A child with multiple absent extraocular muscles
4
Short Reports A Child With Multiple Absent Extraocular Muscles Jane Hart, DBO, a Anthony G. Quinn, FRANZCO, FRCOphth, DCH, a and David Taylor, FRCS, FRCP, FRCOphth b We report on a child with congenital absence of multiple extraocular muscles, left ptosis, develop- mental delay, and weakness of the left arm. We discuss the potential management of this child, with presumed bilateral third nerve palsies, particularly with reference to strabismus surgery and anterior segment ischemia. CASE REPORT A male baby initially presented at 8 weeks old with a history of a bilateral, large angle (approximately 90 de- grees), constant exotropia since birth. His parents had noted that his eyes never moved from their divergent position and they were concerned about possible visual impairment. The pregnancy and full-term, vaginal deliv- ery were normal. An amniocentesis was performed during pregnancy, and chromosome analysis was normal. His father had a congenital color vision deficiency but there was no other family history of note. He presented to our department at 11½ months old and on examination his vision was 6/620 binocularly with Kee- ler preferential looking. His vision was difficult to assess, due to his age, and we were using forced choice preferen- tial viewing tests. We had to look for head movement as fixation instead of eye movement. At 16 months old, his uniocular visions were RE 6/76 and LE 6/96 with Cardiff cards at 50 cm. Pupillary reactions to a light were normal with no afferent pupil defect. He had a marked exotropia; both eyes were fixed in extreme abduction and would not adduct at all. There was fine manifest right beating and occasionally rotary nystagmus with both eyes open, which became worse in the left eye when fixing with the right eye. No ocular movements were demonstrable in either eye using active rotation of the head to induce vestibular system generated eye movements (“Doll’s head eye move- ments”). His pupils reacted normally to light. He had a left upper lid ptosis with a visible skin crease in both upper lids. The interpalpebral apertures measured 6 mm for the right and 4 mm for the left, although this did vary with his alertness (Figure 1). There was a right fixation preference with a large face turn to the left. This fixation preference may have been partly due to this inability to fix with the left eye unless the left lid was lifted. On cycloplegic refraction he was hypermetropic in both eyes (6.0D retinoscopy right and left). His right disk had a small cup and the left showed mild pallor and a central cup with an irregular outer border. The fundi were otherwise normal. The electroretinogram showed normal retinal responses. Independent flash visual evoked potentials (VEP) were of similar size with either eye, with a latency within normal limits for his age. Pattern reversal VEPs were degraded, broadened, and better seen with larger check sizes. The right pattern reversal VEP appeared to be better than the left and the VEP was reported as suggesting a poor-to-moderate level of vision. A magnetic resonance imaging scan showed a normal brain with some focal enlargement in the right temporal horn of the lateral ventricle anteriorly, which was thought to be of no significance. There was a lack of extraocular muscles with only the lateral rectus being present right and left (Figure 2). The lateral rectus muscles looked normal on the MRI scan. There was a structure that appears to be the superior ophthalmic vein on the right and left, but no superior rectus muscle (Figures 3 and 4). Surgical exploration of the left temporal sclera was performed to confirm the MRI scan. Following incision of the conjunctiva and Tenon’s capsule, no lateral rectus could be identified with exploration extending to 12 mm from the temporal limbus. No forced duction test had been performed at this time. The fact that there was no marked right ptosis and an upper lid skin crease suggests that some of the levator complex was present on the right. Although there was a upper skin crease on the left, ptosis was also present, suggesting a deficient levator complex. A carotid angiogram was performed to investigate the blood supply to the globe in the absence of extraocular muscles. It was found that the ophthalmic artery was unusual in that it appeared to run without major branches to the superior aspect of the eye and then bifurcate over the globe. From the a West of England Eye Unit, Royal Devon and Exeter NHS Healthcare Trust, Exeter, Devon EX2 5DW, United Kingdom; and b Department of Ophthalmology, Great Ormond Street Hospital for Children NHS Trust, London, WC1N 3JH, United Kingdom. Submitted December 16, 2003. Revision accepted October 21, 2004. Reprint requests: Miss Jane Hart, Orthoptic Department, West of England Eye Unit, RDE NHS Healthcare Trust, Exeter EX2 5DW, UK J AAPOS 2005;9:57-60. Copyright © 2005 by the American Association for Pediatric Ophthalmology and Strabismus. 1091-8531/2005/$35.00 0 doi:10.1016/j.jaapos.2004.10.008 Journal of AAPOS February 2005 57
Transcript of A child with multiple absent extraocular muscles

ares
Short Reports
A Child With Multiple Absent ExtraoculMuscl
Jane Hart, DBO,a Anthony G. Quinn, FRANZCO, FRCOphth, DCH,a and
David Taylor, FRCS, FRCP, FRCOphthbenceevelo
rm. Wild, wticulaanter
d wity 90entsivergle visal ded durmal.ut th
s oldith K
to asspreferemens old,h Care norxotroouldtingn, whthe riin eitestibu
ye mohad a
th upperfor the
with hisreferencereferencewith the
ic in bothdisk hada central
esponses.were of
n normalegraded,he right
e left andrate level
a normaltemporalthought
traocularright andd normalars to bet, but no
lera wascision ofal rectuso 12 mmtest had
is and ane levatorre was apresent,
igate thetraoculartery wasbranchescate over
lthcare Tmology, Gited King
nd Eye
almology
We report on a child with congenital absmultiple extraocular muscles, left ptosis, dmental delay, and weakness of the left adiscuss the potential management of this chpresumed bilateral third nerve palsies, parwith reference to strabismus surgery andsegment ischemia.
CASE REPORT
A male baby initially presented at 8 weeks olhistory of a bilateral, large angle (approximatelgrees), constant exotropia since birth. His parnoted that his eyes never moved from their dposition and they were concerned about possibimpairment. The pregnancy and full-term, vaginery were normal. An amniocentesis was performepregnancy, and chromosome analysis was norfather had a congenital color vision deficiency bwas no other family history of note.
He presented to our department at 11½ monthon examination his vision was 6/620 binocularly wler preferential looking. His vision was difficultdue to his age, and we were using forced choicetial viewing tests. We had to look for head movfixation instead of eye movement. At 16 monthuniocular visions were RE 6/76 and LE 6/96 witcards at 50 cm. Pupillary reactions to a light werwith no afferent pupil defect. He had a marked eboth eyes were fixed in extreme abduction and wadduct at all. There was fine manifest right beaoccasionally rotary nystagmus with both eyes opebecame worse in the left eye when fixing witheye. No ocular movements were demonstrableeye using active rotation of the head to induce vsystem generated eye movements (“Doll’s head ements”). His pupils reacted normally to light. He
From the aWest of England Eye Unit, Royal Devon and Exeter NHS HeaExeter, Devon EX2 5DW, United Kingdom; and bDepartment of OphthalOrmond Street Hospital for Children NHS Trust, London, WC1N 3JH, UnSubmitted December 16, 2003.Revision accepted October 21, 2004.Reprint requests: Miss Jane Hart, Orthoptic Department, West of EnglaRD�E NHS Healthcare Trust, Exeter EX2 5DW, UKJ AAPOS 2005;9:57-60.Copyright © 2005 by the American Association for Pediatric OphthStrabismus.1091-8531/2005/$35.00 � 0
doi:10.1016/j.jaapos.2004.10.008Journal of AAPOS
ofp-e
ithrlyior
h ade-hadentualliv-ingHisere
andee-ess,en-t ashisdiffmalpia;notandichghtherlarve-left
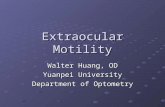
upper lid ptosis with a visible skin crease in bolids. The interpalpebral apertures measured 6 mmright and 4 mm for the left, although this did varyalertness (Figure 1). There was a right fixation pwith a large face turn to the left. This fixation pmay have been partly due to this inability to fixleft eye unless the left lid was lifted.
On cycloplegic refraction he was hypermetropeyes (�6.0D retinoscopy right and left). His righta small cup and the left showed mild pallor andcup with an irregular outer border.
The fundi were otherwise normal.The electroretinogram showed normal retinal r
Independent flash visual evoked potentials (VEP)similar size with either eye, with a latency withilimits for his age. Pattern reversal VEPs were dbroadened, and better seen with larger check sizes. Tpattern reversal VEP appeared to be better than ththe VEP was reported as suggesting a poor-to-modeof vision.
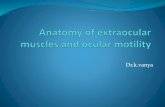
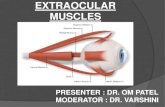
A magnetic resonance imaging scan showedbrain with some focal enlargement in the righthorn of the lateral ventricle anteriorly, which wasto be of no significance. There was a lack of exmuscles with only the lateral rectus being presentleft (Figure 2). The lateral rectus muscles lookeon the MRI scan. There was a structure that appethe superior ophthalmic vein on the right and lefsuperior rectus muscle (Figures 3 and 4).
Surgical exploration of the left temporal scperformed to confirm the MRI scan. Following inthe conjunctiva and Tenon’s capsule, no latercould be identified with exploration extending tfrom the temporal limbus. No forced ductionbeen performed at this time.
The fact that there was no marked right ptosupper lid skin crease suggests that some of thcomplex was present on the right. Although theupper skin crease on the left, ptosis was alsosuggesting a deficient levator complex.
A carotid angiogram was performed to investblood supply to the globe in the absence of exmuscles. It was found that the ophthalmic arunusual in that it appeared to run without majorto the superior aspect of the eye and then bifur
rust,reat
dom.
Unit,
and
the globe.
February 2005 57

obtailobe,ng chf strab
the rift eye
ime fr6/96
king teduressful blid po
Eightn forpperat tim
traocu
fascia, orglobe toAn “eye
lid ptoto see
lliseconds)ch eye and
uscles andnd left.
Journal of AAPOSVolume 9 Number 1 February 200558 Hart, Quinn, and Taylor
A superselective angiogram was suggested tomore detailed view of the blood supply to the gbecause the risks of this procedure on such a youare significant, the procedure, and the question omus surgery, has been deferred.
He had occlusion with an adhesive patch toeye, for 1 hour daily with his parents lifting the leWith occlusion, the right vision improved over t6/76 to 6/38, and the left vision improved from6/76 testing with a forced choice preferential loo
He had a posterior approach levator tuck procthe left ptosis. The operation was initially succefollowing a wound infection postoperatively, thetion returned to its preoperative position.months later he had an anterior levator resectioresidual left ptosis, which improved the left uposition so that he now fixates with the left eyeHe still prefers to fix with the right eye.
DISCUSSION
Correcting strabismus which is due to a lack of ex
FIG 1. Marked divergence of either eye and left upperHead posture not seen because patient’s head is heldface.
muscles presents a major challenge to the surgeon. Tiss
n abutildis-
ghtlid.omto
est.forut,si-
eenthelides.
lar
such as palmaris longus, fascia lata, temporalisperiorbital flap have all been used to anchor thethe periosteum but produce a strabismus fixus.1,2
sis.full
FIG 2. Axial view MRI scan (inversion recovery of 145 mishowing what appears to be a lateral rectus muscle in eadivergent position of eyes.
FIG 3. T1 Coronal view MRI scan showing lateral rectus mwhat appears to be the superior ophthalmic vein, right a
ues muscle prosthesis” has also been reported as being used for

mightctus
ectus,a “simplasialy toimpr
thus mropia.ory h
s munt bloctus mgery
ot alw
scopyr, specwithaxis.the ey
eral c
h cranialtation, atveloping.her mus-of singleof more
n cranio-pupillarye nucleus
and lacker withinisorders,al nervesorted inatholog-h cranial
tion syn-d monthce of ex-rtunatelyrves.
or perform-vans of the
ation.
rgical cor-phthalmol
extraocular;26:80.s. J Pediatr
ctus muscle0;4:246-7.strabismus
56-7.of anterior
copic tech-
f extensive
rgery. Arch
f the ante-phthalmol-
teral rectus
scle. A case1997;104:
absence of;14:355-8.uscle. Am J
ence of theimaging. J
usclesnd lef
Journal of AAPOSVolume 9 Number 1 February 2005 Hart, Quinn, and Taylor 59
absent muscles.3 A further possibility describedto move the lateral rectus under the superior reinsert it near the upper border of the medial rhangback sutures.4 This child appears to havelated” strabismus fixus due to the severe hypoextraocular muscles and surgery would be unlikeprove his ability to move his eyes. Surgery mayhis field of vision temporally since the lateral canobstruct this at present due to the large exotaddition, surgery may improve his compensatposture.
The anterior ciliary vessel of the lateral rectumay contribute significantly to the anterior segmesupply, and recessing or transposing the lateral reput this blood supply at risk. Vessel-sparing surbeen advocated in similar circumstances but is nsuccessful at maintaining perfusion.5-9
He has significant hypermetropia, with a retino�6.0, which puts him at risk of amblyopia. So facles have not been prescribed due to difficultiessitioning the lenses in relation to the visualspeculated that due to the extreme abduction ofcontact lenses would probably decenter.
This patient’s problems may represent bilat
FIG 4. T1 Coronal view MRI scan showing lateral rectus mwhat appears to be the superior ophthalmic vein, right a
genital 3rd nerve palsy with muscle hypoplasia or apla
beandonu-of
im-ove
ayIn
ead
scleoday
hasays
ofta-
po-Wees,
on-
The development of the third, fourth, and sixtnerves occur at around the 4th to 8th week of gesthe same time as the extraocular muscles are deThe SR is the first to appear followed by the otcles. There have been many previous reportsabsent extraocular muscles.10-18 However reportsthan one muscle absent are mainly mentioned ifacial dysostoses.19-21 The presence of normalfunction implies there is at least some third nervfunction present.
Another possible explanation is that the ptosisof extraocular muscles represents another disordthe spectrum of congenital cranial dysinervation dwith deficient development of the affected cranior muscles in the embryo.22 This has been reprelation to Duane’s retraction syndrome where pical reports have confirmed no trace of the sixtnerve along its route.23
Although this child does not have Duane’s retracdrome, a similar teratogenic event during the seconof gestation may have occurred causing the absentraocular muscles and possible lack of nerves. Unfowe are unable to confirm the absence of cranial ne
The authors thank Dr Dorothy Thompson and colleagues fing the neurophysiological studies, and V.T. Thaller and N. ERoyal Eye Infirmary, Plymouth for additional clinical inform
References1. Salazar-Leon JA, Ramirez-Ortiz MA, Vargas M. The su
rection of paralytic strabismus using fascia lata. J Pediatr OStrabismus 1998;35:27-32.
2. Collins CC, Jampolsky A, Scott AB. Artificial muscle forimplantation (abstract). Invest Ophthalmol Vis Sci 1985
3. Scott AB, Miller JM, Collins CC. Eye muscle prosthesiOphthalmol Strabismus 1992;29:216-8.
4. Morad Y, Nemet P. Medial transposition of the lateral rein combined third and fourth nerve palsy. J AAPOS 200
5. Murdock TJ, Mills MD. Anterior segment ischemia aftersurgery with microvascular dissection. J AAPOS 2000;4:
6. Freeman HL, Waltman DD, Patterson JH. Preservationciliary vessels during strabismus surgery: a non-microsnique. J Pediatr Ophthalmol Strabismus 1992;29:38-43.
7. Girand LJ, Beltranena F. Early and late complications omuscle surgery. Arch Ophthalmol 1960;64:576-84.
8. Vila-Coro AA. Vascular microdissection in strabismus suOphthalmol 1990;108:1034-6.
9. McKeown CA, Lambert HM, Shore JW. Preservation orior ciliary vessels during extraocular muscle surgery. Oogy 1989;96:498-505.
10. Sandall GS, Morrison JW Jr. Congenital absence of lamuscle. J Pediatr Ophthalmol Strabismus 1979;16:35-9.
11. Taylor RH, Kraft SP. Aplasia of the inferior rectus mureport and review of the literature. Ophthalmology3;415-8.
12. Ingham PN, McGovern ST, Crompton JL. Congenitalthe inferior rectus muscle. Aust NZ J Ophthalmol 1986
13. Munoz M. Congenital absence of the inferior rectus mOphthalmol 1996;121:327-9.
14. Chan TK, Demer JL. Clinical features of congenital abssuperior oblique muscle as demonstrated by orbital
andt.
sia. AAPOS 1999;3:143-50.

ior obl;16:375erior re7;34:38
of a la-60.ansposies of ab7:4287rior obl
lar muscles
chaffer DB.craniofacial
ital cranialDisord in
ral DuanesArch Oph-
Journal of AAPOSVolume 9 Number 1 February 200560 Hart, Quinn, and Taylor
15. Pinchoff BS, Sandall G. Congenital absence of the supertendon in craniofacial dysostisis. Ophthalmol Surg 1985
16. Lin P-Y, Yen M-Y. Congenital absence of bilateral infmuscles: a case report. J Pediatr Ophthalmol Strabismus 199
17. Zoller CC, Graf M, Kaufmann H. Unilateral aplasiarectus muscle. Klin Monatsbl Augenheilkd 2001;218:155
18. Gamio S, Tartara A, Zelter M. Recession and anterior trof the inferior oblique muscle (RATIO) to treat three casinferior rectus muscle. Binocul Vis Strabismus Q 2002;1
19. Drummond GT, Keech RV. Absent and anomalous supe
and superior rectus muscles. Can J Ophthalmol 1989;24:27ique-7.ctus2-4.
teral
tionsent-95.ique
20. Greenberg MF, Pollard ZF. Absence of multiple extraocuin craniosynostosis. J AAPOS 1998;2:307-9.
21. Diamond GR, Katowitz JA, Whitaker LA, Quinn GE, SVariations in extraocular muscle number and structure indysostosis. Am J Ophthalmol 1980;90:416-8.
22. Gutowski NJ, Bosley TM, Engle EC. The congendysinnervation disorders. (CCDDs). Neuromusculpress.
23. Hotchkiss MG, Miller NR, Clark AW, Green WR. Bilateretraction syndrome. A clinical–pathological case report.
5-9. thalmol 1980;98:870-4.
An Eye on the Arts – The Arts on the Eye
You say you haven’t got the expertise for art and are just a writer, saying whatyou want to say and whenever you want to.
“But writing is also a form of art.”You insist that writing is a technical skill.“It just requires learning the technique, like you for example, you’ve learnt
how to operate with a scalpel. I don’t know if you’re a surgeon or a physicianbut that’s not important. As long as you acquire the technique anyone can writejust like anyone can learn how to use a scalpel.”
She laughs.You go on to say you don’t believe that art is sacrosanct, art is just a way of
life. People have different ways of life, art can’t represent everything.“You’re very intelligent,” she says.“You’re not exactly stupid yourself,” you say.“But some people are stupid.”“Who?”“Artists. They only perceive with their eyes.”“Artists have artists’ modes of perception, they rely more on visual percep-
tion than writers.”“Can visual perception allow one to understand a person’s intrinsic value?”“I don’t think so, but the crux of the matter is what is value? This differs
according to the individual, people have their own ways of looking at this. It isonly for those with similar values that different values have any meaning. Iwon’t be ingratiating and say that you are beautiful and I don’t know whetheryou are all beatiful inside, but I can say that it is enjoyable talking with you.Don’t people exist in order to have some pleasure? Only fools go out lookingfor unhappiness.”
“I also feel happy when I am with you.”—Gao Xingjian (from Soul Mountain)