A 1 ARIFLO ® (cilomilast) Tablets, 15 mg September 5, 2003 NDA 21-573 Pulmonary - Allergy Drugs...
120
A A ARIFLO ARIFLO ® ® (cilomilast) Tablets, (cilomilast) Tablets, 15 mg 15 mg September 5, 2003 September 5, 2003 NDA 21-573 NDA 21-573 Pulmonary - Allergy Drugs Pulmonary - Allergy Drugs Advisory Committee Meeting Advisory Committee Meeting
-
Upload
stewart-lewis -
Category
Documents
-
view
216 -
download
0
Transcript of A 1 ARIFLO ® (cilomilast) Tablets, 15 mg September 5, 2003 NDA 21-573 Pulmonary - Allergy Drugs...

A A 11
ARIFLOARIFLO®® (cilomilast) Tablets, 15 mg (cilomilast) Tablets, 15 mg
September 5, 2003September 5, 2003
NDA 21-573NDA 21-573
Pulmonary - Allergy Drugs Pulmonary - Allergy Drugs Advisory Committee MeetingAdvisory Committee Meeting

A A 22
ARIFLOARIFLO®® (cilomilast) (cilomilast)Tablets, 15 mgTablets, 15 mg
David Wheadon, M.D.David Wheadon, M.D.Senior Vice President Senior Vice President
Regulatory Affairs Regulatory Affairs GlaxoSmithKlineGlaxoSmithKline

A A 33
Chronic ObstructiveChronic ObstructivePulmonary DiseasePulmonary Disease
EmphysemaEmphysema Chronic BronchitisChronic Bronchitis

A A 44
Impact of COPD in the USImpact of COPD in the US
• Affects an estimated 24 million AmericansAffects an estimated 24 million Americans11
• Annual cost $32.1 billion in 2002Annual cost $32.1 billion in 200222
– $18 billion in direct healthcare costs$18 billion in direct healthcare costs– $14.1 billion in indirect morbidity and mortality $14.1 billion in indirect morbidity and mortality
costscosts
• The fourth leading cause of The fourth leading cause of deathdeath33
– 123,974 deaths in 2001123,974 deaths in 2001
1. Mannino DM, 1. Mannino DM, et al.et al. MMWRMMWR 2002; 51(No. SS06):1-16. 2002; 51(No. SS06):1-16.2. NHLBI, 2. NHLBI, Morbidity and Mortality Chartbook on Cardiovascular, Lung and Blood Diseases, Morbidity and Mortality Chartbook on Cardiovascular, Lung and Blood Diseases,
2002.2002. 3. CDC, 3. CDC, National Vital Statistics ReportsNational Vital Statistics Reports, Vol. 51, No. 5, March 14, 2003., Vol. 51, No. 5, March 14, 2003.

A A 55
Mannino DM, Mannino DM, et al.et al. MMWR, MMWR, 2002; 51(SS06):1-16. 2002; 51(SS06):1-16. Pastor PN, Pastor PN, et al.et al. National Center for Health StatisticsNational Center for Health Statistics, 2002, 2002
COPD Mortality is IncreasingCOPD Mortality is Increasing
-48.0%
-19.9%
-6.9% -6.9%
25.5%
-50
-40
-30
-20
-10
0
10
20
30
40
50
Per
cen
t ch
ang
e
HIV
CAD
Stroke Cancer
COPD
Percent change in age-adjusted death rates in theUS over 10 years (1990-2000)

A A 66
Prognosis in Chronic Prognosis in Chronic Obstructive Pulmonary DiseaseObstructive Pulmonary Disease
% S
urv
ival
% S
urv
ival
YearsYears
NormalsNormals>> 50% Predicted 50% Predicted40-49% Predicted40-49% Predicted30-39% Predicted30-39% Predicted<30% Predicted<30% Predicted
100100
9090
8080
7070
6060
00 11 22 33
FEVFEV11
Anthonisen N, Anthonisen N, Am Rev Respir DisAm Rev Respir Dis 1986; 133(1):14-20 1986; 133(1):14-20

A A 77
Unmet Medical NeedUnmet Medical Need
• Limited treatment optionsLimited treatment options
• Only bronchodilators are approved for Only bronchodilators are approved for COPD COPD – Address only bronchoconstriction Address only bronchoconstriction
• Smoking cessation is the only Smoking cessation is the only intervention known to reduce the rate of intervention known to reduce the rate of decline of FEVdecline of FEV11

A A 88
COPD is a Complex DiseaseCOPD is a Complex Disease
Progressive Loss of Lung Progressive Loss of Lung FunctionFunction
Reduced Quality of LifeReduced Quality of LifeExacerbationsExacerbations
MortalityMortality
Broncho-Broncho-
constrictionconstriction
InflammationInflammation
StructuralStructural
ChangesChangesAirflow Airflow
Limitation & Limitation &
HyperinflationHyperinflation

A A 99
Ariflo:Ariflo:Second Generation PDE4 InhibitorSecond Generation PDE4 Inhibitor• Highly Selective PDE4 Highly Selective PDE4
inhibitorinhibitor
– 100% bioavailability 100% bioavailability – Low plasma variabilityLow plasma variability– Low potential for drug Low potential for drug
interactionsinteractions– Improved safety profileImproved safety profile
• Tablet administered orally Tablet administered orally twice a day twice a day
• Ariflo is an important new Ariflo is an important new option for the treatment of option for the treatment of COPDCOPD
OO
CNCN
COOHCOOH
HHHH33COCO

A A 1010
Theophylline:Theophylline:Non-Selective PDE InhibitorNon-Selective PDE Inhibitor
• Pharmacological activityPharmacological activity– MethylxanthineMethylxanthine– Non-selective PDE inhibitorNon-selective PDE inhibitor– Adverse effects may be related to PDE3 inhibitionAdverse effects may be related to PDE3 inhibition– Effects on other pharmacological pathwaysEffects on other pharmacological pathways
(i.e., adenosine receptor antagonism)(i.e., adenosine receptor antagonism)
• Unpredictable pharmacokinetic profileUnpredictable pharmacokinetic profile– Drug and food interactions Drug and food interactions – Wide blood level variation (i.e., elderly, smokers)Wide blood level variation (i.e., elderly, smokers)– Need for blood level monitoringNeed for blood level monitoring

A A 1111
Phase III Development ProgramPhase III Development Program
Study/RegionStudy/Region DurationDuration
2 Pivotal NA2 Pivotal NA 24 weeks24 weeks
2 Pivotal EU2 Pivotal EU 24 weeks24 weeks
1 Cardiovascular Safety NA1 Cardiovascular Safety NA 12 weeks12 weeks
1 Induced sputum NA1 Induced sputum NA 12 weeks12 weeks
1 Lung biopsy EU1 Lung biopsy EU 12 weeks12 weeks
1 Lung volume NA1 Lung volume NA 12 weeks12 weeks
1 Open-Label Extension NA1 Open-Label Extension NA 12-36 months12-36 months
1 Open-Label Extension EU1 Open-Label Extension EU 12-36 months12-36 months
Exposure to Ariflo from above studies represents nearly 3,000 patient yearsExposure to Ariflo from above studies represents nearly 3,000 patient years

A A 1212
Poorly Reversible Population Poorly Reversible Population Studied in Ariflo Clinical StudiesStudied in Ariflo Clinical Studies
AsthmaAsthma COPDCOPD
Fully Reversible Fully Reversible Lung FunctionLung Function
Fixed Fixed Airways Airways DiseaseDisease
Reversibility

A A 1313
Proposed IndicationProposed Indication
ARIFLOARIFLO®® is indicated for the maintenance of is indicated for the maintenance of lung function (FEVlung function (FEV11) in patients with chronic ) in patients with chronic
obstructive pulmonary disease (COPD) who obstructive pulmonary disease (COPD) who are poorly responsive to albuterol (increase are poorly responsive to albuterol (increase in FEVin FEV11 of of <<15% or 15% or << 200 mL). 200 mL).

A A 1414
Order of GSK PresentationOrder of GSK Presentation
• Rationale for the Use Rationale for the Use of Ariflo in COPDof Ariflo in COPD
–Dr. Katharine KnobilDr. Katharine Knobil
Order of GSK PresentationOrder of GSK Presentation
–Dr. David WheadonDr. David Wheadon• Conclusion and Q&AConclusion and Q&A
–Dr. Katharine KnobilDr. Katharine Knobil• Efficacy Data from Efficacy Data from Ariflo Clinical ProgramAriflo Clinical Program
–Dr. Kathy RickardDr. Kathy Rickard• Safety of ArifloSafety of Ariflo
–Dr. Frank SciurbaDr. Frank Sciurba• Assessment of Outcome in Assessment of Outcome in COPDCOPD


A A 1616
Rationale for theRationale for theUse of Ariflo in COPDUse of Ariflo in COPD
Katharine Knobil, M.D.Katharine Knobil, M.D.Senior Director Senior Director
Respiratory Clinical Development and Medical AffairsRespiratory Clinical Development and Medical Affairs
GlaxoSmithKlineGlaxoSmithKline

A A 1717
COPD is a Complex DiseaseCOPD is a Complex Disease
Progressive Loss of Lung Progressive Loss of Lung FunctionFunction
Reduced Quality of LifeReduced Quality of LifeExacerbationsExacerbations
MortalityMortality
Broncho-Broncho-
constrictionconstriction
InflammationInflammation
StructuralStructural
ChangesChangesAirflow Airflow
Limitation & Limitation &
HyperinflationHyperinflation

A A 1818
Inflammatory Cells in COPDInflammatory Cells in COPD
Adapted from Retamales I, Adapted from Retamales I, et al.et al. Am J Respir Crit Care MedAm J Respir Crit Care Med 2001; 164:469-473. 2001; 164:469-473.
Calhoun WJ, et al. Calhoun WJ, et al. Am J Respir Crit Care MedAm J Respir Crit Care Med 2001; 165:730b-731b. 2001; 165:730b-731b.
Cel
ls i
n t
issu
e x
10C
ells
in
tis
sue
x 10
88
**
*
**
*p<0.01 vs control and mild*p<0.01 vs control and mild

A A 1919
Airway CD8+ T-cellAirway CD8+ T-cellCorrelation with Airflow LimitationCorrelation with Airflow Limitation
Adapted from Saetta M, Adapted from Saetta M, et al. Am J Respir Crit Care Medet al. Am J Respir Crit Care Med 1998; 157:822-826 1998; 157:822-826
CD
8+
(c
ells
/mm
CD
8+
(c
ells
/mm
22 ))
FEVFEV11 (% predicted) (% predicted)
10001000
0000 1101105050 7070 9090
400400
200200
800800
600600
6060 8080 100100
pp= 0.01= 0.01rho = -0.63rho = -0.63
A A 2020
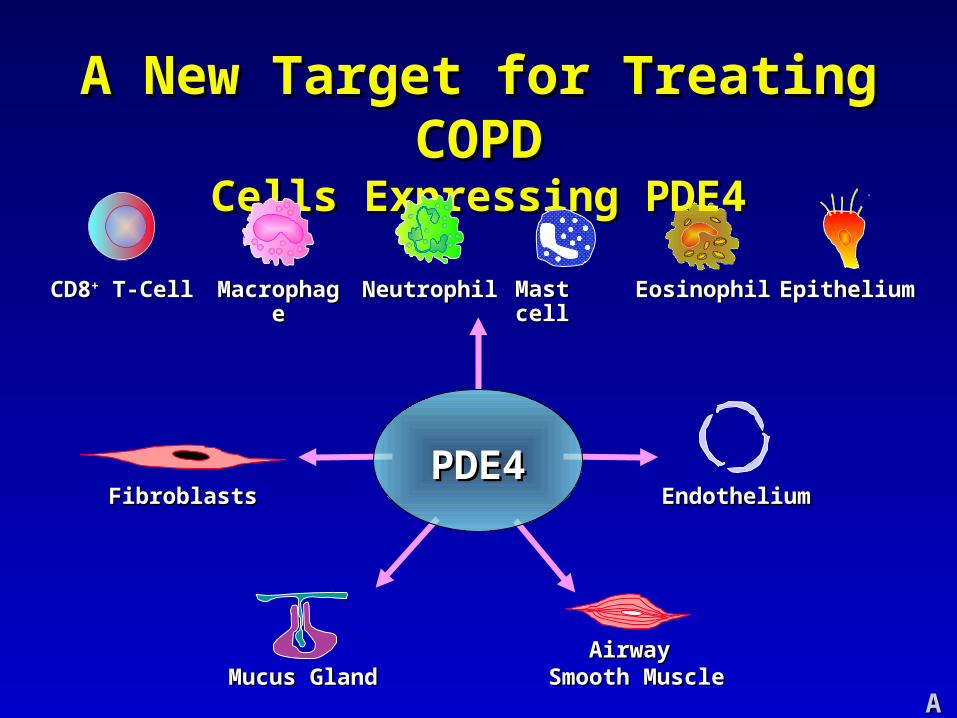
A New Target for Treating COPDA New Target for Treating COPDCells Expressing PDE4Cells Expressing PDE4
NeutrophilNeutrophilMacrophageMacrophageCD8CD8++ T-Cell T-Cell EosinophilEosinophil EpitheliumEpitheliumMast cellMast cell
Mucus GlandMucus GlandAirwayAirway
Smooth Muscle Smooth Muscle
EndotheliumEndotheliumFibroblastsFibroblastsPDE4PDE4

A A 2121
Cyclic AMPCyclic AMPATPATP
Adenyl cyclaseAdenyl cyclase
Inhibition of Inhibition of Fibrosis/RemodelingFibrosis/Remodeling
Epithelial CellsEpithelial CellsFibroblastsFibroblasts
Smooth Muscle Smooth Muscle RelaxationRelaxation
PDE4PDE4
5'-AMP5'-AMP
Anti-InflammatoryAnti-InflammatoryCD8+ T cellsCD8+ T cellsMacrophagesMacrophagesNeutrophilsNeutrophils
ArifloAriflo
A Novel Approach to Treating COPD: A Novel Approach to Treating COPD: PDE4 InhibitorsPDE4 Inhibitors

A A 2222
Cilomilast Attenuates Fibroblast Cilomilast Attenuates Fibroblast ActivityActivity
In vitroIn vitro, cilomilast inhibited:, cilomilast inhibited:
• Release of MMP-1 and Release of MMP-1 and MMP-9 from fibroblastsMMP-9 from fibroblasts
• Activation of MMP-1 and Activation of MMP-1 and MMP-9 MMP-9
• Degradation of collagen Degradation of collagen by fibroblastsby fibroblasts
• Suggests potential of Suggests potential of PDE4 inhibitors to affect PDE4 inhibitors to affect remodelingremodeling
Kohyama T, Kohyama T, et al. Am J Respir Cell Mol Biolet al. Am J Respir Cell Mol Biol 2002; 27:487-494. 2002; 27:487-494.
Alveolar Wall DestructionAlveolar Wall Destruction

A A 2323
Cilomilast Attenuates Release of Cilomilast Attenuates Release of Chemoattractants for Human NeutrophilsChemoattractants for Human Neutrophils
Adapted from Profita M, Adapted from Profita M, et al.et al. ThoraxThorax 2003; 58:573-579 2003; 58:573-579
Bronchial Epithelial Cells Sputum Cells
Neu
tro
ph
ils p
er h
igh
po
we
r fi
eld
Neu
tro
ph
ils p
er h
igh
po
we
r fi
eld 400400
00BaselineBaseline CilomilastCilomilast
(1 (1 M)M)
100100
300300
200200
400400
00BaselineBaseline CilomilastCilomilast
(1 (1 M)M)
100100
300300
200200
P<0.006P<0.008
Cells obtained from patients with COPD by bronchoscopy and sputum inductionCells obtained from patients with COPD by bronchoscopy and sputum induction

A A 2424
Study 076: Ariflo Decreased Study 076: Ariflo Decreased Macrophages in Bronchial BiopsiesMacrophages in Bronchial Biopsies
-75
-50
-25
0
25
50
Ch
an
ge
in s
ub
-ep
ith
elia
l m
ac
rop
ha
ge
s/a
rea
tis
su
e
Placebo Ariflo
Difference from placebo: p=0.005

A A 2525
Study 076: Ariflo Decreased CD-8+ Study 076: Ariflo Decreased CD-8+ Lymphocytes in Bronchial BiopsiesLymphocytes in Bronchial Biopsies
-250
-200
-150
-100
-50
0
50
100
150
Ch
an
ge
in s
ub
-ep
ith
elia
l CD
8+
ly
mp
ho
cy
tes
/are
a t
iss
ue
Placebo Ariflo
Difference from placebo: p=0.055

A A 2626
BronchoconstrictionBronchoconstriction
Mediator Release From Pro-inflammatory CellsMediator Release From Pro-inflammatory Cells Influx of Inflammatory CellsInflux of Inflammatory Cells
Edema and AdhesionEdema and Adhesion
Mucus HypersecretionMucus Hypersecretion
Mucus GlandMucus GlandAirwayAirway
Smooth Muscle Smooth Muscle
EndotheliumEndothelium
Airway RemodellingAirway Remodelling
FibroblastsFibroblastsARIFLOARIFLO
NeutrophilNeutrophilMacrophageMacrophageCD8CD8++ T-Cell T-Cell EosinophilEosinophil EpitheliumEpitheliumMast cellMast cell
Potential Therapeutic Benefits of ArifloPotential Therapeutic Benefits of Ariflo


A A 2828
Ariflo Clinical Ariflo Clinical Development ProgramDevelopment Program
Katharine Knobil, M.DKatharine Knobil, M.D..
Senior Director Senior Director Respiratory Clinical Development and Medical AffairsRespiratory Clinical Development and Medical Affairs
GlaxoSmithKlineGlaxoSmithKline
Efficacy DataEfficacy Data

A A 2929
Phase III Development Plan Phase III Development Plan Pivotal StudiesPivotal Studies
StudyStudy Abbreviated TitleAbbreviated Title LocLoc PatientsPatients Study DurationStudy Duration
039039 Pivotal Phase IIIPivotal Phase III NANA 647647 24 weeks24 weeks
156156 Pivotal Phase III Pivotal Phase III NANA 825825 24 weeks24 weeks
091091 Pivotal Phase III Pivotal Phase III EUEU 711711 24 weeks24 weeks
042042 Pivotal Phase III Pivotal Phase III EUEU 700700 24 weeks24 weeks

A A 3030
Phase III Development Plan Phase III Development Plan Supporting StudiesSupporting Studies
StudyStudy Abbreviated TitleAbbreviated Title LocLoc PatientsPatients Study DurationStudy Duration
110110 Induced Sputum Induced Sputum NANA 6565 12 weeks12 weeks
076076 Lung Biopsy Lung Biopsy EUEU 5959 12 weeks12 weeks
168168 Cardiovascular Safety Cardiovascular Safety NANA 282282 12 weeks12 weeks
041041 Long-term Safety Long-term Safety NANA 355355 up to 3 yearsup to 3 years
040040 Long-term Safety Long-term Safety EUEU 723723 up to 3 yearsup to 3 years
111111 Static Lung Volumes Static Lung Volumes NANA 156156 12 weeks12 weeks

A A 3131
Study Design: Pivotal StudiesStudy Design: Pivotal Studies
4 weeks4 weeks 24 weeks24 weeks
Ariflo 15mg BID Ariflo 15mg BID
PRNPRNalbuterolalbuterol Placebo BID Placebo BID
PlaceboPlaceboRun-inRun-in

A A 3232
Key Inclusion CriteriaKey Inclusion Criteria
• COPD diagnosisCOPD diagnosis
• 40-80 years old40-80 years old
• >> 10 pack year history of smoking 10 pack year history of smoking
• Symptoms*Symptoms*
*except NA Study 156*except NA Study 156

A A 3333
Key Inclusion CriteriaKey Inclusion Criteria
Lung Function Lung Function
• FEVFEV11 (post albuterol): 30 - 70% predicted (post albuterol): 30 - 70% predicted
• FEVFEV11/FVC (pre albuterol): /FVC (pre albuterol): <<70% predicted70% predicted
• Poorly reversible to albuterolPoorly reversible to albuterol– << 15% or 15% or << 200ml 200ml

A A 3434
Response to Albuterol in COPD Response to Albuterol in COPD Clinical Development ProgramsClinical Development Programs
1. COMBIVENT Inhalation Aerosol Study Group, 1. COMBIVENT Inhalation Aerosol Study Group, ChestChest 1994; 105:1411-1419. 2. Mahler D, 1994; 105:1411-1419. 2. Mahler D, et al. Chestet al. Chest 1999; 115:957-965. 3. Rennard S, 1999; 115:957-965. 3. Rennard S, et al. Am J Respir Crit Care Medet al. Am J Respir Crit Care Med 2001; 163:1087-1092. 4. Mahler D, 2001; 163:1087-1092. 4. Mahler D, et al. Am J Respir Crit Care Medet al. Am J Respir Crit Care Med 2002; 166:1084-1091. 5. Hanania NA, 2002; 166:1084-1091. 5. Hanania NA, et al. Chestet al. Chest 2003 2003 In Press.In Press.
11 2,3,4,52,3,4,5 4,54,5

A A 3535
Key Exclusion CriteriaKey Exclusion Criteria
• Clinical diagnosis of asthmaClinical diagnosis of asthma
• FEVFEV11 variability >20% from Screening to variability >20% from Screening to
BaselineBaseline
• Exacerbation or oral steroid Exacerbation or oral steroid administration during run-in periodadministration during run-in period

A A 3636
Efficacy AssessmentsEfficacy AssessmentsCo-Primary EndpointsCo-Primary Endpoints
• Change from baseline in FEVChange from baseline in FEV1 1 – Measured in AM prior to the next dose Measured in AM prior to the next dose
(trough)(trough)
• Change from baseline in total score of Change from baseline in total score of the St. George’s Respiratory the St. George’s Respiratory Questionnaire (SGRQ) Questionnaire (SGRQ) – A health-related quality of life instrumentA health-related quality of life instrument

A A 3737
Efficacy AssessmentsEfficacy Assessments Secondary EndpointsSecondary Endpoints
• Change from baseline in FVCChange from baseline in FVC
• COPD ExacerbationsCOPD Exacerbations
• Post exercise breathlessnessPost exercise breathlessness(Borg scale)(Borg scale)
• Summary symptom score Summary symptom score – Not collected in NA study 156Not collected in NA study 156
• 6-Minute walk6-Minute walk

A A 3838
Baseline CharacteristicsBaseline Characteristics
NANA EU EU
039 039 156 156 042042 091091n=647n=647 n=825n=825 n=700n=700 n=711n=711
AgeAge 65.365.3 64.564.5 64.664.6 62.862.8
Female (%)Female (%) 3838 4141 2020 1414
Race % (W/B)Race % (W/B) 93/393/3 93/693/6 99/099/0 98/098/0
Active smokers (%)Active smokers (%) 4545 4646 4343 3838
FEVFEV11 (% Predicted) (% Predicted) 49.749.7 50.250.2 49.049.0 50.350.3
2 reversibility (% 2 reversibility (% )) 7.37.3 8.68.6 5.15.1 5.05.0
DLCO (% Predicted)DLCO (% Predicted) 58.558.5 55.355.3 70.870.8 70.070.0
Chronic Bronchitis (%)Chronic Bronchitis (%) 61.561.5 37.537.5 80.180.1 89.689.6

A A 3939
Mea
n C
han
ge
fro
m B
asel
ine
Mea
n C
han
ge
fro
m B
asel
ine
in T
rou
gh
FE
Vin
Tro
ug
h F
EV
11 (L
) (
L)
WeekWeek
-0.1
-0.08
-0.06
-0.04
-0.02
0
0.02
0.04
0.06
0.08
0.1
0 2 4 8 12 16 20 24 AVG24
WKS
EP
Placebo
Ariflo
P<0.001P=0.002
Ariflo Maintains FEVAriflo Maintains FEV11
NA Study 039NA Study 039

A A 4040
P<0.001P<0.001
Ariflo: Consistent Treatment EffectAriflo: Consistent Treatment EffectM
ea
n C
ha
ng
e f
rom
Ba
se
lin
e i
n
Tro
ug
h F
EV
Me
an
Ch
an
ge
fro
m B
as
eli
ne
in
T
rou
gh
FE
V11
(L)
(L
)
P=0.002P=0.002
NA Study 039NA Study 039
-0.1-0.1
-0.08-0.08
-0.06-0.06
-0.04-0.04
-0.02-0.02
00
0.020.02
0.040.04
0.060.06
0.080.08
0.10.1
00 22 44 88 1212 1616 2020 2424 AVGAVG2424
WKSWKS
EPEP
PlaceboPlaceboArifloAriflo
P=0.013P=0.013P=0.024P=0.024
NA Study 156NA Study 156
-0.1-0.1
-0.08-0.08
-0.06-0.06
-0.04-0.04
-0.02-0.02
00
0.020.02
0.040.04
0.060.06
0.080.08
0.10.1
00 22 44 88 1212 1616 2020 2424 AVGAVG2424
WKSWKS
EPEP
PlaceboPlaceboArifloAriflo
P=0.146P=0.146
WeekWeek
P=0.055P=0.055
EU Study 091EU Study 091
Me
an
Ch
an
ge
fro
m B
as
eli
ne
in
T
rou
gh
FE
VM
ea
n C
ha
ng
e f
rom
Ba
se
lin
e i
n
Tro
ug
h F
EV
11 (L
) (
L)
-0.1-0.1
-0.08-0.08
-0.06-0.06
-0.04-0.04
-0.02-0.02
00
0.020.02
0.040.04
0.060.06
0.080.08
0.10.1
00 22 44 88 1212 1616 2020 2424 AVGAVG2424
WKSWKS
EPEP
PlaceboPlacebo
WeekWeek
P=0.050P=0.050
P=0.044P=0.044
EU Study 042EU Study 042
-0.1-0.1
-0.08-0.08
-0.06-0.06
-0.04-0.04
-0.02-0.02
00
0.020.02
0.040.04
0.060.06
0.080.08
0.10.1
00 22 44 88 1212 1616 2020 2424 AVGAVG2424
WKSWKS
EPEP
PlaceboPlaceboArifloArifloArifloAriflo

A A 4141
Decline in Lung Function in Long-term COPD StudiesDecline in Lung Function in Long-term COPD Studies
Follow-up, yearFollow-up, year
2.752.75
2.702.70
2.652.65
2.602.60
2.552.55
2.502.50
2.452.45
Me
an
FE
VM
ea
n F
EV
11 (L
) (
L) Usual CareUsual Care
Screen 2Screen 2 11 22 33 44 55
FE
VF
EV
1 1 (L
)(L
)
MonthMonth
1.501.50
1.451.45
1.401.40
1.351.35
1.301.30
1.251.25
1.201.20-3-3 00 33 66 99 1212 1515 1818 2121 2424 2727 3030 3333 3636
7575
FE
VF
EV
1 1 (m
l)(m
l)
MonthMonth-6-6 -3-3 00 33 66 99 1212 1515 1818 2121 2424 2727 3030 3333 3636
-225-225
5050252500
-25-25-50-50-75-75
-100-100-125-125-150-150-175-175-200-200 M
ea
n C
ha
ng
e f
rom
Ba
se
lin
e
Me
an
Ch
an
ge
fro
m B
as
eli
ne
F
EV
FE
V1 1
(l)
(l)
PlaceboPlacebo
MonthMonth00 33 66 99 1212 1515 1818 2121 2424 2727 3030 3333 3636
-0.25-0.25
00
-0.05-0.05
-0.10-0.10
-0.15-0.15
-0.20-0.20
PlaceboPlacebo
Lung Health StudyLung Health Study ISOLDEISOLDE
EUROSCOPEUROSCOP Copenhagen CityCopenhagen City
PlaceboPlacebo
2.802.80
SmokingSmokingInterventionIntervention
FPFP
BudesonideBudesonide
BudesonideBudesonide

A A 4242
Health-Related Quality of LifeHealth-Related Quality of LifeSt. George’s Respiratory QuestionnaireSt. George’s Respiratory Questionnaire
• Disease-specific (respiratory disease)Disease-specific (respiratory disease)
• Measures the impact of COPD on quality of lifeMeasures the impact of COPD on quality of life
• Components of SGRQComponents of SGRQ– Symptoms Symptoms – Activity Activity – Impact Impact
• Decrease in score indicates improvement in Decrease in score indicates improvement in QOL QOL – Change of -4.0 is a clinically meaningful Change of -4.0 is a clinically meaningful
improvementimprovement

A A 4343
Ariflo Significantly ImprovesAriflo Significantly ImprovesQuality of LifeQuality of Life
-1.3
0.4
-3.7-3.2
-4
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
0.5
1
Placebo
Ariflo
Mea
n C
han
ge
fro
m B
asel
ine
Mea
n C
han
ge
fro
m B
asel
ine
in
SG
RQ
sco
rein
S
GR
Q s
core
Improvement Improvement in patient’s in patient’s
QOLQOL
-4.1-4.1p<0.0001p<0.0001
Difference from Difference from placeboplacebo
-1.9-1.9p=0.017p=0.017
NA Study 039NA Study 039 NA Study 156NA Study 156

A A 4444
Change From Baseline In Total SGRQ Change From Baseline In Total SGRQ Scores Averaged Over 24 WeeksScores Averaged Over 24 Weeks
-2.3
-4.9
-1.3
-2.7
-4.2
-3.2
-3.7
-6
-5
-4
-3
-2
-1
0
1
PlaceboAriflo
Ch
ang
e fr
om
Bas
elin
e in
SG
RQ
Sco
reC
han
ge
fro
m B
asel
ine
in S
GR
Q S
core
Improvement Improvement in patient’s in patient’s
QOLQOL
NA Study 039NA Study 039 NA Study 156NA Study 156 EU Study 042EU Study 042 EU Study 091EU Study 091
0.40.4

A A 4545
Ariflo Pivotal ResultsAriflo Pivotal ResultsSecondary EndpointsSecondary Endpoints
StudyStudy 039039 156156 091091 042042
MeasureMeasure NANA NANA EUEU EUEU
FVCFVC TT TT
6-minute Walk6-minute Walk —— — — —— ——
Symptom ScoreSymptom Score —— N/A N/A ——
Post-exercise Post-exercise T T TT TT BreathlessnessBreathlessness
COPD ExacerbationsCOPD Exacerbations —— ——
= P <0.05 versus placebo= P <0.05 versus placebo— — = P >0.2 versus placebo= P >0.2 versus placeboT = 0.05 T = 0.05 << P P << 0.2 in favor of Ariflo 0.2 in favor of Ariflo

A A 4646
Percent of Patients Exacerbation-FreePercent of Patients Exacerbation-Free
50
55
60
65
70
75
80
85
90
95
100
0 50 100 150 200
50
55
60
65
70
75
80
85
90
95
100
0 50 100 150 200
50
55
60
65
70
75
80
85
90
95
100
0 50 100 150 200
50
55
60
65
70
75
80
85
90
95
100
0 50 100 150 200
NA Study 156NA Study 156No symptoms No symptoms required at entryrequired at entry
P=0.2113P=0.2113
P=0.0094P=0.0094
NA Study 039NA Study 039 P=0.0037P=0.0037
Per
cen
tag
e E
xace
rbat
ion
-Fre
eP
erce
nta
ge
Exa
cerb
atio
n-F
ree
EU Study 042EU Study 042 P=0.7912P=0.7912EU Study 091EU Study 091
DaysDays
Per
cen
tag
e E
xace
rbat
ion
-Fre
eP
erce
nta
ge
Exa
cerb
atio
n-F
ree
DaysDays
PlaceboPlaceboArifloAriflo

A A 4747
Supporting StudiesSupporting Studies

A A 4848
Long Term Extension StudiesLong Term Extension Studies
• Evaluate long term safety and tolerabilityEvaluate long term safety and tolerability
• Further evaluate FEVFurther evaluate FEV11 over time over time
• Open-Label Extension of the pivotal studiesOpen-Label Extension of the pivotal studies– Subjects from NA Study 039 were eligible to enter Subjects from NA Study 039 were eligible to enter
Study 041Study 041– Subjects from EU Studies 042 and 091 were Subjects from EU Studies 042 and 091 were
eligible to enter Study 040eligible to enter Study 040
• Concomitant COPD medication use allowed Concomitant COPD medication use allowed

A A 4949
Study 041
Long-Term Extension Long-Term Extension NA Study 041: FEVNA Study 041: FEV11
Week
EP
Study 039

A A 5050
Long-Term Extension Long-Term Extension EU Study 040: FEVEU Study 040: FEV11
Week
Studies 042, 091 Study 040

A A 5151
Patient with COPDPatient with COPDNormal Chest X-rayNormal Chest X-ray
Physiology of HyperinflationPhysiology of Hyperinflation

A A 5252
Lit
ers
Lit
ers
88
66
44
22
00
TotalTotalLungLung
CapacityCapacity
TidalTidalVolumeVolume
Functional Functional ResidualResidualCapacityCapacity ResidualResidual
VolumeVolume
NormalNormal
ResidualResidualVolumeVolume
Functional Functional ResidualResidualCapacityCapacity
COPDCOPD
TotalTotalLungLung
CapacityCapacity TidalTidalVolumeVolume
Physiology of HyperinflationPhysiology of Hyperinflation

A A 5353
Study 111: Static Lung VolumesStudy 111: Static Lung Volumes
4 weeks4 weeks 12 weeks12 weeks
Ariflo 15mg BID (n=79) Ariflo 15mg BID (n=79)
PRNPRNalbuterolalbuterol Placebo BID (n=77)Placebo BID (n=77)
PlaceboPlaceboRun-inRun-in

A A 5454
Change From Baseline In Pre-albuterol Change From Baseline In Pre-albuterol Volume Of Trapped Gas (D)Volume Of Trapped Gas (D)
Difference from placebo = -180 ml (week 12), -140 ml (EP)Difference from placebo = -180 ml (week 12), -140 ml (EP)
D = TLCD = TLCboxbox – TLC – TLChehe
WEEKWEEK
0.50.5
0.40.4
0.30.3
0.20.2
0.10.1
0.00.0
-0.1-0.1
-0.2-0.2
-0.3-0.3
-0.4-0.4
-0.5-0.5
-0.6-0.6
00 2 4 8 12 EP 2 4 8 12 EP
PlaceboPlacebo
ArifloAriflo
Ch
ang
e in
Vo
lum
e o
f T
rap
ped
Gas
(L
)C
han
ge
in V
olu
me
of
Tra
pp
ed G
as (
L)

A A 5555
Ariflo Reduces Residual Volume Ariflo Reduces Residual Volume
Difference from placebo at Endpoint = -390mlDifference from placebo at Endpoint = -390ml
Ch
ang
e in
Res
idu
al V
olu
me
(L)
Ch
ang
e in
Res
idu
al V
olu
me
(L)
WeeksWeeks

A A 5656
Ariflo Reduces Functional Ariflo Reduces Functional Residual Capacity Residual Capacity
Difference from placebo at Endpoint = -290mlDifference from placebo at Endpoint = -290ml
Ch
ang
e in
FR
C (
L)
Ch
ang
e in
FR
C (
L)
WeeksWeeks
P=0.022

A A 5757
Can Ariflo be Compared to Can Ariflo be Compared to Theophylline?Theophylline?
• No comparable studies of similar designNo comparable studies of similar design– Small numbers of patients (8 to 60 patients)Small numbers of patients (8 to 60 patients)11
– Short duration (1 day to 8 weeks)Short duration (1 day to 8 weeks)– Criteria for reversibility vary between studiesCriteria for reversibility vary between studies
• Non-selective PDE inhibitorNon-selective PDE inhibitor– Primarily bronchodilator effectPrimarily bronchodilator effect– Predominantly due to inhibition of PDE3Predominantly due to inhibition of PDE322
– Weak activity at PDE4Weak activity at PDE433
11Ram FSF, Ram FSF, et al. Cochrane Database of Systematic Reviewset al. Cochrane Database of Systematic Reviews 2003. 2003.2 2 TheolairTheolair®® Prescribing Information Prescribing Information33Howell, Howell, et al. J Pharmacol. Exp. Ther.et al. J Pharmacol. Exp. Ther. 1993; 264: 609-615. 1993; 264: 609-615.

A A 5858
Can Ariflo be Compared to Can Ariflo be Compared to Theophylline?Theophylline?
ZuWallack RL, ZuWallack RL, et al. Chestet al. Chest 2001; 119:1661-1670. 2001; 119:1661-1670.
Data on file, Data on file, GlaxoSmithKline (SLGA4020/21).GlaxoSmithKline (SLGA4020/21).
Ch
an
ge
fro
m B
as
eli
ne
in
FE
VC
ha
ng
e f
rom
Ba
se
lin
e i
n F
EV
11 (L
) (
L)
HourHour HourHour
Day 1Day 1 Week 12Week 12
-0.1-0.1
-0.05-0.05
00
0.050.05
0.10.1
0.150.15
0.20.2
0.250.25
0.30.3
0.350.35
00 11 22 33 44 55 66 77 88 99 1010 1111 1212
ITTITT
-0.1-0.1
-0.05-0.05
00
0.050.05
0.10.1
0.150.15
0.20.2
0.250.25
0.30.3
0.350.35
00 11 22 33 44 55 66 77 88 99 1010 1111 1212
ITTITTNon-reversibleNon-reversible Non-reversibleNon-reversible

A A 5959
Efficacy SummaryEfficacy SummaryCo-Primary EndpointsCo-Primary Endpoints
FEVFEV11::
• Maintenance of FEVMaintenance of FEV11 over 24 weeks with over 24 weeks with statistically significant benefit over placebo in statistically significant benefit over placebo in both NA pivotal studiesboth NA pivotal studies
• Magnitude of effect consistent across NA and EU Magnitude of effect consistent across NA and EU studiesstudies
SGRQ:SGRQ:
• Significant improvement in health-related quality Significant improvement in health-related quality of life versus placebo in both NA studiesof life versus placebo in both NA studies
• Consistent improvement from baseline in Ariflo Consistent improvement from baseline in Ariflo groups across NA and EU studiesgroups across NA and EU studies

A A 6060
Efficacy SummaryEfficacy SummarySupporting DataSupporting Data
• Decrease in relative risk of moderate to Decrease in relative risk of moderate to severe exacerbations in Studies 039 severe exacerbations in Studies 039 and 091and 091
• Maintenance of FEVMaintenance of FEV11 observed in the observed in the
long term studies for up to 84 weeks long term studies for up to 84 weeks
• Substantial reduction in hyperinflationSubstantial reduction in hyperinflation

A A 6161
Efficacy ConclusionsEfficacy Conclusions
• COPD is a complex and progressive COPD is a complex and progressive diseasedisease
• Poorly reversible populationPoorly reversible population
– Difficult to treat, more rapid decline in Difficult to treat, more rapid decline in FEVFEV11
• Ariflo targets inflammation specific to Ariflo targets inflammation specific to COPDCOPD
• Efficacy data support proposed indicationEfficacy data support proposed indication


A A 6363
Safety of ArifloSafety of Ariflo
Kathy Rickard, M.D.Kathy Rickard, M.D.
Vice President Vice President
Respiratory Clinical Development and Medical AffairsRespiratory Clinical Development and Medical Affairs
GlaxoSmithKlineGlaxoSmithKline

A A 6464
Safety OverviewSafety Overview
• Phase I & II studiesPhase I & II studies– Over 50 studies including clinical Over 50 studies including clinical
pharmacology and dose rangingpharmacology and dose ranging
• Phase III studiesPhase III studies
– Adverse eventsAdverse events– Gastrointestinal Safety Gastrointestinal Safety – Cardiovascular Safety Cardiovascular Safety – Long term safety up to 3 yearsLong term safety up to 3 years

A A 6565
Safety Exposure Safety Exposure
• 3,445 patients in all Phase III COPD 3,445 patients in all Phase III COPD studies studies – 2,119 Ariflo; 1,326 placebo2,119 Ariflo; 1,326 placebo
• 2,883 patients in the pivotal 24-week 2,883 patients in the pivotal 24-week COPD studiesCOPD studies– 1,792 Ariflo; 1,091 placebo1,792 Ariflo; 1,091 placebo
• Over 1,000 patients in long-term Over 1,000 patients in long-term extension studiesextension studies– Nearly 3,000 patient-years of exposure to Nearly 3,000 patient-years of exposure to
ArifloAriflo

A A 6666
All Randomized PatientsAll Randomized PatientsPlacebo Placebo ArifloAriflon=1091n=1091 n=1792n=1792
Adverse Experience* Adverse Experience* %% %%
TotalTotal 76.976.9 78.378.3COPD COPD 36.236.2 30.430.4NauseaNausea 5.05.0 15.715.7DiarrheaDiarrhea 7.97.9 14.414.4Abdominal PainAbdominal Pain 7.17.1 11.711.7Upper Respiratory Tract infectionUpper Respiratory Tract infection 10.310.3 8.88.8HeadacheHeadache 7.07.0 8.28.2DyspepsiaDyspepsia 2.52.5 6.86.8VomitingVomiting 1.61.6 6.16.1InjuryInjury 5.05.0 5.45.4CoughingCoughing 5.35.3 3.53.5
COPD 24-week Studies: AEsCOPD 24-week Studies: AEs
* Includes adverse experiences reported for * Includes adverse experiences reported for >>5% of patients in either of the treatment groups5% of patients in either of the treatment groups

A A 6767
COPD 24-week Studies:COPD 24-week Studies:Withdrawal Due to AEsWithdrawal Due to AEs
All Randomized PatientsAll Randomized PatientsPlacebo Placebo ArifloAriflo
Adverse Experience*Adverse Experience* n=1091n=1091 n=1792n=1792%% %%
TotalTotal 11.711.7 17.517.5NauseaNausea 0.50.5 5.15.1Abdominal PainAbdominal Pain 0.70.7 4.34.3DiarrheaDiarrhea 0.60.6 3.63.6COPDCOPD 3.83.8 2.22.2VomitingVomiting 0.30.3 1.41.4Dyspepsia Dyspepsia 0.10.1 1.01.0DizzinessDizziness 0.20.2 0.90.9HeadacheHeadache 0.10.1 0.90.9FlatulenceFlatulence 0.10.1 0.50.5
* Includes adverse experiences reported for * Includes adverse experiences reported for >>0.5% of patients in either of the treatment 0.5% of patients in either of the treatment groupsgroups

A A 6868
Rationale for Extensive GI Rationale for Extensive GI MonitoringMonitoring
• Class-related GI adverse eventsClass-related GI adverse events
• Medial necrosis in rat mesenteric arteries Medial necrosis in rat mesenteric arteries seen at seen at >>30mg/kg/day 30mg/kg/day – Not observed in primatesNot observed in primates– No intestinal ischemia observed No intestinal ischemia observed
• Medial necrosis also seen with theophylline Medial necrosis also seen with theophylline and caffeine in rodentsand caffeine in rodents– No association of mesenteric ischemia over No association of mesenteric ischemia over
decades of use in humansdecades of use in humans
Collins JJ, Collins JJ, et al. Fundam Appl Toxicolet al. Fundam Appl Toxicol 1988; 11:472-484. 1988; 11:472-484. Johansson S, Johansson S, Acta Pathol Microbiol ScandActa Pathol Microbiol Scand 1981; 89:185-191. 1981; 89:185-191.

A A 6969
Extensive GI Safety Monitoring Extensive GI Safety Monitoring
• Physical examsPhysical exams
• Laboratory assessmentsLaboratory assessments
• Orthostatic vital signsOrthostatic vital signs
• Fecal occult blood testsFecal occult blood tests
• GI adverse events of concernGI adverse events of concern– Any GI adverse event that interfered with Any GI adverse event that interfered with
patient’s daily activitiespatient’s daily activities

A A 7070
Extensive GI Safety Monitoring Extensive GI Safety Monitoring
• Patients who completed study:Patients who completed study:
– 6 fecal occult blood tests6 fecal occult blood tests– 10 sets of laboratory evaluations10 sets of laboratory evaluations– 13 sets of vital signs13 sets of vital signs– 4 sets of orthostatic vital signs4 sets of orthostatic vital signs

A A 7171
COPD 24-week Studies:COPD 24-week Studies:GIAEs of ConcernGIAEs of Concern
All Randomized PatientsAll Randomized PatientsPlacebo Placebo ArifloAriflo
Adverse Experience*Adverse Experience* n=1091n=1091 n=1792n=1792(Preferred term)(Preferred term) %% %%
TotalTotal 4.84.8 12.912.9Abdominal PainAbdominal Pain 2.62.6 5.95.9DiarrheaDiarrhea 2.12.1 5.25.2NauseaNausea 0.60.6 4.34.3VomitingVomiting 0.50.5 2.92.9DyspepsiaDyspepsia 0.30.3 1.61.6MelenaMelena 0.80.8 0.90.9FlatulenceFlatulence 0.20.2 0.90.9
* Includes adverse experiences reported for * Includes adverse experiences reported for >>0.5% of patients in either of the treatment groups0.5% of patients in either of the treatment groups

A A 7272
Cumulative Incidence of GI Adverse Cumulative Incidence of GI Adverse Events of Concern in Pivotal StudiesEvents of Concern in Pivotal Studies
00
55
1010
2020
2525
00 3030 9090 120120 180180 210210
Study DayStudy Day
% o
f P
atie
nts
wit
h G
IAE
of
Co
nce
rn%
of
Pat
ien
ts w
ith
GIA
E o
f C
on
cern
ArifloAriflo
PlaceboPlacebo
1515
1501506060141477 2121

A A 7373
Fecal Occult Blood Testing in the Fecal Occult Blood Testing in the Pivotal StudiesPivotal Studies
All Randomized PatientsAll Randomized Patients
Placebo Placebo ArifloAriflo
n=1091n=1091 n=1792n=1792
Total Total
# Tested# Tested 788788 12561256 # Positive n (%)# Positive n (%) 12 (1.5%)12 (1.5%) 27 (2.2%)27 (2.2%)
GIAEs of ConcernGIAEs of Concern n=52 n=52 n=231n=231
# Tested# Tested 4242 205205
# Positive n (%)# Positive n (%) 5 (11.9%)5 (11.9%) 16 (7.8%)16 (7.8%)

A A 7474
Reports of Bowel Ischemia in the Reports of Bowel Ischemia in the Clinical ProgramClinical Program
PlaceboPlacebo ArifloAriflo
Pivotal TrialsPivotal Trials# Cases# Cases 22 00Person-Years ExposedPerson-Years Exposed 444444 683683Incidence Rate per 1000 pyIncidence Rate per 1000 py 4.54.5 00
Long Term ExtensionLong Term Extension# Cases# Cases Not ApplicableNot Applicable 33Person-Years ExposedPerson-Years Exposed …… 18001800Incidence Rate per 1000 pyIncidence Rate per 1000 py …… 1.71.7
TotalTotal# Cases# Cases 22 33Person-Years ExposedPerson-Years Exposed 444444 24832483Incidence Rate per 1000 pyIncidence Rate per 1000 py 4.54.5 1.21.2
py=person yearspy=person years

A A 7575
Incidence of Serious Adverse Events Incidence of Serious Adverse Events in Pivotal Studiesin Pivotal Studies
All Randomized PatientsAll Randomized PatientsPlacebo Placebo ArifloAriflon=1091n=1091 n=1792n=1792
Serious Adverse Event: n (%)Serious Adverse Event: n (%)
TotalTotal 96 (8.8%) 96 (8.8%) 104 (5.8%)104 (5.8%)
Gastrointestinal body system Gastrointestinal body system 12 (1.1%)12 (1.1%) 10 (0.6%) 10 (0.6%)
Cardiovascular body system* 28 (2.6%)Cardiovascular body system* 28 (2.6%) 20 (1.1%) 20 (1.1%)
Respiratory body systemRespiratory body system 31 (2.8%)31 (2.8%) 30 (1.7%) 30 (1.7%)
*Includes events reported for cardiovascular general, heart rate and rhythm, *Includes events reported for cardiovascular general, heart rate and rhythm, and myocardial, endocardial, pericardial valve body systems.and myocardial, endocardial, pericardial valve body systems.

A A 7676
GI Safety SummaryGI Safety SummaryNo Evidence ofNo Evidence of Bowel IschemiaBowel Ischemia
• Mesenteric vasculopathy occurred only in Mesenteric vasculopathy occurred only in rodentsrodents
• No evidence of bowel ischemia in animals, No evidence of bowel ischemia in animals, including ratsincluding rats
• Extensive GI safety monitoring demonstrated Extensive GI safety monitoring demonstrated no serious GI effectsno serious GI effects
• Incidence of bowel ischemia was comparable Incidence of bowel ischemia was comparable between Ariflo and placebobetween Ariflo and placebo

A A 7777
Extensive Cardiovascular Safety Extensive Cardiovascular Safety Monitoring Monitoring
• CV safety issues with non-selective CV safety issues with non-selective PDE inhibitorsPDE inhibitors
• Myocardial necrosis at high, lethal Myocardial necrosis at high, lethal doses (doses (>>80mg/kg/day) in rat toxicity 80mg/kg/day) in rat toxicity studiesstudies
• CV Safety (vital signs, ECGs, Holters)CV Safety (vital signs, ECGs, Holters)
Whitehurst VE, Whitehurst VE, et al. Toxicologyet al. Toxicology 1996; 100:113-121. 1996; 100:113-121.

A A 7878
Extensive Cardiovascular Safety Extensive Cardiovascular Safety MonitoringMonitoring
• >70,000 ECGs >70,000 ECGs – >68,000 ECGs in patients with COPD>68,000 ECGs in patients with COPD
– >6,000 ECGs at C>6,000 ECGs at Cmaxmax
• >1,000 Holters>1,000 Holters– 24-hour Holter monitoring in over 400 24-hour Holter monitoring in over 400
patients patients

A A 7979
Extensive ECG Monitoring Revealed Extensive ECG Monitoring Revealed No Safety Issues with ArifloNo Safety Issues with Ariflo
*>5% of patients in any treatment group*>5% of patients in any treatment group
All Randomized PatientsAll Randomized PatientsPlacebo % Placebo % Ariflo %Ariflo %
New Onset ECG Abnormalities* New Onset ECG Abnormalities* n=1091n=1091 n=1792n=1792
Sinus BradycardiaSinus Bradycardia 13.613.6 14.414.4Q-T Interval IncreasedQ-T Interval Increased 12.412.4 12.312.3T-wave Abnormal NOST-wave Abnormal NOS 13.013.0 9.59.5Premature Atrial Contractions NOSPremature Atrial Contractions NOS 10.310.3 9.09.0Intraventicular Block NOSIntraventicular Block NOS 6.26.2 8.18.1S-T Changes NonspecificS-T Changes Nonspecific 9.49.4 8.18.1Poor R-wave ProgressionPoor R-wave Progression 9.09.0 7.67.6Sinus TachycardiaSinus Tachycardia 5.85.8 6.06.0PVCs NOSPVCs NOS 2.82.8 5.75.7Sinus ArrhythmiaSinus Arrhythmia 7.17.1 5.65.6Left Atrial Hypertrophy (P mitrale)Left Atrial Hypertrophy (P mitrale) 5.85.8 4.94.9PVCs UnifocalPVCs Unifocal 7.27.2 4.64.6

A A 8080
QTc Interval Similar Between QTc Interval Similar Between Treatment GroupsTreatment Groups
All Randomized PatientsAll Randomized Patients
Placebo Placebo ArifloAriflo n=1091n=1091 n=1792n=1792
Mean QTc* (msec)Mean QTc* (msec) BaselineBaseline 424 424 425425 Change from Baseline at EPChange from Baseline at EP 0.1 0.1 -0.4-0.4
QTc* Increases from baseline at any time-pointQTc* Increases from baseline at any time-point Patients with 30-60msec change**Patients with 30-60msec change** 144 (18.6%) 144 (18.6%) 212 (17.3%)212 (17.3%) Patients with >60msec change*Patients with >60msec change** 23 (3.0%)* 23 (3.0%) 21 (1.7%) 21 (1.7%)
*Bazett’s correction*Bazett’s correction
**in patients with a normal QTc at Baseline**in patients with a normal QTc at Baseline

A A 8181
New Onset Cardiac Events:New Onset Cardiac Events:24-Hour Holter Monitoring24-Hour Holter Monitoring
New Onset n (%)New Onset n (%)Cardiac Event Cardiac Event PlaceboPlacebo Ariflo Ariflo
Atrial FibrillationAtrial Fibrillation 00 2 (0.7)2 (0.7)
Atrial FlutterAtrial Flutter 00 1 (0.4)1 (0.4)
First Degree AV BlockFirst Degree AV Block 5 (3.6)5 (3.6) 6 (2.2)6 (2.2)
Mobitz Type 1Mobitz Type 1 00 2 (0.7)2 (0.7)
Mobitz Type 2Mobitz Type 2 2 (1.4)2 (1.4) 1 (0.4)1 (0.4)
Sinus BradycardiaSinus Bradycardia 12 (12.2)12 (12.2) 29 (15.1)29 (15.1)
Sinus PauseSinus Pause 6 (4.3)6 (4.3) 4 (1.5)4 (1.5)
Supraventricular TachycardiaSupraventricular Tachycardia 29 (46.8)29 (46.8) 65 (45.5)65 (45.5)
Non-Sustained VTNon-Sustained VT 11 (8.3)11 (8.3) 23 (8.7)23 (8.7)

A A 8282
Incidence of Serious Adverse Events Incidence of Serious Adverse Events in Pivotal Studiesin Pivotal Studies
All Randomized PatientsAll Randomized PatientsPlacebo Placebo ArifloAriflon=1091n=1091 n=1792n=1792
Serious Adverse Event: n (%)Serious Adverse Event: n (%)
TotalTotal 96 (8.8%) 96 (8.8%) 104 (5.8%)104 (5.8%)
Gastrointestinal body system Gastrointestinal body system 12 (1.1%)12 (1.1%) 10 (0.6%)10 (0.6%)
Cardiovascular body system* Cardiovascular body system* 28 (2.6%)28 (2.6%) 20 (1.1%)20 (1.1%)
Respiratory body systemRespiratory body system 31 (2.8%)31 (2.8%) 30 (1.7%)30 (1.7%)
*Includes events reported for cardiovascular general, heart rate and rhythm, *Includes events reported for cardiovascular general, heart rate and rhythm, and myocardial, endocardial, pericardial valve body systems.and myocardial, endocardial, pericardial valve body systems.

A A 8383
Serious Adverse Events with Fatal Serious Adverse Events with Fatal Outcome in the Pivotal StudiesOutcome in the Pivotal Studies
PlaceboPlacebo ArifloAriflo
n=1091n=1091 n=1792n=1792
Fatal SAEs* Fatal SAEs* 5 (0.5%)5 (0.5%) 7 (0.4%)7 (0.4%)
*None were considered related to treatment.*None were considered related to treatment.

A A 8484
Safety Data from Long Term Safety Data from Long Term Extension StudiesExtension Studies
• Greater than 1,000 patients for up to 3 yearsGreater than 1,000 patients for up to 3 years
• Over 25,000 ECGs performedOver 25,000 ECGs performed
• Safety data similar to pivotal trialsSafety data similar to pivotal trials– No cardiovascular safety issues identifiedNo cardiovascular safety issues identified– No gastrointestinal safety issues identifiedNo gastrointestinal safety issues identified

A A 8585
Additional Safety AssessmentsAdditional Safety AssessmentsClinical Pharmacology StudiesClinical Pharmacology Studies
• Male reproductiveMale reproductive
• NeuroendocrineNeuroendocrine
• Drug-drug interactionsDrug-drug interactions

A A 8686
Male Reproductive SystemMale Reproductive System
• Nonclinical studies with Ariflo showed Nonclinical studies with Ariflo showed testicular degeneration in rats and rabbits, testicular degeneration in rats and rabbits, but not in mice or primatesbut not in mice or primates
• Ariflo 15mg BID or placebo was administered Ariflo 15mg BID or placebo was administered to 100 healthy, young male subjects for 12 to 100 healthy, young male subjects for 12 weeksweeks
• No evidence of a clinically significant effect No evidence of a clinically significant effect on sperm number, motility, or morphology in on sperm number, motility, or morphology in humanshumans

A A 8787
Neuroendocrine SystemNeuroendocrine System
• Adrenocortical hypertrophy in ratsAdrenocortical hypertrophy in rats– Stimulation of the HPA-axis is well-recognized Stimulation of the HPA-axis is well-recognized
response of rats to PDE inhibitors response of rats to PDE inhibitors
• Mammary tumors at high dose in mice Mammary tumors at high dose in mice associated with pseudopregnancy associated with pseudopregnancy
• No evidence of an effect on prolactin, ACTH, No evidence of an effect on prolactin, ACTH, serum or urinary cortisol levels in humansserum or urinary cortisol levels in humans
Kumari M, Kumari M, et al. Brit J Pharmacolet al. Brit J Pharmacol 1997; 121:459-468. 1997; 121:459-468.Law LW, Law LW, Proc Soc Exp Biol MedProc Soc Exp Biol Med 1941; 48:486-487. 1941; 48:486-487.

A A 8888
Interaction StudiesInteraction Studies
• No evidence of interactions:No evidence of interactions:– Albuterol, ipratropium, theophylline, prednisolone, Albuterol, ipratropium, theophylline, prednisolone,
warfarin, and digoxinwarfarin, and digoxin– SmokingSmoking
• No effect on bioavailability with magnesium-No effect on bioavailability with magnesium-aluminum-dimethicone antacid or foodaluminum-dimethicone antacid or food
• Potential for increased GI intolerance Potential for increased GI intolerance – Co-administration with erythromycin Co-administration with erythromycin – Severe hepatic impairmentSevere hepatic impairment– Severe renal impairmentSevere renal impairment

A A 8989
Ariflo Safety ConclusionsAriflo Safety Conclusions
• Extensive safety data with exposure to Ariflo Extensive safety data with exposure to Ariflo up to 3 yearsup to 3 years
• For patients with GI adverse events, most For patients with GI adverse events, most occurred early and were mild to moderate in occurred early and were mild to moderate in intensityintensity
• Serious AEs, including GI, were infrequent Serious AEs, including GI, were infrequent and similar between treatment groupsand similar between treatment groups
• No evidence of an increased risk of No evidence of an increased risk of cardiovascular eventscardiovascular events


A A 9191
Assessment of Outcome in Assessment of Outcome in COPDCOPD
Frank Sciurba, MDFrank Sciurba, MDAssociate Professor of MedicineAssociate Professor of Medicine
Division of Pulmonary, Allergy and Critical Care Division of Pulmonary, Allergy and Critical Care
Medicine University of PittsburghMedicine University of Pittsburgh

A A 9292
The Face of Chronic Obstructive The Face of Chronic Obstructive Pulmonary Disease (COPD)Pulmonary Disease (COPD)
EmphysemaEmphysema ChronicChronic Bronchitis

A A 9393
0
10
20
30
40
50
60
HospitalStay
60 Days 180 Days 1 Year 2 Years
Mo
rtal
ity
(%)
Mo
rtal
ity
(%)
Median length of hospital stay: 9 daysMedian length of hospital stay: 9 daysMedian cost of hospitalization: $7,100Median cost of hospitalization: $7,100Readmission rate (6 months): 44%Readmission rate (6 months): 44%
Time After HospitalizationTime After Hospitalization
Connors AF, Connors AF, et al.et al. Am J Respir Crit Care MedAm J Respir Crit Care Med. 1996;154:959-967. 1996;154:959-967
Health Care Utilization and Health Care Utilization and Mortality Due to ExacerbationsMortality Due to Exacerbations

A A 9494
No single parameter in patients No single parameter in patients with COPD is sufficient to be with COPD is sufficient to be
considered the gold standard to considered the gold standard to assess outcome.assess outcome.
— — A. Fishman, 1994A. Fishman, 1994

A A 9595
Clinical Research in COPD:Clinical Research in COPD:Needs and OpportunitiesNeeds and Opportunities
• NHLBI Workshop SummaryNHLBI Workshop Summary
– What measures of disease status are useful What measures of disease status are useful indices therapeutic benefit?indices therapeutic benefit?
– What can be done to promote the development What can be done to promote the development and testing of novel agents for the treatment of and testing of novel agents for the treatment of COPD? efforts that may reduce these barriers …COPD? efforts that may reduce these barriers …exploration of alternative outcome measures”exploration of alternative outcome measures”
Croxton TL, Croxton TL, et al.et al. Am J Respir Crit Care Med Am J Respir Crit Care Med 2003; 167:1142.2003; 167:1142.

A A 9696
FEVFEV11: Advantages: Advantages
• On average reflects function and On average reflects function and prognosisprognosis
• Reproducible measureReproducible measure
• Responsiveness to various therapies Responsiveness to various therapies well establishedwell established

A A 9797
Prognosis in Chronic Prognosis in Chronic Obstructive Pulmonary DiseaseObstructive Pulmonary Disease
% S
urv
ival
% S
urv
ival
YearsYears
NormalsNormals>> 50% Predicted 50% Predicted40-49% Predicted40-49% Predicted30-39% Predicted30-39% Predicted<30% Predicted<30% Predicted
100100
9090
8080
7070
6060
00 11 22 33
FEVFEV11
Anthonisen N, Anthonisen N, Am Rev Respir DisAm Rev Respir Dis 1986; 133(1):14-20 1986; 133(1):14-20

A A 9898
FEVFEV11: Limitations: Limitations
• Marked Marked individualindividual variation in symptoms and variation in symptoms and disability independent of FEVdisability independent of FEV11
• Symptomatic and functional response to Symptomatic and functional response to therapy may be independent of FEVtherapy may be independent of FEV11
• May not reflect changes in important disease May not reflect changes in important disease activity which could lead to long term activity which could lead to long term functional decline or frequency of functional decline or frequency of exacerbationsexacerbations

A A 9999
SGRQ = St. George’s Respiratory QuestionnaireSGRQ = St. George’s Respiratory Questionnaire*Higher scores = worse quality of life*Higher scores = worse quality of lifeAdapted with permission from Jones PW. Adapted with permission from Jones PW. ChestChest 1995; 107(suppl): 187S-193S. 1995; 107(suppl): 187S-193S.
100100
9090
8080
7070
6060
5050
4040
3030
2020
1010
0000 2020 4040 6060 8080 100100 120120
FEVFEV11 (% predicted) (% predicted)
SGRQ SGRQ ScoreScore
r=0.30r=0.30P<0.001P<0.001
Normal Normal Means 2 SDMeans 2 SD
Correlation of Quality of Life Scores Correlation of Quality of Life Scores (SGRQ*) with FEV(SGRQ*) with FEV11 in Patients with COPD in Patients with COPD

A A 100100
Spirometric Changes with Spirometric Changes with Increasing Degrees of ObstructionIncreasing Degrees of Obstruction
00
11
22
33
44
55
66
77
00 11 22 33 44 55 66
SecondsSeconds
LitersLiters(BTPS)(BTPS)

A A 101101
Residual VolumeResidual Volume
ResidualResidualVolumeVolume (RV) (RV)
Normal PatternNormal PatternObstructive PatternObstructive Pattern
FunctionalFunctionalResidual Residual Capacity Capacity
(FRC)(FRC) FunctionalFunctionalResidualResidualCapacityCapacity
Vital Capacity Vital Capacity
Vital Vital Capacity Capacity
(VC)(VC)

A A 102102
Hyperinflation in EmphysemaHyperinflation in Emphysema

A A 103103
Lung and Chest Wall Forces at Lung and Chest Wall Forces at End-Expiration in COPD vs. NormalEnd-Expiration in COPD vs. Normal
NormalNormal
Adapted From O’Donnell.Adapted From O’Donnell.
Chest wall recoil remainsChest wall recoil remainsinward resulting in ainward resulting in athreshold load at the threshold load at the start of inspirationstart of inspiration
Flattened shortened Flattened shortened diaphragm muscle diaphragm muscle inefficient in force inefficient in force generationgeneration
COPDCOPD

A A 104104

A A 105105
Dynamic Lung Volume Regulation During Dynamic Lung Volume Regulation During Exertion in COPD Compared to NormalExertion in COPD Compared to Normal
O’Donnell. O’Donnell. ChestChest 2000; 117:42S-47S. 2000; 117:42S-47S.
2020
EELVEELV
00 4040 6060 80804040
6060
8080
140140
120120
100100
% p
red
icte
d T
LC
% p
red
icte
d T
LC
TLCTLC
normalnormal
EELV (FRC)EELV (FRC)
TLCTLC
COPDCOPD
Ventilation (L/min)Ventilation (L/min)

A A 106106
Bronchodilator Responses in Patients Bronchodilator Responses in Patients with “Irreversible” Emphysemawith “Irreversible” Emphysema
Ch
ang
e fr
om
Bas
elin
e p
ost
-alb
ute
rol
Ch
ang
e fr
om
Bas
elin
e p
ost
-alb
ute
rol
(L)
(L)
*p<0.05*p<0.05
O’Donnell, DE. O’Donnell, DE. Eur Resp JEur Resp J 2001; 18:914-920. 2001; 18:914-920.
0.10*0.08*0.09*
-0.51*
-0.27*-0.37*-0.45*
-0.21*-0.31*
-1
-0.5
0
0.5
1FEV1
RV
FRC
All Patientsn=84
Moderaten=48
Severen=36

A A 107107
Number of Inflammatory CellsNumber of Inflammatory Cellsper mper m22 of Lung Surface Area of Lung Surface Area
Air SpaceAir Space TissueTissue
ControlControl MildMild SevereSevere ControlControl MildMild SevereSevere
NeutrophilsNeutrophils 2020 5050 300*300* 2424 2929 140* 140* (x10(x1088/m/m22))
MacrophagesMacrophages 270270 330330 4000*4000* 4.54.5 4.44.4 71*71*(x10(x1088/m/m22))
CD8+CD8+ 4040 4646 1400*1400* 3131 3434 250*250*(x10(x1088/m/m22))
*Different from Control and Mild (p <0.01) *Different from Control and Mild (p <0.01)
Retamales I, Retamales I, et al.et al. Am J Respir Crit Care MedAm J Respir Crit Care Med 2001; 164:469-473. 2001; 164:469-473.
Calhoun WJ,Calhoun WJ, et al. Am J Respir Crit Care Med et al. Am J Respir Crit Care Med 2001;2001; 165:730b-731b.165:730b-731b.

A A 108108
- S. Shapiro- S. Shapiro
The Cigarette Burns Out The Cigarette Burns Out But the Inflammation But the Inflammation
Rages OnRages On

A A 109109
Smoking Cessation: Anti-inflammatory ModelSmoking Cessation: Anti-inflammatory Model
Participants = 5887
Pre
dic
ted
FE
VP
red
icte
d F
EV
11 (%
) (
%)
Adapted from Anthonisen N, Adapted from Anthonisen N, et al.et al. JAMAJAMA. 1994;272:1497-1505. . 1994;272:1497-1505.
8282
8080
7878
7676
7474
7272
BL BL 1 1 22 33 44 55Annual VisitsAnnual Visits
QuittersQuittersSmokersSmokers
1516
38043804
1207
32643264
1067
28642864
972
25262526
910
22982298

A A 110110
Mea
n C
han
ge
fro
m B
asel
ine
Mea
n C
han
ge
fro
m B
asel
ine
in T
rou
gh
FE
Vin
Tro
ug
h F
EV
11 (L
) (
L)
WeekWeek
-0.1
-0.08
-0.06
-0.04
-0.02
0
0.02
0.04
0.06
0.08
0.1
0 2 4 8 12 16 20 24 AVG24
WKS
EP
Placebo
Ariflo
P<0.001P=0.002
Ariflo Maintains FEVAriflo Maintains FEV11
NA Study 039NA Study 039

A A 111111
Ariflo Reduces Residual Volume Ariflo Reduces Residual Volume
Difference from placebo at Endpoint = -390mlDifference from placebo at Endpoint = -390ml
Ch
ang
e in
Res
idu
al V
olu
me
(L)
Ch
ang
e in
Res
idu
al V
olu
me
(L)
WeeksWeeks

A A 112112
Study 076:Study 076:Ariflo Decreased Inflammatory Cells in Ariflo Decreased Inflammatory Cells in
Bronchial BiopsiesBronchial Biopsies
-75
-50
-25
0
25
50
Ch
an
ge
in s
ub
-ep
ith
elia
l m
ac
rop
ha
ge
s/a
rea
tis
su
e
Placebo Ariflo
Difference from placebo: p=0.005
-250
-200
-150
-100
-50
0
50
100
150
Ch
an
ge
in s
ub
-ep
ith
elia
l CD
8+
ly
mp
ho
cy
tes
/are
a t
iss
ue
Placebo Ariflo
Difference from placebo: p=0.055

A A 113113
ConclusionsConclusions
• Clinically relevant outcomes of novel anti-Clinically relevant outcomes of novel anti-inflammatory agents for COPDinflammatory agents for COPD
– Stabilization of FEVStabilization of FEV11
– Reduction in lung hyperinflationReduction in lung hyperinflation– Airway inflammationAirway inflammation
• FEVFEV11
– Useful measure of severity and outcome in COPDUseful measure of severity and outcome in COPD– May not reflect other clinically important May not reflect other clinically important
measures of lung hyperinflation and inflammatory measures of lung hyperinflation and inflammatory activityactivity


A A 115115
Summary RemarksSummary Remarks
David Wheadon, M.D.David Wheadon, M.D.
Senior Vice PresidentSenior Vice President
Regulatory Affairs Regulatory Affairs
GlaxoSmithKlineGlaxoSmithKline

A A 116116
COPD Mortality is IncreasingCOPD Mortality is Increasing
Mannino DM Mannino DM et al.et al. MMWR, MMWR, 2002: 51(SS06);1-16. 2002: 51(SS06);1-16. Pastor PN Pastor PN et al. National Center for Health Statisticset al. National Center for Health Statistics, 2002., 2002.
-48.0%
-19.9%
-6.9% -6.9%
25.5%
-50
-40
-30
-20
-10
0
10
20
30
40
50
Per
cen
t ch
ang
e
HIV
CAD
Stroke Cancer
COPD
Percent change in age-adjusted death rates in theUS over 10 years (1990-2000)

A A 117117
BronchoconstrictionBronchoconstriction
Mediator Release From Pro-inflammatory CellsMediator Release From Pro-inflammatory Cells Influx of Inflammatory CellsInflux of Inflammatory Cells
Edema and AdhesionEdema and Adhesion
Mucus HypersecretionMucus Hypersecretion
Mucus GlandMucus GlandAirwayAirway
Smooth Muscle Smooth Muscle
EndotheliumEndothelium
Airway RemodellingAirway Remodelling
FibroblastsFibroblastsARIFLOARIFLO
NeutrophilNeutrophilMacrophageMacrophageCD8CD8++ T-Cell T-Cell EosinophilEosinophil EpitheliumEpitheliumMast cellMast cell
Potential Therapeutic Benefits of ArifloPotential Therapeutic Benefits of Ariflo

A A 118118
Ariflo:Ariflo:A New Treatment Option for COPDA New Treatment Option for COPD
• Achieved co-primary endpoints in both Achieved co-primary endpoints in both North American studiesNorth American studies
• No serious safety issuesNo serious safety issues
• Lack of interactionsLack of interactions
• Oral treatment may improve complianceOral treatment may improve compliance

A A 119119
External ExpertsExternal Experts
Loren Laine, M.D.Loren Laine, M.D.Chief, GI SectionChief, GI SectionL.A. County – U.S.C. Medical CenterL.A. County – U.S.C. Medical CenterProfessor of MedicineProfessor of MedicineUniversity of Southern California University of Southern California Medical SchoolMedical School
Christina Wang, M.D.Christina Wang, M.D.Program DirectorProgram DirectorGeneral Clinical Research CenterGeneral Clinical Research CenterHarbor-UCLA Medical CenterHarbor-UCLA Medical CenterProfessor of MedicineProfessor of MedicineDavid Geffen UCLADavid Geffen UCLASchool of MedicineSchool of Medicine
Jeremy N. Ruskin, M.D.Jeremy N. Ruskin, M.D.Director, Cardiac Arrhythmia ServiceDirector, Cardiac Arrhythmia ServiceMassachusetts General HospitalMassachusetts General HospitalAssociate Professor of MedicineAssociate Professor of MedicineHarvard Medical SchoolHarvard Medical School
Gary Koch, Ph.D.Gary Koch, Ph.D.Professor of BiostatisticsProfessor of BiostatisticsUniversity of North CarolinaUniversity of North Carolina