October 29,2006
2
Presentation Outline
• Why trade health services?
• Philippine v Global Situation
• Modes of trade
• Implications of health services trade on HRH development
• Current and proposed solutions

AAAH 1st Conference October 29,2006
3
Why Trade Health Services?

AAAH 1st Conference October 29,2006
4
Exports and Imports of Health Services
to generate jobs & income
to upgrade hard & soft infrastructure
to generate revenues
*Expand scope of services*Improve quality*Provide efficient services
In principle…….
AAAH 1st Conference October 29,2006
5
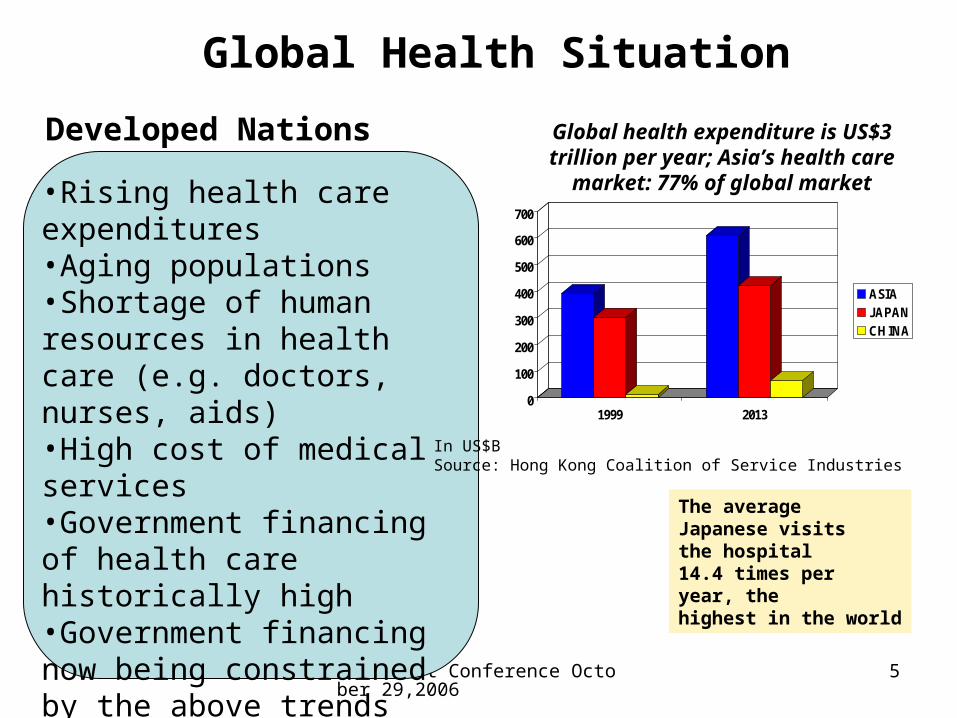
Developed Nations
•Rising health care expenditures•Aging populations•Shortage of human resources in health care (e.g. doctors, nurses, aids)•High cost of medical services•Government financing of health care historically high•Government financing now being constrained by the above trends
Global Health Situation
0
100
200
300
400
500
600
700
1999 2013
ASIAJAPANCHINA
Global health expenditure is US$3 trillion per year; Asia’s health care market: 77% of
global market
In US$BSource: Hong Kong Coalition of Service Industries
The average Japanese visitsthe hospital 14.4 times peryear, thehighest in the world

AAAH 1st Conference October 29,2006
6
Developing Nations
Global Health Situation
•Budget on health services relatively small•Providers lack financial resources
to upgrade
•Health care financing mostly from private
BUT:•Large pool of trainable human resources •Have advantage in tourism
•Need additional fiscal resourcesto fund higher health budgetrequirement
Philippine Scenario55% private financing43% public financing (including social insurance)
DOH budget – 1.6% of totalbudget on social, economic& other services (including finance charges)
Relatively slow expansion &modernization programs, operations not viable
Increasing migration of healthprofessionals
AAAH 1st Conference October 29,2006
7
Modes of Trade
AAAH 1st Conference October 29,2006
8
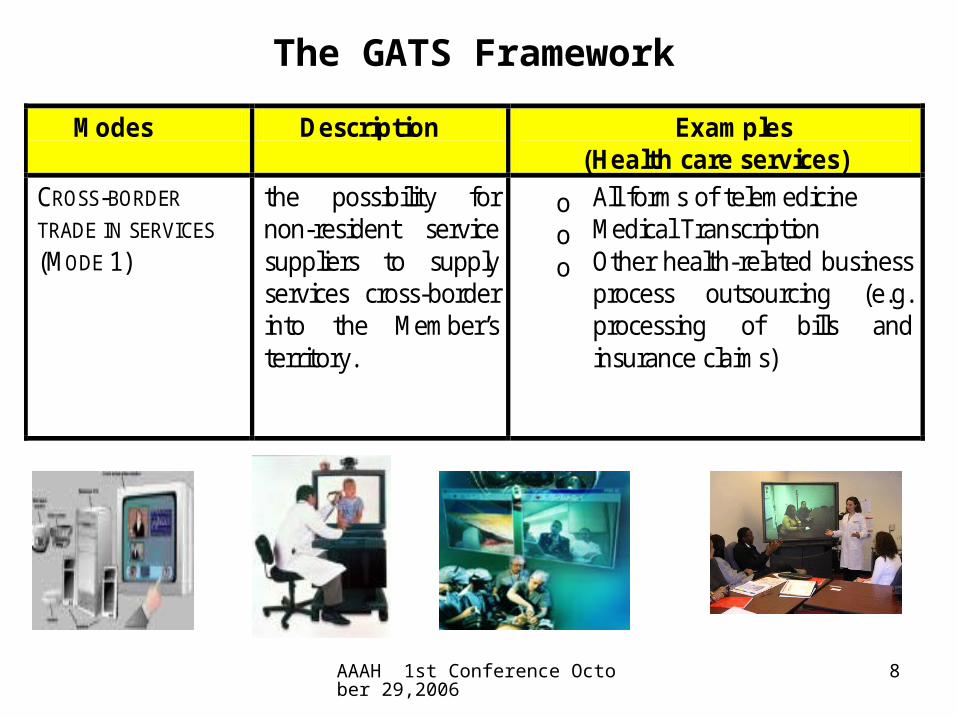
Modes Description Examples (Health care services)
CROSS-BORDER
TRADE IN SERVICES (MODE 1)
the possibility for non-resident service suppliers to supply services cross-border into the Member’s territory.
o All forms of telemedicine o Medical Transcription o Other health-related business
process outsourcing (e.g. processing of bills and insurance claims)
The GATS Framework
AAAH 1st Conference October 29,2006
9
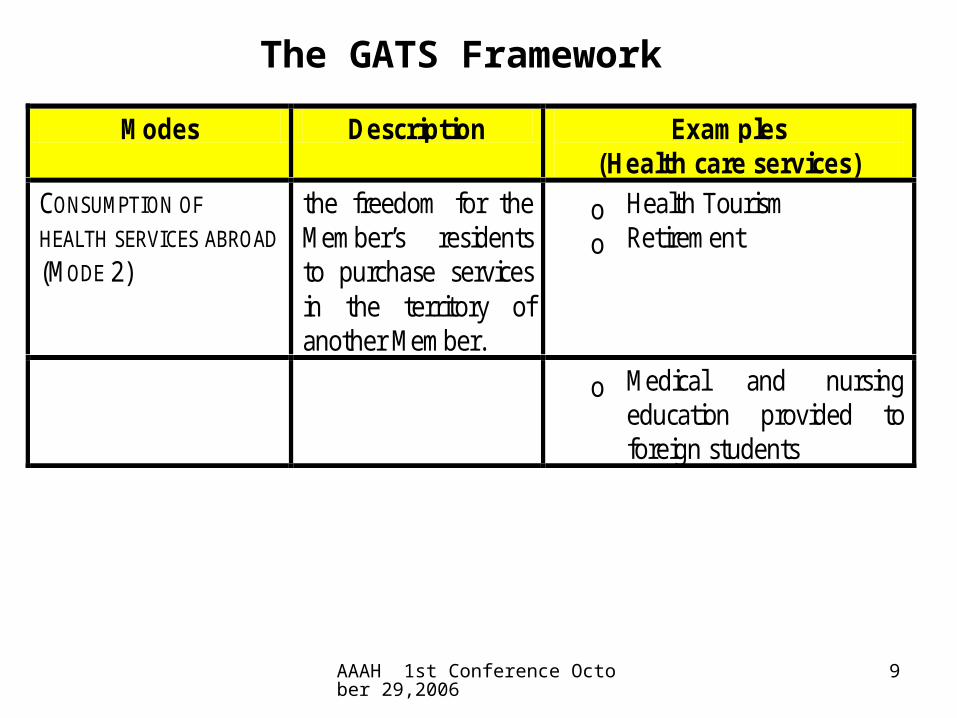
Modes Description Examples (Health care services)
CONSUMPTION OF HEALTH SERVICES ABROAD (MODE 2)
the freedom for the Member’s residents to purchase services in the territory of another Member.
o Health Tourism o Retirement
o Medical and nursing education provided to foreign students
The GATS Framework
AAAH 1st Conference October 29,2006
10
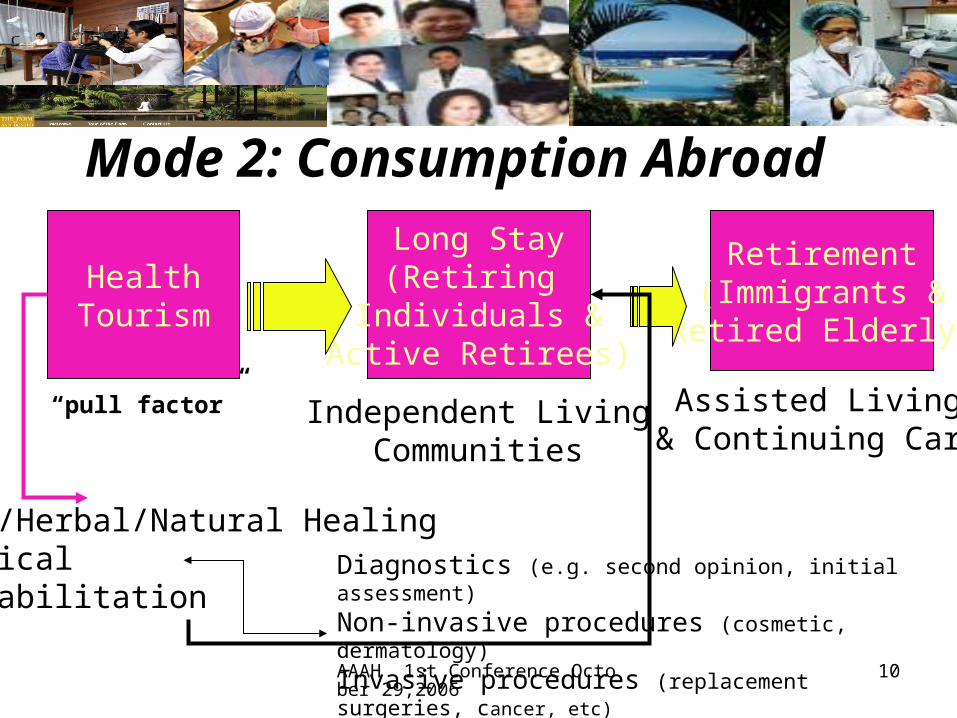
Spa/Herbal/Natural HealingMedicalRehabilitation
HealthTourism
Long Stay(Retiring
Individuals &Active Retirees)
Retirement(Immigrants &Retired Elderly)
Diagnostics (e.g. second opinion, initial assessment)
Non-invasive procedures (cosmetic, dermatology)
Invasive procedures (replacement surgeries, cancer, etc)
Independent LivingCommunities
Assisted Living& Continuing Care
Mode 2: Consumption Abroad
“pull factor”

AAAH 1st Conference October 29,2006
11
Major Drivers for Movement of Patients
Aging PopulationsShortage of Health ProfessionalsHigh Cost of Medical ServicesPoor Health Facilities in home countriesLong waiting for
treatment & surgery

AAAH 1st Conference October 29,2006
12
Major Players in AsiaCountry Volume of Foreign
Patients Export Revenues
Current Markets Targets
Thailand 800,000
US$470 million in revenues
Americans 59,000 Japanese 130,000 Britons 14,000
US$2B (2010)
India 150,000 Middle East and South Asian US$1 (2012)
Malaysia 122,000 foreign patients
($9.4 million).
60% of foreigners who seek treatment are from Indonesia, another 10% are from Brunei, Vietnam, Singapore and Thailand. The rest are from West Asia, South Asia (Bangladesh and India) and Japan.
US$1B ( 2010)
Singapore 150,000 –200,000 (spent S$345 M a year
US$915 M
Indonesians and Malaysians account for 70-85%
1 million international patients per year by 2012 US$2B
Source: NTO wesbites
AAAH 1st Conference October 29,2006
13
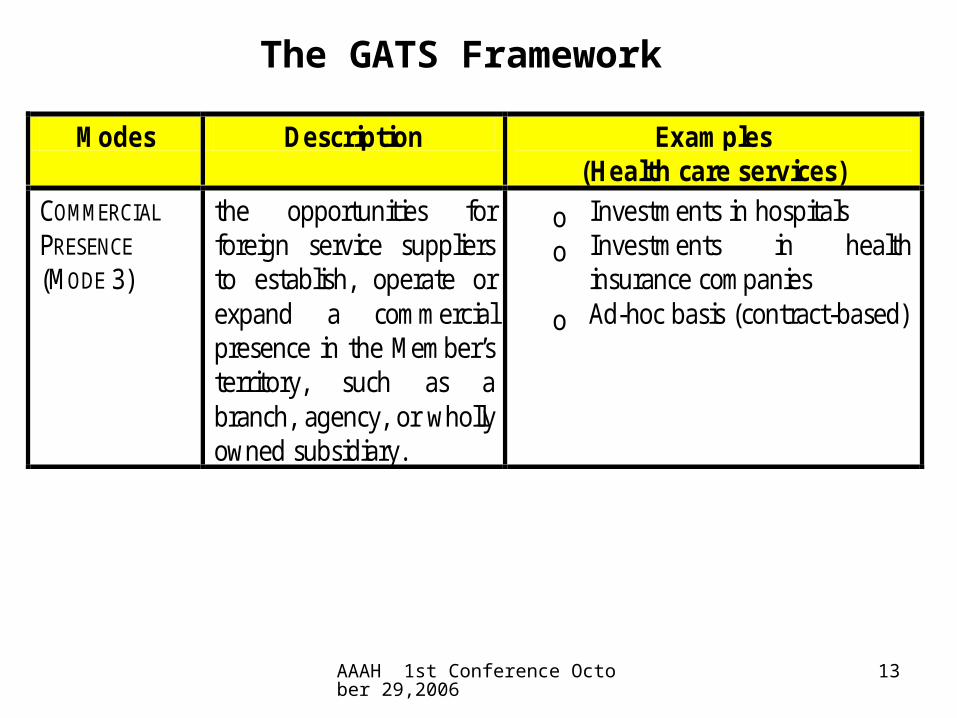
Modes Description Examples (Health care services)
COMMERCIAL
PRESENCE (MODE 3)
the opportunities for foreign service suppliers to establish, operate or expand a commercial presence in the Member’s territory, such as a branch, agency, or wholly owned subsidiary.
o Investments in hospitals o Investments in health
insurance companies o Ad-hoc basis (contract-based)
The GATS Framework
AAAH 1st Conference October 29,2006
14
Mode 3: Commercial Presence
• Options: – Philippine providers set up branches
abroad (exports)– Philippines attract investments in medical
zones or existing facilities (e.g Bumrungrad in Asian Hospital) – imports – and improve finances and enhance local linkages

AAAH 1st Conference October 29,2006
15
Modes Description Examples (Health care services)
MOVEMENT OF
HEALTH
PROFESSIONALS (MODE 4)
the possibilities offered for the entry and temporary stay in the Member’s territory of foreign individuals in order to supply a service.
o temporary movement of health personnel to provide services abroad
o short-term health consulting assignments.
The GATS Framework

AAAH 1st Conference October 29,2006
16
Mode 4: Movement of Natural Persons
• Shortage of Medical Professionals Abroad• Philippines is major exporter in this trade• Migration will still continue • Seek better market access and national
treatment for our health professionals• Foreign medical professionals are allowed entry
only under certain intra-company arrangements or contracts but not allowed to practice or establish commercial presence

AAAH 1st Conference October 29,2006
17
Summary of Risks/Trade-OffsModes of Trade Health Policy Objectives
Equity Quality Efficiency
Cross-border Remote areas serviced
Improved v. Substantial investment
Movement of Consumers
“crowding out” of nationals
Migration of public health workers to private
v. Improved quality
Skills upgrading
v. Possible loss of investment
Commercial Presence
Possible two-tier system
v. Possible freeing up of resources
Movement of Natural Persons
Reduced access to services
Loss of quality Loss of public investments v. foreign exchange remittances
Source:Adam and Kinnon (1998)

AAAH 1st Conference October 29,2006
18
•Aging Populations in
OECD
•Shortage of medical professionals
•Exports of Medical Professionals
•Commercial presence on ad-hoc basis•Tele-education and/ormovement of foreignstudents to the Phil•High Cost of Medical
Services
•Health Tourism •Long Stay•Retirement
•Requirements for maintenanceof patient records•Relatively high cost of labor fortranscription
Telemedicine
•Poor healthcare systemsin developing nations
•Telemedicine (tele-diagnosis/teleconsultation)
post-consultation *between patient and physician or *between physicians
Medical Transcription
•Aging Populations inOECD
•Shortage of medical professionals
•Exports of Medical Professionals
•Commercial presence on ad-hoc basis•Tele-education and/ormovement of foreignstudents to the Phil•High Cost of Medical
Services
•Health Tourism •Long Stay•Retirement
•Requirements for maintenanceof patient records•Relatively high cost of labor fortranscription
Telemedicine
•Poor healthcare systemsin developing nations
•Telemedicine (tele-diagnosis/teleconsultation)
post-consultation *between patient and physician or *between physicians
Medical Transcription
Exportable Health Services
AAAH 1st Conference October 29,2006
19
Health Services trade and HRH Development

AAAH 1st Conference October 29,2006
20
Major Issue: Human Resources Development
Health TourismRetirement
*Exodus of Doctors and Nurses*Decline in Enrollment in Medicine*Rapid Increase in Enrollment in Nursing*Decline in Quality of Nursing Education
Poor National Health Care System
Low Salaries of Medical ProfessionalsLack of Opportunities for Medical Professionals in the CountryLow Budget on Health Expenditures

AAAH 1st Conference October 29,2006
21
Deployment of Nurses (POEA,2005)
Year Deployed OFW Nurses
Migrant Nurses Total Outflow of Nurses
1992 5,747 1,226 6,973
2000 7,683 1,230 8,913
2001 13,536 1,575 15,111
2002 11,911 2,248 14,159
2003 8,773 2,246 11,019

AAAH 1st Conference October 29,2006
22
Nurse Medics• Enrollment in nursing in NCR increased from
8,600 in 1998-99 to 34,277 in SY 2003-04• Enrollment in medicine declined from 7,162 in
SY 1998-99 to 6,551 in SY 2003-04• Enrollment in medicine declined from 9,106 in
SY 2002-03 to 6,551 in SY 2003-04

AAAH 1st Conference October 29,2006
23
Deterioration of Quality (PRC,2006)
Year NLE Examinees
NLE Passers
% Passing
1994 41,459 25,477 61%
2000 9,270 4,602 50%
2002 9,453 4,228 45%
2003 15,624 7,528 48%
2004 25,294 (62%)
12,581 49.7%
2005 50,280 25,951 51.6%

AAAH 1st Conference October 29,2006
24
Performance of Nursing SchoolsCHED NURSING SCHOOL REPORT CARD (CHED, 2005)
CATEGORY AVERAGE % BOARD PERFORMANCE
NUMBER OF SCHOOLS
% OF SCHOOLS
OUTSTANDING PERFORMANCE
90%-ABOVE 12 4.4
HIGH PERFORMANCE
75-89% 15 8.5
AVERAGE PERFORMANCE
50-74% 46 26.2
LOW PERFORMANCE
30-49% 64 36.5 58.2
VERY LOW PERFORMANCE
BELOW 30% 38 21.7
SUB TOTAL: 175 65.0
SCHOOLS WITH LESS THAN 5- YEAR AVERAGE
94 35.0
TOTAL 269 100.00

AAAH 1st Conference October 29,2006
25
Current and Proposed Solutions

AAAH 1st Conference October 29,2006
26
Major Goal
In the exchange ensure
Mutual Benefits!

AAAH 1st Conference October 29,2006
27
Government is supporting these initiatives….
DTI-Board of Investments2005 Investments Priorities Plan
Department of TourismDepartment of Health
Executive Order No. 372
NEDA MTPDP 2005-2010
PEZA
There’s need to coordinate and harmonize private and public sector initiatives.
Focus of private-public partnership (Cluster-based Approach):
•Upgrading quality of hard and soft infrastructure•Work towards reaching international standards of health care delivery•Explore the potentials of the local market to upgrade quality

AAAH 1st Conference October 29,2006
28
Strategic Directions: HRH Master Plan
Human Resource Development Increase health budget specifically on HRH Dev’t
To increase benefits allowable via social health insurance in order to increase demand for health care by 3 timesStrengthen capacity of Philhealth as an insurerAccess to funds by physicians particularly those in the provinces
Improve retention/return schemes: e.g. brain circulation Encourage lifelong learning (building credentials): Career mgt. Pursue proposals of NIH and PMA:
National Service ActCreation of Commission on Health Human Resources Development (can be part of the overall national structure)

AAAH 1st Conference October 29,2006
29
Strategic Directions:HRHMP
Developing Firm InfrastructureNeed for database/inventory of facilities and business networks here and abroadAccreditation of major hospitals with JCIAccess to financing via investment opportunities (e.g. joint ventures, management contracts)Cluster-based Approach: Closer links among associations across health and related industries (e.g. medical, travel, IT, etc.), government and academe

AAAH 1st Conference October 29,2006
30
Options for Negotiations• Conduct multi-stakeholder meetings to discuss Philippine
position in the GATS framework, regional arrangements, and bilateral arrangements specifically:
• Identifying the benefits and costs in relation to health objectives
• Implementation of exchange compensation schemes• Open up activities with significant inflows of capital that
would enhance local linkages• Identifying options for allowing foreign medical practitioners
and foreign investors and mutual recognition of licenses and standards
AAAH 1st Conference October 29,2006
31
Thank You !
Mabuhay!

AAAH 1st Conference October 29,2006
32
Major Drivers for Movement of Patients
• Aging Populations in OECD
Country 1996 2010 Australia 15.6 19.3 Canada 16.2 20.4 Denmark 16.5 23.0 France 20.2 22.5 Germany 21.0 25.1 Italy 22.1 26.1 J apan 21.0 29.8 Netherlands 17.9 22.3 Switzerland 19.3 23.6 UK 20.7 23.3 US 16.4 18.8
In the year 2025, the proportion of those 65 and over will be highest in Japan, followed by Italy.
Source: WB

AAAH 1st Conference October 29,2006
33
Major Drivers for Movement of Patients
Country Extent of Shortage and Year
Canada 78,0000 (2011)113,000 (2016)
Australia 31,000 (2006)40,000 (2010)
Aging PopulationsShortage of Health Professionals
Sources:

AAAH 1st Conference October 29,2006
34
Major Drivers for Movement of Patients
Aging PopulationsShortage of Health ProfessionalsHigh Cost of Medical Services 0 20000 40000 60000 80000 100000
Bangkok
Singapore
London
USA
India
Kuala Lumpur
Japan
Philippines
0 500 1000 1500 2000 2500 3000 3500 4000
Bangkok
Singapore
London
USA
Kuala Lumpur
Japan
Philippines
Cost of Daily HospitalizationUSA – US$1,742Japan – US$800Philippines – US$25-40
Cost of Cardiac ByPass Surgery (in US$)
Cost of Comprehensive Male Examination
Source: PATA; UA&P
Source: PATA;UA&P

AAAH 1st Conference October 29,2006
35
Major Drivers for Movement of Patients
Aging PopulationsShortage of Health ProfessionalsHigh Cost of Medical ServicesPoor Health Facilities in home countries
•Citizens of Micronesian States and other Southeast Asian countriessuch as Indonesia take advantage ofthe cheaper cost of services andbetter quality of facilitiesin developing countries like Thailand,Philippines, India
AAAH 1st Conference October 29,2006
36
Need for Strategic Directions
•Lack of framework on the development of the health services sector•Absence of unified body to address local health sector and trade concerns •Lack of human resources development plan in relation to the needs of the local population and trade potentials•Absence of roadmap on exportable health services •Lack of inventory of health care providers/health professionals•Lack of discussions on the implications of the GATS among doctors, nurses or students and how to address possible risks•Lack of statistics on the contributions of other modes of health services trade(e.g. health tourism)BUT – private sector initiatives are existing

AAAH 1st Conference October 29,2006
37
Strategic Directions• Institutional Structure
– Foster private sector initiatives– Government to support or enable rather than increase intervention– Public-private mix to optimize scarce resources and create forum for public
discussions– Clearly define the national structure (from the existing inter-agency groups) to
address development of health services and trade in health services (e.g human resource development, coordination among stakeholders, development of common vision and targets)
• London Medicine• Australia’s National Health Industry Development Forum• Singapore Medicine• Malaysia’s 5-Committees
– Establishment of an incentive structure targeted at specific services such as health tourism and designed to attract capital flows and enhance local linkages (already initiated by BOI)

AAAH 1st Conference October 29,2006
38
Need for Strategic Directions• Domestic Policies
– Foreign Direct Investment – Policies to ensure universal access (Let’s not
ignore domestic market potentials)– Regulatory Policy on Standards and Accreditation
• International Policies – Work on insurance portability– Recognition of hospital and professional
standards