A Coordinated Approach To Child Health Center for Health Promotion and Prevention Research...
29
A Coordinated A Coordinated Approach Approach To Child Health To Child Health Center for Health Promotion and Prevention Research University of Texas-Houston School of Public Health
-
Upload
quentin-robbins -
Category
Documents
-
view
216 -
download
2
Transcript of A Coordinated Approach To Child Health Center for Health Promotion and Prevention Research...

A Coordinated Approach A Coordinated Approach To Child HealthTo Child Health
Center for Health Promotion and Prevention Research
University of Texas-HoustonSchool of Public Health

“Schools have more influence on the lives of youth than any other social institution except the family, and provide a setting in which, friendship networks develop, socialization occurs and norms that govern behavior are developed and reinforced.”
Healthy People 2010
http://web.health.gov/healthypeople
Why is this important?Why is this important?
Some facts about Some facts about the health status health status of children in the U.S.of children in the U.S.

ObesityObesity
Now affects 1 in 3 Americans; 63% of men & 55% of women have BMI > 25
Growing problem in youth; % overweight has tripled since 1970

Actual Causes of Death in the Actual Causes of Death in the United States, 1990United States, 1990
Source: McGinnis JM, Foege WH. JAMA 1993;270:2207-12.
400,000
300,000
100,000 90,000
30,000 20,000
0
100,000
200,000
300,000
400,000
500,000
Tobacco Diet/Activity Alcohol Microbialagents
Sexualbehavior
Illicit use ofdrugs

Percentage of U.S. Youth Who Percentage of U.S. Youth Who Were Overweight*, by AgeWere Overweight*, by Age
13%
10.7%
4.1%
14.0%
10.7%
4.6%
0
2
4
6
8
10
12
14
16
1963-70 1971-74 1976-80 1988-94 1999
Percent
Ages 6-11 Ages 12-17* >95th percentile for BMI by age and sex based on NHANES I reference data
Source: Troiano RP, Flegal KM. Pediatrics 1998;101(3):497-504. NHANES 1999, National Center for Health Statistics

Type 2 DiabetesType 2 Diabetes
Type 2 Diabetes was formerly known as “adult onset diabetes”, but there has been an increasing incidence of type 2 diabetes in youth. Rosenbloom et al., 1999
Approximately 85% of children diagnosed with type 2 diabetes are overweight or obese. American Diabetes Association
As the US population becomes increasingly overweight, researchers expect type 2 diabetes to appear more frequently in younger children. American Diabetes Association
Higher prevalence in Hispanics (1.9x) & African Americans (1.7x). NIDDK, 2000

Adverse CVD Risk Factor Adverse CVD Risk Factor Levels in ChildrenLevels in Children
Percent of children, aged 5-10, with 1 or more adverse CVD risk factor levels:
27.1%
Source: Freedman DS et al. Pediatrics 1999; 103:1175-82`
Percent of overweight children, aged 5-10, with 1 or more adverse CVD risk factor levels
60.6%

Physical InactivityPhysical Inactivity Increase in TV, Internet,
Computer Use Physical activity declines
steadily during adolescence.– MMWR, CDC Guidelines, 1997
Only 36% of kids in the US have daily PE class
Only ½ of all American youth regularly participate in vigorous physical activity
– Youth Risk Behavior Survey

Super Size It!!Super Size It!! Portion sizes are getting bigger and bigger! McDonald’s now has the “Mighty Kids” Happy
Meal– A regular size happy meal with a cheeseburger,
fries, and a coke would have 690 calories, 24 grams of fat, and 980 mg of sodium
– A mighty kids happy meal with a double cheeseburger, fries and a coke would have 820 calories, 34 grams of fat, and 1400 mg of sodium – remember, this is ONE MEAL!!

Soda ConsumptionSoda Consumption
Recently, researchers found that consumption of sugar-sweetened drinks is associated with increased obesity– For each additional serving of a
sugar-sweetened beverage, BMI and frequency of obesity increased Ludwig DS,
et al. Lancet 2001;357:505-08.

How can we combat this How can we combat this “obesity epidemic?”“obesity epidemic?”
We know the problem – what is the solution?
Prevention is the key!– Teaching our kids to eat nutritiously
and to get regular physical activity– Changing the school environment– Changing family norms– Coordinated School Health

What is CATCH?CATCH stands for Coordinated Approach To
Child Health (formerly known as the Child and Adolescent Trial for Cardiovascular Health)
It is part of a Coordinated School Health Program designed to prevent sedentary behavior, poor dietary choices, and tobacco use through changes at the elementary school level

Rationale
High prevalence of CVD and early onset among adults
Prevent risk factors for type 2 diabetes in children
Lifestyle related risk factors potentially modifiable:– Diet– Physical Activity– Smoking

Unique Features
First trial to integrate school, child & familyEthnically diverse populationFour geographic areas of the U.S.
– California– Louisiana– Minnesota– Texas
Large number of schools (N=96)

How Is CATCH a Coordinated School Health Program?

CATCH Components
Classroom Curriculum
Food Service
Physical Education
Family
It’s All About Healthier KidsIt’s All About Healthier KidsIt’s All About Healthier KidsIt’s All About Healthier Kids

Physical EducationStudents will be involved in
MVPA for 50% of class timeStudents are provided many
opportunities to participate and practice skills
Students enjoy physical activityStudents are encouraged to be
physically active outside of school

Classroom Curricula 3-5th grades (15-24 sessions/year) Objectives are for students to be able
to: – Identify, Practice, & Adopt healthy eating &
physical activity behaviors Focus on:
– Knowledge – Modeling by cartoon and peers– Skills training & Self-monitoring– Social skills (tobacco refusal)– Social norm setting

Family ProgramHomework done by child with
parent/grown-up assistance– Focus on skills development &
changing family norms – Complements the curricula
Family fun nights– health fairs with parent/child &
community participation

Eat Smart Program (School Food Service)
The vision for CATCH Eat Smart is to provide children with tasty
lower fat, saturated fat, and sodium school meals while
maintaining required levels of essential nutrients and student participation. Daily throughout
the school year.

Four Target Areas of Eat Smart
Menu Planning
Food Purchasing
Food Production
Promotion

Does CATCH Work?Reduced total fat and saturated fat content of school
lunches. Increased moderate-to-vigorous physical activity
(MVPA) during P.E. classes. Improved students’ self-reported eating and physical
activity behaviors.Effects persisted over three years without continued
intervention.
Luepker RV, et al (1996). JAMA, 275(10), 768-76.Nader PR, et al (1999). Arch Pediatr Adolesc Med, 153(7), 695-704.

Moderate to Vigorous PA(Percent of Lesson Time)
30
35
40
45
50
55
60
0 1 2 3 4 5 6
Intervention Control
Healthy People 2000 Objective 1.9
Semester
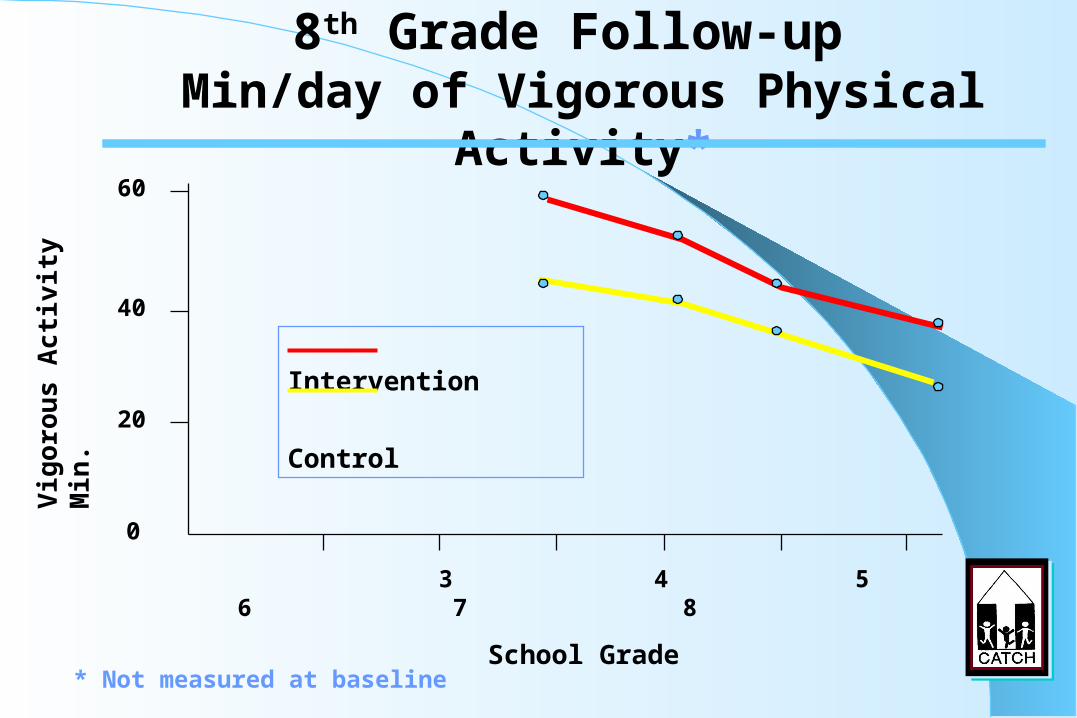
8th Grade Follow-up Min/day of Vigorous Physical Activity*
3 4 5 6 7 8
School Grade
Intervention
Control
60
40
20
0
Vig
oro
us A
cti
vit
y
Min
.
* Not measured at baseline

8th Grade Follow-up Dietary Fat Intake
3 4 5 6 7 8
School Grade
_______ Intervention
- - - - - - Control
34
32
30
0Die
tary
Fat,
% o
f En
erg
y

Advantages: Well studied, well documented. Approved by State Board of Education & TDH Minority Council as culturally compatible for all race/ethnic groups. Other schools are using it, endorsed by colleagues and professional associations (e.g. TMA, TAHPERD, PTA, etc.).
Compatibility: Most schools have PE and food service and health education requirements. CATCH meets CDC and State guidelines. Parents, teachers, and students like the program.
Complexity: IT’S NOT – CATCH modifies rather than replaces. Trialability: Program costs little to implement. CATCH staff conducts
training, which is supported by the TDH – Diabetes Program/Council. Observability: Visible school environmental changes. Principal
receives positive reinforcement, school health apparent. Assist in accountability.
Why are schools adopting CATCH?

Conclusions and Recommendations
CSHP enhance school connectedness, student health, staff and family wellness, and educational outcomes.
CATCH demonstrated that behaviors such as eating foods high in saturated fat and physical inactivity can be changed.
A coordinated school health program can be implemented in schools & it is possible to broadly disseminate a coordinated program.

Handy Resources
Contact the CATCH Office:
Peter Cribb, Program Director
phone (512) 346-6163 or fax (512) 346-6802
CATCH website:http://www.sph.uth.tmc.edu/chppr/catch