2015 Presentation for Providers 2
25
Evaluation And Management Coding For Psychiatry KEY COMPONENTS OF DOCUMENTATION PRESENTER: DEBBIE FLEMINGS, CPC 1
-
Upload
debbie-flemings-cpc -
Category
Documents
-
view
83 -
download
0
Transcript of 2015 Presentation for Providers 2
Evaluation And
Management Coding For
PsychiatryKEY COMPONENTS OF DOCUMENTATION
PRESENTER: DEBBIE FLEMINGS, CPC
1
Why Is Documentation So Important?
Accurate documentation of medical records provides for program
integrity, ensures patient safety, and protects our providers.
Providers’ claims must be accurate and billable with the correct code, not
just the code that offers the greatest reimbursement.
This ensures that payer programs such as Medicare and Medicaid pay the
correct amount – not too much, not too little, and ensures that the
programs pay the right people.
Healthcare delivery is becoming increasingly more complex and the
medical data describing the services performed is growing. Increased
medical complexity requires increased documentation complexity.
2
Why Is Medical Coding So Important?
Medical coding helps prove the medical necessity of treatment.
The narrative text is matched to a code that has a corresponding charge.
This coding of services is the main source for accurate reimbursement of
services.
Insurance companies often perform random reviews to ensure charges
are valid. Accurate coding and detailed documentation help insurance
companies to understand why specific charges were submitted.
3
What Is The Purpose Of Auditing?
Quality healthcare is based on accurate and complete clinical
documentation in the medical record. The best way to improve our
clinical documentation and the livelihood of our organization is through
medical record auditing.
Goals: Improve the financial health of our practice.
Audits specifically target and evaluate procedural and diagnosis code
selection as determined by physician documentation.
4
“
”
If It Isn’t Documented, It Hasn’t Been
Done
AN ADAGE THAT IS FREQUENTLY HEARD IN THE HEALTH CARE SETTING
Bringing It All Together:
Accurate and complete documentation can serve purposes that are outside of their existing purposes such as, legal interests of the affected individuals. The medical professionals are then, protected by maintaining records which serve as valuable references. They can also explain potential health risks for the family of which the individual belongs.
These specific tasks will help maintain a highly systematic and organized record keeping.
5
Introducing E/M Coding
General Principles
Reason for the encounter and relevant history, physical examination findings, and prior diagnostic test results
Assessment, clinical impression or diagnosis
Plan for care
Date and legible identity of the observer
Rationale for ordering ancillary services should be easily inferred
Appropriate health risk factors should be identified
Document the patient’s response to, changes in treatment, and revision of diagnosis
Past and present diagnoses should be accessible
The CPT and ICD-10-CM codes reported should be supported
6
E/M Key
Component
Overview
7
History
Examination
Medical Decision Making
Counseling
Coordination of Care
Time
Nature of presenting problem
History Detail
HistoryChief Complaint
History of Present Illness
Past, Family, and Social History
Review of Systems
Chief ComplaintCC states the reason for the encounter
May be from the provider perspective
May be from the patient perspective
All Levels of History Require a CC
HPIDescription of the development of the patient’s present illness from the first sign and/or symptom or from the previous encounter to the present.
Elements:
Location, Quality, Severity, Duration, Timing, Context, Modifying Factors, and Associated Signs/Symptoms
8
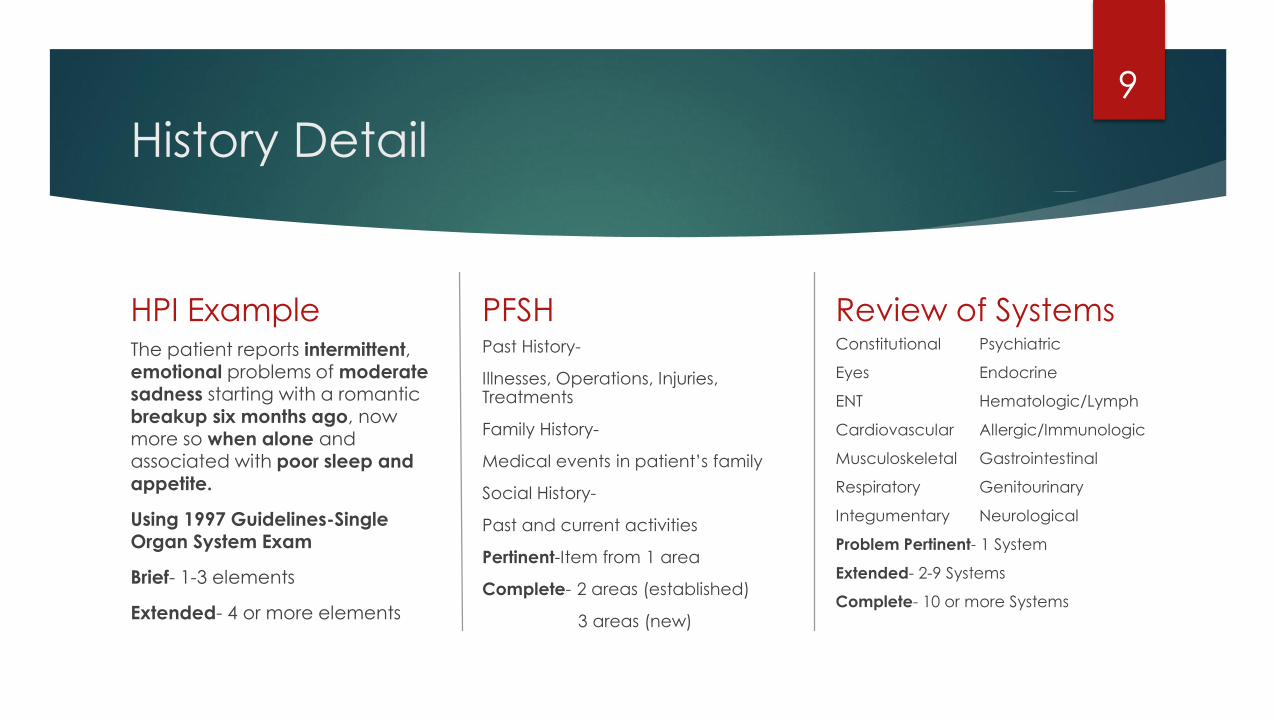
History Detail
HPI ExampleThe patient reports intermittent, emotional problems of moderatesadness starting with a romantic breakup six months ago, now more so when alone and associated with poor sleep and
appetite.
Using 1997 Guidelines-Single Organ System Exam
Brief- 1-3 elements
Extended- 4 or more elements
PFSHPast History-
Illnesses, Operations, Injuries, Treatments
Family History-
Medical events in patient’s family
Social History-
Past and current activities
Pertinent-Item from 1 area
Complete- 2 areas (established)
3 areas (new)
Review of SystemsConstitutional Psychiatric
Eyes Endocrine
ENT Hematologic/Lymph
Cardiovascular Allergic/Immunologic
Musculoskeletal Gastrointestinal
Respiratory Genitourinary
Integumentary Neurological
Problem Pertinent- 1 System
Extended- 2-9 Systems
Complete- 10 or more Systems
9
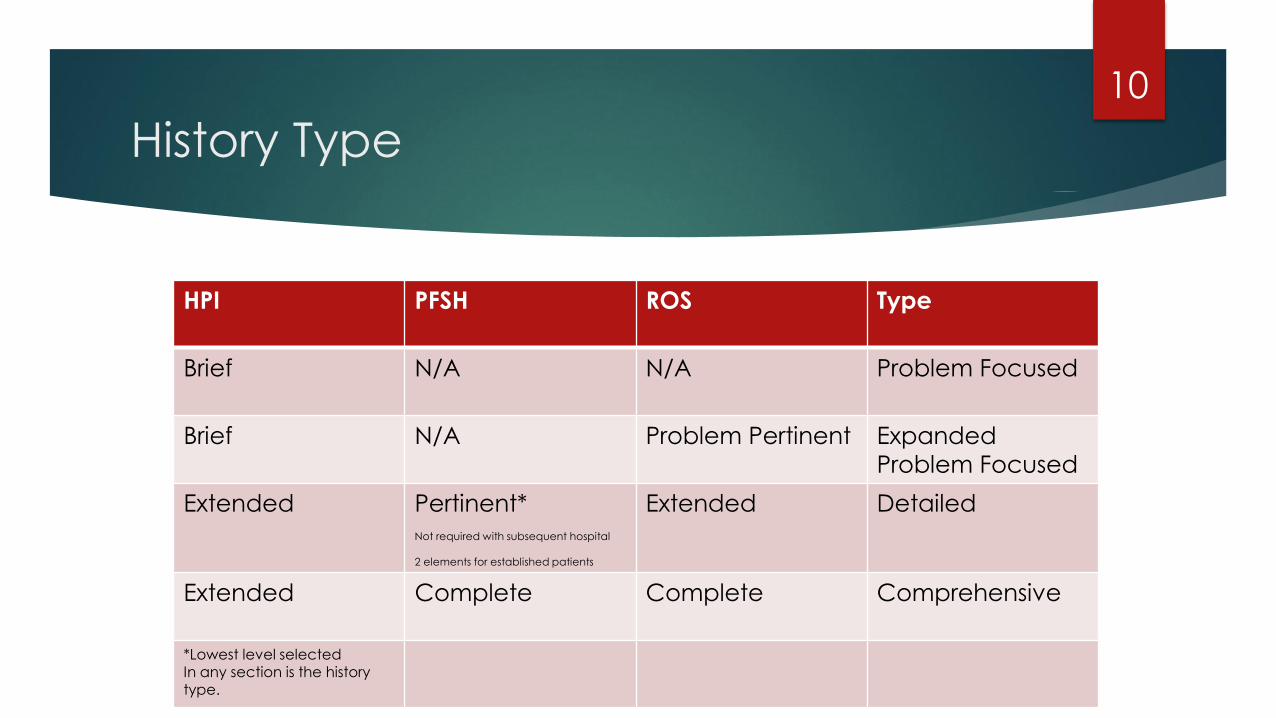
History Type
HPI PFSH ROS Type
Brief N/A N/A Problem Focused
Brief N/A Problem Pertinent Expanded
Problem Focused
Extended Pertinent*Not required with subsequent hospital
2 elements for established patients
Extended Detailed
Extended Complete Complete Comprehensive
*Lowest level selectedIn any section is the history
type.
10

Psychiatric Examination Detail
Constitutional
Three Vital Signs:
Sitting or standing blood
pressure,
supine blood pressure, pulse
rate and regularity
respiration, temperature,
height, weight
*Shaded
Musculoskeletal
Assessment of muscle strength and
tone, with notation of any atrophy or
abnormal movements
Examination of gait and station
*Unshaded
Mental Status ExamSpeech
Thought process
Associations
Abnormal or psychotic thoughts
Judgment and insight
Orientation
Recent and remote memory
Attention span and concentration
Language
Fund of knowledge
Mood and affect *Shaded
11
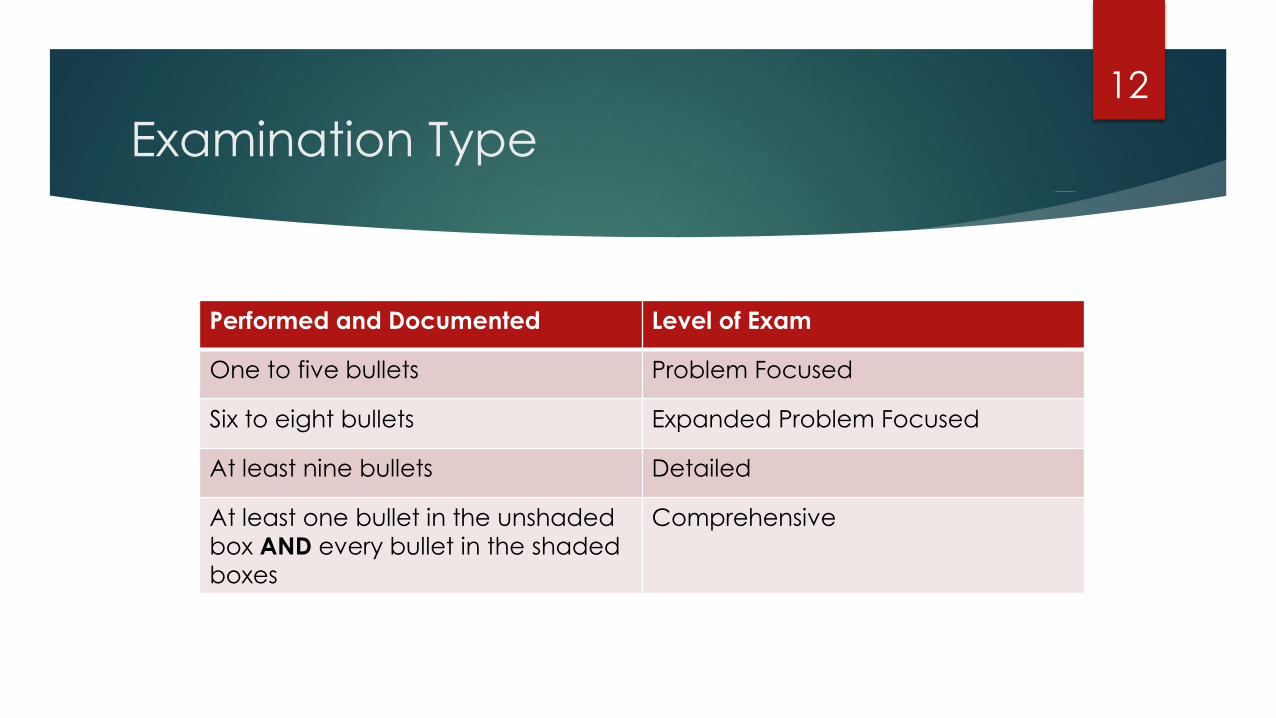
Examination Type
12
Performed and Documented Level of Exam
One to five bullets Problem Focused
Six to eight bullets Expanded Problem Focused
At least nine bullets Detailed
At least one bullet in the unshaded
box AND every bullet in the shaded
boxes
Comprehensive
Medical Decision
Making Process
13
Number of diagnoses or
management options
Amount and/or complexity of
data to be reviewed
Risk of complications and/or
morbidity or mortality
*2/3 elements must be met or exceeded for scoring
level of MDM
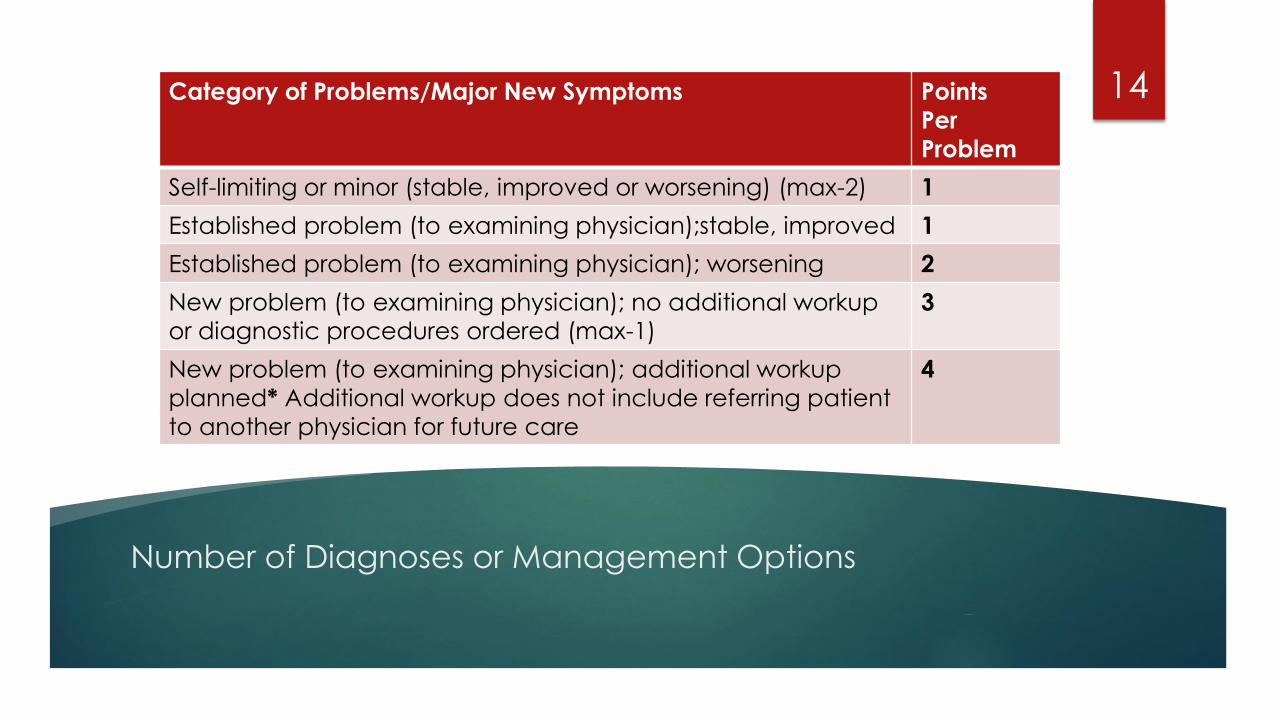
Number of Diagnoses or Management Options
14Category of Problems/Major New Symptoms Points
Per
Problem
Self-limiting or minor (stable, improved or worsening) (max-2) 1
Established problem (to examining physician);stable, improved 1
Established problem (to examining physician); worsening 2
New problem (to examining physician); no additional workup
or diagnostic procedures ordered (max-1)
3
New problem (to examining physician); additional workup
planned* Additional workup does not include referring patient
to another physician for future care
4
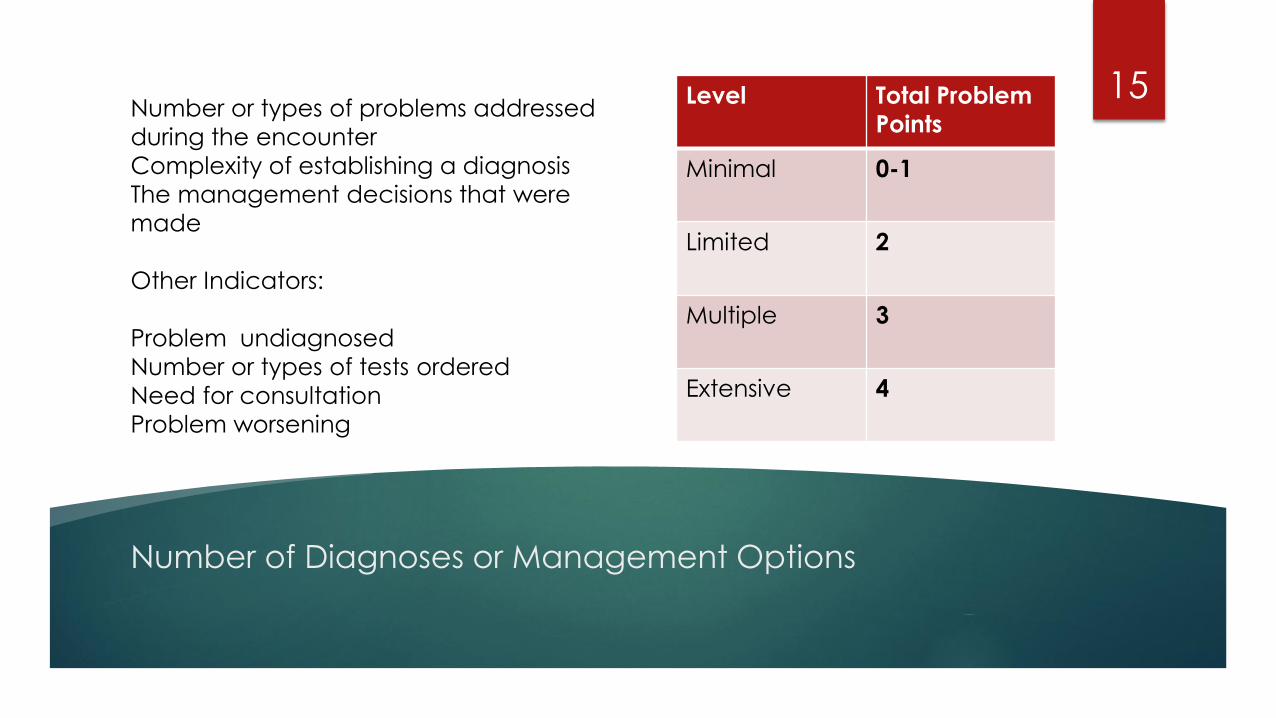
Number of Diagnoses or Management Options
15Number or types of problems addressed
during the encounter
Complexity of establishing a diagnosis
The management decisions that were
made
Other Indicators:
Problem undiagnosed
Number or types of tests ordered
Need for consultation
Problem worsening
Level Total Problem
Points
Minimal 0-1
Limited 2
Multiple 3
Extensive 4
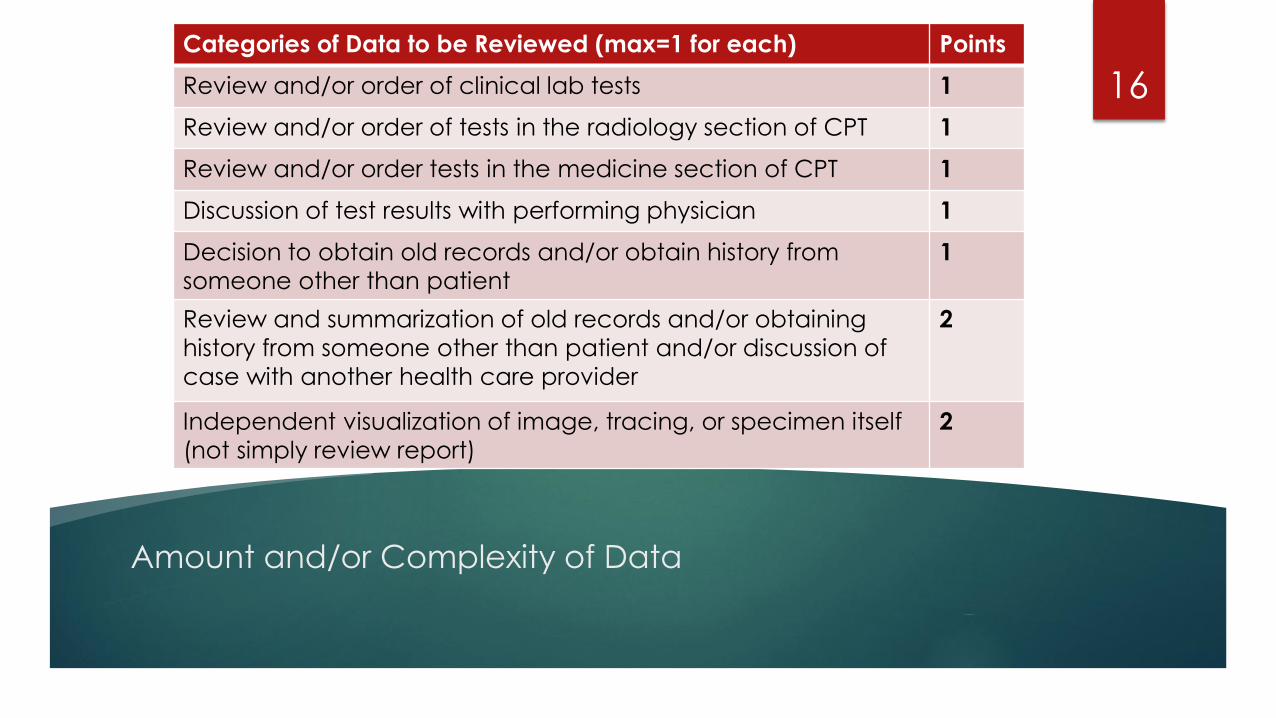
Amount and/or Complexity of Data
16
Categories of Data to be Reviewed (max=1 for each) Points
Review and/or order of clinical lab tests 1
Review and/or order of tests in the radiology section of CPT 1
Review and/or order tests in the medicine section of CPT 1
Discussion of test results with performing physician 1
Decision to obtain old records and/or obtain history from
someone other than patient
1
Review and summarization of old records and/or obtaining
history from someone other than patient and/or discussion of
case with another health care provider
2
Independent visualization of image, tracing, or specimen itself
(not simply review report)
2
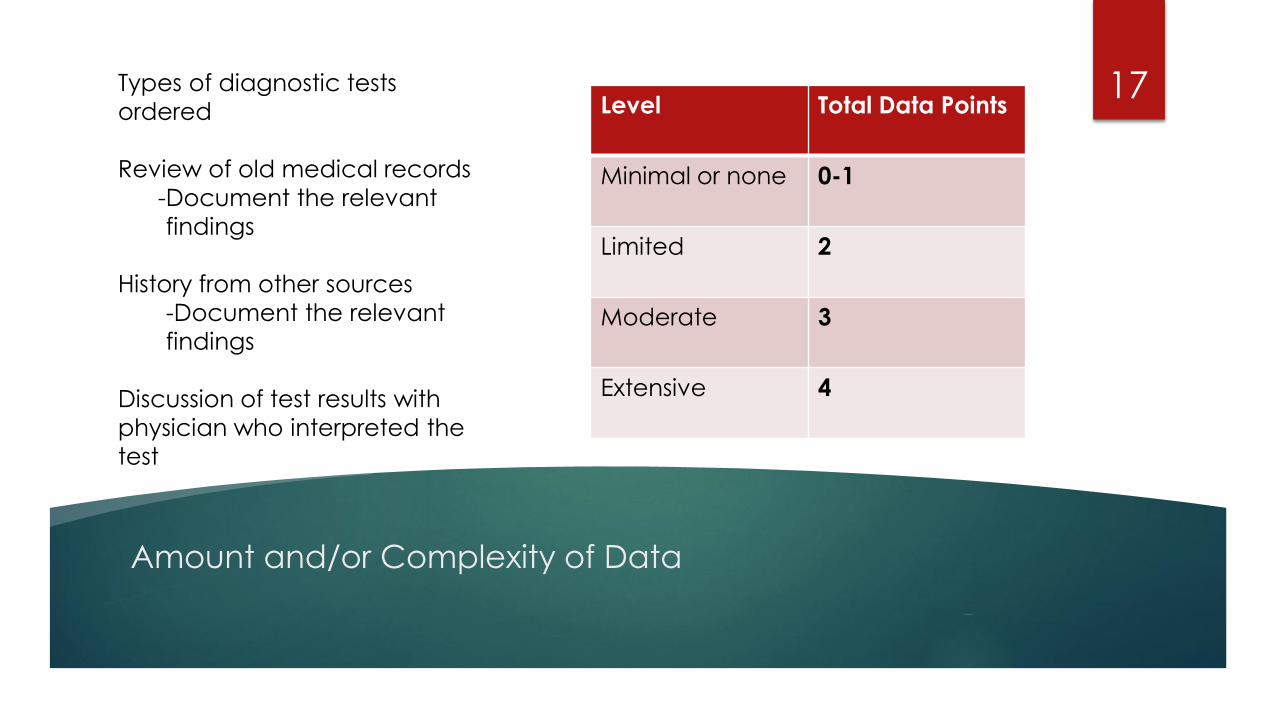
Amount and/or Complexity of Data
17Types of diagnostic tests
ordered
Review of old medical records
-Document the relevant
findings
History from other sources
-Document the relevant
findings
Discussion of test results with
physician who interpreted the
test
Level Total Data Points
Minimal or none 0-1
Limited 2
Moderate 3
Extensive 4
Risk of Significant
Complications,
Morbidity, and/or
Mortality
18
Based on risks associated
with the presenting
problem, diagnostic
procedure, and the
possible management
options
The highest level of risk in
any one of these
categories determines
the overall risk.
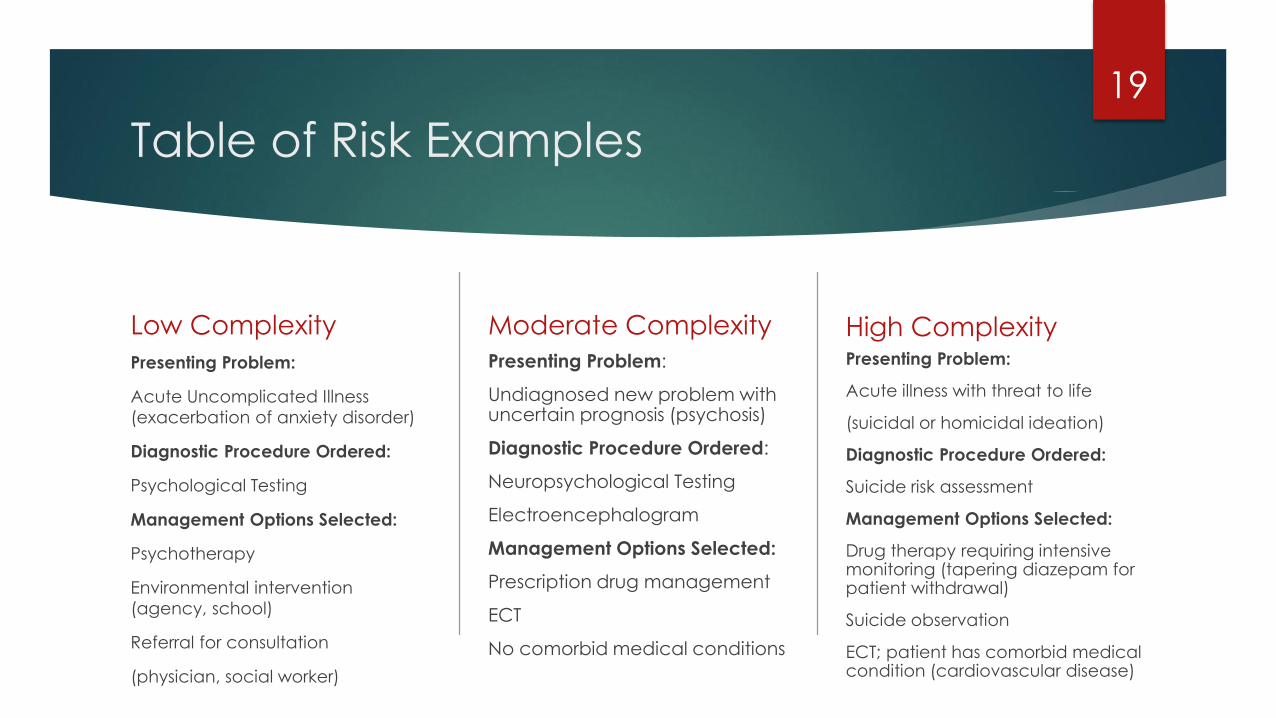
Table of Risk Examples
Low Complexity
Presenting Problem:
Acute Uncomplicated Illness
(exacerbation of anxiety disorder)
Diagnostic Procedure Ordered:
Psychological Testing
Management Options Selected:
Psychotherapy
Environmental intervention
(agency, school)
Referral for consultation
(physician, social worker)
Moderate Complexity
Presenting Problem:
Undiagnosed new problem with uncertain prognosis (psychosis)
Diagnostic Procedure Ordered:
Neuropsychological Testing
Electroencephalogram
Management Options Selected:
Prescription drug management
ECT
No comorbid medical conditions
High ComplexityPresenting Problem:
Acute illness with threat to life
(suicidal or homicidal ideation)
Diagnostic Procedure Ordered:
Suicide risk assessment
Management Options Selected:
Drug therapy requiring intensive monitoring (tapering diazepam for patient withdrawal)
Suicide observation
ECT; patient has comorbid medical condition (cardiovascular disease)
19
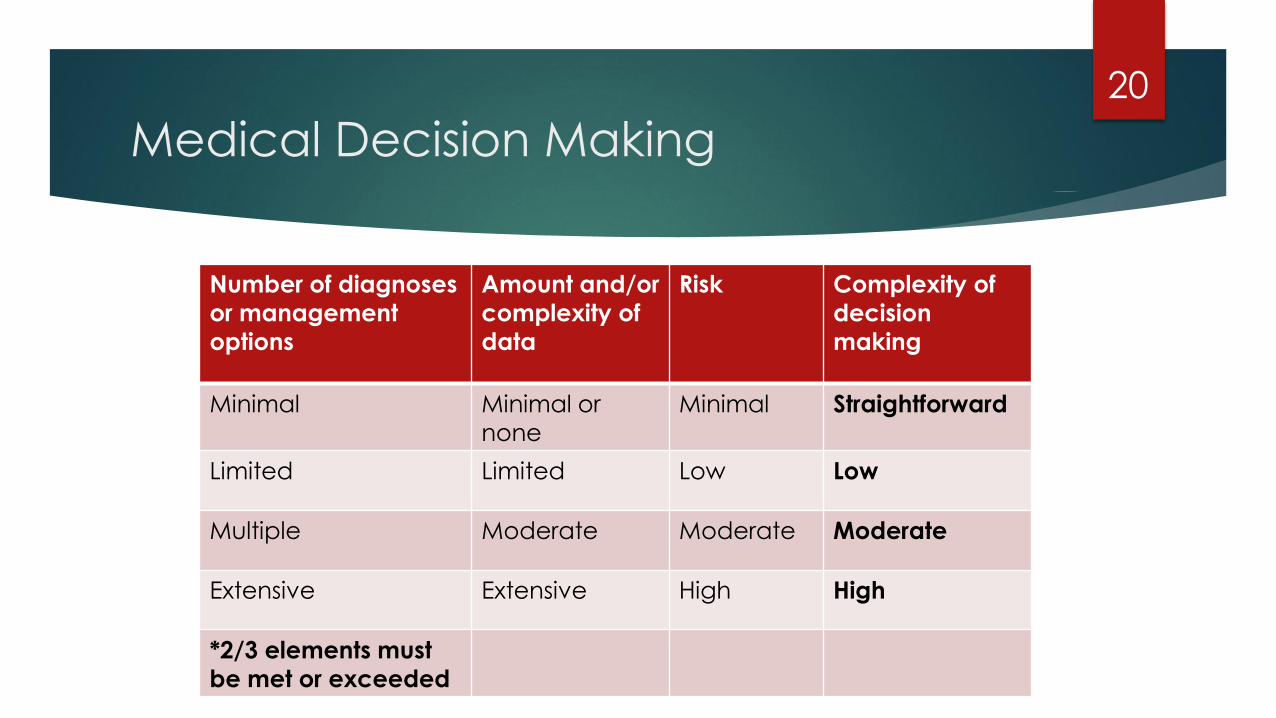
Medical Decision Making
20
Number of diagnoses
or management
options
Amount and/or
complexity of
data
Risk Complexity of
decision
making
Minimal Minimal or
none
Minimal Straightforward
Limited Limited Low Low
Multiple Moderate Moderate Moderate
Extensive Extensive High High
*2/3 elements must
be met or exceeded
Selecting The
Appropriate Level
of E/M Service
21
For New Patients:
The three key components (History,
Exam, and MDM) must meet or
exceed in complexity with the stated
requirements for office visits and
initial hospital care.
Example:
Detailed History, Detailed Exam, and
Low MDM would qualify for 99203.
For Established Patients:
Two of the three key components
must meet or exceed in complexity
with the stated requirements of
office visits and subsequent hospital
care.
Example:
A Comprehensive History,
Comprehensive Exam, and
Moderate MDM still qualifies for
99215 because two out of the three
components meet.
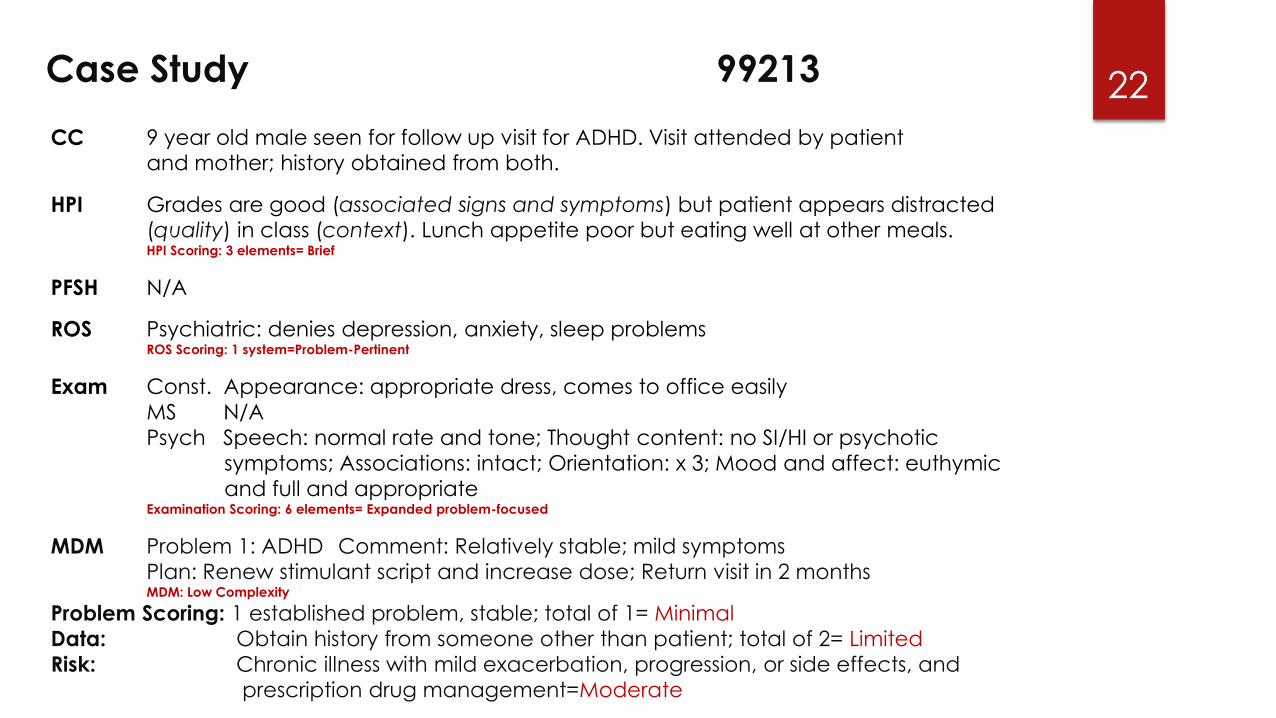
22Case Study 99213
CC 9 year old male seen for follow up visit for ADHD. Visit attended by patient and mother; history obtained from both.
HPI Grades are good (associated signs and symptoms) but patient appears distracted(quality) in class (context). Lunch appetite poor but eating well at other meals.HPI Scoring: 3 elements= Brief
PFSH N/A
ROS Psychiatric: denies depression, anxiety, sleep problemsROS Scoring: 1 system=Problem-Pertinent
Exam Const. Appearance: appropriate dress, comes to office easily
MS N/A
Psych Speech: normal rate and tone; Thought content: no SI/HI or psychotic
symptoms; Associations: intact; Orientation: x 3; Mood and affect: euthymic
and full and appropriateExamination Scoring: 6 elements= Expanded problem-focused
MDM Problem 1: ADHD Comment: Relatively stable; mild symptoms
Plan: Renew stimulant script and increase dose; Return visit in 2 monthsMDM: Low Complexity
Problem Scoring: 1 established problem, stable; total of 1= Minimal
Data: Obtain history from someone other than patient; total of 2= Limited
Risk: Chronic illness with mild exacerbation, progression, or side effects, and
prescription drug management=Moderate
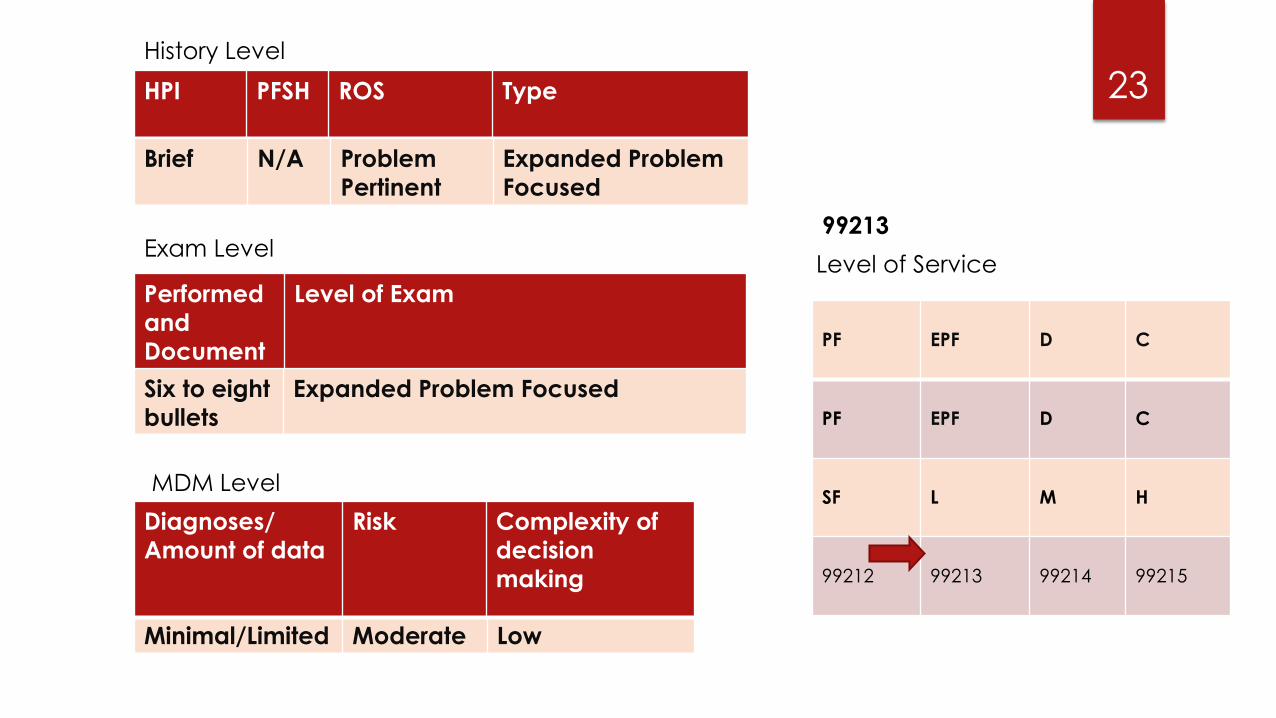
23HPI PFSH ROS Type
Brief N/A Problem
Pertinent
Expanded Problem
Focused
Performed
and
Document
ed
Level of Exam
Six to eight
bullets
Expanded Problem Focused
History Level
Exam Level
MDM Level
Minimal/Limited Moderate Low
Diagnoses/
Amount of data
Risk Complexity of
decision
making
99213
Level of Service
PF EPF D C
PF EPF D C
SF L M H
99212 99213 99214 99215
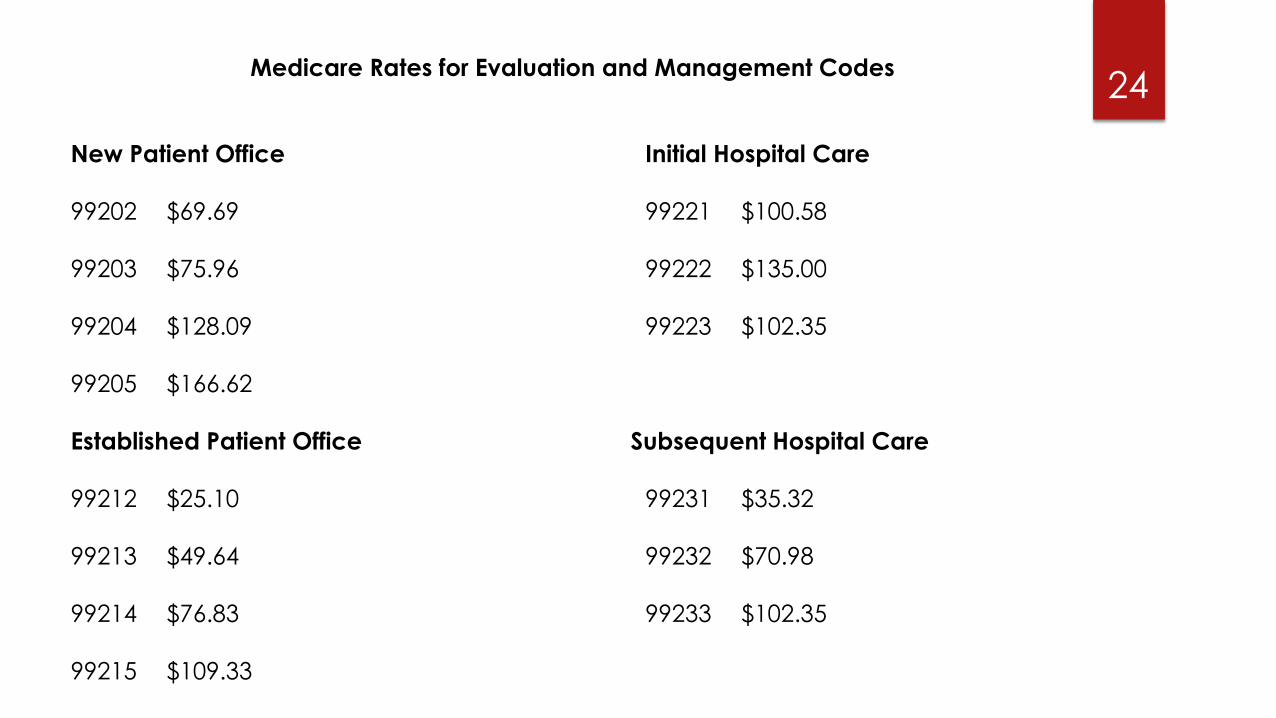
24Medicare Rates for Evaluation and Management Codes
New Patient Office Initial Hospital Care
99202 $69.69 99221 $100.58
99203 $75.96 99222 $135.00
99204 $128.09 99223 $102.35
99205 $166.62
Established Patient Office Subsequent Hospital Care
99212 $25.10 99231 $35.32
99213 $49.64 99232 $70.98
99214 $76.83 99233 $102.35
99215 $109.33
25
Any Questions?