Iliofemoral DVT thrombolysis
36
ILIOFEMORAL DVT THROMBOLYSIS: A NEW STANDARD OF CARE? JK WICKS WELLINGTON HOSPITAL WELLINGTON, NZ
-
Upload
specialistveinhealth -
Category
Health & Medicine
-
view
658 -
download
2
Transcript of Iliofemoral DVT thrombolysis

ILIOFEMORAL DVT THROMBOLYSIS: A NEW STANDARD OF CARE?
JK WICKSWELLINGTON HOSPITAL WELLINGTON, NZ

DVT Intervention:
2 |
• Current Methods of DVT Treatment
• What is PTS and how does it impact the patient, physician and hospital?
• Current DVT treatment guideline changes that may affect current hospital protocols
• Clinical and observational studies supporting rationale for early thrombus removal
• Discuss pharmacomechanical thrombolysis

DVT – “A National Crisis...”U.S. Surgeon General, 2008
• >600,000 Americans are diagnosed with Venous Thromboembolism (VTE) annually3
• VTE is the leading cause of preventable hospital death4 (DVT and PE)
• Deep Vein Thrombosis is the third most common cardiovascular disease3
• 17.9% DVT patients will suffer recurrent VTE within 3 years (DVT/PE)2
• As many as two thirds of all DVT patients will develop Post Thrombotic Syndrome (PTS)1
• U.S. spends upwards of $2.4B to treat DVT annually1
3 |Image courtesy of Anthony J. Comerota, MD

AnticoagulationTherapy
Systemic Thrombolysis
Catheter Directed
Thrombolysis
Pharmaco-mechanical
Thrombolysis
IsolatedPharmaco-mechanical
Thrombolysis
30 Years
30 Years
Evolution of DVT Treatment Options
4 |
19501980
19902000
TODAY

Anticoagulation Alone . . .
…does prevent clot propagation1.
…does reduce risk of pulmonary embolism.
But, it typically…
…does NOT resolve clot.16
…does NOT rapidly resolve symptoms.16
…does NOT prevent PTS (Post Thrombotic Syndrome).9
5 |

Post-Thrombotic Syndrome (PTS)
• Chronic medical condition that may follow DVT due to valve destruction and venous obstruction
• Symptoms may include: • Persistent edema• Pain• Purpura (bleeding into the skin)• Increased skin pigmentation• Itchiness• Cellulitis• Venous stasis ulcers
6
Chronic Ulcers

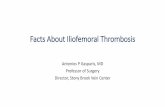
How Post Thrombotic Syndrome Develops
7 |Impairs a patient’s activities of daily living, work performance and
treatment satisfaction (QOL)6
Post Thrombotic Syndrome develops16
Venous insufficiency, hypertension, and reflux contribute to stasis and re-thrombosis16
Residual thrombus propagates until symptomatic again
Post DVT residual thrombus leads to valvular damage

Post Thrombotic Syndrome Sequelae
8 |
Represents a
permanent disability
40-60% of proximal DVT patients
eventually develop PTS6
4% - 8% of patients with PTS will
develop severe symptoms such as
ulcers and skin deterioration5
75% of the cost of treating DVT is related to PTS6
PTS has a lower QOL score than
conditions such as chronic lung disease
and angina6
Kahn SR, Shrler I, Julian JA, Ducruet T, Arsenault, L, Determinants and Time Course of the Postthrombotic Syndrome after Acute Deep Vein Thrombosis, Ann Intern Med. 2008;149:698-
707.

Post Thrombotic Syndrome Long Term Evidence of PTS
9 |
Frequency of PTS with symptomatic DVT7
Follow up Incidence
1 Year 17.3%
2 Years 23%
5 Years 28%
8 Years 29%
Frequency of PTS with symptomatic DVT8
Follow up Incidence
5 years 47%
Frequency of PTS with symptomatic DVT9
Follow up Incidence
1 Year 27%

2004 ACCP DVT Intervention Guidelines
10 |
2004 ACCP guidelines recommended AGAINST thrombolytics for DVT, except for in the use of limb salvage.
ACCP recommend in patients with DVT against the regular use of catheter-directed thrombolysis .
In addition, the ACCP suggested that this treatment should only be considered in patients that are requiring limb salvage.10
© 2004 American College of Chest Physicians

2008 ACCP DVT Intervention Guidelines
11 |
Significant Changes in 2008 for DVT intervention. Thrombolytics are NOW SUGGESTED for acute, proximal DVT.
In the patient population with extensive acute proximal DVT* (eg, iliofemoral DVD, symptoms for < 14 days, good functional status, life expectancy of ≥ 1 year) who have a low bleeding risk, catheter-directed thrombolysis (CDT) is suggested by the ACCP to reduce acute symptoms and post-thrombotic morbidity* in settings where the right expertise and resources are available.
It is also suggested by the ACCP that Pharmacomechanical thrombolysis should be considered over CDT alone in order to shorten treatment time* in settings where the right expertise and resources are available.
When successful CDT has been completed in patients with acute DVT, the recommendation is to utilize the same intensity and duration of anticoagulation therapy as similar to those who do not receive thrombolysis.11
*Emphasis added.This summary not intended to be a substitute for the entire guidelines. Clinicians are advised to review the entire guidelines before deciding a course of action.

2011 American Heart Association Guidelines
•Summary of Recommendations for Endovascular Thrombolysis and Surgical Venous Thrombectomy
12 |*Emphasis added.This summary is not intended to be a substitute for the entire guidelines. Clinicians are advised to review the entire guidelines before deciding a course of action.
For Iliofemoral DVT patients with a low risk of bleeding, Catheter Directed Thrombolysis (CDT), or Pharmacomechanical Catheter Directed Thrombolysis (PCDT), is a reasonable first-line of treatment to achieve more rapid relief of current symptoms and to prevent Post-Thrombotic Syndrome (PTS) despite anticoagulation.1
Because PCDT generally reduces the amount of patient exposure to the thrombolytic drug, selecting PCDT over CDT may be reasonable in the majority of patients receiving endovascular thrombolysis. High risk patients of bleeding and with Chronic DVT (>21 days) should not be given PCDT or CDT.1

2012 SVS and AVF Guidelines • Indications for early thrombus removal: A strategy of early thrombus removal in selected
patients
• Following criteria (a) a first episode of acute iliofemoral deep venous thrombosis, (b) symptoms 14 days in duration, (c) a low risk of bleeding, and (d) ambulatory with good functional capacity and an acceptable life expectancy.
• Early thrombus removal strategies as the treatment of choice in patients with limb-threatening venous ischemia due to iliofemoral deep venous thrombosis with or without associated femoropopliteal venous thrombosis (phlegmasia cerulea dolens).
• Patients with isolated femoropopliteal deep venous thrombosis be managed with conventional anticoagulation therapy because there is currently insufficient evidence to support early thrombus removal strategies in this patient population.
• Techniques for early thrombus removal suggest percutaneous catheter-based techniques (pharmacologic or pharmacomechanical) as first-line therapy for early thrombus removal in patients meeting the criteria in 1.1. We suggest a strategy of pharmacomechanical thrombolysis be considered over catheter-directed pharmacologic thrombolysis alone if expertise and resources are available.
Mark H. Meissner et al, J Vasc Surg 2012;55:1449-62

Clinical Studies
•AbuRahma, Ali et al. (2001) Iliofemoral Deep Vein Thrombosis: Conventional Catheter Directed
Thrombolysis and Percutaneous Transluminal Angioplasty and Stenting.12
• 51 consecutive iliofemoral DVT patients at West Virginia University
• 33 treated with anticoagulation alone were 3% patent at one month and 30% symptom free at 1 year and 2 PEs occurred
• 18 treated with CDT +/- PTV and stent were 89% patent at one month and 83% symptom free at one year with no PEs
• No mortality difference
14 |

Clinical Studies•Elsharawy, M. and Elzayat, E. (2002) Early Results of Thrombolysis vs Anticoagulation in Iliofemoral
Venous Thrombosis.13
• 35 patients were randomized into anticoagulation alone (17) or thrombolysis
(18) groups
• 12% of patients treated with anticoagulation alone were patent at six months and 41% had signs of venous reflux
• 72% of patients treated with thrombolysis were patent and only 11% had signs of venous reflux
15 |

Catheter-Directed Thrombolysis for Iliofemoral DVT
16 |
Lysis Anticoag P-Value
Elsharawy et al13
Eur J Vasc Endovasc Surg 2002; 24:209(N=35) (6 month)
72% 12% <0.001
Enden et al18
J Thromb Haemost 2009; 7:1268(N=103) (6 month)
64% 36% 0.004
PatencyRandomized Studies

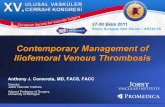
Outcome Measures after Iliofemoral DVT LysisClinical Study Results: Villalta Score Vs. Percent Lysis
17 |Grewal, P. et al. Quantity of clot lysed after catheter-directed thrombolysis for iliofemoral deep venous thrombosis correlates with postt-hrombotic morbidity. J Vasc Surg. 2010 May;51(5):1209-14
Greater clot lysis = less PTS
42 patients underwent catheter directed thrombolysis and/or pharmacomechanical thrombolysis. The percent of lysis was evaluated and patients were divided into 2 groups. Mean follow-up interval was 14 months.
Group 1 (n=33)> 50% Lysis
• CEAP Score: 0.85
• Villalta Scale: 2.38
Group 2 (n=9)< 50%
• CEAP Score: 3.13
• Villalta Scale: 6.25

Long-term outcome after additional catheter-directed thrombolysis versus standard treatment for acute iliofemoral deep vein thrombosis (the CaVenT study): A randomised controlled trial
•20 Hospitals
•Patient ages 18 – 75 with first time iliofemoral DVT
•Symptoms within first 21 days
•Randomized and double-blinded to CDT or Anticoagulation
•209 patients total
•108 control (anticoagulation)
•101 CDT
•Assessments:
•Patency at 6 months
•Villalta score at 24 months
Cavent Study

Cavent Study – Results• CDT Group
• 3 major & 5 clinically relevant Bleeds = ~ 8%• 20 total bleed complications = ~ 12% minor bleed rate• 6 month patency = 65.9%• 24 month PTS symptoms = 37 patients or 41.1%
• Control Group (Anticoagulation)
• No reported bleeds• 6 month patency = 47.4%• 24 month PTS symptoms = 55 patients or 55.6%
•Reduction in PTS at 2 years = 14.4%
“This randomized trial was the first to show a clinically significant reduction in PTS after additional CDT compared with
conventional treatment alone.”

Cavent Study: criticisms can we do better?• Increase risk and severity of PTS after proximal DVT
• High % of isolated femoral DVT treated• Residual thrombus correlates with recurrent DVT and increase
PTS• No analysis for treatment success and subsequent PTS
• Limited additional interventions• For residual thrombus• Underlying cause of obstruction (eg May Thurner syndrome)

ATTRACT Study: Rationale and DesignA multicenter randomized trial to evaluate pharmacomechanical catheter-directed thrombolysis (PCDT) for the prevention of postthrombotic syndrome in patients with proximal deep vein thrombosis• Purpose: To determine if PCDT should be routinely used to
prevent PTS in patients with symptomatic proximal DVT above the popliteal vein.
• Study Design:• Multicentered and randomized trial sponsored by the National
Heart Lung and Blood Institute (NHLBI)• Enrolling in the USA• Patient goal is approx. 700• 2/3 of patients are currently enrolled• Designed to test pharmacomechanical catheter-directed
thrombolysis in the treatment of acute DVT to reduce frequency of PTS
• Patients are randomized to receive PCDT + standard therapy vs standard therapy alone (anticoagulation and compression stockings)

Isolated Pharmacomechanical Thrombolysis (PMT) Offers More Effective Thrombus Removal in Less Time and is More Cost Effective than CDT
22 |
• Isolated Segmental Pharmacomechanical Thrombolysis offers more effective thrombus removal in less time and with a reduced dose of thrombolytic agent.*
**Daniel E. Hilleman, PharmDet al, Clinical and Economic Evaluation of the Trellis-8 Infusion Catheter for Deep Vein Thrombosis J Vasc Interv Radiol 2008; 19:377–383)
*Jorge L. Martinez Trabal, MD et al. The quantitative benefit of isolated, segmental, pharmacomechanical thrombolysis (ISPMT) for iliofemoral venous thrombosis. J Vasc Surg 2008;48:1532-7
• The rate of lysis success defined as more than 50% clot resolution was significantly greater for the pharmacomechanical thrombolysis than for Catheter Directed Thrombolysis.
• In addition, the time to achieve lysis was substantially shorter with the PMT than with CDT. The Trellis Infusion Catheter is approximately $1,775.00 less costly to use per patient compared with conventional Catheter Directed Thrombolysis.”**

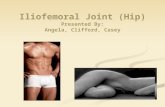
The Trellis Peripheral Infusion System
The Trellis™ system dissolves acute thrombus using isolation balloons, circumferential lytic delivery and oscillating dispersion wire. It is the only pharma-comechanical thrombolysis device that offers thrombus isolation and targeted, lytic delivery.

Balloon Inflation Ports
Oscillation Drive Unit (ODU) with Integrated Dispersion Wire
Infusion/Aspiration Port
Isolated Treatment Zone
8F Multi-LumenCatheter
The Trellis Peripheral Infusion System

The proximal and distal thrombus isolation balloons deliver targeted lytic therapy to minimize the risk of bleeding complications for better patient outcomes.
Isolate
The unique circumferential pattern of the infusion holes and consistent amplitude of the dispersion wire enhance lytic distribution for better dissolution of acute thrombus.
The aspiration window is designed to remove lytic and dissolved thrombus.
Dissolve
Aspirate
The Trellis Peripheral Infusion System

Isolate Thrombus with Unique Balloons
The proximal and distal thrombus isolation balloons deliver targeted lytic therapy to minimize the risk of bleeding complications for better patient outcomes.
Position proximal and distal to the treatment zone







Conclusions: Why Early Thrombus Removal is New Standard of Care
• DVT Treatment has progressed significantly over the last 60 years to include pharmacomechanical
thrombolysis, which is designed to minimize complications for iliofemoral DVT patients
• Post Thrombotic Syndrome is debilitating to the patient and can be severe and decreases quality of life
• Significant guideline changes now suggest the use of pharmacomechanical thrombolysis in proximal DVT
• Clinical studies show improved outcomes over anticoagulation alone:16
• Isolated Pharmacomechanical thrombolysis (Trellis) has benefit over CDT in time to lysis, decrease volume of lytic used and cost effectiveness
33 |

References1. Sharafuddin, M. et al. Endovascular Management of Venous Thrombotic and Occlusive Diseases of the Lower Extremities. J Vasc Interv Radiol 2003; 14:405-423.
2. Spencer FA et al. Patient Outcomes After Deep Vein Thrombosis and Pulmonary Embolism: The Worcester Venous Thromboembolism Study. Arch Intern Med. 2008; 168: 425-430.
3. Arko F. et al. Aggressive Percutaneous Mechanical Thrombectomy of Deep Vein Thrombosis . Arch Sung. 2007; 142: 513-519.
4. National Quality Forum. National Voluntary Consensus Standards for Prevention and Care of Venous Thromboembolism: Policy, Preferred Practices and Initial Performance Measures. 2008.
5. Nicolaides, A, et al. Prevention of Venous Thromboembolism. Int Angiol 1997; 16: (1) 3-38.
6. Kahn SR, Shrler I, Julian JA, Ducruet T, Arsenault, L, Determinants and Time Course of the Postthrombotic Syndrome after Acute Deep Vein Thrombosis , Ann Intern Med. 2008; 149: 698-707.
7. Prandoni, P, Lensing, AW, Prins, MH, et al. Below-Knee Elastic Compression Stockings to Prevent Post-Thrombotic Syndrome: A Randomized Controlled Trial. Ann Intern Med 2004; 141: 249-56.
8. Brandjes DP, Buller HR, Heijboer H, et al., Randomised trial of effect of compression stockings in patients with symptomatic proximal-vein thrombosis. Lancet 1997; 349(9054): 759-62.
9. Susan R. Kahn; Jeffrey S. Ginsberg (2004). Relationship Between Deep Venous Thrombosis and the Postthrombotic Syndrome. Arch Intern Med 2004; 164: 17-26.
10. Schünemann, Holger J. , Deborah Cook, Jeremy Grimshaw, Alessandro Liberati, John Heffner, Victor Tapson and Gordon Guyatt . Antithrombotic and Thrombolytic Therapy: From Evidence to Application: The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. CHEST 2004; 126;401S-428S.
11. Kearon , Clive, Susan R. Kahn, Giancarlo Agnelli, Samuel Goldhaber, Gary E. Raskob and Anthony J. Comerota. Antithrombotic Therapy for Venous Thromboembolic Disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition) Chest June 2008 133:6 suppl 454S-545S; doi:10.1378/chest.08-0658 .
12. AbuRahma, Ali F., MD, Samuel E. Perkins, MD, John T. Wulu, PhD, and Hong K. Ng, MD. Iliofemoral Deep Vein Thrombosis: Conventional Therapy Versus Lysis and Percutaneous Transluminal Angioplasty and Stenting. Annals of Surg 2001; 233: 752-760.
13. Elsharawy, M. And Elzayat, E. Early Results of Thrombolysis vs Anticoagulation in Iliofemoral Venous Thrombosis . A Randomised Clinical Trial. Eur J Vasc Endovasc Surg 2002; 24, 209-214.
14. Grewal, Nina K., MD, Jorge Trabal Martinez, MD, Linda Andrews, RN, and Anthony J. Comerota, MD. Quantity of Clot Lysed after Catheter-Directed Thrombolysis for Iliofemoral Deep Venous Thrombosis Correlates with Postthrombotic Morbidity. J Vasc Surg. 2010 May;51(5):1209-14
15. Comerota, AJ, D. Paolini .Treatment of Acute Iliofemoral Deep Venous Thrombosis: A Strategy of Thrombus Removal . Euro J of Endo Surg: 2007;351-360.
16. Comerota, AJ, Gravett, Marilyn H. Iliofemoral Venous Thrombosis. J Vasc Surg 2007; 46:1065-1076
• •
34 |

References
17. Jaff, Michael R., et al. Managment of Massive and Submassive Pulmonary Embolism, Iliofemoral Deep Vein Thrombosis, and Chronic Thromboembolic Pulmonary Hypertension: A Scientific Statement from the American Heart Association. J of the American Heart Assoc. Apr. 26th, 2011.
18. Enden T, et al. Catheter-directed thrombolysis vs. anticoagulant therapy alone in deep vein thrombosis: results of an open randomized, controlled trial reporting on short-term patency. Journal of Thrombosis and Haemostasis, 7: 1268–1275.
19. Plate G, Eklof B, Norgren L, Ohlin P, Dahlstrom, JA.Venous Thrombectomy for Iliofemoral Vein Thrombosis–10-year results of a Prospective Randomised Study. Eur J Vasc Endovasc Surg 1997;14:367-74 .
35 |

ILIOFEMORAL DVT THROMBOLYSIS: A NEW STANDARD OF CARE?
JK WICKSWELLINGTON HOSPITAL WELLINGTON, NZ