A preliminary study of the percentage of sealer penetration in rootsobturated with the Thermafil and...

of 8
Transcript of A preliminary study of the percentage of sealer penetration in rootsobturated with the Thermafil and...
-
8/7/2019 A preliminary study of the percentage of sealer penetration in rootsobturated with the Thermafil and RealSeal-1 ob
1/8
A preliminary study of the percentage of sealer penetration in rootsobturated with the Thermal and RealSeal-1 obturationtechniques in mesial root canals of mandibular molarsRonald Ordinola-Zapata, DDS,a Clovis M. Bramante, DDS, PhD,aNorberti Bernardineli, DDS, PhD,a Marcia S. Z. Graeff, MSc,bRoberto Brando Garcia, DDS, PhD,a Ivaldo Gomes de Moraes, DDS, PhD,a andGilberto Debelian, DDS, PhD,c Bauru, Brazil; and Oslo, NorwayUNIVERSITY OF SO PAULO AND UNIVERSITY OF OSLO
Objective. The aim of this study was to evaluate the percentage of sealer penetration in root canals lled with theThermal or RealSeal-1 systems analyzed by confocal laser scanning microscopy (CLSM).Study design. Twenty canals in 10 mesial roots of mandibular molars were cleaned and shaped using ProTaper andProFile instruments to a size 35 and .04 taper at the apex and lled using RealSeal-1 or Thermal systems in themesial canal of each root. Horizontal sections were made at the 3 and 5 mm levels from the apex, and the percentageof sealer penetration in the root canal walls was analyzed using CLSM.
Results. Thin layers of sealer (2-30 m) and sealer tags into dentinal tubules were found in the root canal walls in ahigh percentage using both techniques at both evaluated levels, with no statistical differences between the techniques(Student t test: P .05).Conclusion. The percentage of sealer penetration in the root canal walls was similar using both thermoplastic carriersbased systems. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:961-968)
The rst stage of root canal therapy is microbial con-trol, followed by root canal lling. Microbial controlincludes removal of the protein degradation products,toxins, and microbes.1 Root lling has 3 functions: toprevent periapical uids from tracking into the canal tofeed remaining bacteria, to entomb remaining bacteria,and to inhibit coronal leakage of oral bacteria.2
Most obturation techniques use a solid core materialsuch as gutta-percha in conjunction with a sealer. An-other technique uses a polyester resin-based material(Resilon) with a dual-curable dental resin as the sea-ler.3,4 Because gutta-percha or Resilon core materialscannot ll the canal irregularities, a sealer is also used.However, because the sealer can dissolve or shrink, it isthought that the thinner the sealer layer, the less thepotential for gaps developing and thus presumably thebetter the seal.5,6 Thus the use of a heat source can
enhance the thermoplastic properties of both core ma-terials to allow for a thinner sealer layer and a morecomplete obturation.7
Adhesive root llings have been a matter of exten-sive research in the past few years.8 Animal models andlaboratory research have shown similarity or improve-ment of the coronal seal when Resilon was used com-pared with gutta-percha root llings.9-11 Although ad-hesive root llings may be advantageous in theory,several requirements need to be fullled. Many studieshave compared gutta-percha and Resilon systems ad-hesion to the root canal dentin using mostly push-outtests.12,13 Scanning electron microscopy studies haveshown that gaps can be present between the sealer andthe root canal wall with both systems.14 To achieve thegoal of adhesion between the core material, sealer, androot dentin it is essential that there is even distributionof sealer between the core material and the root canalwall. In this way, voids will be avoided and leakagewill be less likely.
Evaluation of root canal lling techniques are com-monly performed in single-rooted teeth. For standard-ization purposes, this model involves the use of acircular root canal. The ability to evaluate the root canallling techniques in teeth with similar root canal diam-eters, avoiding anatomic irregularities, consequentlyimproves the statistical analyses. Although relativestandardization of the internal anatomy is useful for
Supported in part by The State of So Paulo Research Foundation(FAPESP) (2007/01838-7).aDepartment of Endodontics, Bauru Dental School, University of SoPaulo.b Integrated Research Center, Bauru Dental School, University of SoPaulo.cFaculty of Dentistry, University of Oslo.Received for publication Mar 30, 2009; returned for revision Jun 25,2009; accepted for publication Jul 6, 2009.1079-2104/$ - see front matter 2009 Mosby, Inc. All rights reserved.doi:10.1016/j.tripleo.2009.07.016
961
-
8/7/2019 A preliminary study of the percentage of sealer penetration in rootsobturated with the Thermafil and RealSeal-1 ob
2/8
laboratory purposes, irregular anatomy is more fre-quently found in clinical practice, limiting the clinicalextrapolation of laboratory study results. For these rea-sons, the use of a more complex root canal anatomyseems prudent for in vitro evaluation of root canallling methods.
The Thermal technique involves the obturation of theroot canal with heated gutta-percha on a plastic carrier.Genoglu15 stated that carrier-guided gutta-percha tech-niques are easier to use than most of the thermoplastictechniques and are able to reduce the sealer component,showing less leakage in vitro compared with the lateralcompaction technique. Recently a Resilon carrier obtura-tion system (RealSeal-1; SybronEndo, CA) has beenintroduced into the market for uses combined with aSelf-Etch sealer (RealSeal-1; SybronEndo, Orange, CA).The main components of the sealer are methacrylatemonomers, partially containing carboxylic acid groups,
llers of calcium phosphate, Ca-Al-F-silicate (glass iono-mer powder), silanated barium borosilicate glass, and ra-diopaque llers. The carrier is a polysulfone-containingpolymer with radiopaque ller, and the surrounding Re-silon contains polycaprolactone and polyolen polymersloaded with llers, such as bioactive glass, bismuth oxy-chloride, and barium sulfate.11
Recent studies have shown that thermoplasticizedResilon canow into grooves and depressions in a splittooth model7 or in articial lateral canals in a similarfashion to gutta-percha.16 Potential advantages of theResilon-based carrier lling method claimed by the
manufacturer are: 1) The Resilon bonds to the core,eliminating a potential pathway for bacterial leakage; 2)the RealSeal-1 is injection molded, ensuring that thecore is centrally placed in the outer Resilon; and 3) boththe Resilon and carrier are dissolvable in commonlyused solvents as chloroform, ensuring that retreatmentwill be manageable if it becomes necessary.
There is a lack of studies that evaluated lling tech-niques or distribution of sealer using transversal sec-tions in irregular anatomies, such as the mesial rootcanals of mandibular molars. In view of the fact thatthere was no study evaluating the lling ability of theRealSeal-1 technique, the aim of the present prelimi-nary study was to evaluate the percentage of sealerpenetration in mesial root canals of mandibular molarslled with the RealSeal-1 or Thermal systems ana-lyzed by confocal laser scanning microscopy (CLSM).
MATERIAL AND METHODSCollection of teeth
Ten mesial roots of extracted mandibular rst molarswere used in this study. The teeth were stored in salinesolution containing 0.1% sodium azide at 4C until use.The selected mesial roots had 2 separate canals and 2
independent foramina (Weine type III), giving a total of 20 root canals. Root canal curvatures were 20 ac-cording to the Schneider method.17
Root canal preparation and llingAfter preparation of standard access cavities, the work-
ing length of each canal was established by measuring thepenetration of a 15 K-le (Flexole; Dentsply Maillefer,Ballaigues, Switzerland) until it reached the apicalforamen and then subtracting 1 mm. The canals wereprepared with the ProTaper technique (Dentsply Mai-llefer) to a size of the F2 instrument at the workinglength. The handpiece was used with an electric engine(X-Smart; Dentsply Maillefer) at 250 rpm. Instrumen-tation was completed with 30.04 and 35.04 ProFileinstruments (Dentsply-Maillefer) up to the workinglength. A solution of 2.5% sodium hypochlorite (Biod-inmica, Ibipora, Brazil) was used continuously duringthe root canal shaping, 2 mL for each le used. A nalirrigation with sodium hypochlorite was performed for1 minute using a 20 K-le attached to the handpiece of an ultrasound unit (Jet-Sonic Four Plus; Gnatus, Ri-beiro Preto, Brazil) set to the Endo mode withintensity adjusted to level 5 (in a range of 1 to 10). Toeliminate the smear layer, 2 mL 17% EDTA for 3minutes was used followed by a nal rinse of distilledwater.
Twenty root canals (10 buccal and 10 lingual canals)were lled at random using RealSeal-1 and RealSealSE sealer (SybronEndo) or Thermal and ThermaSeal
Plus (Tulsa Dental, Tulsa, OK). One system was usedfor each mesial root canal. First a verier that t looselyto 1 mm short of the working length was selected.RealSeal SE and ThermaSeal Plus sealers were placedinto the canal using conventional Resilon or gutta-percha 35.04 master points. To allow the posterioranalysis under the confocal laser scanning microscope,each sealer was labeled with rhodamine B dye (Sigma-Aldrich, St. Louis, MO) to an approximate concentra-tion of 0.1%.18,19
Obturations were performed by using 35.04 RealSeal-1or Thermal carrier points. The RealSeal-1 (SybronEndo)
and Thermaprep (Dentsply-Tulsa) ovens were used foreach technique, respectively, according to manufac-turer instructions. After the lling procedures, the ac-cess cavity was cleaned by removing excess of obtu-ration material, and 2 radiographs were taken inorthoradial and proximal view. One investigator per-formed all of the clinical procedures.
Sectioning and image analysisResilon- and gutta-perchalled roots were stored in
an anaerobic jar (AnaeroGen; Oxoid, Basingstoke,U.K.) at 37C for 48 hours and then stored at 100%
OOOOE 962 Ordinola-Zapata et al. December 2009
-
8/7/2019 A preliminary study of the percentage of sealer penetration in rootsobturated with the Thermafil and RealSeal-1 ob
3/8
-
8/7/2019 A preliminary study of the percentage of sealer penetration in rootsobturated with the Thermafil and RealSeal-1 ob
4/8
-
8/7/2019 A preliminary study of the percentage of sealer penetration in rootsobturated with the Thermafil and RealSeal-1 ob
5/8
rhodamine B into the sealer is essential toobserve theextent of sealer adaptation and penetration.18
Despite the advantages of confocal microscopy forthe analyses of sealer/dentin interface, it is important todetermine whether or not the dye is leaching from curedresin, because this fact would interfere with the analy-sies of microscopic images.34 In the present study, thisfactor was veried using the orthogonal section tool(Z-optical section). An image should be considered asappropriate if the red uorescence is restricted to thesealer layer and to the lumen of dentinal tubules or
lateral branches. Another consideration is the possibil-ity of the dye to alter the polymerization of the sealerwith potential to reduce the bond strength of the testedmaterials to their substrate.33 In the present work, pilotstudies were performed to verify that the sealers labeledwith 0.1% rhodamine did not alter the ow, accordingto the ADA specication. Also, a complete set of thesealers was found in all of the samples evaluated.However, further studies should address the inuenceof the rhodamine dye on the physicochemical proper-ties of different sealers.
core
BA
Resilon
*
Resilon
core
Resilon
DC
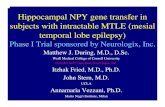
Fig. 2. A, Representative 100 picture of a canal lled with the RealSeal-1 technique. Sealer tags are present in dentinal tubules.Some areas (arrows ) show a well dened uorescent layer between the Resilon and the dentin, corresponding to the sealer. *Thearea in the square in which a consistent uorescent layer is not evident is shown in detail inB, where a thin layer of sealer (5
m) could be seen. No voids were found.C, Representative 100 picture of a canal lled with the RealSeal-1 technique. No voidswere found in this canal. A magnication of the interface is showed inD, where sealer tags are visible in this interface despitethat no layer of sealer could be seen, good adaptation of the Resilon to the canal walls is shown.
OOOOEVolume 108, Number 6 Ordinola-Zapata et al. 965
-
8/7/2019 A preliminary study of the percentage of sealer penetration in rootsobturated with the Thermafil and RealSeal-1 ob
6/8
Earlier studies have used mandibular rst molars
with independent foramens to evaluate apical leakagein lling techniques.22,35 An advantage for comparativepurposes for root canal lling techniques is that sealerscan be directly compared simultaneously in a similardentin structure with similar dentin permeability, be-cause the specimens do not have individual or agevariations. Consequently, bias caused by dissimilarityin dentin structure can be excluded. In spite of theadvantages of the use of mandibular molars during thestudy of the lled area and sealer dentin interface, somecritical points are evident, such as the difculty of standardization of the isthmus areas complicating the
measurement of the gutta-percha or Resilon-lled ar-
eas. However, even with these limitations, it is obviousthat more studies are needed involving more complexanatomic teeth. Future studies need to evaluate theability of different lling techniques to get a completeobturation of irregular anatomies, including isthmuses.Furthermore, to avoid the inuence of anatomic irreg-ularities, serial cross-sections from the pulp chamber tothe apex need to be evaluated to improve the statisticalanalyses.
Because an appropriate lled canal requires an ap-propriate cleaning and shaping procedure, a 35.04 ro-tary le was used at 1 mm from the foramen, because
core
core
GP
GP
D
GP
GP
core
GP
BA
C
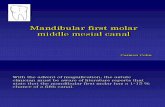
Fig. 3. A, 100 picture of a canal lled with the Thermal technique. Evaluation of the interface shows a good adaptation of gutta-percha to the canal walls in the absence of a sealer layer (B and C, where sealer tags are present in great number insidedentinal tubules).D, Plastic core-dentin interface. A layer of sealer of 10m is evident between the gutta-percha and the dentin,until the plastic core contacts the dentin (arrow ). Sealer tags are still visible in this interface.
OOOOE 966 Ordinola-Zapata et al. December 2009
-
8/7/2019 A preliminary study of the percentage of sealer penetration in rootsobturated with the Thermafil and RealSeal-1 ob
7/8
clinical antimicrobial efcacy using this diameter hasbeen reported compared with a 30.04 diameter in man-dibular molar when sodium hypochlorite was used.36Additionally studies have shown that a diameter of 0.35mm is necessary to allow the irrigant solution to reachthe apex.37
The present study showed that stripping of the plasticcore in Thermal-lled canals was more common com-pared with the RealSeal-1 llings, even when a verierwas used. Similarly, Jarrett et al.38 showed that rootcanals lled with Thermal revealed the carrier directlyagainst the wall of the canals. The CLSM pictures of the core-dentin interface showed that sealer was dis-placed inside the dentin with absence of gaps betweenthe plastic core and the dentin. However, the ability of bacteria to penetrate core/dentin interfaces has not beenstudied yet. To avoid core/dentin interface the use of asmaller size of carrier should be selected when the
Thermal technique is used (i.e., a 30.04 Thermal fora 35.04 apical size).Self-etch sealers have been incorporated recently
into the endodontic practice, such as MetaSeal (Parkell,Farmington, NY) and RealSeal SE. This kind of sealerhas been designed with the intention of combining aself-etching primer and a moderately lled owablecomposite into a single product, to make possible theadhesion to the dentin substrates.39 These sealers aresimilar to self-adhesive luting cements, and it is as-sumed that the bonding mechanism is similar. Phys-icochemical tests were performed by Resende et al.40
to study the solubility of different sealers. Theirresults showed that the Epiphany self-etch sealer(now RealSeal SE) had similar solubility values com-pared with the AH Plus sealer. Interestingly, one of thecomponents of the RealSeal SE sealer is the Ca-Al-Fsilicate (glass ionomer powder). The RealSeal SE man-ufacturer claims that the bonding mechanism to thetooth mineral components is similar to that of glassionomer cements, including an ionic interaction withcalcium and/or phosphate ions (Pentron communica-tion). However, because these sealers are still relativelynew, information on their adhesive properties in EDTA-
treated dentin is still limited.39
Current lling materials must reach many physical,chemical, and biologic requirements. Nevertheless, toreach the benets that the materials proclaim, they mustbe correctly used by the clinicians, preferably with theless sensitive technique. Furthermore, because bacteriais the main etiologic factor of primary and persistentapical periodontitis, future studies using microscopictechniques should be performed to show if the Resilonor gutta-percha interfaces are able to avoid bacterialpenetration, because few studies exist that verify in situthe presence of bacteria in samples showing leakage.41
Furthermore, the relationship between sealer solubility/ dentin infection and the bacterias ability to infectlled dentinal tubules should be explored in futurestudies.
CONCLUSIONSBoth core-carrierbased techniques allowed a thin
layer of sealer with extensive penetration of sealer tagsaround the root canal walls. The percentage of sealerpenetration into the root canal walls was similar usingeither the RealSeal-1 or the Thermal technique.
The authors thank Edimauro de Andrade for his experttechnical assistance.
REFERENCES1. Schilder H. Filling root canals in three dimensions. Dent Clin
North Am 1967;11:723-44.2. Sundqvist G, Figdor D. Endodontic treatment of apical periodon-
titis. In: rstavik D, Pitt Ford TR, editors. Essential endodontol-ogy. 5th ed. Oxford: Blackwell; 2003. p. 242-68.
3. Conner DA, Caplan DJ, Teixeira FB, Trope M. Clinical outcomeof teeth treated endodontically with a nonstandardized protocoland root lled with resilon. J Endod 2007;33:1290-2.
4. Cotton TP, Schindler WG, Schwartz SA, Watson WR, Har-greaves KM. A retrospective study comparing clinical outcomesafter obturation with Resilon/Epiphany or Gutta-Percha/Kerrsealer. J Endod 2008;34:789-97.
5. Kontakiotis EG, Wu MK, Wesselink PR. Effect of sealer thick-ness on long-term sealing ability: a 2-year follow-up study. IntEndod J 1997;30:307-12.
6. De-Deus G, Coutinho-Filho T, Reis C, Murad C, Paciornik S.Polymicrobial leakage of four root canal sealers at two different
thicknesses. J Endod 2006;32:998-1001.7. Alicia Karr N, Baumgartner JC, Marshall JG. A comparison of gutta-percha and Resilon in the obturation of lateral grooves anddepressions. J Endod 2007;33:749-52.
8. Tay FR, Pashley DH. Monoblocks in root canals: a hypotheticalor a tangible goal. J Endod 2007;33:391-8.
9. Leonardo MR, Barnett F, Debelian GJ, de Pontes Lima RK,Bezerra da Silva LA. Root canal adhesive lling in dogs teethwith or without coronal restoration: a histopathological evalua-tion. J Endod 2007;33:1299-303.
10. Eldeniz AU, Orstavik D. A laboratory assessment of coronalbacterial leakage in root canals lled with new and conventionalsealers. Int Endod J 2009;42:303-12.
11. Duggan D, Arnold RR, Teixeira FB, Caplan DJ, Tawil P. Peri-apical inammation and bacterial penetration after coronal inoc-ulation of dog roots lled with RealSeal 1 or Thermal. J Endod2009;35:852-7.
12. Sly MM, Moore BK, Platt JA, Brown CE. Push-out bondstrength of a new endodontic obturation system (Resilon/Epiph-any). J Endod 2007;33:160-2.
13. Jainaen A, Palamara JE, Messer HH. Push-out bond strengths of the dentine-sealer interface with and without a main cone. IntEndod J 2007;40:882-90.
14. Tay FR, Loushine RJ, Weller RN, Kimbrough WF, Pashley DH,Mak YF, et al. Ultrastructural evaluation of the apical seal inroots lled with a polycaprolactone-based root canal lling ma-terial. J Endod 2005;31:514-9.
15. Gencoglu N, Garip Y, Bas M, Samani S. Comparison of differentgutta-percha root lling techniques: Thermal, Quick-ll, Sys-
OOOOEVolume 108, Number 6 Ordinola-Zapata et al. 967
-
8/7/2019 A preliminary study of the percentage of sealer penetration in rootsobturated with the Thermafil and RealSeal-1 ob
8/8
tem B, and lateral condensation. Oral Surg Oral Med Oral PatholOral Radiol Endod 2002;93:333-6.
16. Karabucak B, Kim A, Chen V, Iqbal MK. The comparison of gutta-percha and Resilon penetration into lateral canals withdifferent thermoplastic delivery systems. J Endod 2008;34:847-9.
17. Schneider SW. A comparison of canal preparations in straight
and curved root canals. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1971;32:271-5.18. Bitter K, Paris S, Martus P, Schartner R, Kielbassa AM. A
confocal laser scanning microscope investigation of differentdental adhesives bonded to root canal dentine. Int Endod J 2004;37:840-8.
19. Gharib SR, Tordik PA, Imamura GM, Baginski TA, Goodell GG.A confocal laser scanning microscope investigation of the epiph-any obturation system. J Endod 2007;33:957-61.
20. Perdigao J, Lopes MM, Gomes G. Interfacial adaptation of adhesive materials to root canal dentin. J Endod 2007;33:259-63.
21. Gencoglu N, Samani S, Gunday M. Dentinal wall adaptation of thermoplasticized gutta-percha in the absence or presence of smear layer: a scanning electron microscopic study. J Endod1993;19:558-62.
22. Gutmann JL, Saunders WP, Saunders EM, Nguyen L. An as-sessment of the plastic Thermal obturation technique. Part 2.Material adaptation and sealability. Int Endod J 1993;26:179-83.
23. Shipper G, Orstavik D, Teixeira FB, Trope M. An evaluation of microbial leakage in roots lled with a thermoplastic syntheticpolymer-based root canal lling material (Resilon). J Endod2004;30:342-7.
24. De-Deus G, Reis C, Beznos D, de Abranches AM, Coutinho-Filho T, Paciornik S. Limited ability of three commonly usedthermoplasticized gutta-percha techniques in lling oval-shapedcanals. J Endod 2008;34:1401-5.
25. Wu MK, Kastakova A, Wesselink PR. Quality of cold and warmgutta-percha llings in oval canals in mandibular premolars. IntEndod J 2001;34:485-91.
26. Mamootil K, Messer HH. Penetration of dentinal tubules byendodontic sealer cements in extracted teeth and in vivo. IntEndod J 2007;40:873-81.
27. Sen BH, Piskin B, Baran N. The effect of tubular penetration of root canal sealers on dye microleakage. Int Endod J 1996;29:23-8.
28. Oliver CM, Abbott PV. Correlation between clinical success andapical dye penetration. Int Endod J 2001;34:637-44.
29. Susini G, Pommel L, About I, Camps J. Lack of correlationbetween ex vivo apical dye penetration and presence of apicalradiolucencies. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2006;102:e19-23.
30. Cenci MS, Tenuta LM, Pereira-Cenci T, Del Bel Cury AA, tenCate JM, Cury JA. Effect of microleakage and uoride onenamel-dentine demineralization around restorations. Caries Res2008;42:369-79.
31. Ordinola-Zapata R, Bramante CM, Graeff MZ, del Carpio PA,Vivan RR, Camargo EJ, et al. Depth and percentage of penetra-
tion of endodontic sealers into dentinal tubules after root canalobturation using a lateral compaction technique: a confocal laserscanning microscopy study. Oral Surg Oral Med Oral Pathol OralRadiol Endod. In press.
32. Dalat DM, Spangberg LS. Comparison of apical leakage in rootcanals obturated with various gutta percha techniques using a dyevacuum tracing method. J Endod 1994;20:315-9.
33. DAlpino PH, Pereira JC, Svizero NR, Rueggeberg FA, PashleyDH. Use of uorescent compounds in assessing bonded resin-based restorations: a literature review. J Dent 2006;34:623-34.
34. Bitter K, Paris S, Mueller J, Neumann K, Kielbassa AM. Cor-relation of scanning electron and confocal laser scanning micro-scopic analyses for visualization of dentin/adhesive interfaces inthe root canal. J Adhes Dent 2009;11:7-14.
35. Kytridou V, Gutmann JL, Nunn MH. Adaptation and sealabilityof two contemporary obturation techniques in the absence of thedentinal smear layer. Int Endod J 1999;32:464-74.
36. Shuping GB, Orstavik D, Sigurdsson A, Trope M. Reduction of intracanal bacteria using nickel-titanium rotary instrumentationand various medications. J Endod 2000;26:751-5.
37. Salzgeber RM, Brilliant JD. An in vivo evaluation of the pene-tration of an irrigating solution in root canals. J Endod 1977;3:394-8.
38. Jarrett IS, Marx D, Covey D, Karmazin M, Lavin M, Gound T.Percentage of canals lled in apical cross sectionsan in vitrostudy of seven obturation techniques. Int Endod J 2004;37:392-8.
39. Babb BR, Loushine RJ, Bryan TE, Ames JM, Causey MS, KimJ, et al. Bonding of self-adhesive (self-etching) root canal sealersto radicular dentin. J Endod 2009;35:578-82.
40. Resende LM, Rached-Junior FJA, Versiani MA, Souza-GabrielAE, Miranda CES, Silva-Souza, et al. A comparative study of physicochemical properties of AH Plus, Epiphany, and EpiphanySE root canal sealers. Int Endod J 2009;42:785-93.
41. Saleh IM, Ruyter IE, Haapasalo M, Orstavik D. Bacterial pene-tration along different root canal lling materials in the presenceor absence of smear layer. Int Endod J 2008;41:32-40.
Appendix
SUPPLEMENTARY DATASupplementary data associated with this article can
be found, in the online version, atdoi:10.1016/j.trip-leo.2009.07.016.
Reprint requests:
Ronald Ordinola-ZapataFaculdade de Odontologia de Bauru-USPAl. Octvio Pinheiro Brisolla, 9-75CEP 17012-901BauruSo [email protected]
OOOOE 968 Ordinola-Zapata et al. December 2009
http://dx.doi.org/10.1016/j.tripleo.2009.07.016http://dx.doi.org/10.1016/j.tripleo.2009.07.016http://dx.doi.org/10.1016/j.tripleo.2009.07.016mailto:[email protected]:[email protected]://dx.doi.org/10.1016/j.tripleo.2009.07.016http://dx.doi.org/10.1016/j.tripleo.2009.07.016