5. topical
3
Journal of Dermatological Treatment, 2014; 25: 97–99 © 2014 Informa Healthcare USA on behalf of Informa UK Ltd. ISSN: 0954-6634 print / 1471-1753 online DOI: 10.3109/09546634.2013.852297 EDITORIAL Topical antibiotic monotherapy prescribing practices in acne vulgaris William D Hoover 1 , Scott A Davis 1 , Alan B Fleischer 1 , & Steven R Feldman 1,2,3 1 Center for Dermatology Research, Departments of Dermatology, Wake Forest School of Medicine, Medical Center Boulevard, Winston-Salem, NC 27157-1071, USA, 2 Center for Dermatology Research, Departments of Pathology, Wake Forest School of Medicine, Medical Center Boulevard, Winston-Salem, NC 27157-1071, USA and 3 Public Health Sciences, Wake Forest School of Medicine, Winston-Salem, North Carolina, USA Abstract Objective: The aim of this study is to evaluate the frequency of dosing topical antibiotics as monotherapy in the treatment of acne vulgaris, and physician specialty prescribing these medications. Methods: This study is a retrospective review of all visits with a sole diagnosis of acne vulgaris (ICD-9-CM code 706.1) found on the National Ambulatory Medical Care Survey (NAMCS) in 1993–2010. We recorded the number of visits surveyed where acne vulgaris was the sole diagnosis, number of visits where topical antibiotics were the only treatment prescribed, and the specialty of physician in each encounter. Results: Topical erythromycin or clindamycin were the sole medication prescribed in 0.81% of the visits recorded, with 60% of these prescriptions arising from dermatologists and 40% from non-dermatologists. The trend of prescribing topical antibiotic monotherapy is declining (p < 0.001) over the 18-year study period. Conclusions: The development of resistance of Propionibacterium acnes to topical antibiotic regimens has led to the need to re-evaluate the use of topical antibiotics in the treatment of acne vulgaris. While the rate of topical antibiotic monotherapy is declining, their use should be reserved for situations where the direct need for antibiotics arises. If a clinician feels that antibiotics are a necessary component to acne therapy, they should be used as part of a combination regimen. Key words: erythromycin, clindamycin, antibiotic resistance, practice gap, NAMCS Introduction Topical regimens for acne have traditionally targeted multiple points in the pathogenesis, including the use of topical antibiotics such as erythromycin and clindamycin to address the role of Propionibacterium acnes (P. acnes) (1). Unfortunately, over time bacterial resistance develops when topical antibiotics are used as a sole treatment (2). Given the problems of resistant bacteria and given the avail- ability of many other treatment options, should topical antibiotics ever be prescribed as a monotherapy for acne? Topical antibiotics can be administered concurrently with benzoyl peroxide to decrease the rate of developing resistance, or other options (topical retinoids, other combination regimens) could be used to avoid the use of topical antibiotics alone (3). The purpose of this study is to determine how frequently topical erythromycin and topical clindamycin are used as monotherapy for acne. Methods The National Ambulatory Medical Care Survey (NAMCS) is a nationally representative database documenting physician visits, diagnoses, and prescribing habits from physicians who are not federally employed. The database was sampled in regards to visits in which the sole diagnosis of acne vulgaris (ICD-9-CM code 706.1) was made in the span from 1993 to 2010. Information collected included physician specialty (dermatology vs. non-der- matology) as well as medication prescribed (topical clindamycin or erythromycin monotherapy vs. other). The data were analyzed to determine the frequency of topical antibiotics as monotherapy for acne vulgaris, the trends in prescribing of topical antibiotics with or without benzoyl peroxide over the 18-year period, and differences in prescribing habits between dermatologists and non- dermatologists. We examined the use of topical antibiotics (clin- damycin, erythromycin, sulfacetamide, or dapsone) together with or without benzoyl peroxide, either in a combination product or as separate products. All data analysis was performed using SAS 9.2 (SAS Institute, Cary, NC), and the study was declared exempt by the Wake Forest Baptist Hospital Institutional Review Board. Results Acne vulgaris was the sole diagnosis made in an estimated 69 million visits. Of these visits, topical erythromycin or clin- damycin was the sole prescribed medication in 560 000 visits (0.81%), with 336 000 (60%) of the prescriptions from dermatol- ogists and 224 000 (40%) from non-dermatologists. Over time the frequency of topical antibiotic monotherapy for acne vulgaris has declined (p < 0.001), while the frequency of topical antibiotic therapy combined with benzoyl peroxide had increased (Figures 1 and 2). Discussion Over time, antibiotics become less effective as bacteria develop the means to evade destruction. As bacteria become resistant, they are able to induce resistance in other bacteria by transferring plasmids containing the resistance trait, rendering an antibiotic therapy ineffective for more than just the initial condition (4,5). While topical antibiotics were effective for acne in the past, the growing development of resistance is decreasing their effectiveness and raising concern that use for a common problem like acne could result in more widespread resistance issues. Correspondence: Scott A. Davis, MA, Department of Dermatology, Wake Forest School of Medicine, Medical Center Boulevard, Winston-Salem, NC 27157-1071, USA. Tel: +1 336 716 2702, Fax: +1 336 716 7732, E-mail: [email protected] (Accepted 3 October 2013) J Dermatolog Treat Downloaded from informahealthcare.com by Memorial University of Newfoundland on 08/01/14 For personal use only.
-
Upload
lodewyk-kefas-joshoa -
Category
Documents
-
view
10 -
download
0
description
ok
Transcript of 5. topical

Journal of Dermatological Treatment, 2014; 25: 97–99© 2014 Informa Healthcare USA on behalf of Informa UK Ltd.ISSN: 0954-6634 print / 1471-1753 onlineDOI: 10.3109/09546634.2013.852297
EDITORIAL
Topical antibiotic monotherapy prescribing practices in acne vulgaris
William D Hoover1, Scott A Davis1, Alan B Fleischer1, & Steven R Feldman1,2,3
1Center for Dermatology Research, Departments of Dermatology, Wake Forest School of Medicine, Medical Center Boulevard, Winston-Salem,NC 27157-1071, USA, 2Center for Dermatology Research, Departments of Pathology, Wake Forest School of Medicine, Medical CenterBoulevard, Winston-Salem, NC 27157-1071, USA and 3Public Health Sciences, Wake Forest School of Medicine, Winston-Salem, North Carolina,USA
AbstractObjective: Theaimof this study is toevaluatethefrequencyofdosingtopical antibiotics asmonotherapy in the treatment of acne vulgaris,andphysician specialtyprescribing thesemedications.Methods: Thisstudy isa retrospective reviewofall visitswithasolediagnosisofacnevulgaris (ICD-9-CM code 706.1) found on the National AmbulatoryMedicalCareSurvey(NAMCS)in1993–2010.Werecordedthenumberofvisits surveyedwhereacnevulgariswas thesolediagnosis,numberofvisitswhere topical antibioticswere theonly treatmentprescribed,and the specialty of physician in each encounter. Results: Topicalerythromycin or clindamycin were the sole medication prescribed in0.81% of the visits recorded, with 60% of these prescriptions arisingfromdermatologists and40%fromnon-dermatologists. The trendofprescribing topical antibiotic monotherapy is declining (p < 0.001)over the 18-year study period. Conclusions: The development ofresistance of Propionibacterium acnes to topical antibioticregimens has led to the need to re-evaluate the use of topicalantibiotics in the treatment of acne vulgaris. While the rate oftopical antibiotic monotherapy is declining, their use should bereserved for situations where the direct need for antibiotics arises.If a clinician feels that antibiotics are a necessary component to acnetherapy, they should be used as part of a combination regimen.
Key words: erythromycin, clindamycin, antibiotic resistance,practice gap, NAMCS
IntroductionTopical regimens for acne have traditionally targeted multiplepoints in the pathogenesis, including the use of topical antibioticssuch as erythromycin and clindamycin to address the role ofPropionibacterium acnes (P. acnes) (1). Unfortunately, over timebacterial resistance develops when topical antibiotics are used as asole treatment (2).
Given the problems of resistant bacteria and given the avail-ability of many other treatment options, should topical antibioticsever be prescribed as a monotherapy for acne? Topical antibioticscan be administered concurrently with benzoyl peroxide todecrease the rate of developing resistance, or other options(topical retinoids, other combination regimens) could be usedto avoid the use of topical antibiotics alone (3). The purpose ofthis study is to determine how frequently topical erythromycinand topical clindamycin are used as monotherapy for acne.
MethodsThe National Ambulatory Medical Care Survey (NAMCS) is anationally representative database documenting physician visits,diagnoses, and prescribing habits from physicians who are notfederally employed. The database was sampled in regards to visitsin which the sole diagnosis of acne vulgaris (ICD-9-CM code706.1) was made in the span from 1993 to 2010. Informationcollected included physician specialty (dermatology vs. non-der-matology) as well as medication prescribed (topical clindamycinor erythromycin monotherapy vs. other). The data were analyzedto determine the frequency of topical antibiotics as monotherapyfor acne vulgaris, the trends in prescribing of topical antibioticswith or without benzoyl peroxide over the 18-year period, anddifferences in prescribing habits between dermatologists and non-dermatologists. We examined the use of topical antibiotics (clin-damycin, erythromycin, sulfacetamide, or dapsone) together withor without benzoyl peroxide, either in a combination product oras separate products. All data analysis was performed using SAS9.2 (SAS Institute, Cary, NC), and the study was declared exemptby the Wake Forest Baptist Hospital Institutional Review Board.
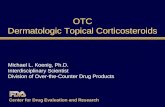
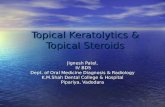
ResultsAcne vulgaris was the sole diagnosis made in an estimated69 million visits. Of these visits, topical erythromycin or clin-damycin was the sole prescribed medication in 560 000 visits(0.81%), with 336 000 (60%) of the prescriptions from dermatol-ogists and 224 000 (40%) from non-dermatologists. Over time thefrequency of topical antibiotic monotherapy for acne vulgaris hasdeclined (p < 0.001), while the frequency of topical antibiotictherapy combined with benzoyl peroxide had increased (Figures 1and 2).
DiscussionOver time, antibiotics become less effective as bacteria develop themeans to evade destruction. As bacteria become resistant, they areable to induce resistance in other bacteria by transferring plasmidscontaining the resistance trait, rendering an antibiotic therapyineffective for more than just the initial condition (4,5). Whiletopical antibiotics were effective for acne in the past, the growingdevelopment of resistance is decreasing their effectiveness andraising concern that use for a common problem like acne couldresult in more widespread resistance issues.
Correspondence: Scott A. Davis, MA, Department of Dermatology, Wake Forest School of Medicine, Medical Center Boulevard, Winston-Salem, NC27157-1071, USA. Tel: +1 336 716 2702, Fax: +1 336 716 7732, E-mail: [email protected]
(Accepted 3 October 2013)
J D
erm
atol
og T
reat
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mem
oria
l Uni
vers
ity o
f N
ewfo
undl
and
on 0
8/01
/14
For
pers
onal
use
onl
y.

While P. acnes has been implicated in the pathogenesis of acnevulgaris implying the need for antibiotics, recent data finds thatinflammation plays a much larger role in acne than previouslyunderstood (1,4). For this reason, a treatment that focuses moreon combating inflammation rather than, or in addition to, alimited antibiotic strategy should be considered (6).
If it is strongly felt, or preferred, by the physician for topicalantibiotics to be a part of the treatment regimen for acne vulgaris,the concurrent use of benzoyl peroxide decreases the risk ofresistance development (7–9). Do we need topical antibioticmonotherapy products? Topical benzoyl peroxide in a combina-tion treatment with a topical antibiotic is more effective ateliminating P. acnes and treating acne vulgaris than treatmentwith either topical benzoyl peroxide or topical antibiotics alone(10,11). However, the potential reduction in adherence with themore complex two-drug regimen could offset the potential ther-apeutic gain. Given the potential for poor adherence in patientswith acne, use of combination topical benzoyl peroxide–clinda-mycin as a single product (available as a generic) or use of abenzoyl peroxide-retinoid product may be appropriate.
Given the development of resistance as well as the efficacies ofother treatment options for acne, perhaps avoiding use topicalantibiotic monotherapy in acne could be considered as a qualitymetric for dermatology.
AcknowledgmentFinancial disclosure: The Center for Dermatology Research issupported by an unrestricted educational grant from Galderma
Laboratories, L.P. S R Feldman is a consultant and speaker forGalderma, Connetics, Abbott Labs, Warner Chilcott, Centocor,Amgen, Photomedex, Genentech, BiogenIdec, and Bristol MyersSquibb. S R Feldman has received grants from Galderma, Con-netics, Astellas, Abbott Labs, Warner Chilcott, Centocor, Amgen,Photomedex, Genentech, BiogenIdec, Coria, Pharmaderm, OrthoPharmaceuticals, Aventis Pharmaceuticals, Roche Dermatology,3M, Bristol Myers Squibb, Stiefel, GlaxoSmithKline, and Novartisand has received stock options from Photomedex. A B Fleischerhas received support for research, speaking, or consulting fromAstellas, Centocor, Amgen, Abbott, Galderma, Stiefel, Medicis,and Intendis and is employed by Merz Pharmaceuticals. W DHoover and S A Davis have no conflicts to disclose.
Declaration of interest: The authors report no conflicts ofinterest. The authors alone are responsible for the content andwriting of the paper.
References1. Beylot C, Auffret N, Poli F, et al. Propionibacterium acnes: an update
on its role in the pathogenesis of acne. J Eur Acad Dermatol Venereol.2013;10, http://www.ncbi.nlm.nih.gov/pubmed/?term=23905540.
2. Leyden JJ, McGinley KJ, Cavalieri S, Webster GF, Mills OH,Kligman AM. Propionibacterium acnes resistance to antibiotics inacne patients. J Am Acad Dermatol. 1983;8:41–45.
3. Eady EA, Farmery MR, Ross JI, Cove JH, Cunliffe WJ. Effects ofbenzoyl peroxide and erythromycin alone and in combination againstantibiotic-sensitive and -resistant skin bacteria from acne patients. Br JDermatol. 1994;131:331–336.
1992Rat
io o
f an
tib
ioti
c-b
enzo
yl p
erox
ide
co
mb
inat
ion
to
an
tib
ioti
c al
on
e
1994 1996 1998 2000 2002 2004 2006 2008 20100
0.5
1
1.5
2
2.5
3
3.5
4
Figure 2. Ratio of prescriptions for topical antibiotics and benzoyl peroxide combined compared to topical antibiotics alone over time. Points are plotted for3-year intervals (1993–1995, 1996–1998, 1999–2001, 2002–2004, 2005–2007, and 2008–2010).
1990 1995 2000 2005 2010
Topical antibioticwith BPOTopical antibioticw/o BPO
Per
cen
t o
f vi
sits
0
5
10
15
20
25
Figure 1. Rates of physician visits with a diagnosis of acne where topical antibiotic and benzoyl peroxide combination is prescribed and visits where topicalantibiotics without benzoyl peroxide is prescribed. Points are plotted for 3-year intervals (1993–1995, 1996–1998, 1999–2001, 2002–2004, 2005–2007, and2008–2010).
W. D. Hoover et al.
J D
erm
atol
og T
reat
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mem
oria
l Uni
vers
ity o
f N
ewfo
undl
and
on 0
8/01
/14
For
pers
onal
use
onl
y.

4. Schafer F, Fich F, Lam M, Garate C, Wozniak A, Garcia P. Antimicrobialsusceptibility and genetic characteristics of Propionibacterium acnesisolated from patients with acne. Int J Dermatol. 2013;52:418–425.
5. Kircik LH. The role of benzoyl peroxide in the new treatment paradigmfor acne. J Drugs Dermatol. 2013;12:s73–s74.
6. McKeage K, Keating GM. Clindamycin/benzoyl peroxide gel (Benza-Clin): a review of its use in the management of acne. Am J ClinDermatol. 2008;9:193–204.
7. Zeichner JA. Optimizing topical combination therapy for the treat-ment of acne vulgaris. J Drugs Dermatol. 2012;11:313–317.
8. Kinney MA, Yentzer BA, Fleischer AB Jr, Feldman SR. Trends in thetreatment of acne vulgaris: are measures being taken to avoid anti-microbial resistance? J Drugs Dermatol. 2010;9:519–524.
9. Gamble R, Dunn J, Dawson A, et al. Topical antimicrobial treatment ofacne vulgaris: an evidence-based review. Am J Clin Dermatol. 2012;13:141–152.
10. Simonart T. Newer approaches to the treatment of acne vulgaris. Am JClin Dermatol. 2012;13:357–364.
11. Whitney KM, Ditre CM. Management strategies for acne vulgaris. ClinCosmet Investig Dermatol. 2011;4:41–53.
Topical antibiotic monotherapy prescribing practices in acne vulgaris
J D
erm
atol
og T
reat
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mem
oria
l Uni
vers
ity o
f N
ewfo
undl
and
on 0
8/01
/14
For
pers
onal
use
onl
y.