5 scanning for dvt
56
1 DVT ultrasound SAH & RNSH 2011 Critical Care Ultrasound Course Thanks to Cindy Lucas… and yet again to Daniel Lichtenstein
-
Upload
nswhems -
Category
Health & Medicine
-
view
7.121 -
download
2
description
Scanning for DVT
Transcript of 5 scanning for dvt

1
DVT ultrasoundSAH & RNSH 2011
Critical Care Ultrasound CourseThanks to Cindy Lucas… and yet again to
Daniel Lichtenstein

DVT! Anatomy ! Below knee DVT?! Compression US:
! Technique! Sites
! What the scan can tell you! Pitfalls

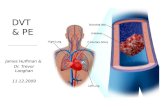
Anatomy of the deep veins

Anatomy of the deep veins
Below the knee!Anterior tibial!Posterior tibial!Peroneal!Gastrocnemial!Soleal
!Variable !Paired !Tricky!!Relevance of DVT?
Above the knee! Popliteal Vein in popliteal
fossa! From confluence of 3 calf
veins! To adductor canal! (Superficial) Femoral! Profunda Femoris joins
4cm below inguinal ligament
! Common Femoral! Long/ great saphenous

Here’s the problem
It would be nice to scan the below knee veins
!Incr sensitivity!Incr accuracy
!Variable !Paired !Tricky!!Relevance of DVT?
But it’s hard!! Variable! Paired! Tiny! Tricky! And most of them don’t
ermbolize! (But some do…)

6
Previous top tip: just look for above knee
Leave the calves to the sonographers!

But Lichtenstein came up with a solution
! Except for the anterior tibials, the below knee veins travel all in a line, a couple cm below the interosseous membrane
! together with their arteries: 2 veins for each artery = 6 vessels, all lined up
! We can see them from the front of the leg!! Probe between the tibia & fibula

8
Now we have 2 options
1. Just above knee: leave the calves to the sonographers!
2. Below knee (anterior approach)

9
DVT scan:Technique

Probe & preset?
! Ideally linear probe / vein preset! But curved probe / FAST preset works
too! Don’t need Doppler

Compression US
! Probe in transverse position! Just squash the vein!! If it squashes easily & completely, there
is no DVT! If it doesn’t, there’s a DVT



Normal veins ! Completely compressible! Press hard enough to just indent the
artery

Features of DVT! Gold standard sign: vein not completely
compressible! You might see thrombus! Vein might fail to augment on Doppler

16
Test

DVT?

DVT?

DVT?

DVT?

DVT?

DVT?

DVT?

Compression US! Pros ! Easy! Rapid ! B mode only! 98% sensitive
Cons! Misses external iliac
DVT! Misses small non-
occlusive DVT

23
Which sites can I compress?

Which sites can I compress?
! Internal Jugular V! Subclavian V! IVC! Saphenofemoral confluence (up fem)! Lower (superf) femoral near adductor hiatus! Long saphenous V! Short saphenous V! Popliteal vein & trifurcation! Beloe knee veins

Which sites should I compress?
! Up to you! The more veins you scan, the more sensitive
you are… eg UL veins add 4% in PE! The fewer you scan, the less irritating it is! 3-point scan is reasonable
1. Upper femoral (confluence)2. Lower femoral (near adductor hiatus)3. Popliteal (irritating if supine) …or …below knee
(weird at first)

1: Groin
! Probe in transverse position! Start just below inguinal ligament! ‘Mickey Mouse’ sign
! Femoral A! Saphenofemoral confluence! Then compress






2: insertion of LSV / GSV

2: insertion of LSV / GSV

3: fem V just above knee
! Adductor hiatus! Medial to the bone ! Hand behind, presses forward







4: popliteal fossa
! Lie patient on side, or lift leg! Popliteal vein
! Superficial to popliteal artery! visualise bone beneath! follow it to the trifurcation






5: below the knee
! Supine patient! Probe transverse! Between tibia & fibula




Handy Hints as you go down the leg
1. Decrease greyscale (dynamic range)2. Decrease frequency3. Increase depth as you go4. Obese: change to curved probe5. Sit with legs over bed / stand up6. Valsalva (humming works)7. Doppler …

Pitfalls
! Duplicate venous systems (duplex popliteal up to 35%)
! Non occlusive thrombus! LSV, SSV! Ant tibial veins! However … ‘90% = 100%’

One more time: Handy Hints ! You don’t need Doppler! You don’t need linear probe! But you won’t be 100%! Below-knee isn’t that hard! Sitting up / standing! Valsalva (humming works)

DVT US: Summary
! Compression US! Groin ! Just above knee! Below knee