2.3 VIP Latrine Construction Project
28
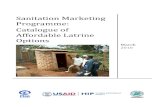
VIP Latrine Construction 2.3.1 Introduction and Case Study with Lessons Learnt Q: What is a VIP Latrine? How is it different from ordinary pit latrine? A: A VIP latrine is a latrine with concrete slab and pit lining with vent pipe; therefore it is more sanitary and safe latrine. It is different from SanPlat latrine, which has concrete slabs but neither vent nor lining and it can be used to improve an existing simple pit latrines. It is necessary to have a pit lining in some soil conditions to prevent collapse. Pipe is made by blocks (or asbestos pipe can be used) and a single VIP can last about 8 years for a family of average 6 people. Q: Why is VIP latrine needed for the community? A: Good sanitation, with good hygiene (i.e. hand washing), acts, as a fundamental “barrier” by ensuring that infection from faecal matter does not spread in the environment. Most of latrines in UUS are traditional pits that neither have vent pipe to control flies (See F-diagram left) nor proper pit lining to ensure safety. Therefore improvement of such existing latrines is recommended. Q: How does a VIP latrine work? A: The latrine slab has two holes, one for the squatting hole and the other for the vent pipe. The pipe sucks air from the pit and fresh air is drawn through the squatting hole. It makes latrine odourless. Flies approaching the latrine are attracted by odours from the pipe but cannot go through the screen into the pit. Those escaping from the latrine are attracted to the light coming down the pipe but are trapped by the screen and cannot escape. It controls both the smells and breaking the disease transmission cycle of flies from the latrine. The slab is reinforced concrete slab, that is strong & large enough to span a pit without log supports.The pit is lined with cement-mortared block, but perforated to allow liquids to escape. 2.3 VIP Latrine Construction Project F-diagram (transmission of disease from faeces) A VIP Latrine A-1-59
Transcript of 2.3 VIP Latrine Construction Project

VIP Latrine Construction
2QoAlshcIc(a
QAhfhltlabccwb
2.3 VIP Latrine Construction Project
.3.1 Introduction and Case Study with Lessons Learnt : What is a VIP Latrine? How is it different from
rdinary pit latrine? : A VIP latrine is a latrine with concrete slab and pit
ining with vent pipe; therefore it is more sanitary and afe latrine. It is different from SanPlat latrine, which as concrete slabs but neither vent nor lining and it an be used to improve an existing simple pit latrines. t is necessary to have a pit lining in some soil onditions to prevent collapse. Pipe is made by blocks or asbestos pipe can be used) and a single VIP can last bout 8 years for a family of average 6 people.
: How does a VIP latrine work? : The latrine slab has two holes, one for the squattingole and the other for the vent pipe. The pipe sucks airrom the pit and fresh air is drawn through the squattingole. It makes latrine odourless. Flies approaching the
atrine are attracted by odours from the pipe but cannot gohrough the screen into the pit. Those escaping from theatrine are attracted to the light coming down the pipe butre trapped by the screen and cannot escape. It controlsoth the smells and breaking the disease transmissionycle of flies from the latrine. The slab is reinforcedoncrete slab, that is strong & large enough to span a pitithout log supports.The pit is lined with cement-mortaredlock, but perforated to allow liquids to escape.
F-diagram (transmission of disease from faeces)
A-1-59
Q: Why is VIP latrine needed for the community? A: Good sanitation, with good hygiene (i.e. hand washing), acts, as a fundamental “barrier” by ensuring that infection from faecal matter does not spread in the environment. Most of latrines in UUS are traditional pits that neither have vent pipe to control flies (See F-diagram left) nor proper pit lining to ensure safety. Therefore improvement of such existing latrines is recommended.
A VIP Latrine

VIP Latrine Construction
Box 2.3.1 Experience from Bauleni and Chibolya
In December 1999, the baseline survey undertaken by JICA discovered that despite 88% of households surveyed had home
latrine of some kind, the majority were ordinary pit latrines that were either full or unsafely constructed. This led to their request
for technical transfer and provision of subsidy to build safe and sanitary latrines, like Ventilated Improved Pit (VIP) latrines.
The overall goal of this pilot project was to transfer skills of VIP to 20 Latrine Construction Group (LCG, trained community
based bricklayers but later named as LCG) members (10 from each settlement) and LCG then promote the VIP technology by
training others in the communities to construct targeted home VIP latrines (40 latrines in zone 8 & 13 in Bauleni and 2
demonstrative communal latrines both in Bauleni and Chibolya).
Prior to the implementation, the RDCs in both communities held meetings to identify community bricklayers, select type of
latrines most appropriate for construction. And an NGO, Africare conducted training of trainer’s (TOT) workshops, which were
divided into two parts, theoretical and practical. During the workshop, the LCG constructed demonstrative communal (public)
VIP latrine as part of their training. These demonstrative VIP latrines brought valuable practical lessons for the bricklayers
(LCGs). A manual for VIP latrine construction was developed after testing during the TOT.
JICA provided the Bauleni community with approximately 75% of the materials subsidy, such as cement, reinforcement bars
and fly screens while the beneficiaries contributed the remaining 25% of the supplies in the form of labour, water, and sand.
Analysis of the community contribution at the end of the study revealed that there were variations from 12 to 32% (some
residents paid extra costs for some contributions at their own cost and on their own initiative to build shower room and paint their
latrines). LCG, RDC and Health Educators (HEs) who began a sensitisation by drama performances and door-to-door campaign.
They also promoted and explained landlords about the benefits of VIP and their contribution.
In Bauleni, the project could not achieve target number of VIP latrine construction due to misuse of materials, some cements
damaged by the heavy rainfall and the failure to prepare river sand and labour cost on time by the beneficiaries. But the project
helped lower income households, and more than 90% of beneficiaries accepted the technology and a concept of community
contribution. Unsanitary condition and damage observed were less than 20% and some damages occurred because quality of sand
collected by the beneficiary was poor.
In Chibolya, the project supplied all the materials to construct a double pits demonstrative communal (public) VIP. At early
stage of demonstration, door rock was vandalised so that the community decided to purchase a much stronger security rock. It
now opens only during weekends for church members who pay user fee. It was suggested, after heavy rainfalls in 2001, that more
careful design is needed for those tough areas (rocky surface, high water table, flooding area during rainy season). Chibolya
LCGs constructed another six VIP latrines both within and outside the settlement without any subsidy. In addition to the lack of
fund, poor land conditions prevented others from increasing another latrines. Some lessons learnt were:
The special designs of latrine will need to be developed to overcome soil contamination and collapsing. Up-lifted VIP
structure and completely sealing the pit with cement or septic tank should be considered in difficult condition (See Annex 8)
RDC should be responsible for supervision of the work done by LCG and also responsible for logistics management of the
project to prevent misuse of materials and to achieve acceptable quality level of the latrine
Technician should check quality of the sand collected by beneficiaries to avoid damage/cracks
Both positive and negative effects of heavy rains should be considered when planning schedule and strategy (i.e. collecting
river sand, training and construction period)
The issues of incentives (payment for the skilled-labour) must be closely explored before initiation of the project
More low income beneficiaries would be benefited if 1) beneficiaries are provided enough time to prepare required
contribution, 2) landlords are legally enforced to build VIP, 3) contribution rate vary according to income level.
A-1-60

VIP Latrine Construction
2.3.2 HOW CAN WE PLAN? (STEP BY STEP)
1. Needs Assessment As sanitation is one of the biggest problems to people’s health in the urban settlements, it is necessary to confirm the prevailing problems perceived by the
people and to find out and gain consensus on the “main problems” of sanitation and hygiene. Also, prior to the planning and selecting appropriate design/technological options, stakeholders need to know and share basic information and situation of the area. It is suggested that household survey be conducted to get baseline data. (Example, See Table 2.3.1)
Table 2.3.1 Data to be Collected and Date Sources Data Data source
Epidemiological data (such as diarrhoea/Cholera incidence in the health centre of the catchments area)
1) Health Centres in charge 2) DHMT
Inventory of latrine technologies used previously Number of shallow-well users and identify their locations Number of landlords, tenants Community’s expressed demand for clean environment Knowledge on health/ hygiene issues Willingness to contribute to the projects Socio-cultural data (social history, gender roles, beliefs,
practices, cultural taboos) Training needs felt by the community and staffs at health
facility
1) Household 2) Knowledge Attitude Practice (KAP) survey (See P13 quantitative social survey) 3) Focus Group Discussions (FGD) 4) Direct Observation 5) Key Informant Interview
2. Identify supporting agencies and groups and set up a team It is important to know about existing ABOs working in the community and how to utilise and enhance capacities of such different groups. In the initial stage, existing community leaders like RDC, NHC and LCC site officers must play a leading role to identify existing groups and create and mobilise a new group like the Latrine Construction Group if required. Experienced NGO should also be identified at this stage.(See Fig. 2.3.1) 3. Conduct PHAST and/or CAP to analyse Problem and Plan for Solutions After identifying community’s problems/needs and stakeholders to implement the project, common hygiene and sanitation practices should be investigated deeply to design the project and for project appraisal, whether it fits with the policies, principles, values and priorities of the community and if it’s feasible. (See PHAST, CAP, page 11,14-15) CAP workshop aims to make strategies, prepare action plans and systems of monitoring and evaluation. The plan should identify the solutions and what actions need to be taken, when, how, by whom and also future actions to prevent or solve problem.
PLAN
A-1-61

VIP Latrine Construction
■ CHECKLIST FOR PLANNING Step Action Checkpoint
1.1 Collect data through Household, Knowledge Attitude Practice (KAP) survey, Focus Group Discussions (FGD), Direct Observation and Key Informant Interview (See PRA/PUA page 10, 11)
Ask Yourself; □From whom is the data to be collected? □Who is responsible for the data collection? □What is the use of the data collected? Who can use the results? □What methods will be used to gather data? □Collect data described in previous page
1.Needs Assessment
1.2 Collect data on government policies, goals and regulatory standard
□Check National/District goals through annual report at each level □ Check National/District standards on technology used for sanitation facilities
2.1 Identify key community stakeholders to work with (which organization/group can be active and sustainable for sanitation facility development)
□If it becomes necessary to form new groups or organisations, build upon what exists and created by other development projects as much as possible (women’s group, bricklayers group etc) □ Consider, gender, economics, and ethnicity balance within community to make sure the project is not captured and monopolized by local elites or any single faction
2.2 Identify which supporting agencies are effective and collaborative
□Identify active staffs of DHMT/LCC-DPH, such as EHTs, for technical advise, support and supervision □Identify NGO with experience of community participatory latrine construction in peri-urban settlements
2. Identify Supporting Agency and Groups and set up a team
2.3 Identify community bricklayers who can work as LCG (Latrine Construction Group) members
□Selection criteria should be discussed: For example; previous knowledge and experience in masonry, physical strength, permanent residency in the target area, not having full-time job, commitment to low-paid community development work □Form sub-committee like LCG under RDC so as to avoid conflict and discommunication
3.1 Conduct PHAST workshop to analyse the problems and let stakeholders learn by themselves from each other (See PHAST page 11)
□Organize PHAST workshop to assess health problems in the community deeper (plenary session for all stakeholders together with NHC/CHW) □Analyse how community’s usual practices may be good or bad for health at the workshop □Analyse how hygiene and sanitation practices of their own and problems may be causing problems in the community
3.2 Identify what might go wrong □ Make the groups to think about possible problems in implementing the plan, and devise ways of overcoming them
3. Conduct PHAST and/or CAP Workshop
3.3 Conduct CAP workshop (2) for planning
□Prepare programme document and conduct CAP workshop to formulate latrine construction and promotion Work Plan (WP) □WP should include Activity, Description, Objectively Verifiable Indicator (OVI), means of verification (MOV), timing, resource required and responsible party (see Table 2.3.10 Example of annual Work Plan) □Agree with the conceptual model and the major objectives over the next 2 years (project period) □Plan for monitoring and evaluation in the work plan; evaluation framework agreed upon
LCG: Latrine Construction Group, NHC: Neighbourhood Health Committee, CHW: Community Health Workers,
EHT: Environmental Health Technician, PHAST: Participatory Health and Sanitation Transformation, LCC-DPH:
Lusaka City Council-Department of Public Health
A-1-62

VIP Latrine Construction
2.3.3 HOW CAN WE DO? (STEP BY STEP)
1. Practical Training This training focuses on practical sessions including construction of demonstrative communal (public) latrine. A sample of training programs used for Bauleni home VIP latrine project is shown in Annex 3. As the work plan
developed in the 1st CAP workshop may not be so specific, it is recommendable to develop more concrete annual work plan at the end of this training workshop. 2. Choose appropriate and acceptable technology suitable for the settlement To be technically, socially and environmentally appropriate, acceptable and affordable, each technology should satisfy basic guidelines (Box 2.3.2). There is no standard VIP latrine design developed in Zambia, but one used for the pilot study is shown in Table 2.3.2 and drawing is attached in Annex 6.
Table 2.3.2 The standard type of single VIP latrine design
Standard Single VIP latrine Design Siting See Box 2.3.3 Size/volume of pit
-3 meters deep 1.3 meters in diameter -Lined it with cement mortared block (3 wheelbarrows of building sand+ four shovels of normal Portland cement)
Cover Slab -Squat hole (14cm X 28m) and pipe hole (14cmX14cm) and footrests -7.5-10cm thickness -Concrete mixture 1:5 cement to sand ratio -Use reinforcement bar (18m for cover slab)
Vent pipe -Made of blocks and cement mortar of mixture ratio of 1: 4 -25cmX35cm (outside), 14cmX14cm (internal space), 2m (height) -Build opposite side of doorway (doorway should face towards the wind)
Superstructure -Any kind of materials can be used (Cement blocks are preferable) Fly screen -Made of stainless steel or plastic (35cm X 45cm)
-Should be fitted to the head of the vent pipe and strong cement mortar Roof -Ferro cement roof (mixture 1:3 cement to sand ratio, 1.3mX1.3m)
-Chicken wire (0.9m X 4m) and reinforcement bar 18m
DO
Box 2.3.2 Basic guidelines of VIP latrine design In some soil conditions (high water table), completely sealed pit lining (not perforated) and up-lifted
(50-75cm above ground) latrine is required to prevent it from collapsing. If you completely seal the pit,
latrine emptying mechanism (use-fee collection to pay for vacuum tanker) should be carefully planned
Cause no harmful surface soil contamination through 100% lining (whether perforated or not) or use
septic tank type
Cause no harmful contamination of untreated portable water sources
Prevent the spread of disease transmitted by flies or rodents (proper length and location of ventilated pipe)
Be free from offensive smells (give odour control) and unsanitary conditions
Present no health risk to people using or maintaining the system
Be culturally acceptable and gender sensitive (ensure privacy)
Proper soak away system (with water pipe and use stones for filtration) should be made to avoid surface
pollution if shower room is separately constructed or same latrine space is used for shower room
A-1-63

VIP Latrine Construction
3.Create demand and then select beneficiaries On top of water supply, sanitary facility improvement can be the spur to changes in hygiene behaviour. But the provision of water and sanitation technology (hardware) alone without changes in hygiene behaviour (software) usually achieves little or no significant health improvements. Therefore, for successful sanitation project, it is crucial not to hurry building facilities when there is little demand, but rather to focus first on hygiene and sanitation promotion to raise awareness and create demand. The sensitisation campaign targeting landlords as well as tenants could increase demand to improve existing facilities so that the project increases ownership. It is also important that community have enough time to examine several options through health education and demonstration models (several technical options of improved latrine) presented to the community in demonstration sites such as clinic, market, and school. 4. Supply of Materials Total cost of a single VIP latrine is about US$190 (Table 2.3.3.). As it is difficult to successfully implement such project without any subsidy at all, it is advisable that about 80% (materials which are not obtainable within the settlement) of the cost is borne by outside sources, such as funds from donor, landlord themselves or some kind of loan assistance (the pilot project provided 75% as the cement price then was lower than present). In the pilot project, community contribution ranged from US$4-36 for single VIP and US$24-54 for double. Price was reduced when a beneficiary was a LCG member who built own VIP, got free river sand in rainy season, crushed stones on his or her own, and/or utilised existing latrine door lock. A sample cost estimate for 5 design options is shown in Annex 7.
Table 2.3.3. Sample estimated cost of standard single VIP latrine as of March 1st, 2001
NOTE: Calculation was made on the assumptions that the donor will pay part of materials cost (80%) and the community contribute 20% to construct a single VIP with vent pipe and full-lining with door and lock. Currency US$1=3,700 kwacha
No. Item Unit Quantity Unit Price(KW)
Total(KW)
TOTAL(US$)
Comment
Donorcontribution
Cement for mouldingblocks
Pocket 18 25500 459000 124 1bag = 50kg of cement(7 bags forbuilding, rest for pipe & slab, pit
Asbestos sheet for roof m 0 35700 0 0 3.6m(if you use concrete roof, noJ-Hock LS 0 600 0 0 (if you use concrete roof, no need)Timber(roof) LS 0 28000 0 0 (if you use concrete roof, no need)Reinforcement bars LS 1.5 40000 60000 16 18m(for 2X2 square slab)Fly screen LS 1 6500 6500 2 50cmX25cmChicken wire sheet 4 6500 26000 7 0.9mX4m(concrete roof)
Communitycontribution
River sand for mouldingblocks, slab and floor
wheelbarrow
5 5000 25000 7
Building sand for structureand plastering
" 14 3500 49000 13
Crushed stones " 4 2000 8000 2 Maximum size= 16mmSkilled Labour latrine 1 45000 45000 12Pad lock 1 4500 4500 1Lock attachment 0 1500 0 0Door 1 10000 10000 3TOTAL 693000 187
141500 38 20%
Donor contribution 551500 149 80%
Community contribution (sand/stones+ labour + other costs)
A-1-64

VIP Latrine Construction
Cost-effectiveness can be achieved through good logistic management (carefully planned purchasing strategies, storage and use) as well as linkage with private sector. It is effective to cut the cost by making the most use of locally available materials (burnt bricks can be used for superstructure) by community contributing their tools and by involving private sector to promote parts of the technology. List of tools necessary for the VIP latrine project for 2 years duration (assuming that the project covers one settlement) are described as follows:
Table 2.3.4 Cost of Tools for VIP 5. Construction Family members should choose sites of the latrine with supervision by the local Environmental Health Technician (EHT).
Box 2.3.3 Siting of VIP latrines
1) Location of sanitation away from water source to avoid ground pollution risk (further described in Table 2.3.8) 2) Where the ground is firm so that the latrine does not collapse 3) The lining should be well sealed and should extend a minimum of 75mm above ground level to prevent rainwater
entering the pit, but in place where water table is high, it should be up-lifted about one meter above ground 4) Near the house so that the latrine can be used easily 5) Away from trees so that air can flow easily over the pipe 6) Airy or well-ventilated area 7) Facing the wind (a door should be facing the wind) so that air blows into the entrance
To assure the future sustainability, community need to learn how to manage implementation process by themselves (The right photo shows female bricklayers’ work supervised by one of the RDC members). Influence by the rain (both positive and negative) should be also carefully considered and necessary measures should be taken to solve the up-coming construction problems.
N o . I te m Q u a n t i t U n it T o ta l T O T AK w K w U S $
1 W h e e l b a r r o w 1 5 1 3 5 0 0 2 0 2 5 0 0 5 52 S h o v e l 2 0 3 6 0 0 0 7 2 0 0 0 0 1 9 53 S p ir i t l e v e l 2 0 1 9 0 0 0 3 8 0 0 0 0 1 0 34 T r o w e ls 2 0 1 4 5 0 0 2 9 0 0 0 0 7 85 T r o w e ls 2 0 1 2 5 0 0 2 5 0 0 0 0 6 86 5 m ta p e 1 0 1 2 5 0 0 1 2 5 0 0 0 3 47 B u i ld in g ta p e 1 0 7 5 5 0 0 7 5 5 0 0 0 2 0 48 B u i ld in g ta p e 1 0 2 1 0 0 0 2 1 0 0 0 0 5 79 B u c k e t 2 0 2 1 0 0 0 4 2 0 0 0 0 1 1 4
1 0 C h a in (3 m ) 2 0 1 0 0 0 0 2 0 0 0 0 0 5 41 1 P ic k 2 0 4 5 0 0 0 9 0 0 0 0 0 2 4 31 2 S tr in g 1 0 8 5 0 0 8 5 0 0 0 2 31 3 W o o d e n flo a t 2 0 6 0 0 0 1 2 0 0 0 0 3 21 4 M e ta l f lo a t 2 0 1 8 0 0 0 3 6 0 0 0 0 9 71 5 G lo v e s 2 0 1 3 5 0 0 2 7 0 0 0 0 7 31 6 G u m b o o ts 2 0 5 0 0 0 0 1 0 0 0 0 0 0 2 7 01 7 R u d d e r 5 1 0 0 0 0 0 5 0 0 0 0 0 1 3 5
T O T A L 6 7 8 7 5 0 0 1 ,8 3 4
k
A-1-
65Currency US$1=3,700 wacha, Price unit of those materials are as of March
2001

VIP Latrine Construction
■■■■ CHECKLIST FOR DOING
Step Action Checkpoint 1.1 Design training programme and prepare training handouts
□Utilize training program used by previous project. Get assistance from NGO and/or EHT/LCC to develop training materials □Plan 2weeks training but consider participants’ daily/weekly schedules □Conduct pre-workshop meetings to check logistical arrangement
1.2 Conduct practical training (theory, technology)
□Don’t conduct training during heavy rainy season (motivation gets lower) □Training certificate and ID card can only be given for those who passed the test (both theory & practical) □Prepare ID card with RDC logo and authorized by DHMT/LCC-DPH
1.3 Make annual work plan and get consensus (See Table 2.3.2: Sample Annual Work Plan)
□Make more concrete annual work plan after 1st CAP workshop □Review work plan, clarify roles and responsibilities of each stakeholders to gain consensus on each issues, then sign MOU
TO AVOID VAGUE AND UNREALISTIC PLAN Think strategically Where and how can we do the most and have the
greatest impact with available resources? Set reachable goals Consider resources and time available to set
goals Be concrete/specific Don’t use vague expressions Consider risks and sustainability
The potential risks can and do affect project. Once the project ceases, what is likely to happen in the area? Can risk to the project be reduced?
1. Practical Training
1.4 Develop monitoring sheet
(See ‘SEE’ section 1.1 P66)
2.1 Compare appropriate, affordable and acceptable options
□Figure out what are the most suitable and cost-effective interventions for the community and make comparisons (pros. and cons.) See previous page for useful criteria
2.Choose appropriate and acceptable technology
2.2 Construct demonstration latrines
□Select which types/designs to be demonstrated □RDC and LCG choose demo sites effective to attract people’s attention and promote use (do not choose sites for someone’s personal gain!) □RDC and LCG should agree on roles and responsibilities for the management of the communal latrines for smooth O&M □Do not collect fee from demo-latrine during demonstration period
3.1 Set up eligibility criteria for beneficiaries
□RDC and LCG should discuss eligibility criteria suitable for the community: such as 1) permanent residency, 2) satisfy community commitment/contribution required by the project
3.2 Conduct sensitisation campaign
□Decide effective strategies (campaign, key messages) to promote hygienic behaviour and importance of safe and sanitary VIP □Use megaphones & arrange drama performances for the campaign
3. Create demand and select beneficiaries
3.3 Choose beneficiary and sign MOU with each beneficiary, LCG & RDC
□Get application forms from candidates and make a short list □RDC interview candidates and select with LCC/NGO support according to the criteria decided in (3.1)
4.1 Collect/purchase tools and materials for construction and store them
□Mobilize community to contribute their construction tools □Investigate price of local materials nearby (river sands, rocks etc) and encourage community to purchase them in cheapest possible way □Purchase tools and materials, check they are delivered on schedule □Check quality of the sand collected/bought by the community □Store materials/tools in safe place (quality control, avoid theft)
4. Supply of Materials
4.2 Stimulate the Private Sector to develop parts of latrines
□Identify possible private sector that handles a range of sanitation goods which are locally manufactured ( such as soap, slabs etc. ) □Support the private sector in developing sanitary facilities and parts
5. Construction
5.1 Management of construction progress
□Check the progress of construction and its quality based on work plan □Check LCG’s work performance every day (See Annex 4) □Check quality of sand/rocks collected by the beneficiary before use □Avoid damage of construction materials during rainy season
LCG: Latrine Construction Group NHC: Neighborhood Health Committee, CHW (Community Health Workers),
EHT: Environmental Health Technician
A-1-66

VIP Latrine Construction
2.3.4 HOW CAN WE SEE? (STEP BY STEP)
1. Monitoring Process monitoring: To make sure if process and progress in terms of organizational structure set-up, construction and training are made on time
according to the work plan developed in the planning workshop. Impact monitoring: To see how the performance of activities have achieved objectives in terms of degree of community participation, human resource development and institutionalisation. It should also ensure Participatory Monitoring. For effective monitoring, it is desirable to develop a monitoring sheet by stakeholders to decide how often they should and who should be responsible for this. An example of progress monitoring sheet is in Table 2.3.5 and a sample Latrine construction & maintenance monitoring sheets are in Annex 4&5.
Table 2.3.5 An Example of Process Monitoring Sheet What is to be checked
Who will check?
How often?
How should it be checked
Likely problems to arise
Action to be taken
By whom
When
1. Slab EHT Every 2 weeks
Observation Surface water may contaminate the water underground
Buy cement to mend the cracks
LCG Immediately
2. 3.
2. Evaluation Evaluation should be carried out, preferably 1 or 2 years after the project starts, with active participation by the community, other community workers, officials and representatives of neighbouring communities if necessary. After the evaluation is concluded, lessons learnt and recommendations should be summarised. The main objectives of the evaluation are: 1) To assess if process/progress were performe
achieving its objectives (how much has been do2) To clarify its objectives and policies and a
workshop were relevant to national goal and po3) To find out what impacts were observed (expec4) To see how efficient the work was done (use of5) To look at the project sustainability (Was man
action solve problems occurred?)
SEE
A-1-67
d effectively on time and made towards ne, or still needs to be done)
ssess its relevance (objectives set in the licies) ted or unexpected, positive or negative) resources input) agement system developed? Was corrective
Participatory Evaluation Workshop

VIP Latrine Construction
■■■■ CHECKLIST FOR SEEING Step Action Checkpoint
1.1 Develop process & impact monitoring sheets
□If there has been a time break between this activity and the previous one (See ‘DO’ section), start with a group discussion to review previous workshop □Show the drawings which represent goals of the project □Have a monitoring sheets (on flip chart) ready (SEE previous page for sample monitoring sheets, Table 2.3.5.) □Ask the person who were selected to manage specific tasks (those who were chosen during the “PLAN” and “DO” workshop activity) to facilitate a discussion on the followings: 1) How to measure, 2) How often progress and impact should be measured, 3) Who should be responsible, 4) likely problems, 5) actions taken by whom by when (SEE Table 2.3.5. as an example) □Set a date for the project evaluation
1.2 Monitor Process to see if the process and progress were made according to the work plan developed in the workshop.
□Check if organisational structure of LCG is formed on right time □Check if organizational capacity is built by using Institutional Capacity Building Monitoring Sheet (See Table 1.3.1 Page22) □Check if selection of beneficiaries are done on right time □Check if construction is done without any delay or if any problems occurs □Check if construction materials are good quality □Check if construction materials are delivered on time □Check if beneficiaries’ on-site training is conducted on time
1.3 Monitor Impact to see if the performance of activities is done to achieve objectives.
□Check every week LCG performances and how many LCG work actively □Check how LCG, RDC, EHT, LCC, NGO are actively play defined roles in each steps of “DO” stage □Check how LCG and RDC had institutional change and learning in the process of latrine development
1. Monitoring
1.4 Water Quality □Conduct monthly water sampling to see surface/portable water pollution 2.1Check Objectives and policies
□Understand why you are evaluating by reviewing the objectives set in the CAP workshop and is relevant with district goal through group discussions
2.2 Evaluate progress of activities
□Check if all activities in the work plan are performed effectively on time by using PROCESS MONITORING SHEETS □Clarify the successful issues and problems occurred □Analyse the problems 1) if community can deal with them by itself, 2) if the participants fully understand, 3) if it can be solved by the community itself) □Find what actions/solutions should be taken for, how they will get more information and when and who will do it for solving, and how they will get outside help to overcome those problems
2.3 Evaluate Project Impact
□Make community walk to create community map to observe community conditions and physical changes directly to evaluate if goals have been met □Ask the group to look at the work plan developed to compare what it planned to do with what it has achieved and check the degree of community participation in all process of the project □Check if the community organisations (RDC/LCG) was grown up and changed by using INSTITUTIONAL BUILDING MONITORING SHEET □Check if LCG, RDC, EHT, LCC, NGO actively played defined roles in each steps of “DO” stage
2.4 Evaluate Efficiency
□Check if the project inputs were cost-efficient (no over/under spent) □Check if timeframe and period were appropriate (not too short or long and good season to construct, etc) to achieve objectives □Check if the inputs of human resource were enough for workload
2. Evaluation
2.5 Evaluate Sustainability
□Check if physical maintenance system is established □Check if institutional capacity was built □Check if school running system is established (income generation, teacher’s allowance, etc)
LCG: Latrine Construction Group, EHT: Environmental Health Technician
A-1-68

VIP Latrine Construction
2.3.5 HOW CAN WE SUSTAIN? (STEP BY STEP)
1. Demonstrative Communal (Pulic) Latrine Maintenance & Management
The benefit of demonstrative latrine is to show people a good example, so it needs to be sited at a place where general public gather, it should also be kept
clean and well maintained. These latrines are often damaged by vandalism unless there is a system to avoid such incidence. Since it is an asset for the community, after demonstration period is finished, it can be used for fund source. The following table 2.3.6 is an example of a system of physical maintenance and management of communal (public) latrines in Bauleni and Chibolya. A sample monitoring sheets of maintenance and use of communal (public) latrines are shown in ANNEX 4. Table 2.3.6 Example of Physical Maintenance and Management System in Bauleni and Chibolya
Bauleni Chibolya Site of demo latrines Back garden of Bauleni Health
Center On the road located in southern boundary of Chibolya (near several churches)
Key holding Sister in Charge of the Health Center
LCG chairman (master key) RDC chairman (spare key)
User-fees and its use No user fee Rental fee collected from the churches (7,500 kwacha /one day use)
Daily cleaning Done by a maid using cleaning tools provided at the clinic
A maid at the church (pastor is RDC member)
Security Security guards for the clinic Church Repair DHMT’s responsibility RDC (from user fee)
2. Communal (households) Latrine Maintenance & Management Each communal (household) latrine, shared by more than 1 household, needs to establish a good maintenance system. The success of on-site training as well as of the system establishment depends if the project could build strong ownership among beneficiaries. A sample On-site training messages are shown in Box 2.3.4.
SUSTAIN
Box 2.3.4. Remember: The following TEN POINT RULES 1. Always use the latrine 2. Help little ones to use it (dirty latrine attracts many flies and other insects) 3. Close the door (latrine has to be kept dark to discourage flies from entering the pit) 4. Wash your hands when you are finished (hands can also be source of transmission) 5. Keep the latrine clean (floor and slab by washing and scrubbing every day with water)
A latrine can be kept odourless by flowing a handful of ash in the latrine every morning 6. Do not throw rubbish into the latrine (this may considerably reduce the useful life of your
latrine) 7. Tell your family if you see fault (watch each other) 8. Learn about good health (from Clinic staffs, Community Health Workers etc.) 9. Check cracks in the slab and superstructure regularly (need to be repaired immediately) 10. Check amount of sludge in the pit once a month (when the pit is 60cm below ground
level, prepare for vacuum cleaning or start building new latrine)
A-1-69

VIP Latrine Construction
The following table 2.3.7 is an example of a maintenance system pilot tested in George compound in Lusaka UUS (supported by JICA Primary Health Care project).
Table 2.3.7 Example of Household Latrine Maintenance System by JICA PHC Project in George
Check Point System established Type of latrine introduced
A household single VIP (completely lined and no perforation to avoid soil contamination) shared by 3 households (18-21 people)
Maintenance cost paid by the beneficiaries 5,000 kw /month/each VIP latrine Account for the money collected 3,000 kw (saved for the future vacuum cleaning)
2,000 kw (used for buying a soap to clean latrine) Supervision done by EHT at George health center Monitoring done by Environmental health committee organized under the clinic Daily cleaning done by One responsible household
3. Environmental Concerns Sanitation systems may pollute the local environment, i.e. the underlying aquifers, or the surface water bodies, or estuaries. The following table 2.3.8 is basic precautions to consider and minimise the risk of possible contamination (surface and ground water).
Table 2.3.8 Precautions for Environmental Concerns Surface pollution 1) All vertical walls of the pit should be 100% lined
2) Lining should be well sealed (completely sealed in high water table area) and should extend a minimum of 75mm above ground level to prevent rainwater entering the pit
Groundwater pollution
1) Downstream of drinking water supplies (the well or borehole) so that waste from the latrine does not drain into the water supply. The following guidelines for distances should be adopted (See these guidelines described in the DEVELOPMENT FRAMEWORK DRAFT by World Bank, May 2000) 7.5m from the drinking water source if the highest seasonal water table is more
than 5m below the bottom surface of the pit 15m from the drinking water source if the highest seasonal water table is
between 1-5m below the bottom of the pit 30m from the drinking water source if the highest seasonal water table is less
than 1m below the bottom of the pit A sample formula with which life span of latrine was calculated is described below.
Box: 2.3.5. A formula to calculate Latrine Life Span Life span(Year) = {(depth of hole: meter)X(π)X(radius of pit: meter)2 } ÷{(number of
people sharing latrine) X(365days)X(0.06 3)} Example of standard type VIP latrine Life Span used in the pilot study (see Table2.3.2 design)
Life Span (used by 6 people)= (2.9X3.14X0.652) ÷÷÷÷(6 X365X2.16-04)=8 Years 4. Further expansion of the project If a low-cost sanitation project is to be feasible, a mechanism of revolving fund, fund raising, or housing/sanitation loan assistance may be considered during the project period and afterwards to carry on the project in the future.
A-1-70

VIP Latrine Construction
■■■■ CHECK LIST FOR SUSTAINING
Step Action Checkpoint 1.1 Key holding □Decide who will hold master and spare keys and watch communal
(public) latrine 1.2 Daily cleaning □Decide who will clean up communal (public) latrine 1.3 Security □Check if there is physical ways to protect demo. latrine (e.g. Door
lock with wire, Neighbour hood watch etc) from vandalism 1.4 Repair □Decide who will repair and pay the cost for any damaged facility or
stolen parts
1.DemonstrativeCommunal (Public) Latrine Physical Maintenance and Management
1.5 User-fees and its use □Decide how much fees should be charged. Consult with community people expected to use those demo latrines which, after the project initial stage, become communal (public) latrine □Decide who will collect, keep money and who is paid for maintenance (buying cleaning agent, vacuum cleaning cost)
2.1 Prepare proper use & maintenance training program and materials (On-site training)
□Don’t include so much information for on-site training program and use more graphics than letters for materials □Make copies of pictorial proper use and maintenance training material to be distributed
2.2 Conduct on-site training
□Conduct training during no business hours □Training should be less than 30 minutes
2.Communal (households) Latrine Physical Maintenance and Management 2.3 User-fees SEE above checkpoint 1.5 and table 2.3.7 as an example
3.1 Ground water pollution
□Before construction, sitting must be carefully done with assistance by EHT/NGO( SEE BOX 2.3.3 “DO” section) □Lining extension should be minimum 75mm above the ground □Pit lining and sealing should be done 100% (perforated or not) depending on the soil/land condition of the area
3.2 Odour control □Ventilation pipe will usually eliminate the problem □Use PITKIN/FATKIN, if not affordable put a bit of ash everyday □A simple stopper in the latrine hole can be used □Clean latrine every morning and afternoon
3. Environmental Concerns
3.3 Latrine Emptying □ If possible, do not empty latrines. Because unless properly managed, using the correct equipment, pit latrine emptying is highly hazardous procedure □Pits to be emptied must be made of more durable materials and the pit must be fully lined to withstand the suction forces □Use “PITKIN” or “FATKIN” to reduce sludge □If possible, construct two-pit latrines that are used alternately, this allows time for the disease-causing organisms in the excreta to die off, making it harmless to handle (need to make sure they are used properly) □If affordable and possible to negotiate the narrow roads and alleys of peri-urban compounds, ask a slurry tanker of LCC by paying (129,000 kwacha/time) or private tanker (480,000 kwacha/time) to come and empty latrines □Slurry tankers can not remove large solid objects such as stones, sticks, tin cans, and plastic bags, so strong promotion campaign is required to persuade the community not to throw such articles into their pits
4. Further expansion of the project
4.1 Sourcing for Funds □ Seek for donor/NGO/Bank fund (loan) by sending a proposal □ Try income generating activities(IGAs) by letting facilities for church, or creating sanitary mart (SEE “DO” section) □ Try fund raising (Brai, Drama, Lottery, Football game) □ Try to contact private company for financial assistance
LCG: Latrine Construction Group, PITKIN/FATKIN: a bio augmentation products to breaks down starches, protein, greases and other organic matter, EHT: Environmental Health Technician
A-1-71

VIP Latrine Construction
2.3.6 LET’S ENVISAGE PROCESS AND ACTORS After understanding ‘Plan, Do, See and Sustain’, let us envisage and illustrate how the project is preceded and implemented. The following figure shows an example of all the process, but the order of actions may be changed and modified on case-by-case basis. A project work plan (Table 2.3.9) and more concrete annual work plan
(Table.2.3.10) must be designed as follows. The work plan should be used as one of the indicators for progress in monitoring and evaluation. Usually it may take 3 months planning period, 3 months for preparation, 15-16 months for construction, and 1 month for evaluation.
Table 2.3.9 Example of a VIP latrine construction project work plan (duration 2 years)
Table 2.3.10 Example of a VIP latrine construction project Annual work plan
WORKPLAN
& ACTORS
M1-3 M4-6 M7-9 M10-12 M13-15 M16-18 M19-21 M22-24PLAN 1.Identify Problem/Assess Needs
2.Identify Supporting Agencies3.Analyse Problem and Plan forsolution
DO 4.Plactical Training and5.Create Demand6.Select Beneficiaries7.Supply Materials8.Construction9.Follow-up Training
SEE 10.Monitoring11.Evaluation
SUSTAIN 12.Maintenance and Operation
M ainActivity/Subactivity No.
Description Indicator M eans ofVerification
(M OV)
ResourceCommunity
input
Resourcerequired
External input
ResponsibleParty
Timing
1.1Practical Training andW orkshop
1.1.1
Design trainingprogramme and preparetraining handouts
1.1.2
Conduct practicaltraining(theory,technology)
1.2 Create Demand
1.2.1ConstructDemonstration latrines
1.2.2Conduct VIP latrinecampaign
1.2.3
Objective (1) A model for safe and sanitary home VIP latrine construction is developed and expanded(2) Health and hygiene conditions of people in the project area are further improved
ProjectOutcome:
(1) A Latrine Construction Group (LCG) is organized under RDC(2) An appropriate training course method (a course module and a manual) for the community isdeveloped by NGO/LCC(3) VIP latrines are installed with cooperation of RDC, LCG, and the community
A-1-72

VIP Latrine Construction
Also when all stakeholders are identified, everybody must recognise their role and responsibilities. In each action/step, different group of people have different level of responsibilities. (Table 2.3.11)
Table 2.3.11 Role and Responsibilities of Stakeholders
The following Venn diagram illustrates how key institutions and groups have interactions. Community has close contacts and cooperation in decision-making with NGO and LCC on daily basis, while donor and DHMT/Clinic play as back supporting agencies as required.
Figure 2.3.1 Stakeholders Relationship (Venn Diagram)
LCG RDCNHC
(CHW) EHT
LCC(site
oficer)Health Center
(DHMT) NGO DonorPLAN 1.Identify Problem/Assess
2.Identify Supporting Agencies3.Analyse Problem and Planfor solution
DO 4.Plactical Training and5.Create Demand6.Select Beneficiaries7.Supply Materials8.Construction9.On site Training
SEE 10.Monitoring11.Evaluation
SUSTAIN 12.Maintenance and OperationPrimary Roles Secondary Roles
Donor
RDC:Management of the logistics Supervision of LCG
NHC(CHW):SensitisationCampaign
LCG:Identify beneficiariesConstruction, M&E
NGO:Purchase materialsTechnical assistance &Advise
LCC:Technical assistance & coordination
Community:Contribution of labour, cashLocally obtainable materials EHT:Technical assistance&
Monitoring&evaluation
Clinic: Supervising EHT,Coordination with RDC, NGO
DHMT:Training of EHTAdvise&policy guidance,Certificate of LCG
NGO
Clinic
EHT
LCC
DHMT
Donor:Provide fund
RDCNHC
(CHW)LCG
Community
Donor
RDC:Management of the logistics Supervision of LCG
NHC(CHW):SensitisationCampaign
LCG:Identify beneficiariesConstruction, M&E
NGO:Purchase materialsTechnical assistance &Advise
LCC:Technical assistance & coordination
Community:Contribution of labour, cashLocally obtainable materials EHT:Technical assistance&
Monitoring&evaluation
Clinic: Supervising EHT,Coordination with RDC, NGO
DHMT:Training of EHTAdvise&policy guidance,Certificate of LCG
NGO
Clinic
EHT
LCC
DHMT
Donor:Provide fund
RDCNHC
(CHW)LCG
Community
A-1-73

Health and Hygiene Education
2QAPsosps QAraPp QAssastIsac QAhwlpaci
2.4 Community/School-based Health and Hygiene Education
.4.1 Introduction and Case Studies with Lessons Learnt : Why is hygiene so important? : Diarrhoea is one of the top three killer diseases in eri-urban settlements in Lusaka. Water supply and anitation improvement may help reducing the incidence f diarrhoea and Cholera. However, whether water and anitation facilities are available or not, the best way to rotect you and your children is to adopt a number of afe hygiene practices in and around the home.
: Why is a participatory approach to health and hygiene e: Health and hygiene practices which are imposed by o
easons: 1) a lack of clear understanding between communitnd 2) often outsiders work for the community rather than wiarticipatory health and hygiene education promotes: 1) Corocess, 2) Confidence, 3) Dignity, 4) Choice, 5) Awareness, a
: Why do schools and community should work together? : On top of the family, schools are the most important pl
timulating learning environment for children and stimulatchools are available, they can act as a model, and teacherslso facilitate a broader impact on communities through tudents schools are in touch with a large proportion of the ho involve the community so that it may support school activitn school health and hygiene programs, we need to improve banitary conditions and facilities available in and around thend software (activities aiming at promoting conditions athildren that help to prevent water and sanitation-related dise
: Why is it important to focus on children? : Childhood is the best time for children to learn ygiene behaviours. Children are future parents and hat they learn is likely to be applied in the rest of their
ives. If children are brought into the development rocess as active participants, they can become change gents within their families and a stimulus to ommunity development, and peer pressure can be nstrumental in this process.
A-1-74
ducation used? utsiders are often not effective for many y perceived needs and those of the outsider th the community. mmunity and household ownership of the nd 6) Co-operation and partnership.
aces of learning for children. Schools are e behavior change. If sanitary facilities in can function as role models. Schools can outreach activities, because through their ouseholds in a community. It is important
ies, or at least not work against them. oth hardware component (total package of school and provide school health services) school and practices of school staff and ases).

Health & Hygiene Education
Box 2.4.1 Community-based Health and Hygiene Education in Bauleni & Chibolya
The settlements where JICA undertook pilot projects have historically lacked access to safe water and sanitation facilities. In December 1999, an NGO, Africare, as the implementing agency, initiated H&H (health and hygiene) education project (both community and school-based) in Bauleni and Chibolya settlements. The overall objective of this project was to improve personal and community hygiene practices through the promotion of participatory H&H approaches. In order to achieve the objective, measurable indicators were
identified as benchmarks. At the end of the pilot phase, it was expected that: the health education campaign using door-to-door visits would reach at least 25% of the targeted population in Chibolya (zones 4 & 5) and Bauleni (zone 8 & 13), and demonstrations by drama groups would be conducted at least three times in each settlement. Africare aimed to train forty health educators (20 in each settlement) at a training of trainers (TOT) workshop on messages of H&H education who would then be able to go into the community and train others.
The effectiveness and popularity of tools used to sensitise the communities on H&H education varied from community to community. Overall, drama performances attracted more beneficiaries and were one of the most effective avenues for information dissemination. The door-to-door visits, posters and church meetings proved to reach handful people and took more time for the delivery of messages, but had the benefit of having immediate beneficiary feedback on the topics presented. Verifiable indicators and achievements in the two settlements and notable changes in hygiene behaviour of the community observed in post-project household/KAP survey (2000) in comparison with Baseline survey (1999) are summarised as below:
Output Verifiable indicators
Achieved
In Bauleni, To educate 25% of all targeted area population of zone 8 and 13
Health education of 793 people in zone 8 and 13
160% (1263 people) of the targeted community (793 people) was reached through door-to-door campaign (47.3% of 300 houses were visited, according to post household survey)
In Chibolya, To educate 25% of all targeted area population of zone 4 &5
Health education of 1,000 people in zone 4 and 5
69.5% (695 people) of the targeted community (1,000 people) was reached through door-to-door campaign (31.7% of 300 houses were visited, according to post household survey)
Number of educational drama performances conducted in target area of both settlements
3 performances for each settlement
Bauleni: 4 performances (65% attended according to post household survey) Chibolya: 3 performances (49.3% attended according to post household survey)
Bauleni 1999 Bauleni 2000 Chibolya 1999 Chibolya 2000 Drinking water Chlorination
14% use Chlorine ↑↑↑↑49% use Chlorine 18% use Chlorine ↑↑↑↑28% use Chlorine
Washing hands after handling infant faces
53% water and soap 22% water only
↑↑↑↑70% water and soap ↑↑↑↑27% water only
47% water and soap 20% water only
↑↑↑↑70% water and soap ↑↑↑↑22% water only
Washing hands before handling/eating food
29% water and soap 67% water only
↑↑↑↑44% water and soap ↓↓↓↓52% only
23% water and soap 75% water only
↑↑↑↑51% water and soap ↓↓↓↓43% water only
Cover waste with soil to reduce rodents
57% yes ↑↑↑↑59% yes 50% yes ↑↑↑↑62% yes
Household waste disposal
20% dump in collection site
↑↑↑↑ 29% dump in collection site
30% dump in collection site
↑↑↑↑ 42% dump in collection site
In this regard, some lessons learnt and recommendations were: Primary role of supervising health volunteers should be under the clinic, not RDC since clinic is professional
organisation in the area of health. However RDC should continue collaborating with health centre to identify and solve problems in the community.
The RDC, in order to avoid drop-outs and high turnover rates within the volunteer resources in the future, should be advised to take time to screen each applicant and arrange individual interviews with interested people to be volunteers. Suggested criteria for the selection are: commitment to volunteer work, sufficient level of household income, previous volunteer and/or work experiences, literacy level, health background, period of residency, and not overlapping with other community development works.
The duration of the training workshops for community volunteers should give sufficient time for the participants to fully acquire the key messages being discussed.
Seed money for health educators should be provided to start income generating activities for future sustainability of the volunteer group.
Monthly monitoring sheets should be simplified ensuring that the community can complete them properly. Where there is no clinic, a Sub-health centre needs to be established, so that health educators have a base and
also receive continuous support and supervision by professional staff.
A-1-75

Health & Hygiene Education
Box 2.4.2 School-based Health and Hygiene Education Project in Chibolya
In line with the community based Health and Hygiene (H&H) Education in Bauleni and Chibolya
mentioned in Box 2.4.1, Africare initiated the School based Health and Hygiene Education Project (SH&H) at CHIBOLAY MIDDLE SCHOOL (public school) in April 2000. It aimed at combining the SH&H with those of Community-based H&H Project in Chibolya. The overall objective of this four-month component was to develop and promote a participatory child –to-child and child-to-adult health and hygiene education campaign aiming to improve the H&H
conditions in Chibolya school and the settlement. This was carried out through mobilising the school and the community to jointly promote H&H activities and practices of good health. The main activities were to disseminate information and teach behaviour change through the development of the School Health Coordinating Committee (SHCC) and the capacity building of the PTA and the school drama performance group. Initially, Africare identified a 12-member SHCC consisting of teachers, pupils, and members of the community (such as church, parents, and community schoolteacher). Africare then conducted a workshop in collaboration with CARE PROSPECT (CP), already working on water, sanitation and health education (WASHE) activities within the targeted communities, and the local clinic that was the major collaborator in the School Health Component. The 3 days workshop aimed to expose the SHCC members to basic water, sanitation and health and hygiene concepts and activities. Using participatory methods, the SHCC was able to identify their own health and sanitation concerns necessary for needed the most immediate attention. A comprehensive four months School Health Work Plan was developed based on the needs identified. Africare and CP who assisted the SHCC made a training manual outlining key messages. Throughout the implementation, the planned activities were monitored through weekly meetings involving the community, school officials, and NGOs. The RDC and its zone members were also instrumental partners in this component. By working with stakeholders in the community (such as health centre, community school teachers, and church organisation) school students’ activities were linked to the communities in which they reside. Verifiable indicators and achievements in the two settlements are as follows:
Output Verifiable indicators Achieved Establishment of school health coordinating committee
Committee to facilitate the school health activities in place
12 members composed of teachers, pupils and parents established
SHCC meetings Wednesday weekly meetings were held 7meetings held from May to July Community mobilization Meetings held to mobilize community
and school pupils 2 planned mobilization and sensitization meetings held
Refuse disposal (a) 2 refuse pits dug (b) 26 carton boxes sourced (c) 8drums or bins sourced
(a) 2 refuse pits dug (b) 4 carton boxes sourced (c) No drums or bins sourced
Drama performances Number of performances done by student/outside drama groups
3 performances done
Drama trainings School drama trained by outsider group 3 drama training sessions completed Repair existing toilets in the school
2 toilets repaired No toilet was repaired due to financial constraints (not budgeted) but fund raising activities were initiated
Increase low water pressure Number of additional tap stands installed No additional tap stands installed because the school has no resources (not budgeted) but fund raising activities were started
In this regard, some lessons learnt and recommendations were: The study revealed that similar project is replicable to other schools. The Ministry of Education and the Ministry of Health
should discuss application of similar strategy not only in the government schools but also in the community school. Health Centre Staff (such as Environmental Health Technician )should serve as an additional resources as they provide
supervision and technical advises to SHCC and it should also report to both DEO(District Education Office) and DHMT Linking school students’ health activities with the communities is an effective approach to bridge the gap between school
and the community. Duration of SHCC training should provide sufficient time for at least 2 weeks the participants will fully absorb the key
messages covered and it should be held during dry season. PTA should be actively involved, as their role is to oversee school activities. Private drama group trained school drama group and the clinic was quite effective in working with the student group and
provided the skills necessary to empower the student group in the dissemination of the health and hygiene education messages to the school and the community.
Because of limitation of time and budget, this study only aimed at strengthening organisational structure and networking for School Health Education Project, and it did not include hardware such as providing school health services and improvement of sanitary facilities at the school. It is recommended therefore to combine these lessons with those of national level pilot school-health project (health services and health education), BEESIP program funded by USAID.
A-1-76

Health & Hygiene Education
2.4.2 HOW CAN WE PLAN? (STEP BY STEP)
1. Needs Assessment It is important to identify with community about “main problems” regarding health and hygiene (H&H) and share basic information and data before
selecting appropriate design and technological options. It is suggested that household/school health survey be conducted to get baseline data. (Example see below Table 2.4.1)
Table 2.4.1 Data Items and Sources Data Data source Epidemiological data (such as diarrhoea/Cholera incidence in the health
centre of the catchments area) 1) Health Centres in charge 2) DHMT
Inventory of latrine technologies used previously Number of shallow-well users and identify their locations Number of landlords, tenants Community’s expressed demand for clean environment Knowledge on health/ hygiene issues Willingness to contribute to the projects Socio-cultural (social history, gender roles, practices, cultural taboos) Training needs felt by the community/School and staff at health facility
1) Household 2) Knowledge Attitude Practice (KAP) survey (See Page13) 3) Focus Group Discussions (FGD) 4) Direct Observation 5) Key Informant Interview
National/District goals and plans through annual reports National/District rules on medical / health human resources (such as
Clinic staffs, EHT, NHC, CHW etc.)
1) Annual reports, plans
Water at schools Presence of a tap, pump or tank, the appropriateness or the design and accessibility for small children, condition of the source, availability of water for: flushing latrines, anal cleansing, hand washing and drinking water, Maintenance arrangements, including availability of spare parts Sanitation at schools Presence of latrines, ratio of latrines for boys and girls, cleanliness of the latrines and presence of cleaning materials, drainage of waste water, garbage disposal
1) Focus Group Discussions (FGD) 2) Direct Observation 3) Key Informant Interview 4) School Mapping
Hygiene behaviour of boys and girls Safe drinking, safe water handling and storage, washing hands after defecation and before handling food, children using latrines for defecation, children using latrines or urinals for urination, regular cleaning of facilities, covering food
1) School health (KAP) survey
2) Participatory class room discussion
2. Identify supporting agencies and groups and set up a team It is important to know about existing ABOs working in the community and how to utilise and enhance capacities of such different groups. In the initial stage, existing community leaders like RDC, NHC and schoolteachers must play a leading role to identify existing groups and create a new group or mobilise existing ones (i.e. CHW, SHCC) for H&H and sanitation improvement project. It is also necessary to consider gender, economics and ethnicity balance. 3. Conduct PHAST and/or CAP to analyse Problem and Plan for Solutions After identifying community’s problems/needs and stakeholders working together to implement the project, common hygiene and sanitation practices should be investigated deeply to design the project and for project appraisal (whether it fits with the policies, principles, values and priorities of the community and if it’s feasible) by using PHAST and CAP (See page11, 14-15). CAP workshop aims to make strategies, prepare action plans and systems of monitoring and evaluation. The plan should identify the solutions and what actions needs to be taken, when, how, by whom and also future actions to prevent or solve problem.
PLAN
A-1-77

Health & Hygiene Education
CHECKLIST FOR PLANNING
Step Action Checkpoint 1.1 Collect data through PRA/PHAST workshops. (See PRA/PHAST page 10, 11)
Ask Yourself; □◆◆◆◆From whom is the data to be collected? □◆◆◆◆Who is responsible for the data collection? What is the use of the data collected? Who can use the results? □◆◆◆◆What is the use of the data collected? Who can use the results? □◆◆◆◆What methods will be used to gather data? □◆◆◆◆Collect data described in previous page
1. Needs Assessment
1.2 Collect data on government policies, goals and regulatory standard on Health/Education
□◆◆◆◆Check National/District goals and plans through annual reports. □◆◆◆◆Check National/District rules on medical/health human resources (such as Clinic staffs, EHT, NHC, CHW etc.).
2.1 Identify key community/school stakeholders to work with (which organization/group can be active and sustainable for health education project)
□◆◆◆◆If it becomes necessary to form new groups or organizations, build upon what exists and created by other development projects as much as possible(NHC,CHW, health sub-committee, School Maintenance Committee ). □◆◆◆◆Examine if CHW, NHC or RDC can handle all process or if other sub-committee/groups should join. □◆◆◆◆Consider, gender, economics, and ethnicity balance to make sure the project is not captured/monopolised by local elites.
2.2 Identify which supporting agencies are effective and collaborative
□◆◆◆◆Identify active staffs of DHMT (EHT) for technical advise and support. □◆◆◆◆Identify NGO with experience of community participatory health and hygiene education in peri-urban settlements.
2.3 Identify community health volunteers who can work as CHW members and form a group
□Selection criteria should include; 1) Commitment to volunteer work, 2) sufficient level of household income, 3) previous volunteer experiences, 4) literacy level, 5) health background, and 6) period of residency. □Form CHW under NHC and the clinic to directly implement the project. □Do not overlap one person’s role with other community development works (e.g. Not all RDC members should be selected as CHW).
2. Identify Supporting Agency and Groups then set up a team
2.4 Identify school/ community members who can work as SHCC members and form a group
◆Selection must be done carefully, first meet leaders from school and the community to decide how many people should be selected. ◆Criteria for teachers should include: the teacher can act as a role model and have good contacts in the community, he/she has a genuine interest in SH and the teacher can be allocated some time for taking SH activities in the school. Gender balance should be considered. ◆Select about 12 (not more) members consisting of students, teachers, community leaders, PTA, CHW, RDC, health centre ).
3.1 Conduct Participatory training workshop (PHAST) to analyse the problems and identify risk practices
□◆◆◆◆ Organize PHAST workshop to assess health problems in the community deeper (plenary session for all stakeholders including LCG). □ ◆◆◆◆Analyse how community/school students’ usual practices may be good or bad for health. □◆◆◆◆Analyse hygiene and sanitation practices and problems may be causing problems in the community.
3.2 Identify what might go wrong □◆◆◆◆Get the groups to think about possible problems in implementing the plan, and devise ways of overcoming them. □◆◆◆◆Check if concentration of workload (especially women) is appropriate.
3. To conduct PHAST and/or CAP workshop
3.3 Conduct CAP workshop (2) for planning
□◆◆◆◆ Prepare programme document and conduct CAP workshop to formulate latrine construction and promotion Work Plan (WP). □◆◆◆◆WP include Activity, Description, Objectively Verifiable Indicator (OVI) , Means of Verification (MOV), timing, resource required and responsible party (SEE Fig.2.4.7. Example of work plan). □◆◆◆◆Agree with the conceptual model and the major objectives over the next 2 years (1 year for School Health Project). □◆◆◆◆Plan for monitoring and evaluation in the work plan; evaluation framework agreed upon.
◆School Health Component Checkpoints NHC: Neighbourhood Health Committee, CHW: Community Health
Workers, EHT: Environmental Health Technician LCG: Latrine Construction Group
A-1-78

Health and Hygiene Education
2.4.3 HOW CAN WE DO? (STEP BY STEP)
1.Practical Training This training includes more practical learning sessions. Training should be
approximately 6 weeks (4-5 weeks classroom and 1-2 weeks field work) for CHW (community health workers) and 2 weeks for SHCC (school health coordination committee) both using participatory learning and action methodologies. Since the work plan developed in the 1st workshop may not be so specific, it is recommendable to develop more concrete annual work plan at the end of this training. An example of CHW training contents are summarised below and CHW training program and SHCC training program are attached in Annex 8-11. 2. Implementation of Health /Hygiene Promotion (and school health services) Activities In order to motivate community people’s behaviour change, it should not be top-down like traditional educational approach. The components of a communication plan of health and hygiene promotion strategy should be decided first as shown in table 2.4.2. The first step is finding out what and why the community (especially mothers and children) like and dislike about the target practices through Focus Group Discussions and interviews (this process is now called “Behaviour trials”), and then uses these positive values to motivate further behaviour change. In addition to the above methods, promotional drama performances and church meetings attract more community people but door-to-door campaigns are also effective to assure messages were delivered to the communities.
Table 2.4.2 Components of a communication plan Items Description
Behaviour change objectives Behaviour “A” will go from X% to Y% by the year XXXX. Target practices The key health & hygiene practices that replace risk practices Target audiences Age, sex, number in each group Positioning Motivation for behaviour change Channels of communication Educational drama, door-to-door visits, radio, schools, community
meetings, Communication materials The materials you develop for your activities Monitoring Methods for monitoring in progress, in activities, in outputs, and in
behaviour change For school health, not only health education and EH infrastructure development (sanitation and water) but also health services such as general health check-ups and treatment should be given to the pupils, because currently malnutrition levels are worsened in Zambian school children by the increase in parasitic infestations due to unsafe drinking water and poor sanitation. Parasitic infections in children can result in diarrhoea, anorexia and general malaise. When children are heavily burdened with worms, they eat even less and their absorption and retention of certain nutrients is impaired. Consequently, this diminishes children’s learning capacity and their ability to pay attention and to concentrate.
DO
A-1-79

Health and Hygiene Education
■■■■ CHECKLIST FOR DOING
Step Action Checkpoint 1.1 Design training programme and prepare training handouts
□◆Utilize training program used by previous project such as CHW training of 6weeks developed by DHMT&JICA. Plan 2 weeks training for SHCC. Consider participants’ daily/weekly schedules. □◆Conduct pre-workshop meetings to check logistical arrangements. □◆Topics should be covered under the training are: Basic sanitation and safe water chain, hygiene, other PHC issues such as Malaria, Nutrition, TB, HIV/AIDS, Family Planning, Action Planning, and Community Empowerment.
1.2 Conduct practical training and evaluate the training
□◆Don’t conduct training during heavy rainy season (many difficulties due to lack of motivation). □◆Training certificate should be given only for those whopassed the test □◆Prepare ID cards authorized by DEO/DHMT.
1.4 Make annual work plan and get consensus
(See Fig 2.4.2 for Sample Work Plan)
□◆Make more concrete annual work plan at the end of the training. □◆ Review work plan, clarify roles and responsibilities of each stakeholders to gain consensus on each issues, then sign MOU How to avoid vague and unrealistic plan, (see 2-3 “DO” section)
1. Practical Training
1.5 Develop monitoring sheet (See ‘SEE’ section p80) 2.1 Choose appropriate and
acceptable strategies □◆Figure out the most suitable and cost-effective interventions. □◆Decide on components of communication plan (see Table 2.4.2. as an example) that includes 1) behaviour change objectives, 2) feasible target practices, 3) target audiences, 4) message positioning, and 5) communication plan
2.2 Conduct sensitisation campaign
□◆Decide effective strategies (campaign, key messages) to promote safe drinking water, safe excreta disposal and personal and food hygiene. □◆Use megaphones & arrange drama performances for the campaign.
2.3 Conduct door-to-door campaign
□Introduce yourself and explain you are volunteer health worker. □Find a place to sit down and talk with people (do not stay standing). □Involve community, not only EXPLAINING, ASK questions, let them show their knowledge, beliefs, and behaviour (two way communication).
2.4 Prepare and conduct promotional drama performances
□◆Find if there is any local drama group (in community/school) or invite drama group from other area to learn from them (how to write simple script, handle audiences, effective use of dancing and music). □◆Decide on content of the drama, appropriate time (short play, broken into scenes), day and invite audiences. Rehearse/practice before the show (three scene play is suggested). □◆Do not let community leaders dominate the discussion. □◆Always spare some time for the audiences voice their opinions (Q&A, interviewing) and to understand if they understand.
2.5 Training other teachers
◆Selection of teachers to be trained should be carefully done. (See 2.3, 2.4 “Plan”). ◆SHCC member teachers should plan for training other teachers by using participatory technique. ◆Construction of a VIP latrine at the teachers’ premises will help enhance teachers’ appreciation of sanitary facilities.
2.6 Health talks (in and outside of school curriculum)
◆Make arrangement with health centre staff to hold a session. ◆Plan schedule (morning session etc.) and topics, and prepare materials.
2.7 School health check-ups twice/year
◆Make arrangement with EHT and the clinic. ◆Collect health data of students through check-ups, analyse them and provide deworming pill, and conduct malaria treatment. ◆Collect small fee from parents for deworming medicine.
2. Implementation of Health and Hygiene Promotion (and school health services) Activities 2.5, 2.6, 2.7 and 2.8 are only for School based Health and Hygiene Education
2.8 VIP latrine demo at school ◆See 2-3 VIP latrine construction project see “DO 1-6 ” section.
◆School Health Component Checkpoints DHMT: District Health Management Team, CHW: Community Health
Workers, PHC: Primary Health Care, DEO: District Education Office, EHT: Environmental Health Technician
A-1-80

Health and Hygiene Education
2.4.4 HOW CAN WE SEE? (STEP BY STEP)
1. Monitoring Progress Monitoring: To make sure if process and progress in terms of organisational structure set-up, construction and training are made on time
according to the work plan developed in the planning workshop. Impact Monitoring: To see how the objectives were achieved in terms of degree of community participation, human resource development and institutionalisation. The following table 2.4.3 is the types of monitoring sheet introduced to assist the health educators and supervisors to record monitor and assess their door-to-door promotional activities in the community and to see whether their coverage is also recording some impact. The summary of monitoring sheet is shown in table 2.4.4 and a sample can be referred in Annex 12.
Table 2.4.3 Device of Monitoring Sheet Name Characteristics of the Sheet
Register book
□ Gives information (name, plot number, family members, environmental health situation) about each household visit
□ Tracing the households being reached by numbers can be easily seen and counted
Monthly return forms
□ Gives summarized monthly data and information (such as total number of people received health education door-to-door visit per month, topics covered etc.)
□ It is a simple and easy sheet to be filled by community health workers (educators)
Table 2.4.4 An Example of Process Monitoring Sheet
What is to be checked
Who will check?
How often?
How should it be checked
Likely problems to arise
Action to be taken By whom
When
1. Door-to-door campaign
EHT Every month
Monthly return forms
Some CHW drop out
Examine performance and replace if necessary
CHWs
Within the month
2. Drama
CHWs Each time Record of drama session
Topic not well understood
Change or simplify script, discuss with drama group
CHWs Before next session
2. Evaluation Evaluation should be carried out, preferably 1 or 2 years after the project starts, with active participation by the community, other community workers, officials and representatives of neighbouring communities if necessary. After the evaluation is concluded, lessons learnt and recommendations should be summarised. The main objectives of the evaluation are: 1) To assess if process/progress were performed effectively on time and made towards
achieving its objectives (how much has been done, or still needs to be done) 2) To clarify its objectives and policies and assess its relevance (objectives set in the
workshop were relevant to national goal and policies) 3) To find out what impacts were observed (expected or unexpected, positive or negative) 4) To see how efficient the work was done (use of resources input) 5) To look at the project sustainability (Was management system developed? Was corrective
action solve problems occurred?)
SEE
A-1-81

Health and Hygiene Education
■■■■ CHECKLIST FOR SEEING
Step Action Checkpoint 1.1 Develop process & impact monitoring sheets
□◆If there has been a time break between this activity and the previous one (See ‘DO’ section), start with a group discussion to review what was decided at the previous workshop. □◆Show the drawings which represent goals of the project. □◆Have a monitoring sheets (on flip chart) ready (SEE previous page for sample monitoring sheets). □◆Ask the person who were selected to manage specific tasks (those who were chosen during the “PLAN” and “DO” workshop activity) to facilitate a discussion on the followings: 1) How to measure, 2) How often progress and impact should be measured, 3) who should be responsible, 4) likely problems, 5) actions taken by whom by when. (See Table 2.4.4.). □◆Set a date(a few days) for the project evaluation.
1.2 Monitor Process to see if the process and progress were made according to the work plan developed in the workshop.
□◆Check if organisational structure of CHW/SHCC is established and organizational capacity is build by using INSTITUTIONAL CAPACITY BUILDING MONITORING SHEET.(See Table 1.3.1.) □◆Check if activities planned are on schedule by using PROCESS
MONITORING SHEET. (See Table 2.4.4.) □◆Check if anything went wrong and why.
1. Monitoring
1.3 Monitor Impact to see if the performance of activities is done towards achieving objectives.
□◆Check impacts on community(students), either positive, negative, planned or unforeseen. □◆Check how CHW(SHCC), RDC, EHT, LCC, NGO are actively play defined roles in each steps of “DO” stage □◆Check how CHW(SHCC) had institutional change and learning in the process of latrine development through monitoring sheet. □◆Check every week how many CHW work actively consider replacing drop outs.
2.1 Check Objectives and policies
□◆Understand why you are evaluating by reviewing the objectives set at the CAP workshop and its relevance with district goal.
2.2 Evaluate progress of activities
□◆Check if all activities in the work plan are performed effectively on time by using PROCESS MONITORING SHEETS □◆Clarify the successful issues and problems encountered through mapping, community role play etc □◆Analyse the problems 1)if community can deal with them by itself, 2)if the participants fully understand, 3) if it can be solved by the community itself. □◆Find what actions/solutions should be taken for, how they will get more information and when and who will do it for solving, and how they will get outside help to overcome those problems
2.3 Evaluate Project Impact □◆Ask the group to look at the work plan developed to compare what it planned to do with what it has achieved and check the degree of participation in all process of the project □◆Check if the community organisations (NHC/CHW/SHCC) were grown-up by using INSTITUTIONAL BUILDING MONITORING SHEET □◆Check if CHW, SHCC, RDC, EHT, LCC, NGO actively played defined roles in each steps of “DO” stage
2.4 Evaluate Efficiency □◆Check if the project inputs were cost-efficient. □◆Check if timeframe and period were appropriate (not too short or long and good season to construct, etc) to achieve objectives. □◆Check if the inputs of human resources were enough for workload
2. Evaluation
2.5 Evaluate Sustainability □◆Check if physical maintenance system is established. □◆Check if institutional capacity was built. □◆Check if school running system is established (income generation, teacher’s allowance, etc).
◆◆◆◆School Health component NHC: Neighbourhood Health Committee, CHW (Community Health Workers), EHT:
Environmental Health Technician, SHCC: School Health Coordination Committee
A-1-82

Health and Hygiene Education
2.4.5 HOW CAN WE SUSTAIN? (STEP BY STEP)
1. Institutional Capacity Building Improving institutional/organisational capacities are very important not only for ensuring good quality of voluntary health workers (such as CHWs) or SHCC members’ activities but also achieving sustainable project. A group
mechanism to increase commitment and motivation to carry out their agreed responsibilities should be established at the planning stage. Box 2.4.3 is an example of such a mechanism.
Box. 2.4.3 Mechanism for Incentives for NHC (CHWs) and SHCC Agree with health facility such as nearby health center that members can receive supervisory visit by the
professional staff (health staff) at least once a month Establish a monthly meetings with health facility staff to, review achievements, constraints and discuss
solutions and future plans. Group members themselves decide on penalties for those not working hard and evaluate institutional capacity
of their own each month and decide on replacement, change in roles Provision of I.D card and a certificate to provide form of identity for recognition by the community members Some remuneration (from water project incomes etc.) system Some members are benefited from other project (such as water, sanitation, micro finance)
2. Management of School Health Facilities Financial and human resources constraints make the government difficult to be responsible for school health environment. Therefore, we must encourage students, teachers and parents to improve the school environment. Table 2.4.5 is for school health facilities improvements: Table. 2.4.5 Guidelines for School Health Facilities Improvements
Category REMARKS Water □If water is used for flush toilet, water point should be near the latrine
□Hand washing facilities should be built near the latrine and allow for the placement of soap or other cleaning agents □Piped water supply with public tap should be considered □Capacity of water supply system should be designed based on demand during the peak hours since school water system is connected to the municipal system
Sanitation □VIP is most suitable in areas where sufficient water for flushing is not available. It is Advisable to build separate latrine for teachers □Site selection of latrine needs careful consideration (close to school building is better but if too close, stench may penetrate the classrooms) □It is not advisable to burn garbage, in view of health hazards such as respiratory diseases. Plastic and tin waste have to be dealt with separately (Recycling/disposed through LCC collection system)
2. Maintenance of School Health Facilities Good cleaning and maintenance system of the water and sanitation facilities is the most important. Poor maintenance system often causes an even bigger health risk than scattered defecation. Stagnant water around tap stands and blocked drainage channels attracts rodents and forms a breeding place for mosquitoes. It must be planned before construction. 3. Further expansion of the project
If a Community and School H&H education project can be sustainable, a mechanism of revolving fund or fund raising may be considered during the project period and afterwards.
SUSTAIN
A-1-83

Health and Hygiene Education
■■■■ CHECK LIST FOR SUSTAINING Step Action Checkpoint
1. Institutional capacity building
1.1 CHW/SHCC sustainability (how to avoid dropouts)
□◆Hold periodical meetings to check progress/process as well as institutional capacity (see “SEE” section 1-2, 2-3 in detail). □◆Make guideline for the group that clearly describe group rules, each person’s defined roles and responsibilities, and penalties if any.
2.1 Problem analysis of environmental health conditions at school
◆Assess current conditions at school (see “PLAN” for more information) by using participatory exercises such as: drawing of maps of the neighbourhood, indicating water sources, latrines, solid waste collection points. Indicates areas which constitute a health risk
2. Management of School Health Facilities 2.2 Appropriate
technology and selection of sites
◆Consider the following when planning (see“PLAN”) and selecting the right technology. 1) Technical Department: required service level, present and potential water sources and their capacities and quality, capital and O&M costs of technical options, local technical skills needed for construction and O&M. 2) Support: support from private sector or NGOs, technical support capacity of LCC, DHMT, and DEO for maintenance, and cooperation between departments involved (health, education, technical etc.). 3) Community/School: Number of students and staff, estimated total/peak consumption, required service level, ability to pay costs for O&M, ability/ willingness to maintain facilities, clarity on how maintenance will be arranged before construction starts, present type of school water supply, latrine, cultural aspects to be considered. ◆Select technology location of the facilities applicable for the current school setting. ◆Involve community skilled mason, parents, private sectors in construction to limit costs (Be careful not to exploit children for labour). ◆SHCC should be responsible for construction, funds, materials, transportation and design, and M&E (see previous “SEE” section).
3. Maintenance of school health facilities
3.1 Maintenance ◆It is important that schools/communities contribute as much as possible to the O&M costs since it will increase feeling of responsibility, ownership and motivate them to maintain facilities ◆Possible funding options are: contribution from parents, donations from political parties or religious groups and school maintenance budget (See 4.1) ◆Cleaning could be done by several organisational options such as: cleaning committee, by classes on a rotation basis, with or without a rewarding mechanism. ◆Even though students are involved, final responsibility, involving supervision and corrective action if needed, should usually remain with the SHCC
4. Further expansion of the project
4.1 Sourcing for Funds
□Seek for donor/NGO fund by sending a proposal □Try income generating activities (IGAs) by letting facilities for church, or creating sanitary mart (SEE “DO” section) □Try fund raining (Brai, Drama, Lottery, Football game) □Try to contact private company for financial assistance. □Consult with health centre in charge to start promoting “Clorin” as one of revolving fund system (500kw-350kw=150kw can be kept by CHWs per bottle). □seek possibility of other forms of revolving fund (T-shirt selling, soya beans revolving etc.)
◆School Health Component Checkpoints DEO: District Education Office, DHMT: District Health Management
Team, SHCC: School Health Coordination Committee
A-1-84

Health and Hygiene Education
2.4.6 LET’S ENVISAGE PROCESS AND ACTORS After understanding ‘Plan, Do, See and Sustain’, let us envisage and illustrate how the project is preceded and implemented. A project work plan (Table 2.4.6) and more concrete annual work plan (Table 2.4.7) must be designed as follows. The work plan should be used
as one of the indicators for progress in monitoring and evaluation. Table 2.4.6 Example of a Health and Hygiene Education Project work plan
Table 2.4.7 Example of an ANNAUAL work plan for Community Education
WORKPLAN
& ACTORS
SCHOOL HEALTH PROJECT M1 M2 M3 M4 M5 M6 M7 M8 M9 M10 M11 M12COMMUNITY HEALTH PROJECT M1-2 M3-4 M5-6 M7-8 M9-10 M11-12 M13-14 M15-16 M17-18 M19-20 M21-22 M23-24
PLAN 1.Identify Problem/Assess Needs2.Identify Supporting Agencies3.Analyse Problem and Plan forsolution
DO 4.Plactical Training5.Implementation of Health andHygiene education (School HealthServices)
SEE 6.Monitoring7.Evaluation
Main Activity/Subactivity No.
Description Indicator Means ofVerification
(MOV)
ResourceCommunity
input
Resourcerequired
External input
ResponsibleParty
Timing
1.1 Workshop
1.1.1Design training programme andprepare training handouts
1.1.2Conduct practicaltraining(theory, technology)
1.1.3 1.1.4
1.2
Implementation of Health andHygiene Education (and schoolhealth services) Activities
1.2.1 Conduct sensitisation campaign 1.2.2 Door-to-door campaign 1.2.3 Educational drama 1.2.4 Training of other teachers
(3) Community based health and hygiene education program activities are implemented
Objective
Project Outcome: (1) A Community Health Workers are organized under Clinic
(1) A model for participatory health and hygiene education is developed by the community
(2) An appropriate training course method (a course module and a manual) is developed
(2) Health and hygiene conditions of people in the project area are further improved with the added impactof the Water Supply Project
A-1-85

Health and Hygiene Education
Also when all stakeholders are identified, everybody must recognise their role and responsibilities. In each action/step, different group of people have different level of responsibilities. (Table 2.4.8)
Table 2.4.8 Role and Responsibilities of Stakeholders
The following Venn diagram illustrates how key institutions and groups have interactions. Community has close contacts and cooperation in decision-making with NGO and LCC on daily basis, while donor and DHMT/Clinic play as back supporting agencies as required.
Figure 2.4.1 Stakeholders Relationship (Venn Diagram)
NHC/CHW/SHCC RDC EHT
LCC(site
oficer)Health Center
(DHMT) NGO DonorPLAN 1.Identify Problem/Assess
Needs2.Identify SupportingAgencies3.Analyse Problem andPlan for solution
DO 4.Plactical Training5.Implementation of Healthand Hygiene education(School Health Services)
SEE 6.Monitoring7.Evaluation
SUSTAIN 8.Institutional CapacityPrimary Roles Secondary Roles
Donor
RDC:Collaboration,monitoring activities(bi monthly meetings)
NHC (CHW):Sensitization CampaignHealth&hygiene educationM&E
NGO:Training, Technical assistance &Advise
LCC site officer: Identify Problems, coordination and support
Community:Contribution through attending meetings, drama performances
EHT:Technical assistance&Monitoring&evaluation
Clinic: Supervising staffs,Coordination with RDCand school
DHMT:Training, Advise & policy guidance, provide schoolHealth services
Community
NGOEHT,
Public HealthNurses
LCC
Donor:Provide fund
RDC
NHC(CHW)
Clinic
SHCC
School
DHMTDEODEO:Supervise schoolAdvise&policy guidance,
School: Supervising SHCC,Coordination with RDC,clinic
SHCC: Planning, implementation, M&E
Donor
RDC:Collaboration,monitoring activities(bi monthly meetings)
NHC (CHW):Sensitization CampaignHealth&hygiene educationM&E
NGO:Training, Technical assistance &Advise
LCC site officer: Identify Problems, coordination and support
Community:Contribution through attending meetings, drama performances
EHT:Technical assistance&Monitoring&evaluation
Clinic: Supervising staffs,Coordination with RDCand school
DHMT:Training, Advise & policy guidance, provide schoolHealth services
Community
NGOEHT,
Public HealthNurses
LCC
Donor:Provide fund
RDC
NHC(CHW)
Clinic
SHCC
School
DHMTDEODEO:Supervise schoolAdvise&policy guidance,
School: Supervising SHCC,Coordination with RDC,clinic
SHCC: Planning, implementation, M&E
A-1-86