6 Pleural Effusion Nursing Care Plans
11
Click here to load reader
-
Upload
jamieboyrn -
Category
Documents
-
view
3.021 -
download
9
Transcript of 6 Pleural Effusion Nursing Care Plans

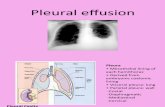
Pleural effusion is an accumulation of fluid in the pleural space. Pleural fluid normally seeps continually into the pleural space from the capillaries lining the parietal pleura and is reabsorbed by the visceral pleural capillaries and lymphatic system. Any condition that interferes with either secretion or drainage of this fluid leads to pleural effusion.
Causes of pleural effusion can be grouped into four major categories:
Increased systemic hydrostatic pressure (e.g., heart failure) Reduced capillary oncotic pressure (e.g., liver or renal failure) Increased capillary permeability (e.g., infection or trauma) Impaired lymphatic function (e.g., lymphatic obstruction caused by tumor)
See other nursing care plans here
Nursing Care Plans
1 Ineffective Breathing Pattern
Ineffective breathing pattern occurs when inspiration and expiration does not provide adequate ventilation. Pleural inflammation causes sharp localized pain that increases deep of breathing, coughing and movement. This can result to shallow and rapid breathing pattern. Distal airways and alveoli may not expand optimally with each breath, increasing the possibility of atelectasis and impaired gas exchange.
AssessmentNursing Diagnosis
PlanningNursing Interventions
RationaleExpected Outcome
Subjective:
Dyspnea
Objectives:
The patient manifested the following:
Tachypnea Presence of
crackles on both lung fields upon auscultation
use of accessory
Ineffective Breathing Pattern RT Decreased Lung Volume Capacity as evidenced by tachypnea, presence of crackles on both lung fields and
Short Term: After 3 hours of nursing interventions the patient will demonstrate appropriate coping behaviors and methods to improve breathing pattern.
Long term:
After 1 to 2
- Establish rapport - Monitor and record vital signs
- Assess breath sounds, respiratory rate, depth and rhythm
- Elevate head of the pt.
- Provide relaxing
- To gain pt/ SO’s trust and cooperation - To obtain baseline data
- To note for respiratory abnormalities that may indicate early respiratory compromise and hypoxia
- To promote lung expansion
Short Term: The patient shall have demonstrated appropriate coping behaviors and methods to improve breathing pattern.
Long term:
The patient shall have applied

muscles RR of 28
The patient may manifest the following:
Cyanosis Orthopnea Diaphoresis
dyspneadays of nursing interventions, the patient would be able to apply techniques that would improve breathing pattern and be free from signs and symptoms of respiratory distress.
environment
- Administer supplemental oxygen as ordered
-Assisst client in the use of relaxation technique
- Administer prescribed medications as ordered
-Maximize respiratory effort with good posture and effective use if accessory muscles.
-Encourage adequate rest periods between activities
- To promote adequate rest periods to limit fatigue
- To maximize oxygen available for cellular uptake
-To provide relief of causative factors
- For the pharmacological management of the patient’s condition
-To promote wellness
- to limit fatigue
techniques that improved breathing pattern and be free from signs and symptoms of respiratory distress AEB respiratory rate within normal range, absence of cyanosis, effective breathing and minimal use of accessory muscles during breathing.
2 Impaired Gas Exchange
Impaired gas exchange is a state in which there is excess or deficit oxygenation and carbon dioxide elimination. The compensatory mechanism of lungs is to lose effectiveness of its defense mechanisms and allow organisms to penetrate the sterile lower respiratory tract where inflammation develops. Disruption of mechanical defenses and ciliary motility leads to colonization of lungs and subsequent infection. Inflamed and fluid-filled alveolar sacs cannot exchange oxygen and carbon dioxide effectively. The release of endotoxins by the microbes can lodge in the brain, affecting the respiratory center in medulla resulting to altered oxygen supply.
AssessmentNursing Diagnosis
PlanningNursing Inter-ventions
RationaleExpected Outcome

Subjective: (none) Objective:
The patient manifested
Several episodes of pallor
Tachypnea
Restlessness
nasal flaring
depth of breathing
Use of accessory muscles for breathing
The pt. may manifest the ff:
Confusion
Cyanosis
Diaphoresis
Impaired Gas Exchange R/T Alveolar –Capillary Membrane Changes and respiratory fatigue Secondary to Pleural Effusion
Short term: After 1 hour of nursing interventions, the pt will verbalize understanding of the interventions given to improve patient’s condition.
Long term:
After 1-2 days of nursing interventions, the pt. will demonstrate improved ventilation and adequate oxygenation of tissues AEB absence of symptoms of respiratory distress.
- Establish rapport - Monitor and record vital signs
- Monitor respiratory rate, depth and rhythm
- Assess pt’s general condition
- Auscultate breath sounds, note areas of decreased/adventitious breath sounds as well as fremitus
- Elevate head of the pt.
- Note for presence of cyanosis
-Encourage frequent position changes and deep-breathing exercises
-Provide supplemental oxygen at lowest concentration indicated by laboratory results and client symptoms/ situation
- Review laboratory results
- Provide health teaching on how to alleviate pt’s condition
Administer prescribed medications as
- To gain pt./SO’s trust and cooperation - To obtain baseline data
- To assess for rapid or shallow respiration that occur because of hypoxemia and stress
- To note for etiology precipitating factors that can lead to impaired gas exchange
-To evaluate degree of compromise
- To enhance lung expansion
- To assess inadequate systemic oxygenation or hypoxemia
-To promote optimum chest expansion
To correct/ improve existing deficiencies
- To determine pt’s oxygenation
Short term: The patient shall have verbalized understanding of the interventions given to improve patient’s condition.
Long term:
The patient shall manifest no signs of respiratory distress.

ordered status
- To empower SO and pt
For the pharmacological management of the patient’s condition
3 Activity Intolerance
Presence of a space-occupying liquid in the pleural space, the lung recoils, inward, the chest wall recoils outward, and the diaphragm is depressed inferiorly. This may lead to decrease lung volume and may result to significant hypoxemia and can only be relieved by thoracentesis. Due to inadequate ventilation there would be limitations in activity as tolerance to activity may occur.
Assessment
Nursing Diagnosis
PlanningNursing Inter-ventions
RationaleExpected Outcome
Subjective: (none)
Objective:
Patient manifested:
generalized weakness
limited range of motion as observed
use of accessory muscles during breathing
(+) DOB
Activity intolerance related to insufficient oxygen for activities of daily living
Short Term: After 3-4 hours of nursing interventions, the patient will use identified techniques to improve activity intolerance
Long Term:
After 2-3 days of nursing interventions, the patient will report measurable increase in activity
Establish Rapport Monitor and record Vital Signs
Assess patient’s general condition
Adjust client’s daily activities and reduce intensity of level. Discontinue activities that cause undesired psychological changes
Instruct client in unfamiliar activities and in alternate ways of conserve energy
Encourage patient to have adequate bed rest and sleep
To gain clients participation and cooperation in the nurse patient interaction To obtain baseline data
To note for any abnormalities and deformities present within the body
To prevent strain and overexertion
Short Term: The patient shall have used identified techniques to improve activity intolerance
Long Term:
The patient shall have reported measurable increase in activity intolerance.

intolerance. Provide the patient with a calm and quiet environment
Assist the client in ambulation
Note presence of factors that could contribute to fatigue
Ascertain client’s ability to stand and move about and degree of assistance needed or use of equipment
Give client information that provides evidence of daily or weekly progress
Encourage the client to maintain a positive attitude
Assist the client in a semi-fowlers position
Elevate the head of the bed
Assist the client in learning and demonstrating appropriate safety measures
Instruct the SO not to leave the client unattended
Provide client with a
To conserve energy and promote safety
to relax the body
to provide relaxation
to prevent risk for falls that could lead to injury
fatigue affects both the client’s actual and perceived ability to participate in activities
to determine current status and needs associated with participation in needed or desired activities
to sustain motivation of client
to enhance sense of well being
to promote easy

positive atmosphere
Instruct the SO to monitor response of patient to an activity and recognize the signs and symptoms
breathing
to maintain an open airway
to prevent injuries
to avoid risk for falls
to help minimize frustration and rechannel energy
to indicate need to alter activity level
4 Acute Pain
Pain may be considered as Pleuritic chest pain. Pleuritic chest pain derives from inflammation of the parietal pleura, the site of pleural pain fibers. Occasionally, this symptom is accompanied by an audible or palpable pleural rub, reflecting the movement of abnormal pleural tissues.
AssessmentNursing Dx
PlanningNursing Inter-ventions
RationaleExpected Outcome
Subjective: (none)
Objective:
Patient manifested:
(+) DOB
Complains to chest pain on the
Acute pain
Short Term: After 3-4 hours of nursing interventions, the patient’s pain will decrease from 7 to 3 as verbalized by the patient.
Assess patient pain for intensity using a pain rating scale, for location and for precipitating factors. Assess the response to medications every 5
To identify intensity, precipitating factors and location to assist in accurate diagnosis. Assessing response determines effectiveness of medication and whether further interventions are
Short Term: Patient shall have verbalized a decrease in pain from a scale of 7 to 3.
Long Term:
The patient shall have

thoracostomy site
Facial grimaces upon movement
Reports of pain on the thoracostomy area, described as sharp provoked by breathing non-radiating, with a pain scale of 7 out of 10
Patient may manifest:
Restlessness
Confusion
Irritability
Long Term:
After 2-3 days of nursing interventions, the patient will demonstrate activities and behaviors that will prevent the recurrence of pain.
minutes
Provide comfort measures.
Establish a quiet environment.
Elevate head of bed.
Monitor vital signs, especially pulse and blood pressure, every 5 minutes until pain subsides.
Teach patient relaxation techniques and how to use them to reduce stress.
required.
To provide nonpharmacological pain management.
A quiet environment reduces the energy demands on the patient.
Elevation improves chest expansion and oxygenation.
Tachycardia and elevated blood pressure usually occur with angina and reflect compensatory mechanisms secondary to sympathetic nervous system stimulation.
Anginal pain is often precipitated by emotional stress that can be relieved non-pharmacological measures such as relaxation.
demonstrated activities and behaviors that will prevent the recurrence of pain.
Other nursing diagnoses:
5 Impaired Skin Integrity RT Surgical Procedure [Thoracentesis] 6 Disturbed Body Image RT Insertion of Chest Thoracostomy Tube